19
COMMUNITY MANAGEMENT OF ACUTE MALNUTRITION IN UNDER-FIVE CHILDREN

COMMUNITY MANAGEMENT OF ACUTE MALNUTRITION IN UNDER-FIVE CHILDREN
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
1
INDEX
Understanding malnutrition
The need in India
Alignment to Sustainable Development Goals
The solution
Why is CMAM recommended?
Implementing a CMAM program
a. Duration of program
b. Identifying a community
c. Community mapping
d. Identifying a credible implementation partner
e. Selecting and training community health workers
f. Securing government buy-in
g. Securing community buy-in
h. Establishing a baseline
i. Monitoring and evaluation
Important considerations
How can companies help?
Appendix 1 - Key technical terms
Appendix 2 - Cost of CMAM programs (per child cured) from literature
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
2
Program summary
Specific problems addressed•Malnutrition
Target Population•Children under the age of 5•Mothers
Target communities•Rural•Urban•Tribal•Communities hit with natutal disasters/ emergencies
Budget•Human-resource intensive
Linked programs•HBNC•Maternal care (ante natal and delivery)
Minimum period of support•3 years
Linkage with government•Integarted Child Development Scheme (ICDS)
Specific focus in RMNCH+A•Child health (0-5 year olds)
1
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
3
Understanding malnutrition1 Malnutrition is a group of conditions in children and adults generally related to poor quality or insufficient quantity of nutrient intake, absorption, or utilization.
There are two major types of malnutrition:
• Protein-energy malnutrition - resulting from deficiencies in any or all nutrients • Micronutrient deficiency diseases - resulting from a deficiency of specific
micronutrients
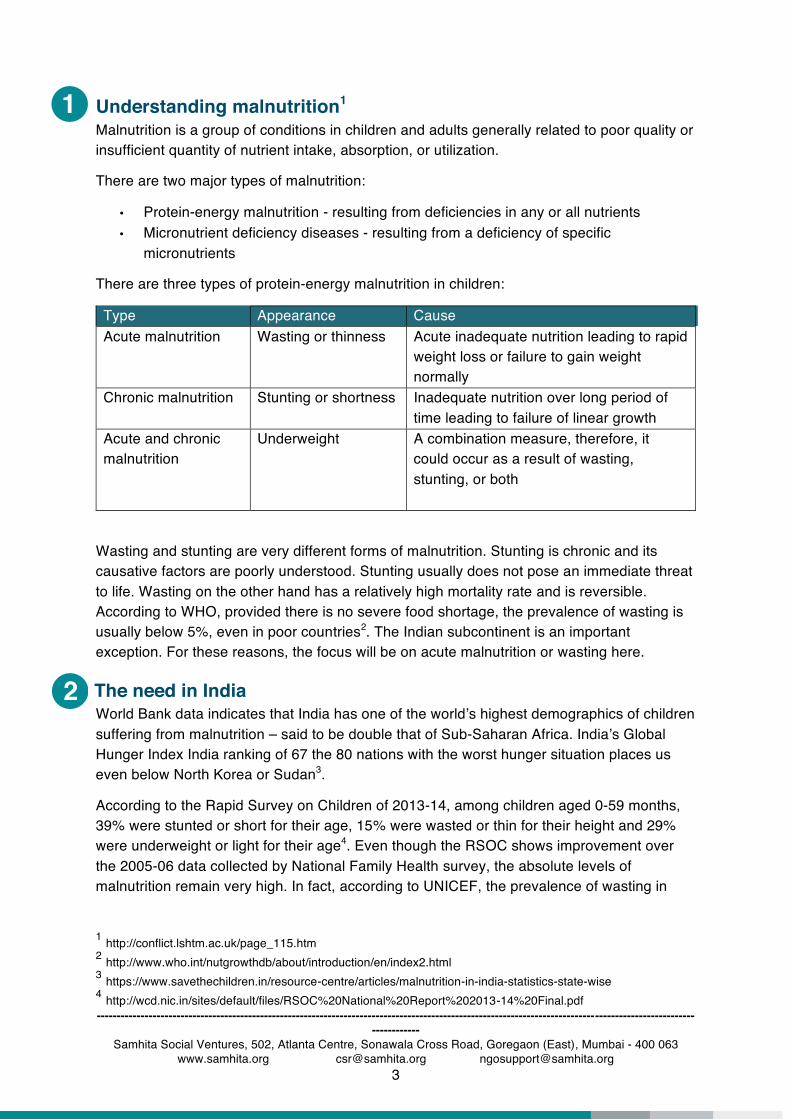
There are three types of protein-energy malnutrition in children:
Type Appearance Cause Acute malnutrition Wasting or thinness Acute inadequate nutrition leading to rapid
weight loss or failure to gain weight normally
Chronic malnutrition Stunting or shortness Inadequate nutrition over long period of time leading to failure of linear growth
Acute and chronic malnutrition
Underweight A combination measure, therefore, it could occur as a result of wasting, stunting, or both
Wasting and stunting are very different forms of malnutrition. Stunting is chronic and its causative factors are poorly understood. Stunting usually does not pose an immediate threat to life. Wasting on the other hand has a relatively high mortality rate and is reversible. According to WHO, provided there is no severe food shortage, the prevalence of wasting is usually below 5%, even in poor countries2. The Indian subcontinent is an important exception. For these reasons, the focus will be on acute malnutrition or wasting here.
The need in India World Bank data indicates that India has one of the world’s highest demographics of children suffering from malnutrition – said to be double that of Sub-Saharan Africa. India’s Global Hunger Index India ranking of 67 the 80 nations with the worst hunger situation places us even below North Korea or Sudan3.
According to the Rapid Survey on Children of 2013-14, among children aged 0-59 months, 39% were stunted or short for their age, 15% were wasted or thin for their height and 29% were underweight or light for their age4. Even though the RSOC shows improvement over the 2005-06 data collected by National Family Health survey, the absolute levels of malnutrition remain very high. In fact, according to UNICEF, the prevalence of wasting in
1 http://conflict.lshtm.ac.uk/page_115.htm 2 http://www.who.int/nutgrowthdb/about/introduction/en/index2.html 3 https://www.savethechildren.in/resource-centre/articles/malnutrition-in-india-statistics-state-wise 4 http://wcd.nic.in/sites/default/files/RSOC%20National%20Report%202013-14%20Final.pdf
2

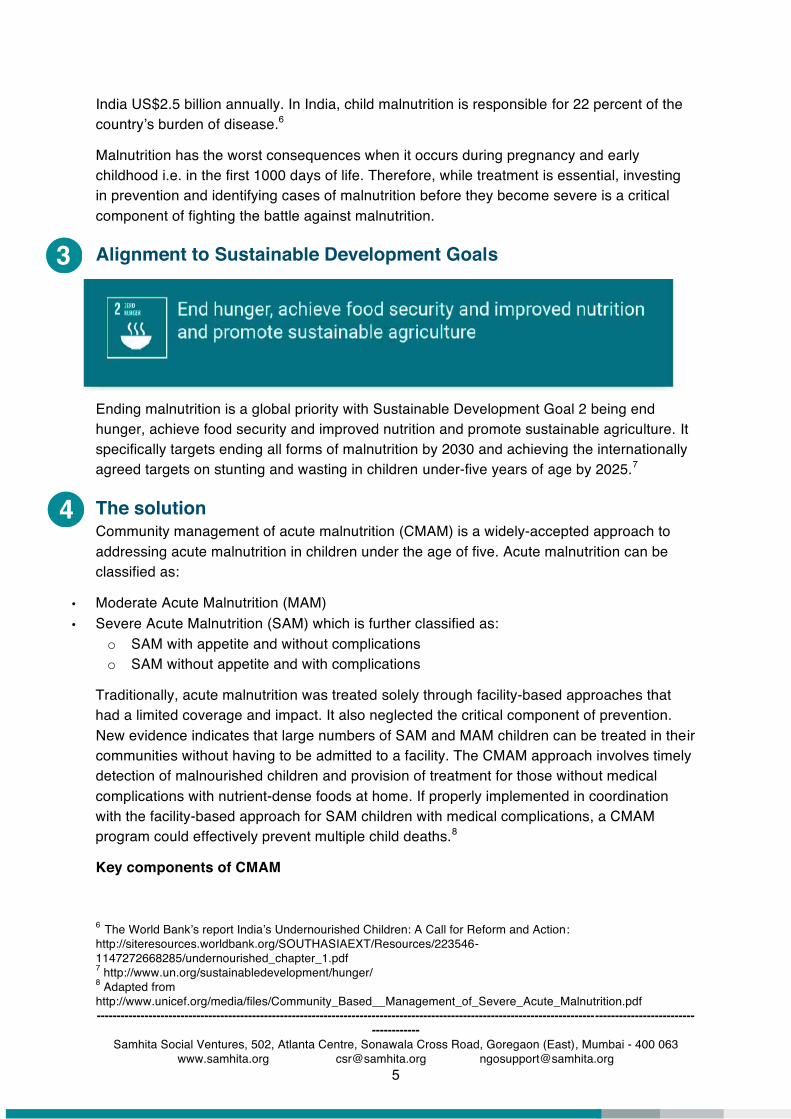
Critical>15%
Serious10 to <15%_ _ _ _ _ _ _ _ _ _ _ _ _Public health emergency line
Poor 5 to <10%
Acceptable<5%
no data
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
4
South Asia is so severe, at just under 15 per cent, that it is approaching the level of a critical public health problem5.
Source: UNICEF
Causes of malnutrition
While the immediate causes of malnutrition are linked to inadequate food intake, both in terms of quality and quantity, it is also influenced by a large number of contributing factors such as poor water and sanitation services, inadequate access to health services, gender inequality and lack of knowledge about good nutritional practices including inadequate breastfeeding, offering the wrong foods, contribute to malnutrition.
Consequences of malnutrition among children
• Physical impairment and increase in mortality -
Malnutrition is a leading contributor to infant, child and maternal mortality and morbidity. A child with severe acute malnutrition (SAM) is 11.6 times more likely to die, and a child with moderate acute malnutrition (MAM) is 3 times more likely to die than a well-nourished child (Olofin, 2013). This is because malnourished children have lowered resistance to infection; they are more likely to die from common childhood ailments like diarrhoeal diseases and respiratory infections; and for those who survive, frequent illness leads to a vicious cycle of recurring sickness and faltering growth.
• Developmental and cognitive impairment –
Under nutrition also affects cognitive and motor development and undermines educational attainment; and, ultimately impacts on productivity at work and at home, with adverse implications for income and economic growth. Micronutrient deficiencies alone may cost
5 http://data.unicef.org/topic/nutrition/malnutrition/#
3
4
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
5
India US$2.5 billion annually. In India, child malnutrition is responsible for 22 percent of the country’s burden of disease.6
Malnutrition has the worst consequences when it occurs during pregnancy and early childhood i.e. in the first 1000 days of life. Therefore, while treatment is essential, investing in prevention and identifying cases of malnutrition before they become severe is a critical component of fighting the battle against malnutrition.
Alignment to Sustainable Development Goals
Ending malnutrition is a global priority with Sustainable Development Goal 2 being end hunger, achieve food security and improved nutrition and promote sustainable agriculture. It specifically targets ending all forms of malnutrition by 2030 and achieving the internationally agreed targets on stunting and wasting in children under-five years of age by 2025.7
The solution Community management of acute malnutrition (CMAM) is a widely-accepted approach to addressing acute malnutrition in children under the age of five. Acute malnutrition can be classified as:
• Moderate Acute Malnutrition (MAM) • Severe Acute Malnutrition (SAM) which is further classified as:
o SAM with appetite and without complications o SAM without appetite and with complications
Traditionally, acute malnutrition was treated solely through facility-based approaches that had a limited coverage and impact. It also neglected the critical component of prevention. New evidence indicates that large numbers of SAM and MAM children can be treated in their communities without having to be admitted to a facility. The CMAM approach involves timely detection of malnourished children and provision of treatment for those without medical complications with nutrient-dense foods at home. If properly implemented in coordination with the facility-based approach for SAM children with medical complications, a CMAM program could effectively prevent multiple child deaths.8
Key components of CMAM
6 The World Bank’s report India’s Undernourished Children: A Call for Reform and Action: http://siteresources.worldbank.org/SOUTHASIAEXT/Resources/223546-1147272668285/undernourished_chapter_1.pdf 7 http://www.un.org/sustainabledevelopment/hunger/ 8 Adapted from http://www.unicef.org/media/files/Community_Based__Management_of_Severe_Acute_Malnutrition.pdf
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
6
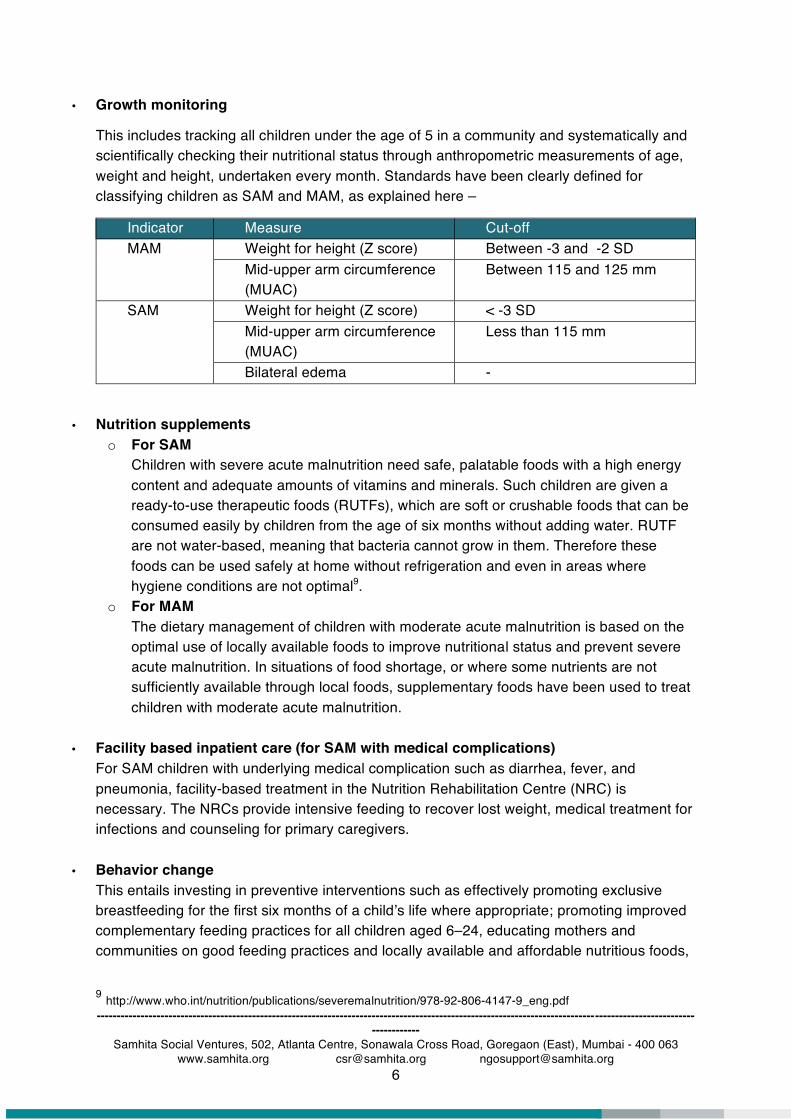
• Growth monitoring
This includes tracking all children under the age of 5 in a community and systematically and scientifically checking their nutritional status through anthropometric measurements of age, weight and height, undertaken every month. Standards have been clearly defined for classifying children as SAM and MAM, as explained here –
Indicator Measure Cut-off MAM Weight for height (Z score) Between -3 and -2 SD
Mid-upper arm circumference (MUAC)
Between 115 and 125 mm
SAM Weight for height (Z score) < -3 SD Mid-upper arm circumference (MUAC)
Less than 115 mm
Bilateral edema -
• Nutrition supplements o For SAM
Children with severe acute malnutrition need safe, palatable foods with a high energy content and adequate amounts of vitamins and minerals. Such children are given a ready-to-use therapeutic foods (RUTFs), which are soft or crushable foods that can be consumed easily by children from the age of six months without adding water. RUTF are not water-based, meaning that bacteria cannot grow in them. Therefore these foods can be used safely at home without refrigeration and even in areas where hygiene conditions are not optimal9.
o For MAM The dietary management of children with moderate acute malnutrition is based on the optimal use of locally available foods to improve nutritional status and prevent severe acute malnutrition. In situations of food shortage, or where some nutrients are not sufficiently available through local foods, supplementary foods have been used to treat children with moderate acute malnutrition.
• Facility based inpatient care (for SAM with medical complications) For SAM children with underlying medical complication such as diarrhea, fever, and pneumonia, facility-based treatment in the Nutrition Rehabilitation Centre (NRC) is necessary. The NRCs provide intensive feeding to recover lost weight, medical treatment for infections and counseling for primary caregivers.
• Behavior change This entails investing in preventive interventions such as effectively promoting exclusive breastfeeding for the first six months of a child’s life where appropriate; promoting improved complementary feeding practices for all children aged 6–24, educating mothers and communities on good feeding practices and locally available and affordable nutritious foods,
9 http://www.who.int/nutrition/publications/severemalnutrition/978-92-806-4147-9_eng.pdf
5
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
7
importance of clean drinking water, handwashing and other hygiene practices. It seeks to promote overall health seeking behavior in the community.
• Strengthening government machinery The Integrated Child Development Scheme (ICDS) is the primary government mechanism to address early childcare needs in India. The anganwadi worker’s mandate includes monthly growth monitoring and provision of supplementary foods. CMAM should ideally leverage the ICDS infrastructure where available, strengthen it and build the anganwadi worker’s capacity to ensure continuity and institutionalization of impact.
The program operates through a network of community health workers (CHW) who screen children for acute malnutrition and undertake BCC activities. The program also has a strong community mobilization component. One of the core objectives is to raise awareness about malnutrition and encourage community participation in CMAM. This would result in the community demanding services and subsequently translate to greater access and higher coverage.
Why is CMAM recommended? • Widely endorsed and accepted: The CMAM model has been widely endorsed by expert
agencies such as WHO and UNICEF. It has been globally recognized as an effective method of tackling the widespread problem of acute malnutrition in children under five, and is currently implemented in more than 70 countries 10.
• Evidence of effectiveness: According to UNICEF’s evaluation of CMAM published in 2013
covering CMAM programs across Chad, Ethiopia, Kenya, Nepal and Pakistan, CMAM was successful in achieving the following outcomes -
10 https://www.usaid.gov/what-we-do/global-health/nutrition/technical-areas/community-based-management-acute-malnutrition
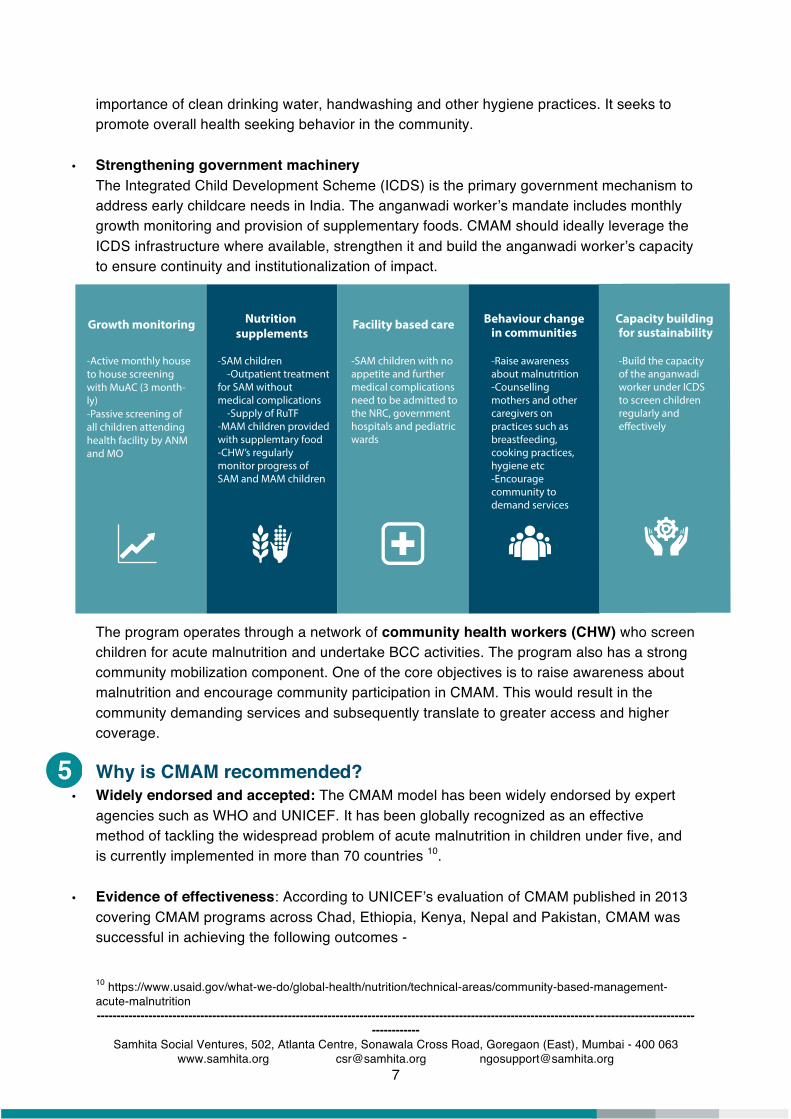
Growth monitoring Nutrition supplements
Facility based care Behaviour changein communities
-Active monthly house to house screening with MuAC (3 month-ly)-Passive screening of all children attending health facility by ANM and MO
-SAM children -Outpatient treatment for SAM without medical complications -Supply of RuTF-MAM children provided with supplemtary food-CHW’s regularly monitor progress of SAM and MAM children
-SAM children with no appetite and further medical complications need to be admitted to the NRC, government hospitals and pediatric wards
Capacity building for sustainability
-Raise awareness about malnutrition-Counselling mothers and other caregivers on practices such as breastfeeding, cooking practices, hygiene etc-Encourage community to demand services
-Build the capacity of the anganwadi worker under ICDS to screen children regularly and
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
8
o Active case finding critically improved admissions to facilities and services o CMAM was effective in helping admitted children to recover from SAM and promoting
prevention through community outreach and MAM management o Community members and health workers affirmed higher levels of knowledge
regarding the impact of nutrition on childhood development.
• Comprehensive: The CMAM approach goes beyond simply treating SAM children and focuses on addressing the problem holistically. The program aims to create awareness and influence behaviour change, thereby strengthening preventive measures for combating acute malnutrition. Concerted efforts are made to ensure that MAM children do not deteriorate into SAM children. To address a complex problem such as malnutrition, a comprehensive approach is imperative.
• Extensive availability of documented resources: The CMAM approach has been
documented extensively by various credible organizations. From program descriptions, to guidelines, to checklists and tools, to case studies and best practices, there is a wealth of information available in the public domain that can be used to gain a deeper insight into the implementation of a successful CMAM program.
• Cost effective: UNICEF and WHO have recognized CMAM as a highly cost-effective
nutrition intervention. Studies examining a CMAM program in Ethiopia found that the cost per child in the CMAM program was $145.50 in comparison to treatment in a therapeutic feeding centre at $320.00.11 Puett et al. found that a CMAM program delivered by CHWs in Bangladesh cost US$26 per DALY averted and US$869 per life saved.12
• Availability of credible implementation partners: Owing to the scale and significance of
the problem of malnutrition, there are a large number of credible organizations in India that are working for the cause.
• Potential for scale: A well-structured CMAM program has the potential to be replicated
across multiple communities and cover a large number of beneficiaries. Once the mechanism for implementation and all the associated nuances are understood, taking the program to scale involves identifying the appropriate communities, adapting the approach accordingly and securing their buy-in.
11 https://www.ncbi.nlm.nih.gov/books/NBK361900/ 12 https://www.ncbi.nlm.nih.gov/pubmed/22879522

6
02Community mapping• A comprehensive survey of household demographics and socioeconomic status• Complete registry of children• Establishing the baseline data
05 Securing government buy-in• Build linkages with locl ICDS departments and nrcs01
Selection of community• Areas with at least 10% of children under 5 as moderately malnourished• Areas with other vulnerabilities
06 Securing community buy-in• Participatory exercise• Door to door mobilsation
07Monitoring and evaluation• Percentage of relapse into SAM and MAM• Percentage of MAM transitioning out due to weight gain• Average weight gain for both MAM and SAM
04Selection and training of CHWs• Select according to best practices• Training conducted in the community• Incentives• Supervision
03Identifying NGOs• Working in healthcare• Strong connect with the community• Strong data management and analysis skills• Strong govenment linkage
Implementing a CMAM program This section will detail the basic framework underpinning any CMAM program. While the model itself consists of certain standardized aspects, to successfully implement this program within a community, it will need to be customized to suit the dynamics of the target community.
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
9
a. Duration of program
A typical CMAM project requires a minimum of three years to yield results in terms of
reducing malnutrition and making the impact sustainable.
b. Identifying a community
Identifying the community in which the program will be implemented depends heavily on the priorities of the funder. For instance some companies are keen to implement programs in the community around their offices or factories, while others may be focused on identifying the most vulnerable communities with the poorest existing indicators. Selection of a community should be done systematically after giving the matter some thought.
Given below is a basic list of factors that should be considered while selecting a community:
• The existing nutritional indicators – CMAM is best suited for areas where at least 10% of children under 5 are moderately malnourished (low weight for height)13. In addition, areas with added vulnerabilities such as food insecurity, isolated from health networks,
13 http://wcdodisha.gov.in/node/405

------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
10
recovering from natural disasters and having a widespread communicable diseases and high crude death rate are also appropriate for CMAM implementation. • Existing network of social organizations (NGOs / CBOs) and programs being implemented – it is important to identify the existing players in the community (if any) and the programs that they are implementing. There are pros and cons to both – a community where there are a lot of programs running and a community where there are no other programs running. In the former, there is scope for collaboration with related programs, the opportunity to partner with established organizations that already have a strong community connect, and the potential to leverage the data collected and infrastructure set up by other players. However, there is also the risk of conflict with other organizations, frustrating the community with multiple interventions,
uncoordinated efforts resulting in replication of efforts and the inability to analyze outcomes solely attributed to the program. In the latter, there is no need for complex coordination with other players and the community does not have any pre-conceived notions of external programs. However, potential hostility / resistance from the community and an extended set-up period would be the key challenges.
• Existing / accessible government infrastructure – there should be a preliminary understanding of the availability of existing government infrastructure such as community health centers, NRCs and anganwadis as it is critical and has an implication when designing and implementing the program.
c. Community mapping
Before designing and rolling out HBNC in any area, the following activities needs to be ideally conducted to understand the gaps, the preferences of the community, availability of resources, assessing the risks etc. All these factors will feed into specific program design and plan for execution. Community mapping includes:
A comprehensive survey of household demographics and socioeconomic status A registry of children Identifying healthcare providers if any and accounting for them in the program design Mapping the healthcare infrastructure in and around the community to identify gaps that may need addressing and establish referral linkages Identifying non-profit community organizations if any
A few helpful resources –
1. Training Guide for Community-
Based Management of Acute
Malnutrition (CMAM), including
community mobilization and M&E -
http://www.fantaproject.org/focus-
areas/nutrition-emergencies-
mam/cmam-training
2. WHO Anthro, a software
consisting of three modules:
• Anthropometric calculator
• Individual assessment
• Nutritional survey
http://www.who.int/childgrowth/softwar
e/en/
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
11
Establishing the baseline data
d. Identifying a credible implementation partner
This is an extremely critical step in the process and will have a huge impact on the outcomes. An efficient implementation partner who is able to establish a strong community connect is vital to a successful CMAM program. The ideal partner would already have a strong community connect and a focus on malnutrition, however this is not always the case. We recommend the following criteria for selecting an implementation partner:
Focused on malnutrition – this may be traded-off for a partner who has no focus on malnutrition but has a very strong presence in the selected community. In this case, it becomes essential to engage with experts or consultants who can guide the design and implementation of the program. Has established or is able to establish a strong community connect Has experience in participatory approaches and experience of creating community leaders Has a successful track record of recruiting and managing a large team of field workers Has worked on influencing behaviour change Has experience collaborating with the government Has an existing physical set-up in the community Has the willingness, ability and resources to collect, manage, analyse and interpret growth data regularly Has an inclination towards rigorous research, keeps abreast of development in the nutrition sector and partnerships with academic/ expert organizations
Again, the type of implementation partner selected depends heavily on the priorities of the funder. While some funders are keen to be actively engaged in the planning and implementation of the program, others are relatively disconnected with the implementation and are more concerned with the expenditure and output reports. For the former, it is important to identify an implementation partner who is excited about and willing to have the funder actively involved. For the latter, it is important to identify an implementation partner who requires minimum supervision and handholding support.
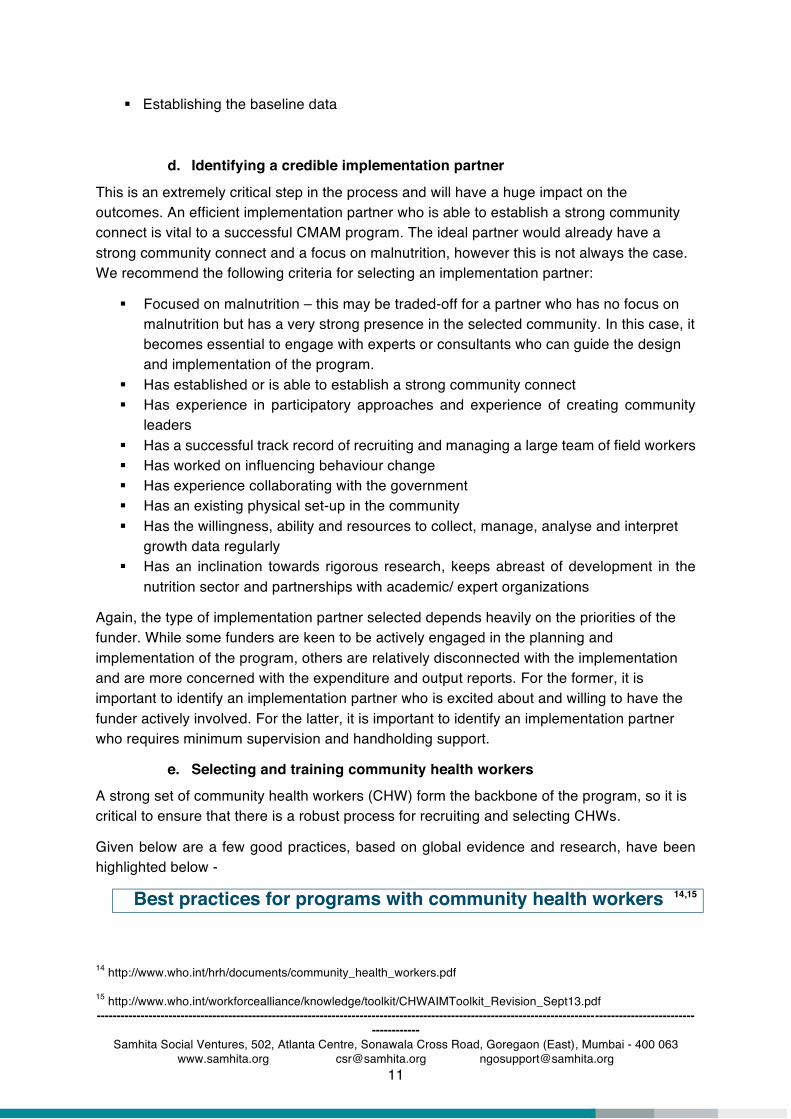
e. Selecting and training community health workers
A strong set of community health workers (CHW) form the backbone of the program, so it is critical to ensure that there is a robust process for recruiting and selecting CHWs.
Given below are a few good practices, based on global evidence and research, have been highlighted below -
Best practices for programs with community health workers 14,15
14 http://www.who.int/hrh/documents/community_health_workers.pdf 15 http://www.who.int/workforcealliance/knowledge/toolkit/CHWAIMToolkit_Revision_Sept13.pdf

------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
12
Every model discussing community health workers emphasize that CHWs should be chosen from the communities they will serve and that communities should have a say in the selection of their CHWs. They should not be unilaterally appointed by village sarpanch or health personnel. The District Health & Family Welfare Society’s guidelines on the process of ASHA selection can be found here. However, sometimes, an external person may command more respect and attention as opposed to a woman in the community who may be viewed as a non-expert. The balance between from within the community or outside should be maintained. Another important selection criterion for CHW selection is language skill, it can be assumed that originating or residing in the community for which a CHW serves would ensure that she speaks the local language16. The job description and role of the CHW should be documented and have specific expectations (e.g. workload, time per day, maximum travel distance and role of community) and tasks (e.g. home visits, weighing children, providing food supplements etc., you can find the specific tasks in Appendix 3). There is a great diversity of approaches, location, organization and length of training, but there is agreement on one matter - that continuing or refresher training is as important as initial training. A good training protocol would allow ‘classroom’ training to be followed by a regular period of application of that knowledge in the community and then going back to the classroom for more learning. CHW programmes hinges on regular and reliable support and supervision, this is often among the weakest links in CHW programmes. In addition to supervision, other forms of support, such as the reliable provision of transport, ambulance, drug supplies and equipment have been identified as another factor in CHW effectiveness. The CHW should be offered a balanced incentive package that could include financial incentives such as salary and bonuses and non financial incentives such as recognition, certification, uniforms etc. It is important to position the remuneration appropriately, such that it is not seen as the primary motivating factor. The CHW should be ideally accountable to the community, her role should be understood by the community.
f. Securing government buy-in
Before implementing the CMAM program we recommend securing requisite government permissions and co-opting the local ICDS departments. This is an essential step as it ensures that the program is aligned to the existing government priorities, that the implementation does not get disrupted by the local authorities and facilitates the use of existing infrastructure within the community. The program should actively strengthen the capacity of ICDS to be able to undertake these activities with the same rigour, as this alone can guarantee continuity of impact once the funders exit the program. It is helpful to position the program as something that will help and benefit the ICDS workers in future and help them achieve their targets better.
16 http://www.mchip.net/sites/default/files/mchipfiles/07_CHW_Recruitment.pdf
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
13
g. Securing community buy-in
This is a crucial step in implementing a CMAM program and requires due effort and attention. It can take between 3 to 6 months. A CMAM program can only be successful once the community buys into it. Local nutritional practices are dominated by the customs and traditions of the community and therefore it becomes essential to secure the confidence of all the stakeholders. This step is about establishing a strong presence in the community and building trust. It involves:
• Initiating and sustaining a dialogue with the members of the community • Using participatory methods to get them engaged • Understanding their perceptions and challenges • Establishing a relationship with them • Demonstrating the value of the program • Using innovative methods such as mobile technology to remind parents of
feeding practices and disseminate messages on BCC
h. Establishing a baseline
Conducting a baseline study before implementation will reveal the existing indicators and the community’s perception around nutrition. This information will be useful both while planning the program, as well as when the outcomes are being measured. The methodology can be decided based on the time constraints, the receptiveness of the community and the availability of manpower. We recommend a combination of household surveys, focus group discussions and key stakeholder interviews that capture quantitative and qualitative data. The selected CHWs can be trained to conduct the data collection activities.
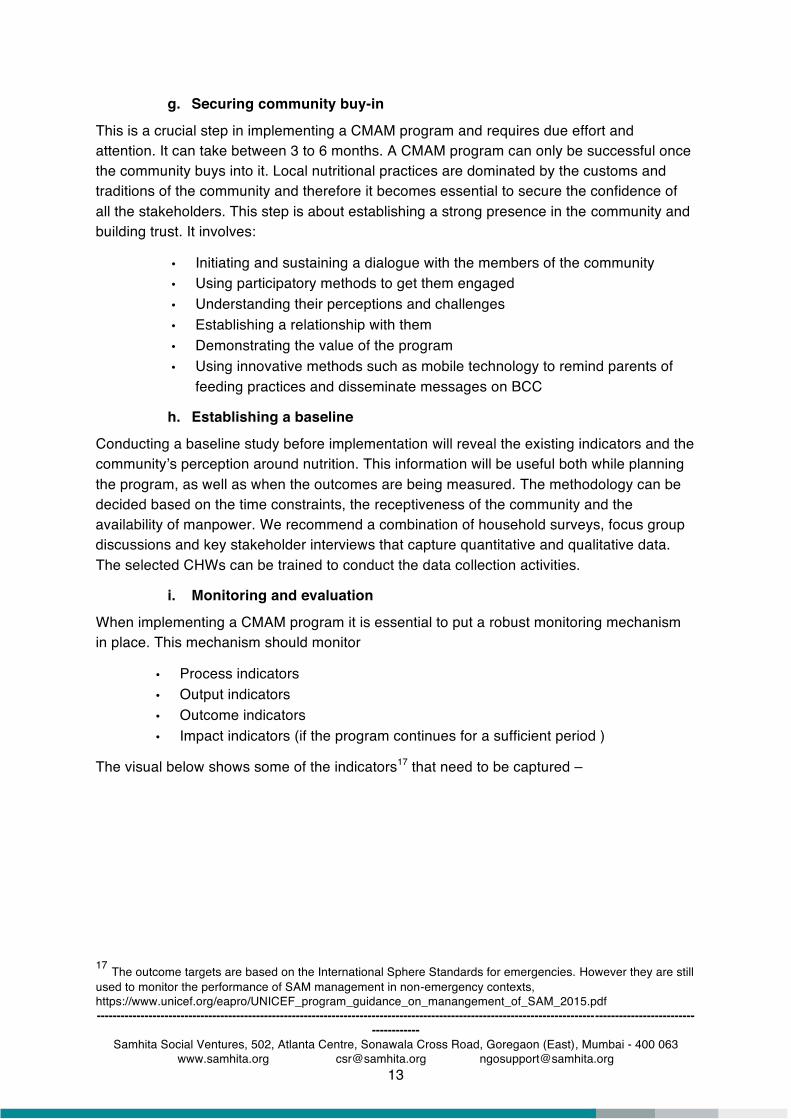
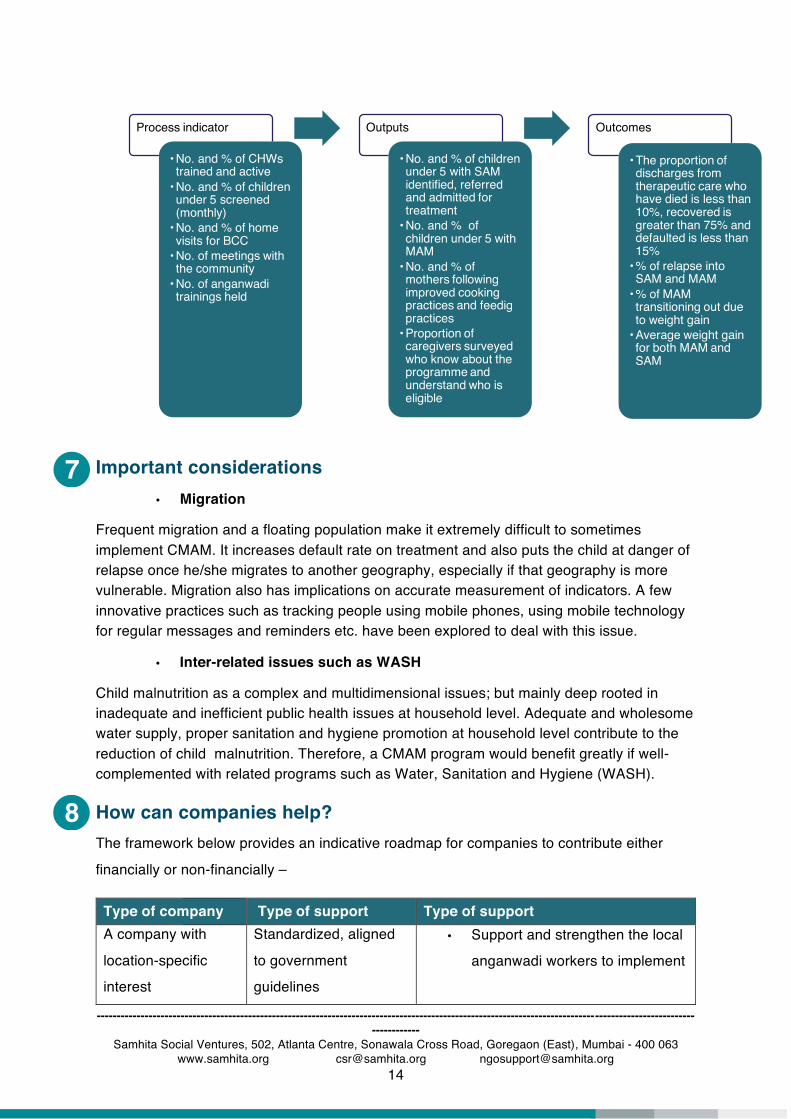
i. Monitoring and evaluation
When implementing a CMAM program it is essential to put a robust monitoring mechanism in place. This mechanism should monitor
• Process indicators • Output indicators • Outcome indicators • Impact indicators (if the program continues for a sufficient period )
The visual below shows some of the indicators17 that need to be captured –
17 The outcome targets are based on the International Sphere Standards for emergencies. However they are still used to monitor the performance of SAM management in non-emergency contexts, https://www.unicef.org/eapro/UNICEF_program_guidance_on_manangement_of_SAM_2015.pdf
8
7
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
14
Important considerations • Migration
Frequent migration and a floating population make it extremely difficult to sometimes implement CMAM. It increases default rate on treatment and also puts the child at danger of relapse once he/she migrates to another geography, especially if that geography is more vulnerable. Migration also has implications on accurate measurement of indicators. A few innovative practices such as tracking people using mobile phones, using mobile technology for regular messages and reminders etc. have been explored to deal with this issue.
• Inter-related issues such as WASH
Child malnutrition as a complex and multidimensional issues; but mainly deep rooted in inadequate and inefficient public health issues at household level. Adequate and wholesome water supply, proper sanitation and hygiene promotion at household level contribute to the reduction of child malnutrition. Therefore, a CMAM program would benefit greatly if well-complemented with related programs such as Water, Sanitation and Hygiene (WASH).
How can companies help? The framework below provides an indicative roadmap for companies to contribute either
financially or non-financially –
Type of company Type of support Type of support
A company with
location-specific
interest
Standardized, aligned
to government
guidelines
• Support and strengthen the local
anganwadi workers to implement
Process indicator
• No. and % of CHWs trained and active
• No. and % of children under 5 screened (monthly)
• No. and % of home visits for BCC
• No. of meetings with the community
• No. of anganwadi trainings held
Outputs
• No. and % of children under 5 with SAM identified, referred and admitted for treatment
• No. and % of children under 5 with MAM
• No. and % of mothers following improved cooking practices and feedig practices
• Proportion of caregivers surveyed who know about the programme and understand who is eligible
Outcomes
• The proportion of discharges from therapeutic care who have died is less than 10%, recovered is greater than 75% and defaulted is less than 15%
• % of relapse into SAM and MAM
• % of MAM transitioning out due to weight gain
• Average weight gain for both MAM and SAM

9
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
15
Type of company Type of support Type of support
CMAM through training and
technical support
Customized, going
beyond government
requirements
• Can replicate CMAM in their
geographies with help of NGO
partners
A company with
specific core
competency such as
IT or media industry
Catalytic • Create app-based training and
M&E solutions for CHWs
• Design behaviour-change
messages for the target group
based on consumer research
• Run mass or social media
campaigns
A company with a
strategic interest in
CMAM such as
pharma, diagnostic
equipment or food
and beverage
industry
Non-financial • Provide requisite medicines and/
or equipment
• Design and produce fortified18
foods such as flour, oil, salt, milk
etc. or in case of existing
products, ensure access and
affordability to bottom of pyramid
markets
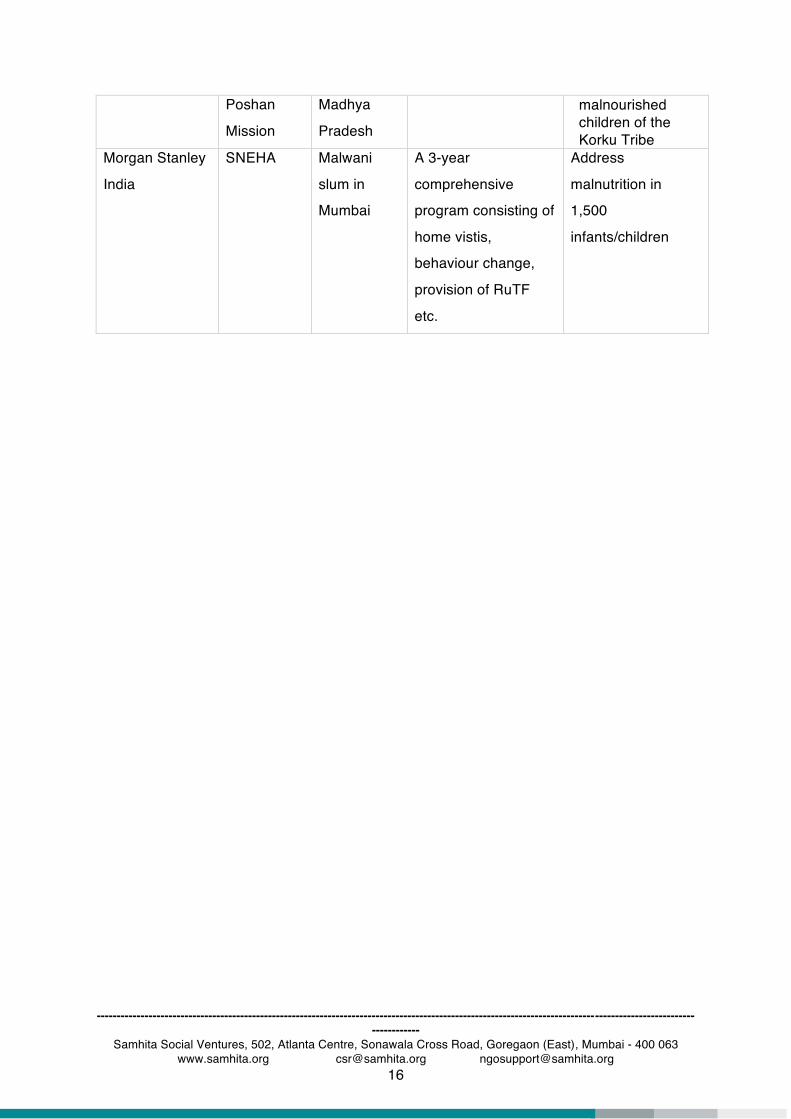
Examples of corporate partnerships for CMAM
Company
Other partners
Geography
Project description
Impact
Glenmark
Pharmaceuticals
Limited19
Spandan
Samaj
Sewa
Samiti and
Atal Bal
Khalwa
Block of
Khandwa
district in
The objective was to
reduce child mortality
among the
marginalized Korku
tribe.
More than 1200 malnourished children successfully treated for SAM Impacted over 4500
18 Fortification means deliberately increasing the content of essential micronutrients such as iron, Vitamin A, Vitamin D, Iodine, etc, in a food product so as to improve its nutritional quality with minimal risk to health. 19 Glenmark Foundation' Announces Positive Impact of its Child Health Programme in Madhya Pradesh Focused on the Marginalized Korku Tribe
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
16
Poshan
Mission
Madhya
Pradesh
malnourished children of the Korku Tribe
Morgan Stanley
India
SNEHA Malwani
slum in
Mumbai
A 3-year
comprehensive
program consisting of
home vistis,
behaviour change,
provision of RuTF
etc.
Address
malnutrition in
1,500
infants/children
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
17
Appendix 1 - Key technical terms • Mid-upper arm circumference (MUAC)20 is the circumference of the left upper arm,
measured at the mid-point between the tip of the shoulder and the tip of the elbow. It is used to assess nutritional status. MUAC is considered the gold standard for CMAM programs around the world.
• Edema21 is the retention of water in the tissues of the body that causes swelling. Bilateral edema is a sign of kwashiorkor, a form of severe acute malnutrition.
• Anthropometry22 is the scientific study of the measurements and proportions of the human body. It is a widely used, inexpensive and non-invasive measure of the general nutritional status of an individual or a population group. The three commonly used anthropometric indices are listed below. Each of these indicators is expressed in standard deviation units from the median of the reference population. MUAC is part of anthropometry and corresponds to weight for height. MUAC of less than 11.5CM corresponds to WFH<-3SD and MUAC 11.6-12.5 corresponds to WFH between -3SD and -2 SD
o Weight-For-Age (WFA) o Height-For-Age (HFA) o Weight-For-Height (WFH) o Mid-upper arm circumference (MUAC)
• Severe Acute Malnutrition (SAM)23 is defined by a very low WFH (standard deviation of less than -3 of the international standard), MUAC less than 11.5 CM24, by visible severe wasting, or by the presence of nutritional oedema. It is a life threatening condition requiring urgent treatment.
• Moderate Acute Malnutrition (MAM)25, also known as wasting, is defined by a WFH with a standard deviation of between -3 and -2 of the international standard or an MUAC of between 11.5 cm cm and 12.5 cm.
• Nutrition Rehabilitation Centre (NRC)26 is a health facility usually set up in a district hospital campus or Community Health Centers. SAM children are admitted to NRCs and provided with medical and nutritional therapeutic care.
• Medical Nutrition Therapy (MNT)27 is a therapeutic approach to treating medical conditions and their associated symptoms via the use of a specifically tailored diet devised and monitored by a professional.
20 http://motherchildnutrition.org/early-malnutrition-detection/detection-referral-children-with-acute- malnutrition/muac.htm 21 http://motherchildnutrition.org/early-malnutrition-detection/detection-referral-children-with-acute-malnutrition/screening-for-acute-malnutrition.html#Bilateral pitting oedema 22 http://nrhm.gov.in/images/pdf/programmes/child-health/guidelines/operational_guidelines_on_fbmc_with_sam.pdf 23 http://www.who.int/nutrition/topics/malnutrition/en/ 24 http://www.factsforlife.org/pdf/stmt_child_growth_sam_final.pdf 25 http://actioncontrelafaim.ca/what-is-acute-malnutrition/types-of-acute-malnutrition/ 26 http://nrcmis.mp.gov.in/NRCConcept.aspx 27 Skipper, Annalynn (2009-10-07). Advanced Medical Nutrition Therapy Practice
• Ready-to-Use Therapeutic Foods (RUTF): RUTF are energy dense, lipid-based micronutrient enhanced pastes used in therapeutic treatment of SAM.28
------------------------------------------------------------------------------------------------------------------------------------------------------------------
Samhita Social Ventures, 502, Atlanta Centre, Sonawala Cross Road, Goregaon (East), Mumbai - 400 063 www.samhita.org [email protected] [email protected]
19
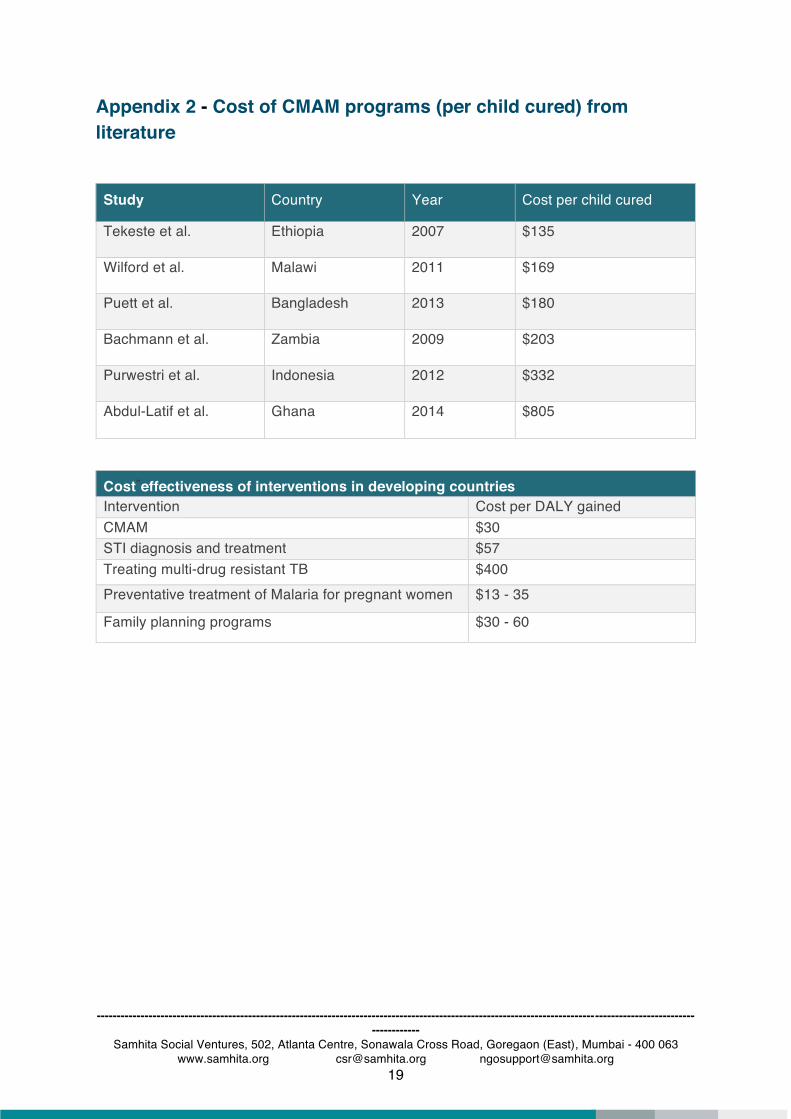
Appendix 2 - Cost of CMAM programs (per child cured) from literature
Study Country Year Cost per child cured
Tekeste et al. Ethiopia 2007 $135
Wilford et al. Malawi 2011 $169
Puett et al. Bangladesh 2013 $180
Bachmann et al. Zambia 2009 $203
Purwestri et al. Indonesia 2012 $332
Abdul-Latif et al. Ghana 2014 $805
Cost-effectiveness of interventions in developing countries
Intervention Cost per DALY gained CMAM $30 STI diagnosis and treatment $57 Treating multi-drug resistant TB $400 Preventative treatment of Malaria for pregnant women $13 - 35
Family planning programs $30 - 60

















