19
Dr. Meenakshi Verma Associate Programme Manager National Health Mission, J&k Prevention of Postpartum Haemorrhage through Community Based Distribution of Misoprostol MV
| Date post: | 19-Jul-2015 |
| Category: |
Healthcare |
| Upload: | dr-verma |
| View: | 74 times |
| Download: | 1 times |

D r . M e e n a k s h i V e r m a
A s s o c i a t e P r o g r a m m e M a n a g e r
N a t i o n a l H e a l t h M i s s i o n , J & k
Prevention of Postpartum Haemorrhage through
Community Based Distribution of
Misoprostol
M V

Haemorrhage (PPH) : >19% maternal deaths in one year in J&K and >36%
maternal deaths in one year in India.
Rationale
PPH - largest contributor to MMR (20 out of 104 MDs in the year 2013-14 in J&K were due to PPH)
Persistent home deliveries in many districts/pockets .. women of marginalised and underserved sub-populations.
Complications common esp. PPH Oral Misoprostol recommended for
prevention of PPH where Inj. Oxytocin unavailable.
Miso administration - no special skills, no refrigeration; easy to store and use.
Global evidence supports distribution by CHWs .
M V

Misoprostol….
Misoprostol an oral prostaglandin E1 analogue that, can be administered immediately following delivery, offers an important alternative for PPH prevention in resource constrained settings and during home births, where Injection oxytocin is not available or where its use is not feasible.
Oral Misoprostol does not require provider skills of administering injections or the consumables for injections or refrigeration and can therefore be stored and used easily. These factors enable programs using Misoprostol for the prevention of PPH to potentially achieve high coverage and use, particularly by women who live in the remote and more inaccessible areas where a health facility may be located at a prohibitively long distance.
M V

Misoprostol- how much it is safe…..
Existing evidence demonstrates that Misoprostol is both safe and effective in the prevention of PPH.
This body of evidence led the World Health Organization (WHO) to amend its model list of essential medicines in March 2011 to include misoprostol for the prevention of PPH in settings “where oxytocin is not available or cannot be safely used”. The WHO Guidelines on “Optimizing HW Roles for MNH Interventions through Task Shifting” have also given a positive recommendation for the use of Misoprostol by a “Lay Worker” for home births, for the prevention of PPH.
Drug can be safely used at the community level through either administration by health providers or distribution by Community Health Workers (CHWs) directly to pregnant women for self-administration at home. M V

Key policy decision
Community based advance distribution of Misoprostol
by ANMs and ASHAs to pregnant women likely to deliver at home
Objective : Bring this life saving commodity to the doorstep of those pregnant women …
not likely to access a health facility for delivery
ANM not likely to attend the delivery
Intended Inst. Del. , but
deliver at home
Deliver in transit
Special Scenarios
Recommendations of Core Group of Experts
M V

Conditionalities for Community Based Distribution
of Misoprostol
Criteria for selection of areas-( pre-identified/pre-
notified)
On pilot basis in Selected districts of
J&K with Home Delivery >20%
14 Districts of the state
Jammu Div:
Doda, Rajouri, Poonch, Kathua,
Kishtwar, Ramban, Reasi, Udhampur
Kashmir Div:
Bandipora, Baramulla, Kargil,
Leh, Kulgam, Kupwara
M V
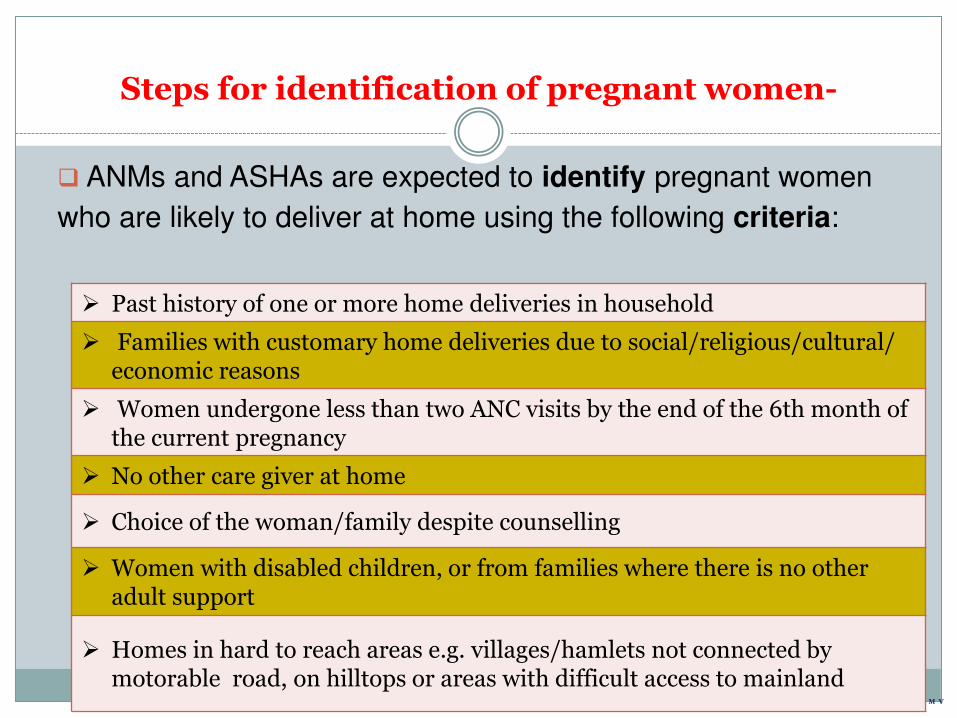
Steps for identification of pregnant women-
ANMs and ASHAs are expected to identify pregnant women
who are likely to deliver at home using the following criteria:
Past history of one or more home deliveries in household
Families with customary home deliveries due to social/religious/cultural/ economic reasons
Women undergone less than two ANC visits by the end of the 6th month of the current pregnancy
No other care giver at home
Choice of the woman/family despite counselling
Women with disabled children, or from families where there is no other adult support
Homes in hard to reach areas e.g. villages/hamlets not connected by motorable road, on hilltops or areas with difficult access to mainland
M V

Responsibility for advance distribution-
Ideally, ANM is the chosen health functionary , BUT in case of non availability , the ASHA is to be empowered to perform this function
M V

Contraindications…..
• SHOULD NOT BE TAKEN DURING PREGNANCY(any time before delivery) due to risk of abortion, pre term labour or rupture uterus.
During Pregnancy
• Exclusion of multiple pregnancy by 8th month before distribution(ASHA/ANM to ensure).
Multiple Pregnancy
Previous C-Section
Severe anaemia
Severe PIH Malpresentation
Myomectomy
Cardiac disease/other
medical complications
M V

“In case multiple pregnancy suspected/diagnosed, referral to appropriate level of facility for
institutional care is imperative…”
M V

Process of distribution-
• 8th month of pregnancy Time of
distribution
• At least twice at one week’s interval with detailed instructions by ANM or ASHA on the self- administration of Misoprostol tablets
Counseling
• As per SBA Guidelines - three tablets of 200 mcg each (total of 600 mcg)
Dosage
• Preferably through home visits by the ANMs or ASHAs with instructions also to female family member
Site of distribution
• Delivery during transit or at home, even if intended at institution- ASHA/family member will give Miso 600mcg
Special Cases
M V

Adverse events-
Though minor & rarely serious, the ANM and ASHA should
record and report all cases of adverse events attributed to the
intake of Misoprostol
Fever/chills & rigors
Nausea/ vomiting
abdominal cramps
Diarrhoea
Headache
Severe allergic reactions
M V

Supply and Storage of Misoprostol Tablets
ANMs to distribute to ASHAs and ensure adequate stock
with them.
Number of doses of Misoprostol to be kept with ASHAs at any point of time =
Number of women enlisted (women expected to deliver at home) + one or
two emergency doses
M V

Recording & Reporting
Stock of Misoprostol to be distributed to the ANM by the
pharmacist/MO – PHC.
ANMs will distribute to the ASHAs.
Pharmacist, ANM & ASHA will maintain records as applicable on stock, details of drug in stock & distribution of tablets.
ASHA will submit monthly report of doses distributed to ANM who in turn will submit consolidated report to Block PHC/CHC.
ANM/ASHA will record & report all adverse events.
M V

Role of ANM/ ASHA….
ASHA shall identify pregnant women for advance distribution of misoprostol with special emphasis on the focus groups viz. households with history of home deliveries only, multi para, abandoned women, migratory groups like Gujjars and Bakarwals.
M V

Role of ANM/ ASHA….
She shall generate awareness, shall motivate and promote the safety and use of misoprostol among the focused groups during VHNDs and home visits. ANM shall also visit the home of the beneficiaries along with ASHA.
M V
Role of ANM/ ASHA….
The ASHAs and ANMs shall enlist and follow up all the pregnant women in the community for advanced distribution of Misoprostol to the targeted women during 8th month of pregnancy through home visits with all the necessary instructions in regard to dose and timing of the drug.
M V

Incentives
ASHAs shall receive an incentive of Rs 100 per beneficiary…
Conditionalities -
Pre-identification and listing of pregnant women likely to deliver at home.
Certification of ruling out multiple pregnancy or other contraindications by the ANM on the MCP card.
Instructions to the woman on the mode and dosage of administration of Misoprostol for prevention of PPH.
Reporting of delivery and recording of side effects if any.
M V

M V
D r . M e e n a k s h i V e r m a
A s s o c i a t e P r o g r a m m e M a n a g e r
N a t i o n a l H e a l t h M i s s i o n , J & k

















