28
Combining Art and Science in the Co-Creation of Value for Patients & Staff June 18, 2009 Susan Shaw, MS, RN Director, Clinical Operations Children’s Hospital Boston
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | shannon-jacobs |
| View: | 214 times |
| Download: | 1 times |

Combining Art and Science in the Co-Creation of Value for Patients & Staff
June 18, 2009
Susan Shaw, MS, RN
Director, Clinical Operations
Children’s Hospital Boston

2
• Primary pediatric teaching hospital of Harvard Medical School
• American Nurses Credentialing Center (ANCC) Magnet Recognition for nursing excellence
• 396-bed comprehensive center for pediatric health care
• One of the largest pediatric medical centers in the United States, offering a complete range of health care services for children from birth through 21 years of age
• Records approximately 22,600 inpatient admissions, and more than 527,500 outpatient visits annually in 204 specialized clinical programs
• Perform 23,000 surgical procedures and 170,000 radiological examinations every year
• 56,000 Emergency Department visits annually
Children’s Hospital Boston – Overview

3
Care and Service
While the technical competence of health care is well established and, at times, breathtaking in its accomplishments,
it is no longer enough to ensure that patients are satisfied, regardless of whether the missing element is called customer service, patient satisfaction, caring competence, beneficence, or good old-fashioned bedside manner. Taken together, these three facts point to the need for combining technical expertise with service excellence in health care to improve clinical care,
as well as the patients’ perception of that care.(Mayer & Cates, Service Excellence in Health Care, JAMA, June 2009)

4
Mission care research communityeducation
Justifiable Costs
Excellent Care
Clinical and
Research Innovatio
n
State-of-the-art
infrastructure
Innovative and
sustainable organizatio
n
Talent destination
Financial sustainabilit
y
Vision: Life Changing Care, World-Changing Research
Strategic Goals
Foundation For Success

5
Strategy Map

6
Definition of Value
Quality + Service + Innovation
Value = _____________________________________
Cost

7
New Definition of Patient Experience Emerging
Family Centered Care• Family centered care is a
philosophy that promotes the inclusion of the patient and family in the care decisions of the patient.
• Embraces the family as a care partner, with the goal of putting the needs of the family first.
Patient Experience• Strategic shift in focus from
operations to the customer • Has family centered care at its core,
but extends beyond a philosophy of care
• Focuses on viewing each encounter with the organization through the customer’s eyes
• Valuable approach when customer relationships are complex and involve multiple “touch points” or points of contact.
• Experience Mapping Not a process map, but an evaluation of initial patient/family expectations and experiences of the continuum of services provided.

8
Background
• Healthcare is characterized by complexity and fragmentation, with discrete silos of information controlled by separate entities. This frequently leaves patients with a sense of frustration as they negotiate the system (Gulati, 2007).
• A study recently completed at the University of Pittsburgh Medical Center (2007) found that 30 departments impact a single patient on the day that he/she undergoes surgery (World Health Congress, 2007).
• The integration of patient experience information (solicited and voluntary) is critical to bridging operational silos and providing a comprehensive approach to management of the patient experience (Russell & Otley, 2003).

9
Recent Analysis of CHB Patient Experience
• De-identified existing satisfaction data over a 2-year time period (August 1, 2006 through July 31, 2008) were examined to identify key satisfaction issues across survey results.
• Content analysis: the text is coded, or broken down, into manageable categories and examined using one of content analysis' basic methods: conceptual analysis or relational analysis.
• Conceptual analysis: examine presence of identified categories with respect to patient satisfaction

10
Major Themes
Environment of Care Accommodations, Infrastructure – includes staffing, availability of equipment, supplies/equipment failure, service delivery.
Quality of Care (Care and Treatment of patient) Care of patient during stay, Unsatisfactory treatment, Lack of support, Did not involve patient in decisions about care, IV starts/lab draws, Medication errors, Patient safety, Pain management
Communication Quality of information (inadequate explanations, conflicting information), inadequate instructions,, Unresponsiveness, Fragmentation of care
Respect and Caring (Staff Attitudes and Behaviors) Insensitivity, poor attitude, discounting patient/family opinions, unprofessional conduct, courtesy, ability of providers to work together
Timeliness Access, Availability, Scheduling, Delays in treatment, Delay in receiving reports or results, timeliness of admission and discharge processes
11
Complaint Data 2006-2008
12
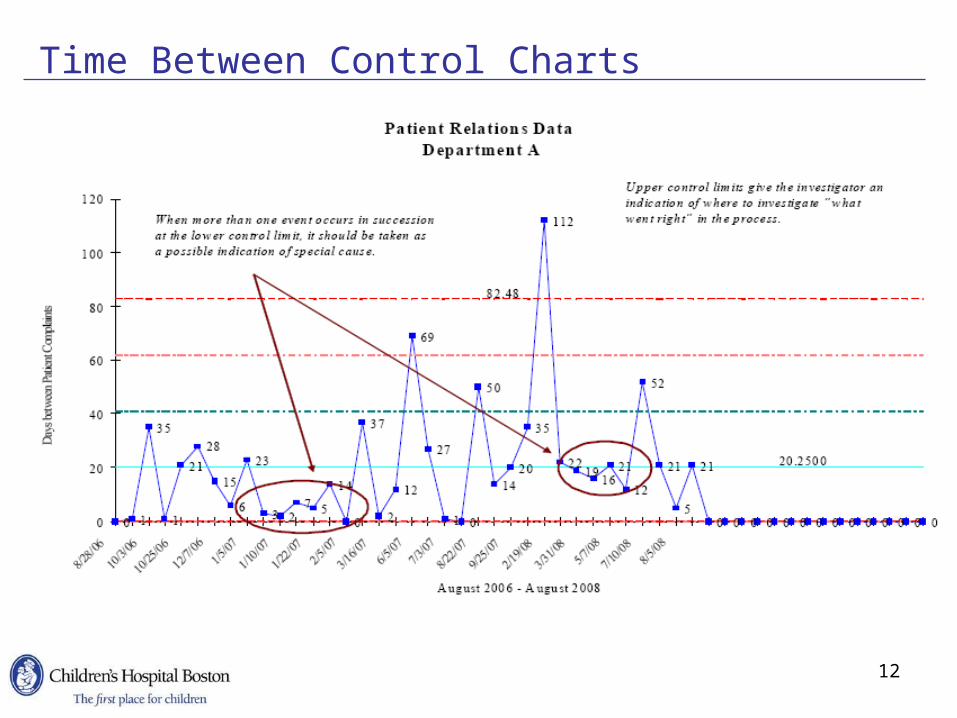
Time Between Control Charts

13
Example: Emergency Department (2004)
•Significant increase in patient complaints•Decrease in staff morale (MDs, RNs, AAs)•Increased patient waiting times•Increased “Left Without Being Seen” (LWBS)
Senior Leadership held local leaders accountable for improvements…development of ED Improvement
Plan

14
Elements of Improvement Plan
• Patient Satisfaction Survey• Increased efforts at “immediate bedding” lead to creative exam
room space (“pull system”)• Referring MD Oversight Committee: ED sub-group• Leader/Patient rounds• Left Without Being Seen• Service Excellence Program• Expanded post-discharge follow up calls• Clinical Operations Group established• Fast-track system developed and optimized• Registration process enhancements (pre-reg, bedside reg)• Increased awareness of and access to chain of command around
patient satisfaction• Student consultation

15
Significant Drivers of Service for Patients/Families
16
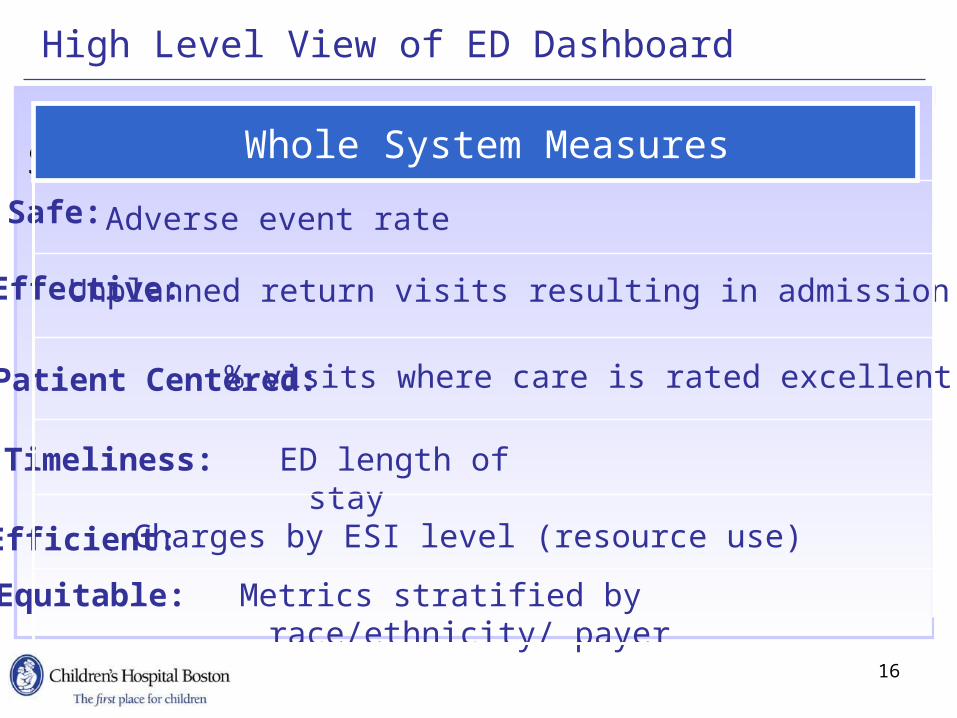
High Level View of ED Dashboard
Equitable: Metrics stratified by race/ethnicity/ payer
Effective:
Safe: Adverse event rate
Whole System
Efficient:
Timeliness: ED length of stay
Patient Centered:
Unplanned return visits resulting in admission
Safe Whole System Measures
% visits where care is rated excellent
Charges by ESI level (resource use)

17
The 3 C’s (Clear Concise Communication) CampaignTechniques to help families ask the appropriate questions to get the answers they need about their child's care
Goals• A collaborative improvement project that targets patient-centered
information management • Create a mechanism to support optimal parent-provider
communication• Analyze the parent comments• Measure the impact of the improvement effort on parents’
experiences with emergency care
Details• Patient-centeredness and parent-provider communication• Existing literature on efficacy for a parent-completed needs
assessment during ED care• Opportunity to use existing satisfaction survey to measure the
impact of an intervention

18

19
Specific Questions AskedTheme Example
Diagnosis What is wrong with his throat?
Does he have a pneumonia?
Does she have an infection?
Evaluation/Treatment Does she need surgery?
Will he need a cast?
Can I get an x-ray to make sure nothing is wrong?
Pain/Pain management What is causing her pain?
How can we stop this pain?
Medication Is she going to be on any medications?
Does she need a stronger med?
Can I give something to reduce the cough?
Anticipatory guidance What do we need to look out for?
How can we help her feel better?
What do we do when this occurs?
Theme Example
Diagnosis What is wrong with his throat?
Does he have a pneumonia?
Does she have an infection?
Evaluation/Treatment Does she need surgery?
Will he need a cast?
Can I get an x-ray to make sure nothing is wrong?
Pain/Pain management What is causing her pain?
How can we stop this pain?
Medication Is she going to be on any medications?
Does she need a stronger med?
Can I give something to reduce the cough?
Anticipatory guidance What do we need to look out for?
How can we help her feel better?
What do we do when this occurs?
Theme Example

20
Primary Outcomes for 3C Implementation
Summary measure of parent-provider communication• Did the doctor listen to what you said about your child? • Was everything done for your child that you think should
have been done?• Was your child’s problem explained to you in a way that you
could understand?• Did the doctor listen to what your child said?• Before leaving the ED, were you told signs to watch for? • Thinking about your involvement in care, would you have
liked more involvement in decisions regarding your child?• Did the doctor and nurse say different things?• Were there times that you needed help but did not get it?
Primary outcome for content analysis • Percentage of completed forms determined to have potential
value to a treating clinician

21
0
10
20
30
40
50
60
70
80
90
100Per
cent
Excellent Very Good
90%
88.33% 83.33%
93.3%
2005 2006 2008
90.37%
2007
87.97%
92.13%
85%
90%
2009
91.66% 90.83%89.17% 85.83%
ED Example – Patient Satisfaction Survey

22
Lessons Learned
• The 3C campaign had a measurable and positive impact on ED communication behaviors as reported by parents
- 0.028 points per day improvement- 2.8 points (95%CI 0.1, 5.5) per 100 days
• Successfully improved communication in the ED, even as workflow and clinicians were challenged by potentially disruptive technologies
• Potential value for ED clinicians in the information shared by parents on written needs and expectations form at the outset of pediatric ED care
• The potential value of information is consistent across varying levels of patient acuity and ED visit types
What was the reason for 3C success?
• The tool itself
• The multi-modal strategy of improvement
• The “modeling” of the behavior

23
Patient Experience InitiativesDevelopment of Patient Experience Committee, charged with:
• Defining care from the patient perspective• Understanding the survey tools currently in use system-wide to assess the
patient experience• Evaluating survey results• Assisting with the development of initiatives to improve the patient
experience• Providing regular reports of the patient experience survey results to senior
leadership
Ambulatory Survey• ECES• Service Recovery• “Extra Mile” Initiatives
Human Resources Partnership• Employee Satisfaction Survey• Employee Selection & Development• Employee Recognition

24
Extra Mile Initiatives
Service Improvement Initiative Adoption in the Ambulatory Areas:
• Team huddles/daily briefings
• Visit checklist, patient info, fact sheets
• Customer service communication, concierge, greeter
• Department communication
• Staff meetings, department orientations
• 3 C’s questionnaire (Clear, Concise, Communication)
• Rounding (management, team, provider)

25
Exceptional Care Exceptional Service (ECES)Our Commitment If there is one promise we all make here at Children's Hospital Boston, it's to serve. Each other. Our patients. Their families. Our community. And those who practice throughout the region and partner with us in care.
We are a family of 11,000 united by optimism, devotion and innovation. We pledge tofoster a culture of exceptional care and exceptional service that supports these standard
EXCELLENCE. We believe that expectations are meant to be exceeded
RESPECT. We treat others with empathy and compassion. We appreciate our differences COMMUNICATION. We speak honestly. We listen carefully. We respond thoughtfully and promptly
COURTESY. We are friendly, professional, welcoming and kind
ENTHUSIASM. We are upbeat and positive, and will go the extra mile
TEAMWORK. We work together. We rely on one another's support and trust

26
ECES Successes
Employee Experience• Employee survey – improvement in all ECES benchmarks (FY06-08)
- Added 2 new courtesy questions to benchmark in FY10• ECES Core Training at New Hire Orientation weekly• Standards & Values added to job description for new applicants as well as the
HR website
Patient Experience• Service Recovery Program developed and
rolled-out to all Ambulatory areas (May 2008-present)
- 18 areas currently participating
• Car Seat Carrier program developed and implemented (September 2008) in main lobby
- Carriers signed out on 176 occasions
- Also available in Waltham
• Ask me! Program
- 18% increase in participation from FY08 to FY09
- Informational brochure created
• Outpatient Satisfaction Survey Round Tables (FY07-09)
Staff Training & Management Support
• 8,100 staff trained to date (2007-2009)
• 8 Management Boosters developed (available on web site)
• 3 Additional ECES training modules developed and rolled-out (administered by HR L&D)
• Workshops/Focus groups in 7 different areas throughout the hospital (focusing on staff courtesy, teamwork, communication)
• Support Services, Patient Services, Satellites and Ambulatory areas
Other• ECES Strategy Team
• 30 members representing all areas of institution
• Ongoing organization-wide communication in Small Talk, Children’s News and ECES Website
• Support all departments implementing ECES initiatives/projects/recognition
Employee Recognition• ECES ‘Employee of the Month’ program (administered
by HR)• 21 employees recognized to date
• ‘Way to Shine!’ program in development (multidisciplinary team)
• Yearly Ask me! celebrations

27
CHB Patient Portal: IndivoHealth

28
There Is Still More Work To Do…
Next Challenge… How do we do it all?• Balance vision, strategies and goals• Integrate care, service AND innovation• Take the “magic” at the bedside or local
program and standardize it across the institution

















