37
Commensal Bacteria- The Good, The Bad and The Unknown Endeavors, Winter 2011

Commensal Bacteria- The Good, The Bad and The Unknown
Endeavors, Winter 2011
The Intestinal Microbiota and Colorectal Cancer
Temitope O. Keku, MSPH, PhD
ProfessorDivision of Gastroenterology and Hepatology
University of North Carolina, Chapel Hill

Background
Gut Bacteria- who is there?
Functional studies- what are they doing?
Summary and conclusions
http://www.the- scientist.com/article/display/15649/
Outline

Colorectal cancer (CRC)
•Accounts for approximately 8.5% of all cancer deaths globally, with ~1.4 million new cases annually.
•In 2010, the global economic burden was ~ $14.1 billion and is expected to increase to $17.4 billion by 2020.
http://globocan.iarc.frSiegel et al. 2014 CA Cancer J. Clin. 2014:64

Male Female
Estimated age-standardized incidence and mortality rates per 100,000 among women and men worldwide.
Colorectal cancer (CRC) incidence varies by geography

CRC: Fourth most common cancer and the second leading cause of cancer death in the
USA
American Cancer Society, 2013
Estimated New Cases
Estimated Deaths
Lung 228,190 159,480
Colorectal 142,820 50,830
Breast 234,580 40,030
Prostate 238,590 29,720
Americans have ~ 5.6% lifetime risk of being diagnosed with CRC

Colorectal cancer is multifactorial
• Colorectal cancer is multistep process involving accumulation of genetic alterations and transformation of normal cells. • Adenomas are intermediate precursors.
Loss ofAPC
Mutationof K-ras
Deletion of 18q
Loss ofp53
Normal epithelium
Proliferation Intermediateadenoma
Early adenoma
(ACF)
Lateadenoma
Carcinoma
ENVIRONMENT
Gut Microbiome

Most bacteria reside in the intestinal communities (gut microbiota)
Stomach 0-102
Colon 1011
Distal Ileum 107-108
Duodenum 102
Jejunum 102
Proximal Ileum 103

Functions of the Gut Microbiota
Protective
Structural Metabolic
Commensal Gut Bacteria
Nutrient absorptionVitamin K, Folate, Biotin,Mg2+, Ca2+, SCFA
Development of Immune system
Protection against Pathogens, Homeostasis

Gut Microbiota are not innocent bystanders. They play a role in various diseases
•Necrotizing enterocolitis (NEC)
• Inflammatory Bowel Diseases (IBD)
•Ulcerative Colitis & Crohn’s Disease
•Colitis-associated cancer
•Colorectal cancer
• Stomach cancer
• Irritable bowel syndrome
• Infectious diarrheas
•Obesity & obesity-associated diseases
• Type I and Type II diabetes
•Asthma & other allergic diseases
•Autism
•Depression

Knock out Mouse
Inflammation Bacteria Incidence of Carcinoma
(Colon/Rectum)
Reference
Conventional Germ-free
IL-10 KO √ E. feacalis 60% 0 Berg et al. 1996
Rag2 KO
Rag2/Tgf1 DKO
√ H. hepaticus 100% 0 Erdman et al. 2003
TCR/P53 DKO √ Normal flora 70% 0 Kado et al. 2001
GPx1/GPx2 DKO
√ Normal flora-Helicobactersp.
28% 0 Chu et al. 2004
KO, knockout; DKO, double knockout; GPx, glutathione peroxidase; TCR, T cell receptor;
Evidence from animal models of inflammation support gut bacteria and CRC association

Gut Bacteria: Who is there?

16S ribosomal RNA gene (rRNA)
• Many members of the gut microbiota are not able to be cultured.
• Universal gene in bacteria – polymorphisms,
makes it reliable for inferring phylogenetic
relationships and characterizing microbial
community composition.
V1 V2 V3 V4 V6V5 V7 V8 V9
Conserved Regions
Variable Regions
16S ribosomal RNA (rRNA) Gene

Maximum likelihood tree generated from the top 371 OTUs using RaxXML EPA server (http://i12k-
exelixis3.informatik.tu-muenchen.de/raxml ). Branches are colored based on Phylum level assignments. Red colored
branches represent OTUs significantly different between cases and controls within each Phylum (at 10% FDR).
•Case: 87 taxa more abundant
•Control: 5 taxa more abundant
ISME J. 2012 Oct;6(10):1858-68

**T-tests on log-normalized abundances of genera in cases vs. controls Only top 11 taxa based
on p-values showing significant differences between cases and controls.
Bacterial Genus Direction in cases RankB-H corrected
p-value**Helicobacter UP 1 0.005Acidovorax UP 2 0.005Lactobacillus UP 3 0.008Cloacibacterium UP 4 0.006Lactococcus UP 5 0.005Stenotrophomonas UP 6 0.007Turicibacter UP 7 0.011Weissella UP 8 0.009Delftia UP 9 0.011
Acinetobacter UP 10 0.011
Streptococcus DOWN 11 0.04
Differences in bacterial abundance between cases and controls
Sanapareddy et al. 2012, ISME J. 6:1858-68

Specific bacteria are associated with the mucosal layer
57-58-comb
A
D E
x200
x400 x1800
G- ProteobacteriaFaecalibacterium
Ruminococcus Lactobacillus
Clostridia
x1800
x400
x400
x400
x400
x400
x400
B C
D E F
G H
Fluorescent in-situ hybridization analysis
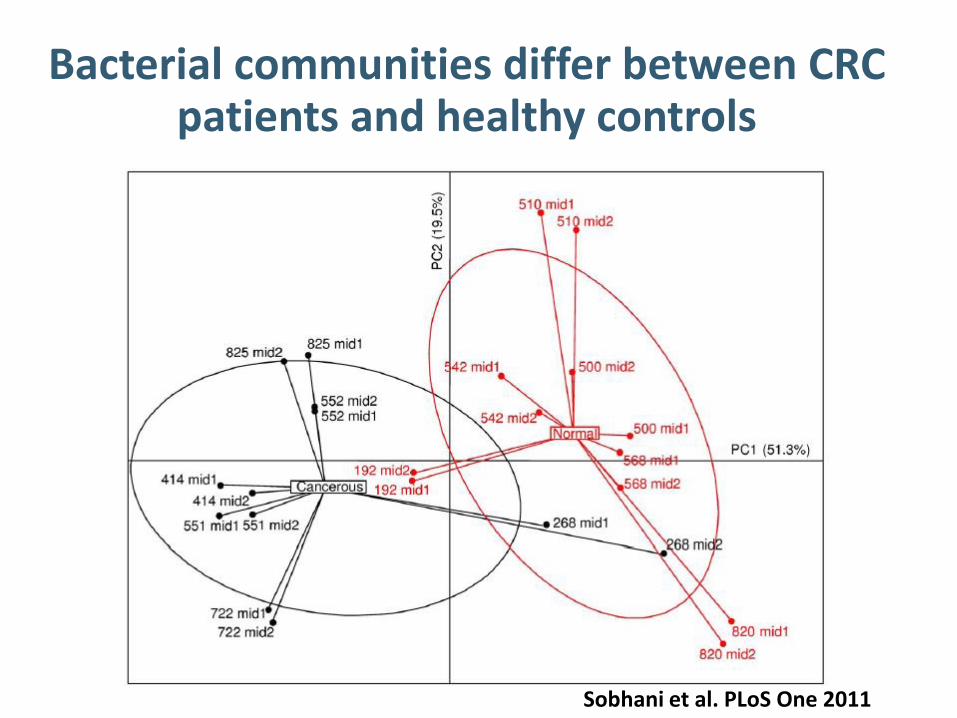
Bacterial communities differ between CRC patients and healthy controls
Sobhani et al. PLoS One 2011

Bacteroides/Prevotella overabundance in CRC than controls
Sobhani et al. PLoS One 2011
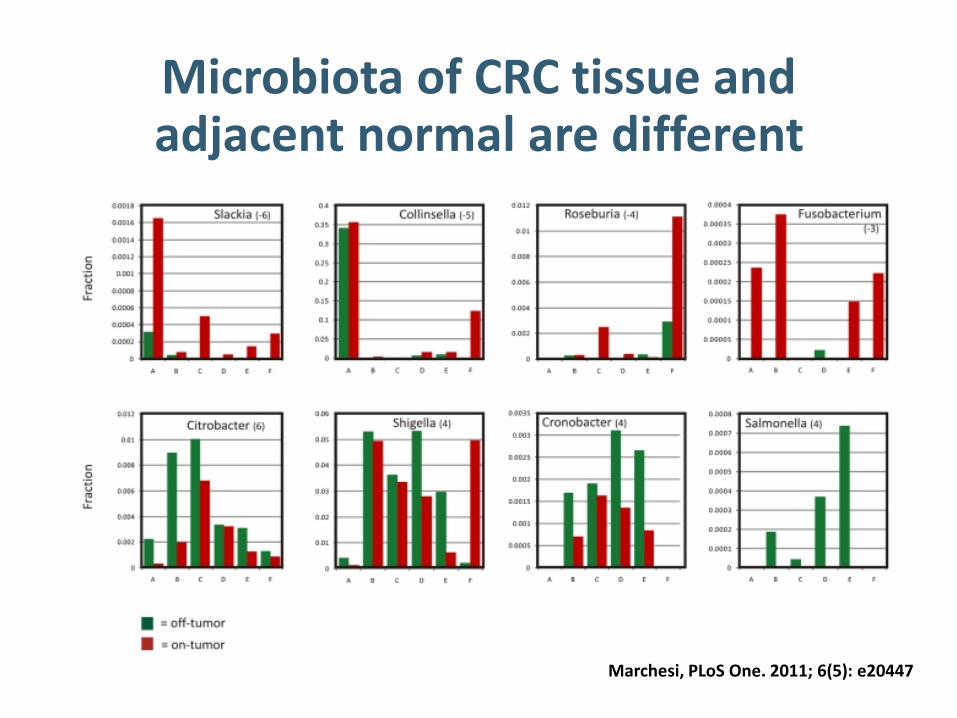
Microbiota of CRC tissue and adjacent normal are different
Marchesi, PLoS One. 2011; 6(5): e20447

Genome Res. 2011 Oct 18.
Genomic analysis identifies association of Fusobacterium with colorectal carcinoma.Kostic et al. Genome Res. 2011 Oct 18
Bacterial signatures of colorectal adenomas and cancer
Abundance of Fusobacterium in rectal mucosal biopsies from adenoma cases and non-adenoma controls. McCoy et al. 2013, PLoS One
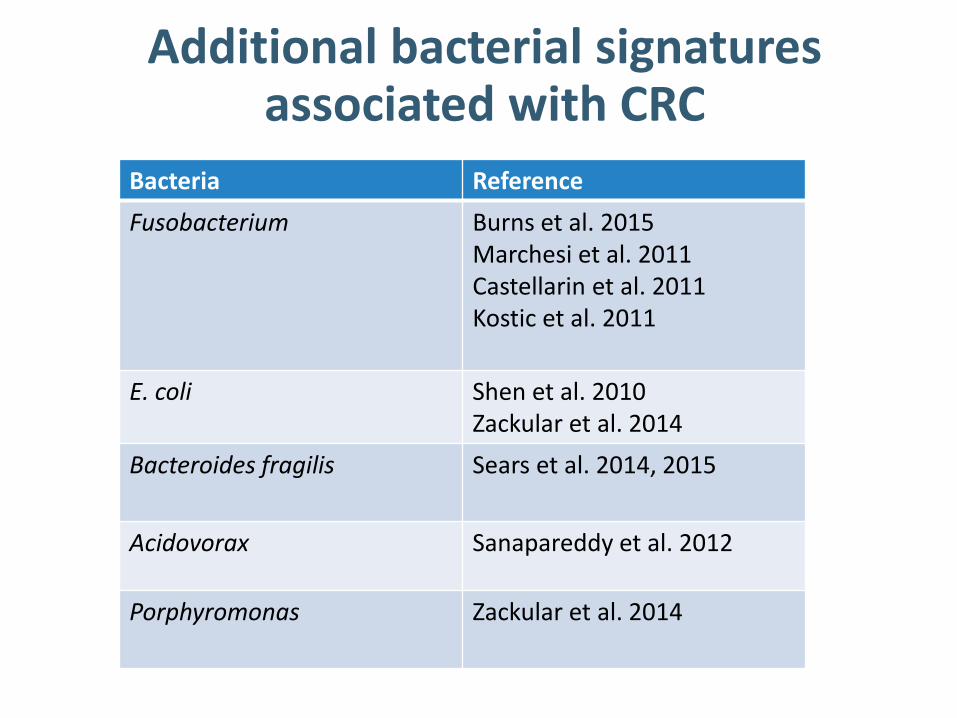
Additional bacterial signatures associated with CRC
Bacteria Reference
Fusobacterium Burns et al. 2015Marchesi et al. 2011Castellarin et al. 2011Kostic et al. 2011
E. coli Shen et al. 2010Zackular et al. 2014
Bacteroides fragilis Sears et al. 2014, 2015
Acidovorax Sanapareddy et al. 2012
Porphyromonas Zackular et al. 2014

Summary
•Changes in gut bacteria community profiles (dysbiosis) are associated with colorectal adenomas and cancer.
•Few bacterial signatures.

Gut Bacteria: What are they doing?

The Metabolome
•Metabolome: group of metabolites produced during metabolic processes.
•Human metabolome consists of metabolites from human cells and microbial cells.
• Changes in the metabolome have recently been associated with many diseases.
» Inflammatory Bowel Disease
» CRC
• Limited studies on microbiota, metabolome and adenomas/CRC.
KEGG Reference Pathway: Metabolic Pathways
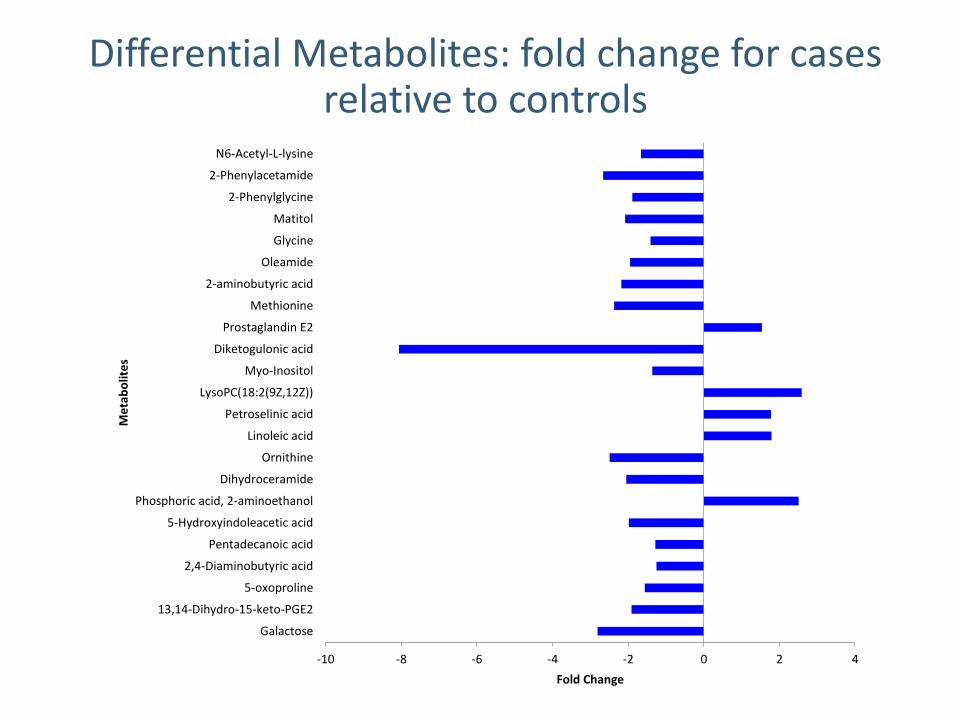
-10 -8 -6 -4 -2 0 2 4
Galactose
13,14-Dihydro-15-keto-PGE2
5-oxoproline
2,4-Diaminobutyric acid
Pentadecanoic acid
5-Hydroxyindoleacetic acid
Phosphoric acid, 2-aminoethanol
Dihydroceramide
Ornithine
Linoleic acid
Petroselinic acid
LysoPC(18:2(9Z,12Z))
Myo-Inositol
Diketogulonic acid
Prostaglandin E2
Methionine
2-aminobutyric acid
Oleamide
Glycine
Matitol
2-Phenylglycine
2-Phenylacetamide
N6-Acetyl-L-lysine
Fold Change
Me
tab
olit
es
Differential Metabolites: fold change for cases relative to controls

Diketogulonic acid
•Most biologically active metabolite of ascorbic acid (vitamin C)
•Vitamin C•Antioxidant - protects cells against oxidative stress from reactive
oxygen species.•Not synthesized by human cells•Obtained from the diet• Typically metabolized by bacteria in the GI tract.
• Low vitamin C -associated with oxidative stress and as such reduced levels of diketogulonic acid may be linked with increased oxidative stress.
• This is a potential link between the microbiome, metabolome, and pathogenesis of adenomas and CRC

Correlation between metabolites bacteria differ for cases and controls

Metabolome Summary •The metabolome is altered in
normal mucosa of patients with adenomas.
•Metabolome and microbiota are differentially correlated in the mucosa of adenoma patients compared to controls.
•Bacterial dysbiosis and altered metabolome may contribute to adenoma and CRC development.

• To develop bacterial signatures that could distinguish individuals with healthy colons from those with either colorectal adenomas or cancer
• To develop bacterial biomarkers or targets for screening and intervention
• Then we need……..
If the long term goal is…

IL10 −/− 129S6/SvEv 8 GF mice (Exp.)
&
129S6/SvEv GF 6 mice (Wild type)Bacteria
Cocktail ‘’pathogenic’ bacteria
OR
Cocktail ‘beneficial’ bacteria
Week 0 2 4 6 8 9
Fecal collection
Quantify bacteria
16S rRNA PCR/qPCR
1. Assess colon for tumors
2. Histology/Inflammation
3. Inflammation (Gene expression):
4. Quantification of bacteria via collection of
fecal/tissue samples
Gavaging ~109 poly-association of 5 bacteria/mouse
05/14 05/29 06/1207/17
Animal Experiments
06/27
National Gnotobiotic Rodent Resource Center, UNC, Chapel Hill
Sacrifice
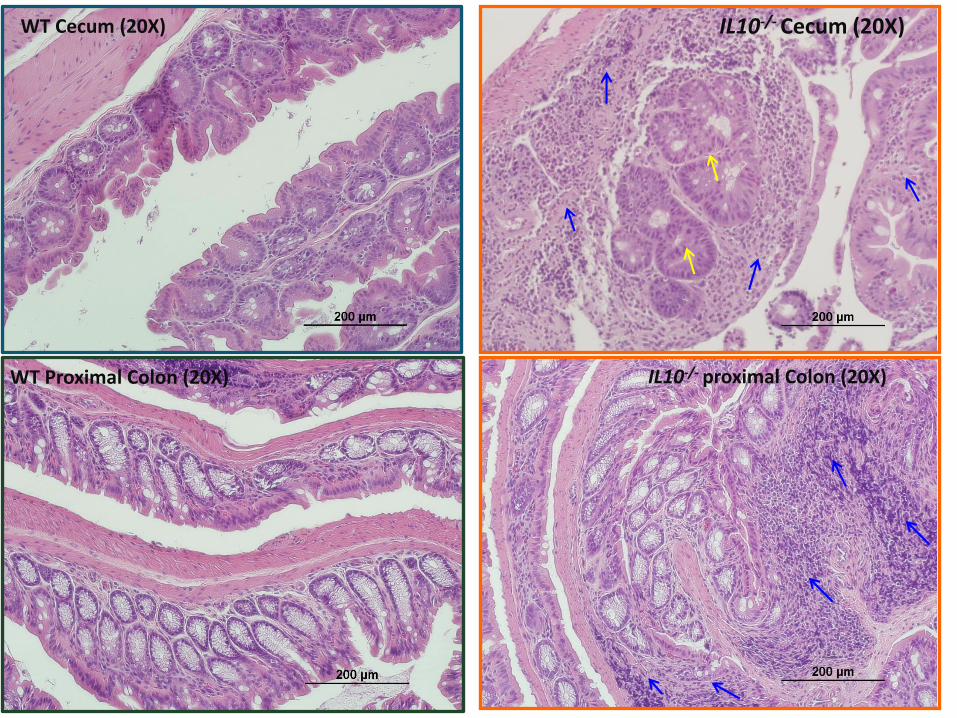
WT Cecum (20X) IL10-/- Cecum (20X)
IL10-/- proximal Colon (20X)WT Proximal Colon (20X)

• Microbial dysbiosis and metabolome may contribute to the development of adenomas and colorectal cancer. (correlation studies)
• Mechanistic studies in animal models are needed.
Summary
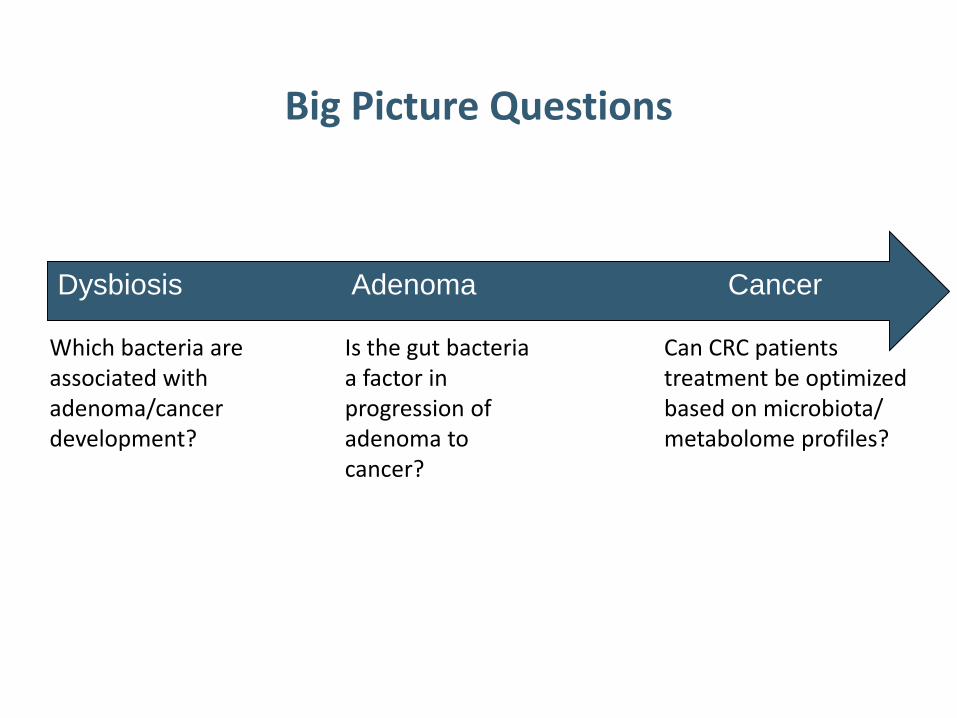
Big Picture Questions
Dysbiosis Adenoma Cancer
Which bacteria are associated with adenoma/cancer development?
Is the gut bacteria a factor in progression of adenoma to cancer?
Can CRC patients treatment be optimized based on microbiota/metabolome profiles?

A Shift Towards Personalized Medicine
Current Medicine
• Reactive Treatment
• One size fits all
• Population-based
Personalized Medicine
• Preventative
• Targeted
• Customized
One Treatment
Treatment A
Treatment B
Treatment C
AcknowledgementsCollaboratorsKeku Lab
• DHS Study Participants
Carolyn SuittDylan PageKayla Ebner
Funding Sources: NIH P30 DK034987, NIH K01 CA093654, NIH P50 CA106991 and NIH R01 CA136887
Histology Core













![Sua MaestaLM 2parte Amarri.ppt [modalità compatibilità] · placental tissue and amniotic fluid with the commensal bacteria from the mother. I nfluence of maternal health conditions](https://static.documents.pub/doc/80x56/5eca59fbc38f4e40c93ea43f/sua-maestalm-2parte-modalit-compatibilit-placental-tissue-and-amniotic-fluid.jpg)




