Combined Transbronchial Needle Aspiration And PET/CT For Mediastinal Staging Of Lung Cancer Şermin Börekçi 1 , Osman Elbek 1 , Nazan Bayram 1 , Nevin Uysal 1 , Kemal Bakır 2 1 Department of Pulmonary Diseases, University of Gaziantep, School of Medicine 2 Department of Pathology, University of Gaziantep, School of Medicine
Transcript
Combined Transbronchial Needle Aspiration And PET/CT
For Mediastinal Staging Of Lung Cancer
Şermin Börekçi1, Osman Elbek1, Nazan Bayram1, Nevin Uysal1, Kemal Bakır2
1Department of Pulmonary Diseases, University of Gaziantep, School of Medicine
2 Department of Pathology, University of Gaziantep, School of Medicine
1.INTRODUCTION AND AIM-I
The most common cancer is lung cancer on
the world
Lung cancer responsible for %12.8 of all
cancer cases, %17.8 of all death due to cancer
on the world, acording to 1999’s datas
The Turkish Thoracic Society. The guide for diagnosis and treatment of lung cancer. Thorax Journal. 2006;7(2):1-35.
1.INTRODUCTION AND AIM-II
The %70 of all lung cancer cases are at
advanced (stage IV) or localy advanced
stage (stage IIIA and IIIB) when diagnosed
and they have no chance to surgery
options for radical treatmentThe Turkish Thoracic Society. The guide for diagnosis and treatment of lung cancer. Thorax Journal.
2006;7(2):1-35.
1.INTRODUCTION AND AIM-III
Staging of patient is important for;
Evoluation of patient for surgery
Planning of treatment options
Determination of prognosis
Detterbeck FC, DeCamp MM, Kohman LJ, Silvestri GA.
Bayram N, Borekci S, Uyar M, Bakır K and Elbek O. Transbronchial needle aspiration in the
diagnosis and staging of lung cancer. Indian J Chest Dis Allied Sci 2008; 50: 273-276.
1949; Schieppati:
The first sampling from tracheal carina by using rigid bronchoscopy
1978; Wang:
Paratracheal lymph node sampling by TBNA
1979; Oho:
Using of flexible neddle with Fiberoptic bronchoscopy
1983; Wang:
Mapping and new kind of neddle for TBNA
1.INTRODUCTION AND AIM-VI
FACTORS FOR SUCCESS
Cell type of Cancer (small cell)
Right sided lesions
Large lymph nodes and masses
Localization of lesions
(paratracheal,
subcarinal)
Experience
Harrow E. Chest, 1991.Haponik EF. Am J Respir Crit Care Med, 1995.Harrow EM. Am J Respir Crit Care Med, 2000.
Herth FJ. Eur Respir J, 2006.
1.INTRODUCTION AND AIM-VII
A limited studies were present abouth
using PET/CT instead of CT with TBNA to
increase the success of TBNA.
Hsu LH, Ko JS, You DL, Liu CC, Chu NM. Respirology 2007; 12: 848-55.
Bernasconi, Gambazzi F, Bubendorf L, Rasch H, Kneilfel S, Tamm M. Eur Respir J 2006; 27:
889-94.
1.INTRODUCTION AND AIM-VIII
In our study we aimed to determine;
The role of TBNA with thorax CT and PET/CT
for lung staging
The comparision with mediastinoscopy
If this approach can reduce to need for
mediastinoscopy.
2. MATERIAL AND METHODS-I
Prospective, invasive, uncontrolled study
Department of Pulmonary Diseases, University of
Gaziantep
From march 2006 to March 2008
The patients who suspected lung cancer
Enlarged mediastinal lymph nodes (≥1 cm) localized on CT
Underwent PET/CT scanning
Consecutive 25 patients
2. MATERIAL AND METHODS-II
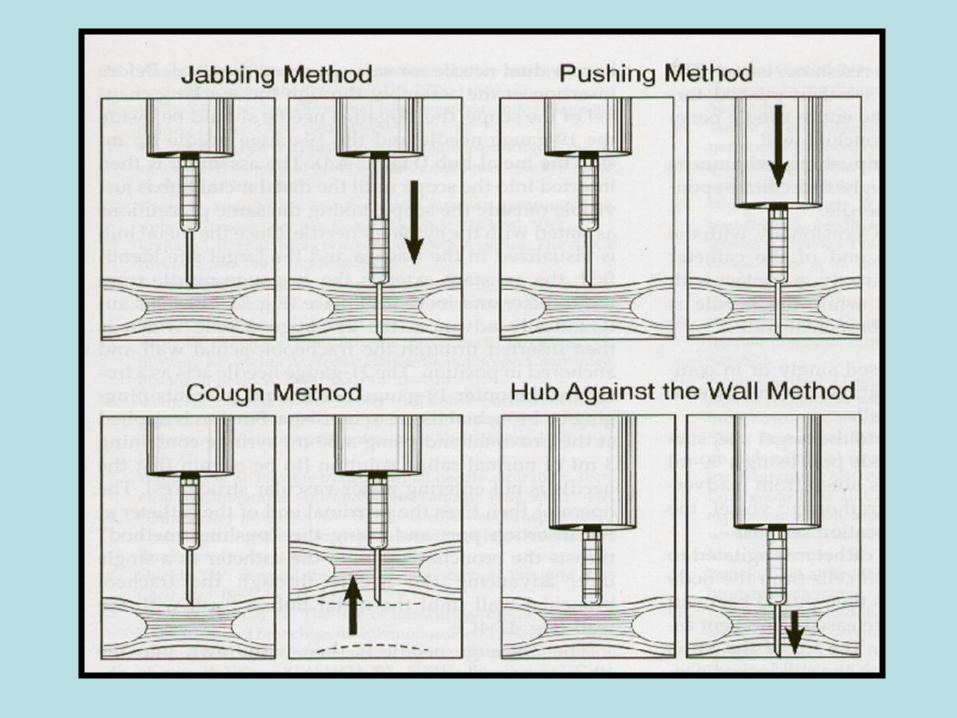
TBNA sampling:Flexible bronchoscopyThorax CT and PET/CT combinationAcording to Wang’s map of lymph node 22 Gauge aspiration needle 4 sampling from each lymph node station Starting from the lymph node that the most advanced stage The other kind of sampling procedures were done after TBNA sampling
2. MATERIAL AND METHODS-III
Evaluation of samples:Adequate Sample: presence of numerous benign lymphoid cells
Negative Malignite: absence of malignant cells
Positive Malignite: presence of malignant cells
2. MATERIAL AND METHODS-IVStatistical Analysis:
Mediastinoscopy was used as “gold standart”. The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy rate for prediction of lymph node staging of PET/CT combined TBNA were calculated.
Descriptive statistics were expressed as mean±standart deviation (SD), interquartile range (IQR) or percent (%) according to kind of data.
2. MATERIAL AND METHODS-V
Statistical Analysis:
The factors that might effect positive TBNA result
were analysed through logistic regression model
P value less than 0.05 was deemed statistically
significant.
The statistical analysis was performed using
SPSS 13.0 for Windows
3.RESULTS-I
Age (year, mean±SD) 58.7±7.6 Gender Male (n,%) 25 (100) Female 0 (0)Smoking (n,%) 25 (100)Smoking (pack/year) (median, IQR) 40 (30-55)
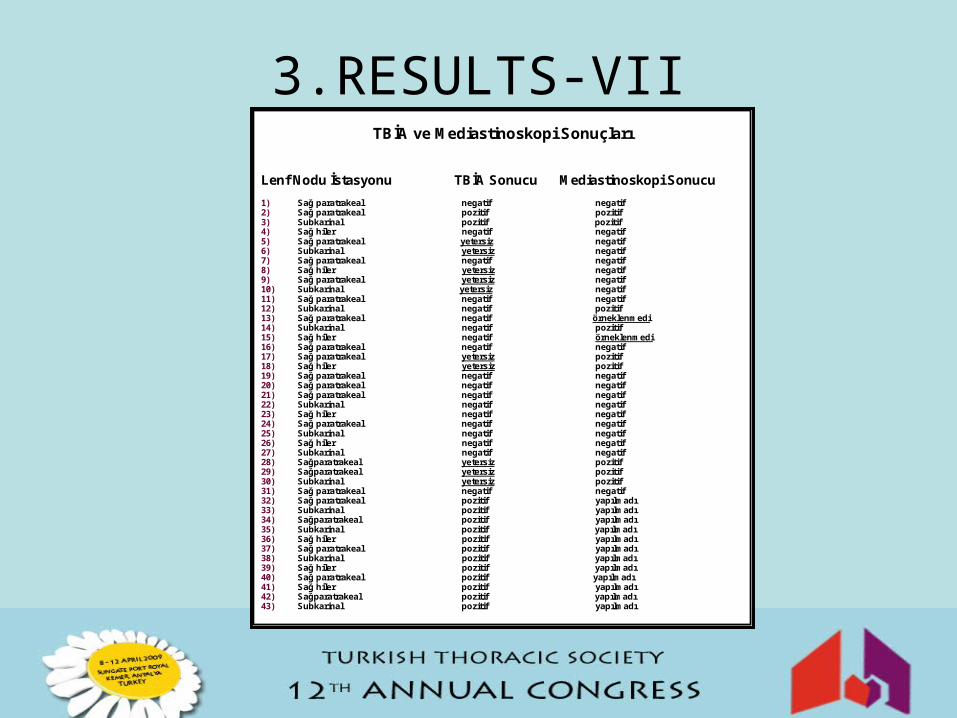
Lenf Nodu İstasyonu TBİA Sonucu Mediastinoskopi Sonucu
1) Sağ paratrakeal negatif negatif2) Sağ paratrakeal pozitif pozitif3) Subkarinal pozitif pozitif4) Sağ hiler negatif negatif5) Sağ paratrakeal yetersiz negatif6) Subkarinal yetersiz negatif7) Sağ paratrakeal negatif negatif8) Sağ hiler yetersiz negatif9) Sağ paratrakeal yetersiz negatif10) Subkarinal yetersiz negatif11) Sağ paratrakeal negatif negatif12) Subkarinal negatif pozitif13) Sağ paratrakeal negatif örneklenmedi14) Subkarinal negatif pozitif15) Sağ hiler negatif örneklenmedi16) Sağ paratrakeal negatif negatif 17) Sağ paratrakeal yetersiz pozitif18) Sağ hiler yetersiz pozitif19) Sağ paratrakeal negatif negatif20) Sağ paratrakeal negatif negatif21) Sağ paratrakeal negatif negatif22) Subkarinal negatif negatif23) Sağ hiler negatif negatif24) Sağ paratrakeal negatif negatif25) Subkarinal negatif negatif26) Sağ hiler negatif negatif27) Subkarinal negatif negatif28) Sağparatrakeal yetersiz pozitif 29) Sağparatrakeal yetersiz pozitif30) Subkarinal yetersiz pozitif31) Sağ paratrakeal negatif negatif 32) Sağ paratrakeal pozitif yapılmadı33) Subkarinal pozitif yapılmadı34) Sağparatrakeal pozitif yapılmadı35) Subkarinal pozitif yapılmadı36) Sağ hiler pozitif yapılmadı37) Sağ paratrakeal pozitif yapılmadı38) Subkarinal pozitif yapılmadı39) Sağ hiler pozitif yapılmadı40) Sağ paratrakeal pozitif yapılmadı41) Sağ hiler pozitif yapılmadı42) Sağparatrakeal pozitif yapılmadı43) Subkarinal pozitif yapılmadı
3.RESULTS-VIII
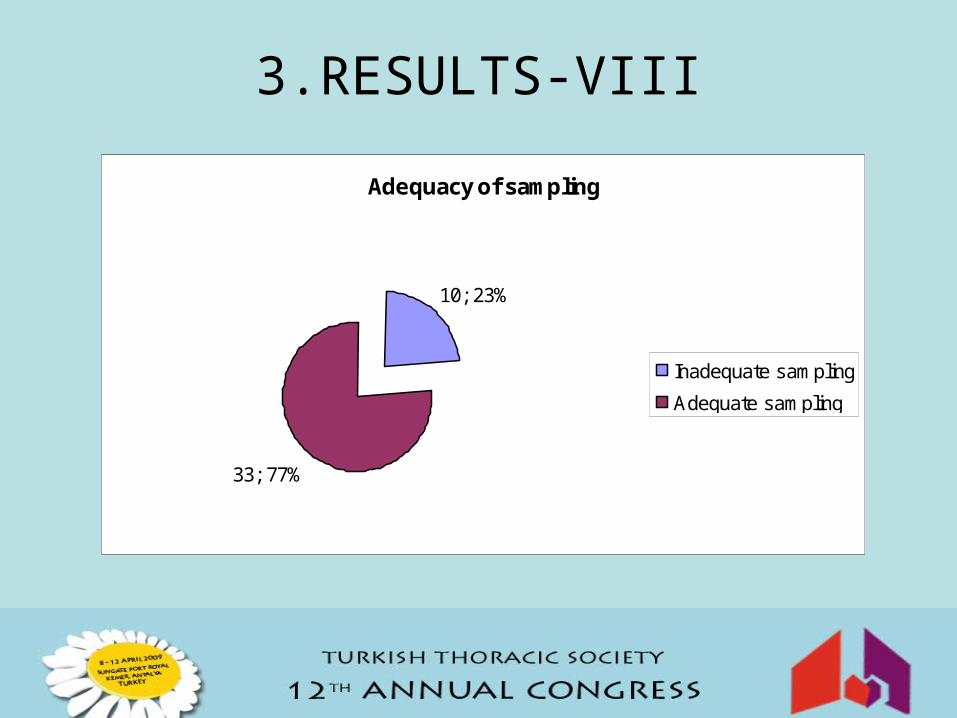
Adequacy of sampling
33; 77%
10; 23%
Inadequate sampling
Adequate sampling
3.RESULTS-IX
Results of Malignity ( positive or negative )
19; 58%
14; 42%Malignity positive
Malignity negative
3.RESULTS-X
Stations of lymph nodes with adequate sampling
15; 46%
10; 30%
8; 24%
Right paratracheal
Subcarinal
Right hilar
p > 0.05
3.RESULTS-XI
Stations of lymph nodes with malign results
6; 42%
4; 29%
4; 29%
Right paratracheal
Subcarinal
Right hilar
p > 0.05
3.RESULTS-XIIMediastinocopy
MalignMediastinoscopy Benign
TBNA Malign 14 0 14
TBNA Benign 2 17 19
Total 16 17 33
TBNA Sensitivity %87
TBİA Specificity %100
Positive predictive value %100
Negative predictive value %89
TBNA false positivity %0
TBNA false negativity %12
3.RESULTS-XIII
The clinical factors that might effect positive TBNA result Factor p
Lymph node location 0.18
LAP on CT 0.33
PET SUV Max ≥5 <0.05*
Broncoscopic properties ( precence of direct or indirect findings) 0.10
Adequate or inadequate TBNA sampling 0.09
Tumor tissue group 0.37
* The PET SUV max≥5 was 11 times increased positive TBNA results [OR=10.68 (1.91-59.62), P<0.01
3.RESULTS-XIV
The Procedures For Diagnosis
11; 44%
10; 40%
3; 12%1; 4%
Toracotomy
Broncus mucosa biopsy
TTNAB
TBB
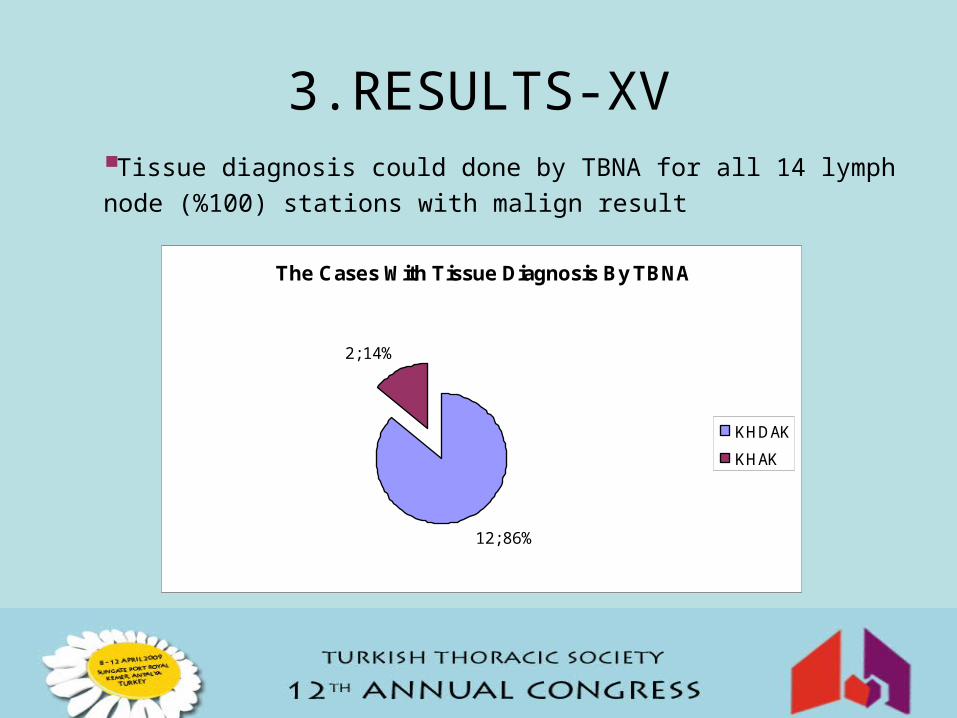
3.RESULTS-XVTissue diagnosis could done by TBNA for all 14 lymph node (%100) stations with malign result
The Cases With Tissue Diagnosis By TBNA
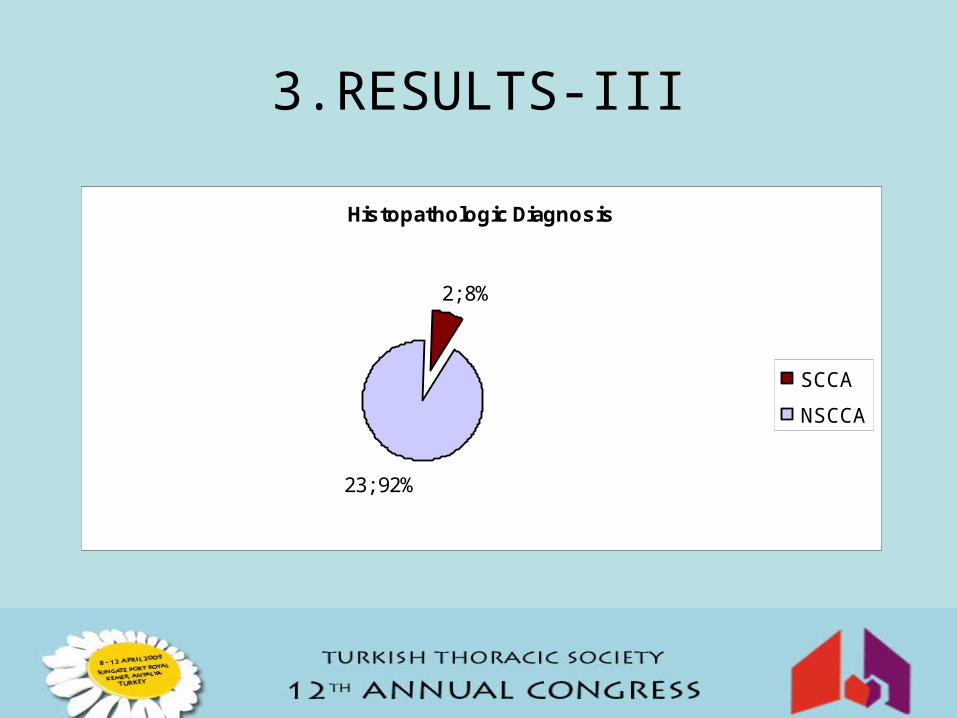
12; 86%
2; 14%
KHDAK
KHAK
3.RESULTS-XVI
The staging was completed with
TBNA in 5/19 (%26) patients without
mediastinoscopy.
The clinical nodal staging of patients before and after TBNA, and final surgical nodal staging after mediastinoscopy