1
© 2010 Regents of the University of Minnesota. All rights reserved.
Common Orthopaedic
Conditions of the Spine
Robert Morgan, M.D, FACS
Department of Orthopaedic Surgery
© 2010 Regents of the University of Minnesota. All rights reserved.
Disclosures
I am not Rick Davis
Vinko Zlomislic UCSD loaned me
some slides
Putting all this into one hour is hard…
© 2010 Regents of the University of Minnesota. All rights reserved.
Objectives
• Demonstrate an
understanding of the most
common spinal problems
and their presentations
• Interpret the patient’s
history, physical
examination and
radiographs
• Establish accurate
diagnoses
2
2
© 2010 Regents of the University of Minnesota. All rights reserved.
Common Orthopaedic Conditions of the
Adult Spine
• Arthritis
• Trauma
• Deformity
• Infection
• Malignancy
• Biopsy
• Debridement
• Reduction
• Stabilization
• Decompression
Pain Surgery
© 2010 Regents of the University of Minnesota. All rights reserved.
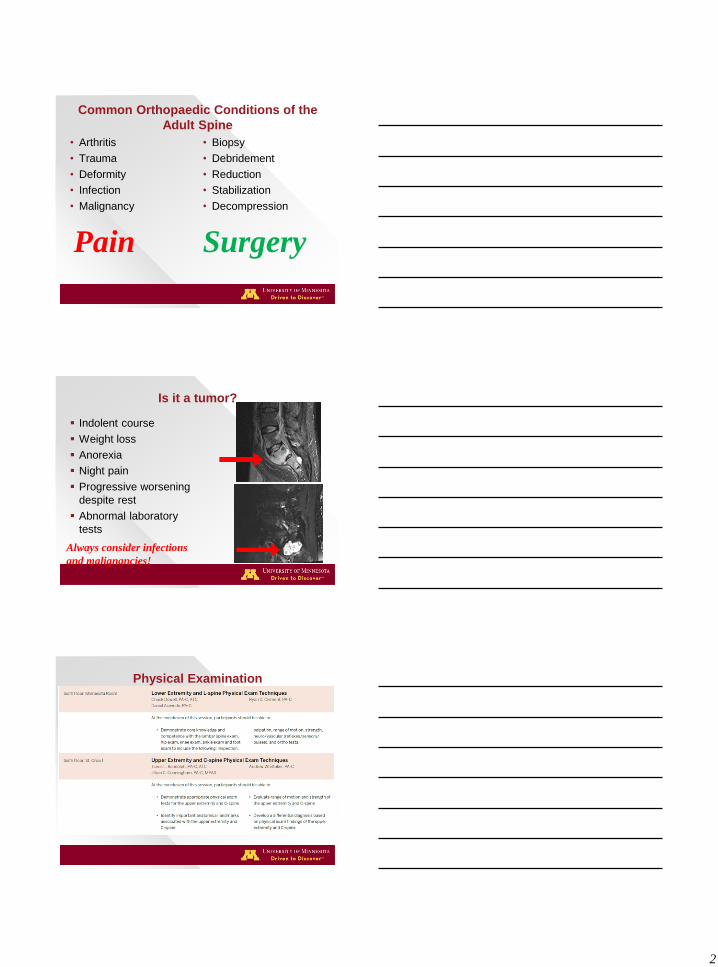
Is it a tumor?
Indolent course
Weight loss
Anorexia
Night pain
Progressive worsening
despite rest
Abnormal laboratory
tests
Always consider infections
and malignancies!
© 2010 Regents of the University of Minnesota. All rights reserved.
Physical Examination
3
© 2010 Regents of the University of Minnesota. All rights reserved.
Joe Lunchbox!
Mid-40’s
Married, couple
of kids
Occasional cigar
Works 40 hours a
week “on the
line”
What is his likelihood of developing low back pain?
What is the impact of debilitating low back pain on society?
© 2010 Regents of the University of Minnesota. All rights reserved.
BACKGROUND
Epidemiology1
• 25% incidence of LBP in US
• 80% of back pain patients seek primary care
United States Healthcare Expenditures Rising
• Over $100 billion annually
–13% pharmacy
–13% primary care
–17% therapy
–17% inpatient services
1. Deyo et al, Annual Review of Public Health
(1991)
2. Dagenais et al, Spine (2008)
© 2010 Regents of the University of Minnesota. All rights reserved.
Healthy Disk-Structure
Nucleus pulposus
• Notochord cells
–proteoglycan
Anulus fibrosus
• Fibrocytes
–collagen
Vertebral endplate
• Chondrocytes
–cartilage
4
© 2010 Regents of the University of Minnesota. All rights reserved.
Healthy Disk-Function
Nucleus pulposus
• Hydrostatic column
Anulus fibrosus
• Restrains
deformation of
nucleus
Vertebral endplate
• transmits
compressive load
© 2010 Regents of the University of Minnesota. All rights reserved.
Healthy Disk-Care and feeding
Nucleus pulposus
• Avascular, aneural
Anulus fibrosus
• Vascular, innervated
Vertebral endplate
• Avascular,
innervated
© 2010 Regents of the University of Minnesota. All rights reserved.
Healthy Disk in Action
Resting supine
• 0.1-0.2 Mpa (1-2 atm)
Standing
• 1 MPa
Bending and Lifting
• 2.5 MPa
5 MPa induces chondrocyte apoptosis!
5
© 2010 Regents of the University of Minnesota. All rights reserved.
Why would a healthy disk fail?
Injury
• Direct trauma
–Accidental
– iatrogenic
• Postural
–Acquired
–Congenital
–Obesity?
Illness
• Inflammatory
arthritis
• Infection
• Vascular disease
–Tobacco?
© 2010 Regents of the University of Minnesota. All rights reserved.
What does it mean for a disk to fail?
No longer able to
transmit load
Nucleus pulposus no
longer avascular
© 2010 Regents of the University of Minnesota. All rights reserved.
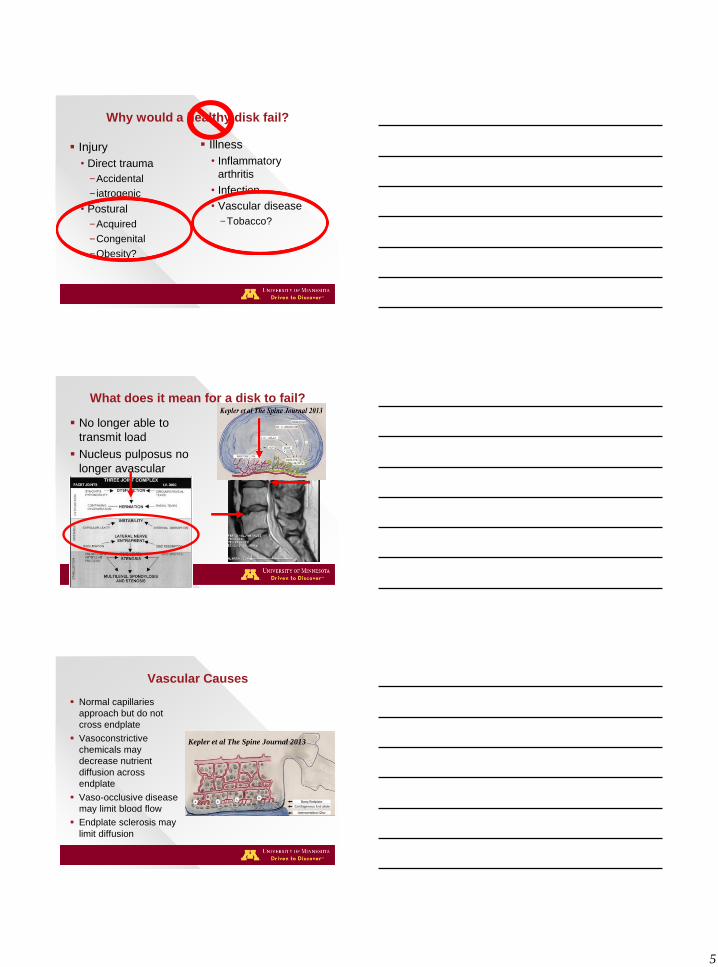
Vascular Causes
Normal capillaries
approach but do not
cross endplate
Vasoconstrictive
chemicals may
decrease nutrient
diffusion across
endplate
Vaso-occlusive disease
may limit blood flow
Endplate sclerosis may
limit diffusion
Kepler et al The Spine Journal 2013
6
© 2010 Regents of the University of Minnesota. All rights reserved.
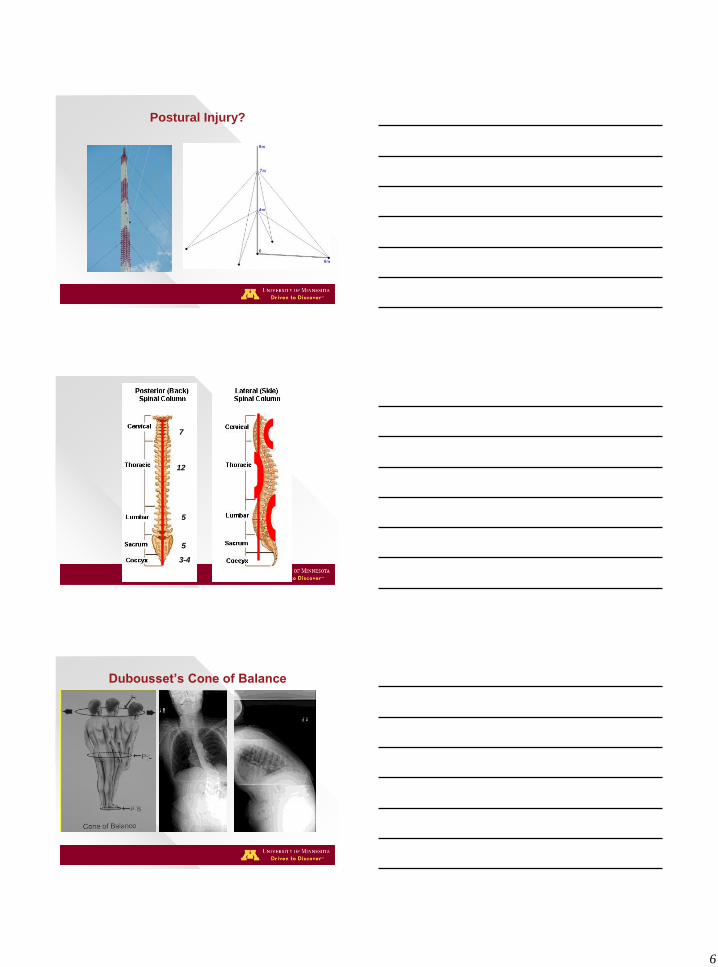
Postural Injury?
© 2010 Regents of the University of Minnesota. All rights reserved.
7
12
5
5
3-4
© 2010 Regents of the University of Minnesota. All rights reserved.
Dubousset’s Cone of Balance
7
© 2010 Regents of the University of Minnesota. All rights reserved.
© 2010 Regents of the University of Minnesota. All rights reserved.
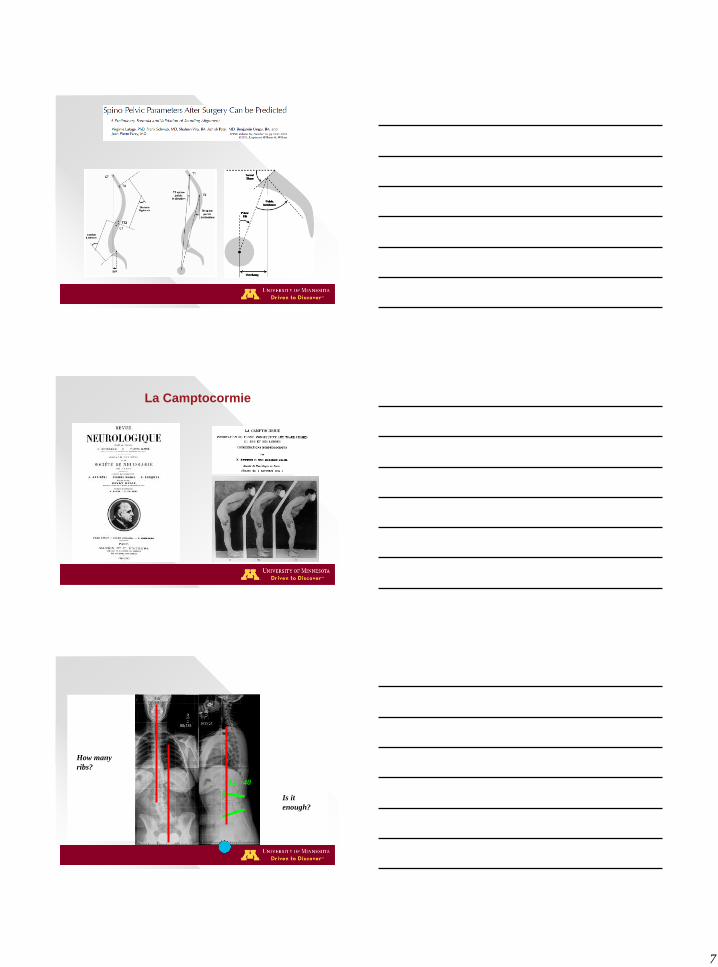
La Camptocormie
© 2010 Regents of the University of Minnesota. All rights reserved.
How many
ribs?
LL=40
Is it
enough?
8
© 2010 Regents of the University of Minnesota. All rights reserved.
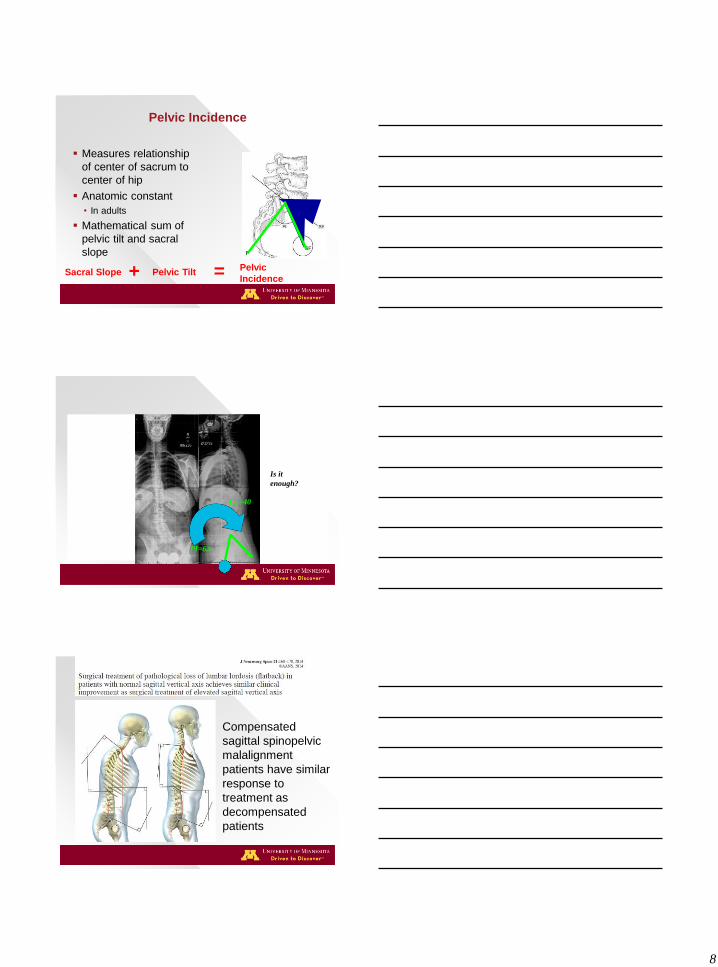
Pelvic Incidence
Measures relationship
of center of sacrum to
center of hip
Anatomic constant
• In adults
Mathematical sum of
pelvic tilt and sacral
slope
Pelvic
Incidence Pelvic Tilt = Sacral Slope +
© 2010 Regents of the University of Minnesota. All rights reserved.
LL=40
Is it
enough?
PI=62
© 2010 Regents of the University of Minnesota. All rights reserved.
Compensated
sagittal spinopelvic
malalignment
patients have similar
response to
treatment as
decompensated
patients
9
© 2010 Regents of the University of Minnesota. All rights reserved.
Spondylolisqesis
I: Dysplastic
II: Isthmic
III: Degenerative
IV: Traumatic
V: Pathologic
1: 1- 25%
2: 26-50%
3: 51-75%
4: 76-100%
5: Greater than 100%
Type (Wiltse) Grade (Meyerding)
Also Marchetti and Bartolozzi
LO
W G
RA
DE
H
IGH
GR
AD
E
© 2010 Regents of the University of Minnesota. All rights reserved.
Anatomic Measurements
Lumbar Index
• Measure of wedging
• Low lumbar index correlates with high grade slips
Slip Angle
• Measure of kyphosis
• Line perpendicular to posterior vertebral body to line parallel to superior endplate
Posterior height
Anterior height =
© 2010 Regents of the University of Minnesota. All rights reserved.
Marchetti and Bartolozzi
High dysplastic • With lysis
• With elongation
Low dysplastic • With lysis
• With elongation
Traumatic • Acute fracture
• Stress fracture
Iatrogenic • Direct
• Indirect
Pathologic • Local
• Systemic
Degenerative • Primary
• secondary
Developmental Acquired
10
© 2010 Regents of the University of Minnesota. All rights reserved.
Stability
“Clinical instability is defined as the loss of the
spine’s ability under physiologic loads to
maintain its patterns of displacement, so as to
avoid initial or additional neurologic deficits,
incapacitating deformity and intractable pain.”
White and Panjabi 1987
© 2010 Regents of the University of Minnesota. All rights reserved.
Upper Cervical Anatomy
Biomechanically Specialized
• Support of “large” Cranial mass
• Large range of motion
–Flexion/extension
–Axial rotation
Unique osteological characteristics
Unique vascular characteristics
© 2010 Regents of the University of Minnesota. All rights reserved.
Anatomy – The Axis
Important transition point for forces within the c-spine
Important anatomical points • Superior and inferior articular
processes are “offset” in the AP direction- due to different functions at each articulation
• Pars interarticularis- due to this transition is a frequent fracture site
• Odontoid process- the “pivot” for rotation
11
© 2010 Regents of the University of Minnesota. All rights reserved.
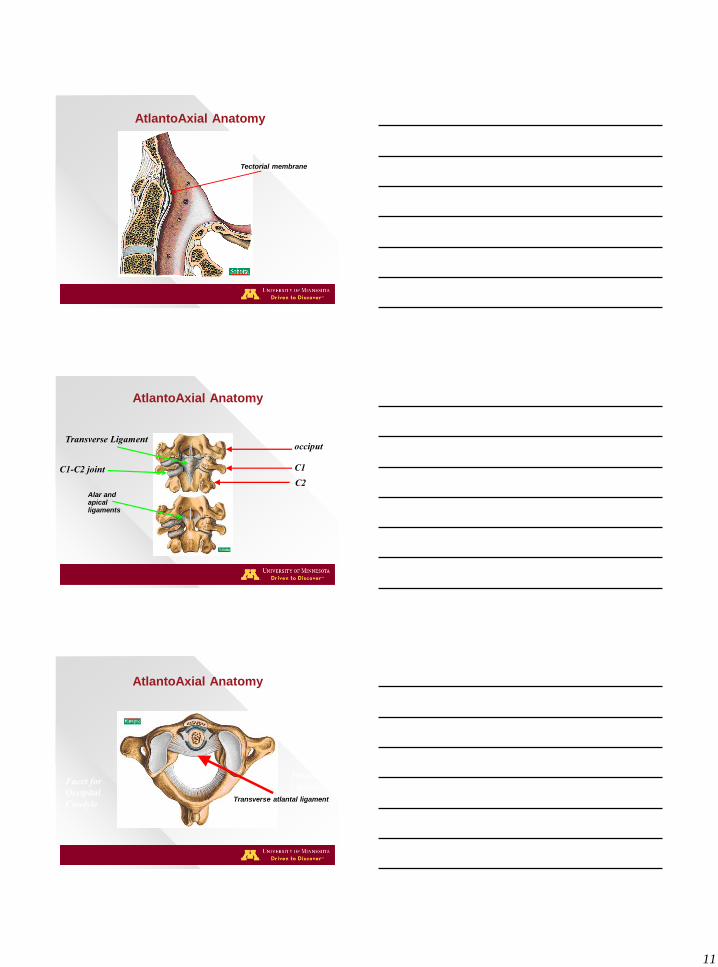
AtlantoAxial Anatomy
Tectorial Membrane Tectorial membrane
© 2010 Regents of the University of Minnesota. All rights reserved.
AtlantoAxial Anatomy
occiput
C1
C2
Transverse Ligament
C1-C2 joint
Alar and apical ligaments
© 2010 Regents of the University of Minnesota. All rights reserved.
AtlantoAxial Anatomy
Transverse
Ligament Facet for
Occipital
Condyle Transverse atlantal ligament
12
© 2010 Regents of the University of Minnesota. All rights reserved.
AtlantoAxial Anatomy
Vertebral
Artery
© 2010 Regents of the University of Minnesota. All rights reserved.
Odontoid Fractures
Most common fracture of Axis (nearly 2/3 of all C2 Fxs)
10 – 20 % of all cervical fractures
Etiology Bimodal distribution
Young - high energy, multi-trauma
Elderly - low energy, isolated injury
(most common C-spine Fx elderly)
© 2010 Regents of the University of Minnesota. All rights reserved.
Radiographic Evaluation
13
© 2010 Regents of the University of Minnesota. All rights reserved.
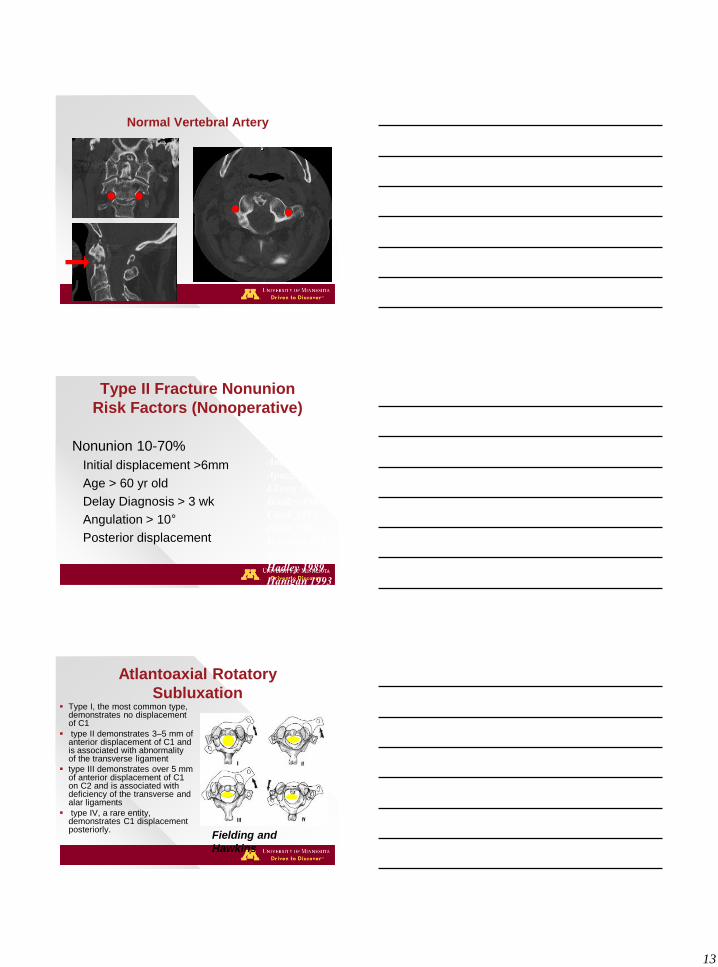
Normal Vertebral Artery
© 2010 Regents of the University of Minnesota. All rights reserved.
Type II Fracture Nonunion
Risk Factors (Nonoperative)
Nonunion 10-70%
Initial displacement >6mm
Age > 60 yr old
Delay Diagnosis > 3 wk
Angulation > 10°
Posterior displacement
Schatzker 1971
Anderson 1974
Apuzzo 1978
Ekong 1981
Hadley 1985
Clark 1985
Dunn 1986
Hanssen 1987
Schweigel 1987
Hadley 1989
Hanigan 1993
Ryan 1993
Seybold 1997
© 2010 Regents of the University of Minnesota. All rights reserved.
Atlantoaxial Rotatory
Subluxation Type I, the most common type,
demonstrates no displacement of C1
type II demonstrates 3–5 mm of anterior displacement of C1 and is associated with abnormality of the transverse ligament
type III demonstrates over 5 mm of anterior displacement of C1 on C2 and is associated with deficiency of the transverse and alar ligaments
type IV, a rare entity, demonstrates C1 displacement posteriorly.
Fielding and
Hawkins
14
© 2010 Regents of the University of Minnesota. All rights reserved.
Motion is life, life is motion
Stabilize in collar
• assess stability
Reduce in longitudinal traction
• Halo
Consider anterior fixation if favorable fracture
Definitive procedure is posterior stabilization
© 2010 Regents of the University of Minnesota. All rights reserved.
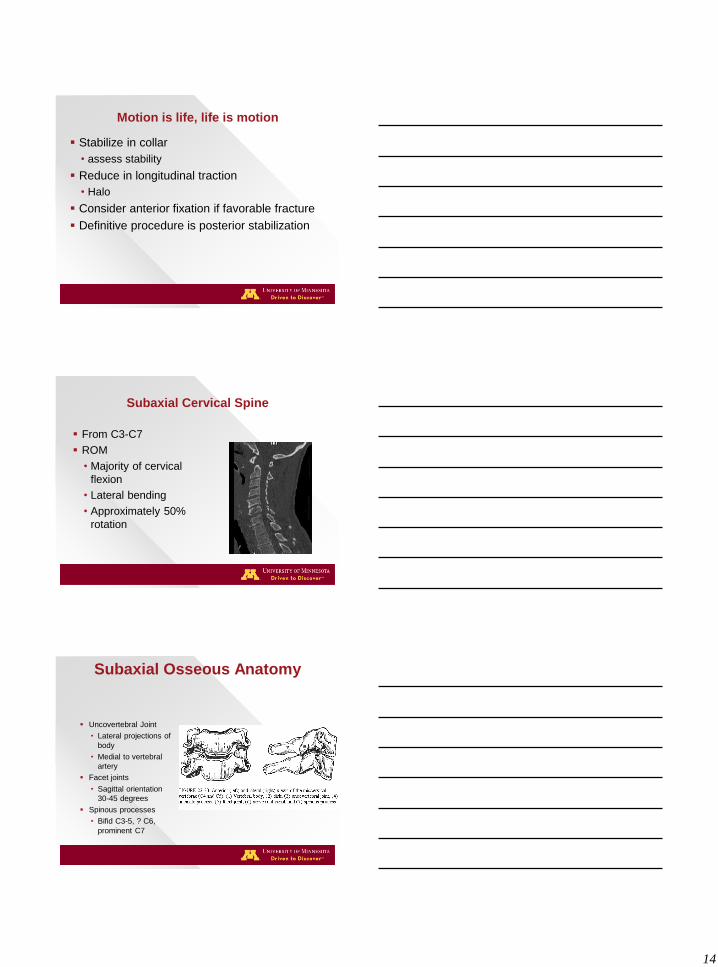
Subaxial Cervical Spine
From C3-C7
ROM
• Majority of cervical
flexion
• Lateral bending
• Approximately 50%
rotation
© 2010 Regents of the University of Minnesota. All rights reserved.
Subaxial Osseous Anatomy
Uncovertebral Joint
• Lateral projections of
body
• Medial to vertebral
artery
Facet joints
• Sagittal orientation
30-45 degrees
Spinous processes
• Bifid C3-5, ? C6,
prominent C7
15
© 2010 Regents of the University of Minnesota. All rights reserved.
Columns Holdsworth 2 column theory
• Anterior Column
–Body, disc, ALL, PLL
• Posterior Column
–Spinal canal, neural arch and posterior
ligaments
© 2010 Regents of the University of Minnesota. All rights reserved.
Initial Management Considerations
Manage the airway
Support spinal cord perfusion
pressure
Obtain appropriate imaging
Reduce dislocations
Remove spinal compression
Restore spinal stability
© 2010 Regents of the University of Minnesota. All rights reserved.
Obtain Appropriate Imaging
CT scan with sagittal and coronal reconstructions
• All cervical spine occiput-T1 (EAST2009)
• All thoracic and lumbar spine with fractures
MRI
• All neurologic deficit
• All patients undergoing operative intervention
• Clearance in obtunded, spondylotic patients
Radiographs
• Upright before discharge
16
© 2010 Regents of the University of Minnesota. All rights reserved.
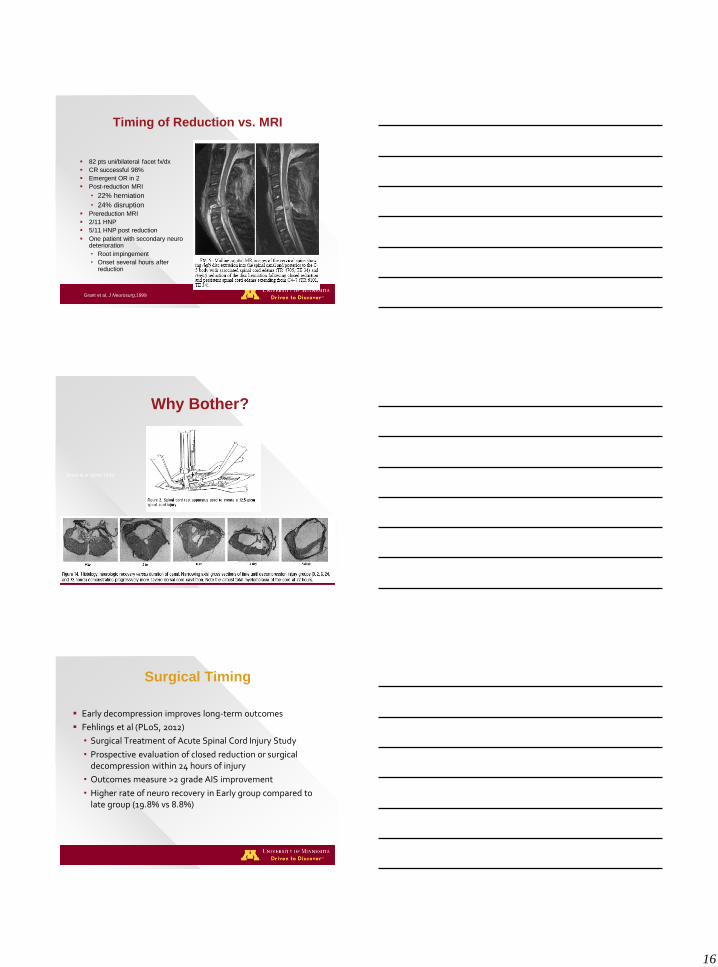
Timing of Reduction vs. MRI
82 pts uni/bilateral facet fx/dx
CR successful 98%
Emergent OR in 2
Post-reduction MRI
• 22% herniation
• 24% disruption
Prereduction MRI
2/11 HNP
5/11 HNP post reduction
One patient with secondary neuro deterioration
• Root impingement
• Onset several hours after reduction
Grant et al, J Neurosurg,1999
© 2010 Regents of the University of Minnesota. All rights reserved.
Why Bother?
Dimar et al Spine 1999
© 2010 Regents of the University of Minnesota. All rights reserved.
Surgical Timing
Early decompression improves long-term outcomes
Fehlings et al (PLoS, 2012)
• Surgical Treatment of Acute Spinal Cord Injury Study
• Prospective evaluation of closed reduction or surgical decompression within 24 hours of injury
• Outcomes measure >2 grade AIS improvement
• Higher rate of neuro recovery in Early group compared to late group (19.8% vs 8.8%)
17
© 2010 Regents of the University of Minnesota. All rights reserved.
AO/OTA Classification
Not specific for
cervical spine
Provides some
treatment guidelines
Type A
• Axial loading;
compression; stable
Type B
• Bending type injuries
Type C
• Circumferential injuries;
multi-axial
© 2010 Regents of the University of Minnesota. All rights reserved.
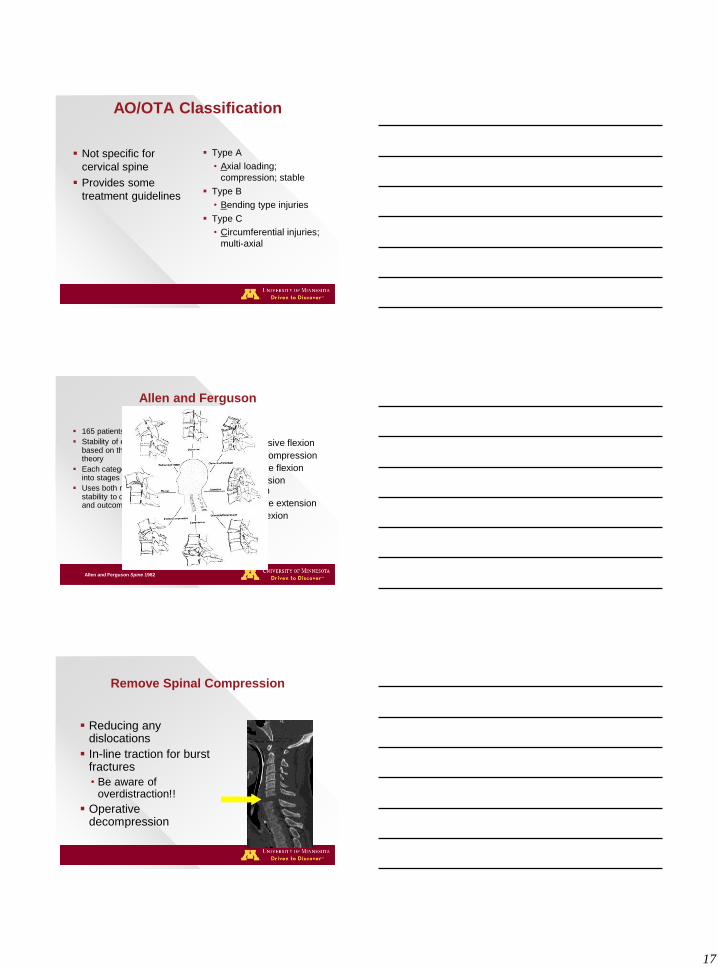
Allen and Ferguson
165 patients
Stability of each pattern is based on the two column theory
Each category is broken down into stages
Uses both mechanism and stability to determine treatment and outcome
• 6 categories
–Compressive flexion
–Vertical compression
–Distractive flexion
–Compression extension
–Distractive extension
–Lateral flexion
Allen and Ferguson Spine 1982
© 2010 Regents of the University of Minnesota. All rights reserved.
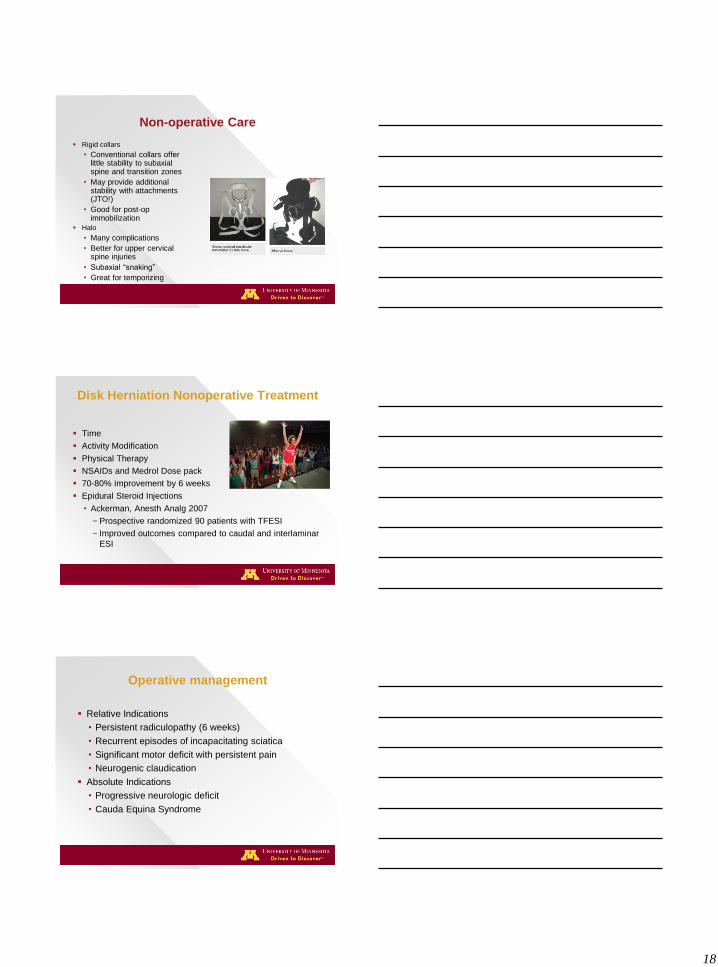
Remove Spinal Compression
Reducing any dislocations
In-line traction for burst fractures
• Be aware of overdistraction!!
Operative decompression
18
© 2010 Regents of the University of Minnesota. All rights reserved.
Non-operative Care
Rigid collars
• Conventional collars offer little stability to subaxial spine and transition zones
• May provide additional stability with attachments (JTO!)
• Good for post-op immobilization
Halo
• Many complications
• Better for upper cervical spine injuries
• Subaxial “snaking”
• Great for temporizing Spinal Orthoses. Steven S. Agabegi, MD, Ferhan A. Asghar, MD and Harry N. Herkowitz, MD J Am Acad
Orthop Surg,18,11, 657-667.
© 2010 Regents of the University of Minnesota. All rights reserved.
Disk Herniation Nonoperative Treatment
Time
Activity Modification
Physical Therapy
NSAIDs and Medrol Dose pack
70-80% improvement by 6 weeks
Epidural Steroid Injections
• Ackerman, Anesth Analg 2007
–Prospective randomized 90 patients with TFESI
– Improved outcomes compared to caudal and interlaminar
ESI
© 2010 Regents of the University of Minnesota. All rights reserved.
Operative management
Relative Indications
• Persistent radiculopathy (6 weeks)
• Recurrent episodes of incapacitating sciatica
• Significant motor deficit with persistent pain
• Neurogenic claudication
Absolute Indications
• Progressive neurologic deficit
• Cauda Equina Syndrome
19
© 2010 Regents of the University of Minnesota. All rights reserved.
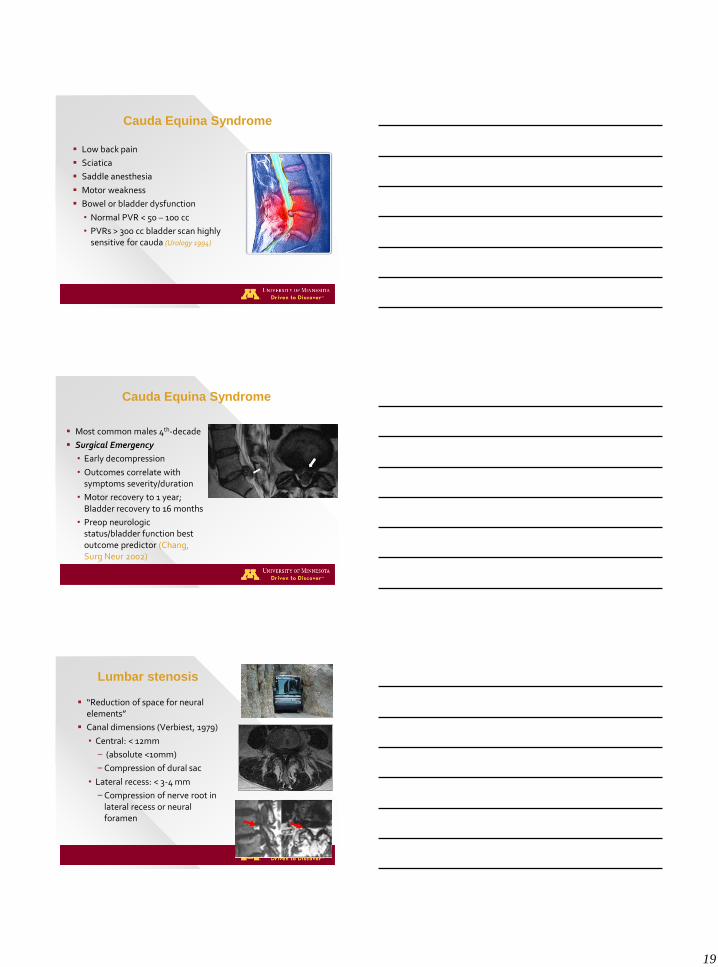
Cauda Equina Syndrome
Low back pain
Sciatica
Saddle anesthesia
Motor weakness
Bowel or bladder dysfunction
• Normal PVR < 50 – 100 cc
• PVRs > 300 cc bladder scan highly sensitive for cauda (Urology 1994)
© 2010 Regents of the University of Minnesota. All rights reserved.
Cauda Equina Syndrome
Most common males 4th-decade
Surgical Emergency
• Early decompression
• Outcomes correlate with symptoms severity/duration
• Motor recovery to 1 year; Bladder recovery to 16 months
• Preop neurologic status/bladder function best outcome predictor (Chang, Surg Neur 2002)
© 2010 Regents of the University of Minnesota. All rights reserved.
Lumbar stenosis
“Reduction of space for neural elements”
Canal dimensions (Verbiest, 1979)
• Central: < 12mm
– (absolute <10mm)
–Compression of dural sac
• Lateral recess: < 3-4 mm
–Compression of nerve root in lateral recess or neural foramen
20
© 2010 Regents of the University of Minnesota. All rights reserved.
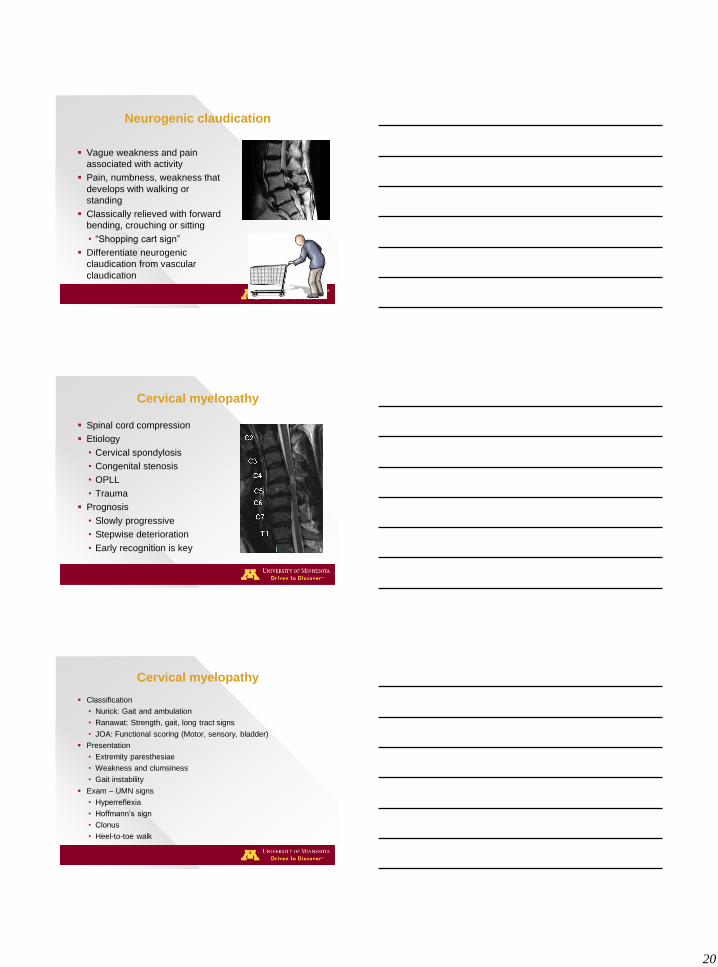
Neurogenic claudication
Vague weakness and pain
associated with activity
Pain, numbness, weakness that
develops with walking or
standing
Classically relieved with forward
bending, crouching or sitting
• “Shopping cart sign”
Differentiate neurogenic
claudication from vascular
claudication
© 2010 Regents of the University of Minnesota. All rights reserved.
Cervical myelopathy
Spinal cord compression
Etiology
• Cervical spondylosis
• Congenital stenosis
• OPLL
• Trauma
Prognosis
• Slowly progressive
• Stepwise deterioration
• Early recognition is key
© 2010 Regents of the University of Minnesota. All rights reserved.
Cervical myelopathy
Classification
• Nurick: Gait and ambulation
• Ranawat: Strength, gait, long tract signs
• JOA: Functional scoring (Motor, sensory, bladder)
Presentation
• Extremity paresthesiae
• Weakness and clumsiness
• Gait instability
Exam – UMN signs
• Hyperreflexia
• Hoffmann’s sign
• Clonus
• Heel-to-toe walk
21
© 2010 Regents of the University of Minnesota. All rights reserved.
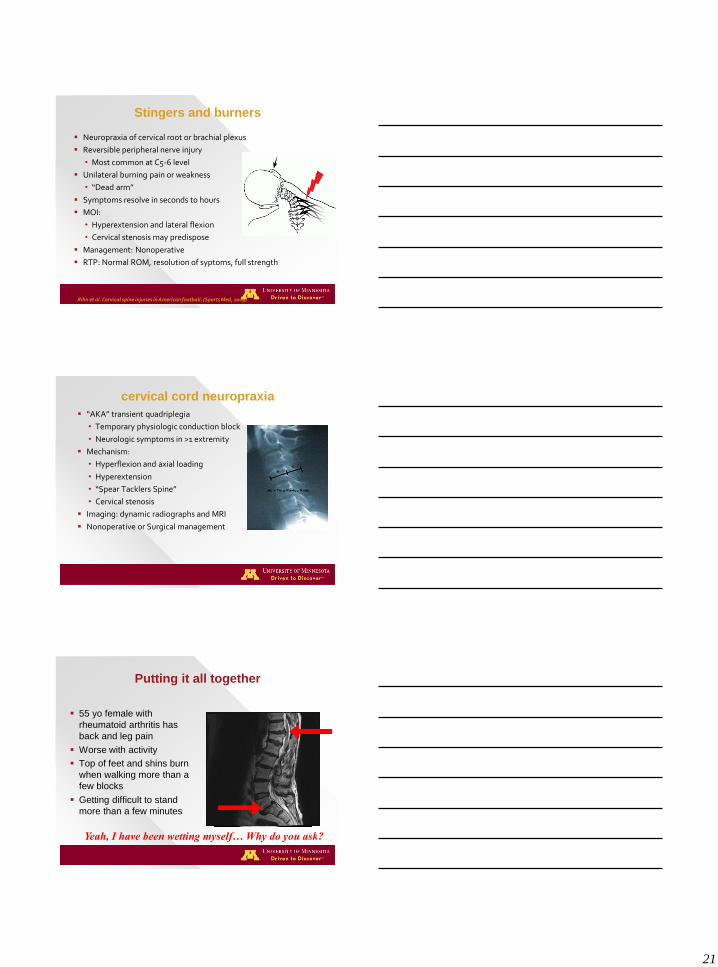
Stingers and burners
Neuropraxia of cervical root or brachial plexus
Reversible peripheral nerve injury
• Most common at C5-6 level
Unilateral burning pain or weakness
• “Dead arm”
Symptoms resolve in seconds to hours
MOI:
• Hyperextension and lateral flexion
• Cervical stenosis may predispose
Management: Nonoperative
RTP: Normal ROM, resolution of syptoms, full strength
Rihn et al. Cervical spine injuries in American football. (Sports Med, 2009)
© 2010 Regents of the University of Minnesota. All rights reserved.
cervical cord neuropraxia
“AKA” transient quadriplegia
• Temporary physiologic conduction block
• Neurologic symptoms in >1 extremity
Mechanism:
• Hyperflexion and axial loading
• Hyperextension
• “Spear Tacklers Spine”
• Cervical stenosis
Imaging: dynamic radiographs and MRI
Nonoperative or Surgical management
© 2010 Regents of the University of Minnesota. All rights reserved.
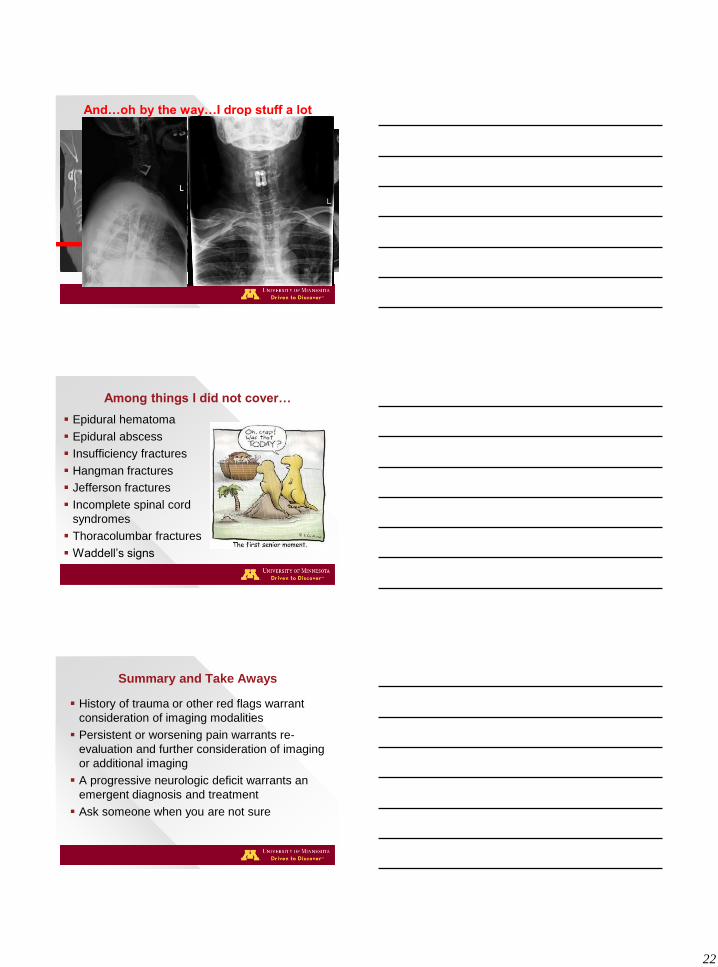
Putting it all together
55 yo female with
rheumatoid arthritis has
back and leg pain
Worse with activity
Top of feet and shins burn
when walking more than a
few blocks
Getting difficult to stand
more than a few minutes
Yeah, I have been wetting myself… Why do you ask?
22
© 2010 Regents of the University of Minnesota. All rights reserved.
And…oh by the way…I drop stuff a lot
© 2010 Regents of the University of Minnesota. All rights reserved.
Among things I did not cover…
Epidural hematoma
Epidural abscess
Insufficiency fractures
Hangman fractures
Jefferson fractures
Incomplete spinal cord
syndromes
Thoracolumbar fractures
Waddell’s signs
© 2010 Regents of the University of Minnesota. All rights reserved.
Summary and Take Aways
History of trauma or other red flags warrant
consideration of imaging modalities
Persistent or worsening pain warrants re-
evaluation and further consideration of imaging
or additional imaging
A progressive neurologic deficit warrants an
emergent diagnosis and treatment
Ask someone when you are not sure
23
© 2010 Regents of the University of Minnesota. All rights reserved.
Questions?
© 2010 Regents of the University of Minnesota. All rights reserved.
Thank You!