The essential publication for BSAVA members Cat breeds – trophies with hidden problems? P7 Saving the Veterinary Poisons Information Service P4 companion OCTOBER 2008 Great Bustards reintroducing one of Britain’s most impressive birds How to use a direct ophthalmoscope P14
Transcript
The essential publication for BSAVA members
Cat breeds – trophies with hidden problems?P7
Saving the Veterinary Poisons Information ServiceP4
The essential publication for BSAVA members
companionOCTOBER 2008
Great Bustardsreintroducing one of Britain’s
most impressive birds
How to use a direct ophthalmoscopeP14
companion
2 | companion
3 Latest NewsEssential Congress and CPD information
4–6 Poisons ServiceJohn Bonner on securing the future of the VPIS
7–9 Cat BreedsPete Wedderburn examines the hidden problems
10–13 Clinical ConundrumInvestigation of Great Dane with abdominal pain
14–16 How To…Use a direct opthalmoscope
17 Congress SpeakerThere’s going to be a doctor in the house
18–19 Heard on the GrapeVINeSelected discussion from the Veterinary Information Network
20–21 Great BustardsJohn Chitty reports on breeding initiatives
22 PetsaversLatest fundraising news
23–25 WSAVA NewsWorld Small Animal Veterinary Association
26 The companion InterviewKim Hamilton of The Blue Cross
27 CPD DiaryWhat’s on in your area
companion is produced by BSAVA exclusively for its members.BSAVA, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB.Telephone 01452 726700 or email [email protected] to contribute and comment.
The emergency surgical case can be both challenging and rewarding for the veterinary surgeon. There is the
initial adrenaline rush of the unknown emergency coming through the door of the clinic with the challenges of what diagnostics are required followed by developing an effective management plan. That’s why the BSAVA has invited a highly respected specialist from the US and a UK expert to tour Britain in November.
Emergency challengesEmergency work is amongst the most rewarding in practice as you have to think logically and rapidly to assess the patient and develop strategies for stabilising and management, which will also work for more general cases.
The Road Show will cover a wide variety of topics including upper airway and thoracic injuries, abdominal and peripheral soft tissue procedures. Using slides and case presentations we will review a wide selection of topics such as diagnosis and management of peritonitis, non-surgical treatment of auricular haematomas, safe gastrointestinal surgery, easy urethrostomies and appropriate wound management. The course will be of particular value to those new to practice in
order to gain invaluable insight into how to perform soft tissue surgery faster, easier, and more successfully.
SpeakersKaren Tobias is a surgeon and lecturer of international acclaim. A graduate of Illinois and a resident at the Ohio State University, she is currently professor of surgery at Tennessee. John Williams is well known to BSAVA members; in his role as Chair of the Congress Scientific Programme Committee, John knows what it takes to deliver the very best CPD and with his surgical expertise will be able to help attendees get the most from their time in theatre.
Where and whenScotland ■ – Wednesday 12 November Stirling Management CentreSouth West ■ – Friday 14 November Cadbury House Hotel, BristolSurrey & Sussex ■ – Monday 17 November Holiday Inn, Gatwick AirportMetropolitan ■ – Wednesday 19 November Bellhouse Hotel, Beaconsfield
FeesMember: ■ £161.70 exc. VAT(£190.00 inc. VAT)Non-member: ■ £315.00 exc. VAT(£370.13 inc. VAT)
Places are limited, but at the time of going to press a few remain.
For more information you can email [email protected] or call 01452 726700. ■
The BSAVA’s Surgical Emergencies Road Show next month promise expert insight into this important subject
SURGERY CPD
companion | 3
CONGRESS
CONGRESS STARTS HERE
FILM READING FOR THE EMERGENCY CASE
The Advanced Programme for BSAVA Congress was released last month, showcasing another
varied and challenging set of lectures delivered by the most prominent speakers from across the globe. In itself, this is the main reason you should attend – and now there’s a way of spreading your CPD budget even further…
A voucher on the back of the Advanced Programme offers those
delegates registering for ‘whole Congress’ the chance to save a further £25 off their registration when they also pay their 2009 membership subscription before 9 January. That means you would get four days of CPD for just £361.00 (inc. VAT) – which is closer to the figure you’d normally pay for a one-day course on a single subject. Plus, when you are a member you also have access to more than 700 hours of Congress lectures
Now is the time to plan your attendance at BSAVA Congress 2–5 April 2009
Dealing with emergency cases can be nerve-racking for anyone, but particularly for those who do not
have much clinical experience or who have taken a career break. X-rays are often an important diagnostic tool when deciding the next step for the emergency patient.
In November, BSAVA is offering a course that will deal with the practicalities of obtaining diagnostic X-rays in emergency situations, and how to recognise important abnormalities. It is particularly aimed at those who feel they need a bit more confidence in, or to refresh their knowledge of, the emergency situation.
Places are limited but at the time of going to press there were some still available. For more information visit the courses section at www.bsava.com or call 01452 726700 to book your place.
Date: Tuesday 11 NovemberVenue: Woodrow HouseSpeaker: Frances Barr Dr MA VetMB PhD DVR DipECVDI MRCVS
FeesMember: ■■ £220.00 exc. VAT (£258.50 inc. VAT)Non-member: ■■ £350.00 exc. VAT (£411.25 inc. VAT) ■
Image reproduced from BSAVA Manual of Canine and Feline Emergency and Critical Care, 2nd edition
online in our three-year MP3 archive. Though listening to all of them is not a condition of membership!
Members will receive the voucher again in the renewal reminders, so there’s no need to miss out. Just register and pay your 2009 subscription early to take advantage of this discount.
The Scientific Programme can be downloaded online from the Congress section of the website. For more information email [email protected] or for membership enquiries call 01452 726700.
The speaker for the BSAVA Lecture is revealed on page 17. ■
VPISVPIS
4 | companion
For more than 40 years, veterinary surgeons dealing with poisoning incidents have had access to a telephone
helpline run by staff at Guy’s Hospital in London. But the future of the Veterinary Poisons Information Service has been threatened by the closure of the human toxicology
unit where it is based. John Bonner reports on the profession’s campaign to keep the service running
POISONS SERVICE
companion | 5
VPIS
Thanks to an authoritative voice answering queries from veterinary practitioners faced with an incident
involving an unfamiliar poison, many animals have been saved from certain death in the last four decades. However, for the organisation which employs those trained toxicologists – the Guy’s and St Thomas’ NHS Foundation Trust – this veterinary service was a minor distraction from its main purpose of providing advice on human poisoning incidents for NHS staff across the UK.
Consequently, the future of the veterinary service has been in doubt ever since the Health Protection Agency (HPA) announced a reorganisation of its national toxicology information service. In that process, the HPA decided to consolidate the service at four regional centres and the London hospital lost its contract to provide advice to the rest of the NHS. None of these four centres had any background or interest in veterinary toxicology and so it seemed likely that the VPIS would also close after the last NHS caller to the Guy’s unit hung up on 25 July.
ReprieveAt a series of meetings with representatives of the BVA and BSAVA, the Trust’s management were made aware of the importance of the service for veterinary practitioners and they agreed to explore the possibilities for keeping it running. It was eventually decided that at least some of the unit’s staff would be kept on to maintain the VPIS and a number of its other subsidiary activities, such as providing emergency supplies of antidotes and antivenoms.
So do we have a solution?This reprieve is not a long-term solution, says BVA President Nick Blayney, who points out that this agreement is just an interim measure. The only way to guarantee the long-term survival of the VPIS is to ensure that its income covers its running costs. “It became apparent during the discussions that for many years the hospital Trust has heavily subsidised the veterinary service. This is something that they are no longer prepared to do and, as a taxpayer, I must say that I would have to agree with them.”
Making it workSo the hospital trust is working with the veterinary organisations on drawing up a business plan for the VPIS. This will be largely based on the results of a questionnaire survey that will be sent out to members of the BVA and BSAVA. That way the two associations should be able to reach most veterinary practices in the UK. It is essential to find out what level of support the service will have from the profession, what they want the service to provide, and how much they are prepared to pay for it.
Paying for the serviceUp until now practices have been able to access the service run by Guy’s, and a smaller unit at Leeds General Infirmary, by paying an annual subscription based on the size of the practice and the number of vets employed. From April 2008 it was decided that there would be a significant increase in the annual subscription, but an analysis of the unit’s caseload showed there was a need for further refinement to the payments system.
Roughly half of all calls from veterinary practices are made at night and at weekends. As a result of the growth in dedicated out-of-hours (OOH) emergency services covering the work of multiple practices, a disproportionate number of calls are now coming from a relatively small number of clinicians. So it is likely that in future contracts there will also have to be some pay-per-use element.
OOH supportAs those practices that still operate their own emergency services are well aware, there are considerable costs involved in employing staff around the clock, particularly if the European Working Time Directive is more strictly enforced. In their discussions with the Trust’s management, the veterinary representatives have therefore been looking at possible options for reducing costs. One suggestion was to cut the amount of time that the service is available, perhaps down to normal office hours. This option remains a possibility. However, this is viewed with very little enthusiasm by the profession’s representatives, who feel this would greatly diminish the value of the service to its subscribers.
Online optionAnother possibility would be to develop a web-based service, building up a database from information supplied by contributing vets, rather like the Wikipedia internet encyclopaedia. However, such a project would share the limitations of any non peer-reviewed source and any mistakes would begin to erode the confidence that practitioners have with the current system.
POISONS SERVICE
6 | companion
VPIS
| companion
There are also doubts as to whether such a website would eliminate the need to have professional toxicologists on permanent stand-by. “A lot of the questions that veterinary surgeons want to ask are about issues that are not very well covered in the scientific literature. It often needs the professional expertise of these toxicologists to extrapolate from other information and to identify possible red herrings. The situations that they are dealing with may be tricky because the available clinical history is often patchy”, says Nick Blayney.
ChallengesFortunately, some of the challenges facing those responsible for reorganising the VPIS are much simpler. One task will be to set up the sort of administration system needed to
track enquiries and bill the clients. This is obviously something that exists in every veterinary practice around the country, yet because of the history of the service and the ad hoc manner in which Guy’s staff began answering queries from veterinary practitioners, such a system has not been considered until now.
The Trust’s management will also need to decide what it feels is a reasonable economic return for the service. Whilst there doesn’t seem to be any intention for the service to have to become a significant profit generator, the BVA and BSAVA recognise that it has to be viable and needs to develop margins that make the service sustainable in the longer term.
Joint enterpriseAs the Trust has made a commitment to continue providing the service, this gives it a much more certain future than some of the options being discussed at an earlier stage of the negotiations. The two sides did consider whether another organisation could be given the responsibility of running the service, perhaps one of the veterinary schools or even the BVA and BSAVA themselves. Maintaining the existing arrangement has avoided the need for complicated negotiations on the ownership and valuation of the information stored on the VPIS database. Veterinary surgeons have always been more diligent than their NHS colleagues in providing feedback to the
service on the results of cases. Therefore, both sides acknowledge that the service is in many respects a joint enterprise between the VPIS staff and its subscribers.
A way aheadThe veterinary profession has agreed to help the Trust identify and develop new sources of income. One of its current activities is as the ‘key holder’ for double-blind clinical trials being conducted by the pharmaceutical industry. If any adverse events occur, the unit’s staff can intervene to protect the safety of participants without the need to abandon the trial. So one area that the Trust will be looking at is to develop an even closer working relationship with companies in the industry, Mr Blayney suggests.
One final question that the profession itself will have to answer is a simple one – who exactly will be paying for the service? “We in the veterinary profession have always been very bad at charging for telephone advice. But if their animal appears to have been poisoned and a client rings up your practice and asks for help, then you have immediately assumed legal responsibility for that case. If the practice rings up the VPIS it will incur a cost and the practice should be able to pass that on to the client. It is expected that a lawyer will charge the client for telephone advice – it is something that we should be considering too.” ■
companion | 7
PEDIGREE CATS
companion | 7
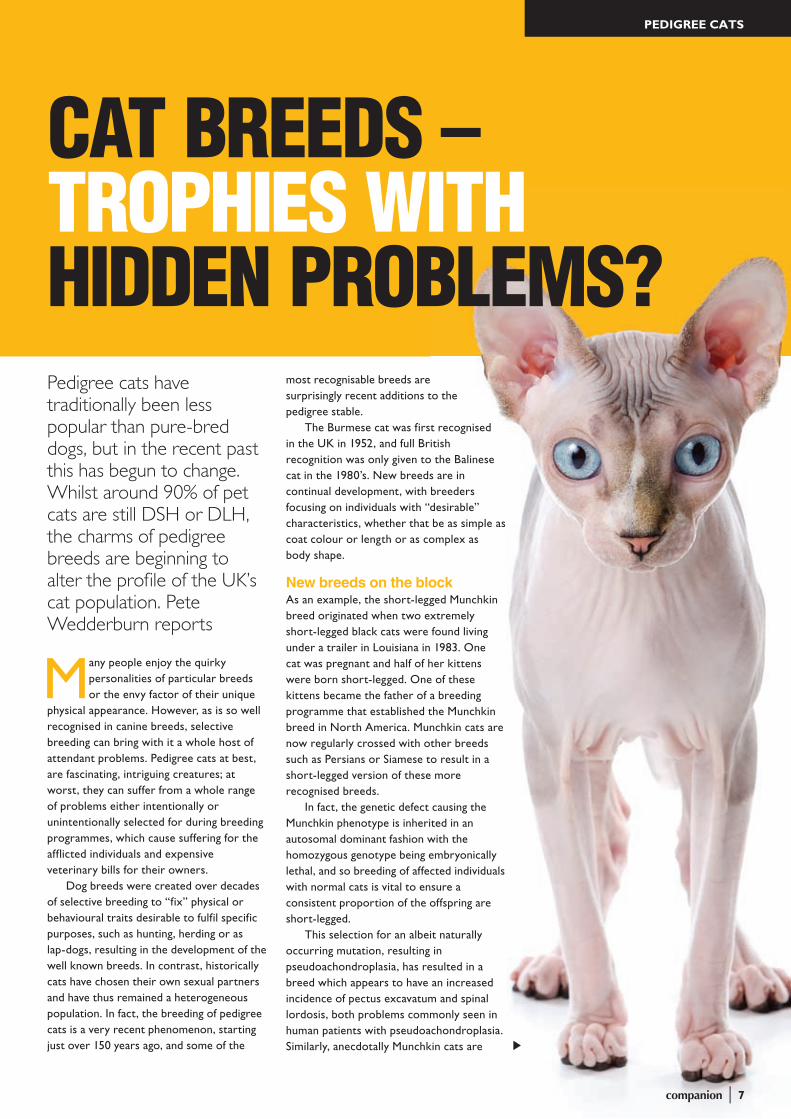
CAT BREEDS – TROPHIES WITH HIDDEN PROBLEMS?Pedigree cats have traditionally been less popular than pure-bred dogs, but in the recent past this has begun to change. Whilst around 90% of pet cats are still DSH or DLH, the charms of pedigree breeds are beginning to alter the profile of the UK’s cat population. Pete Wedderburn reports
Many people enjoy the quirky personalities of particular breeds or the envy factor of their unique
physical appearance. However, as is so well recognised in canine breeds, selective breeding can bring with it a whole host of attendant problems. Pedigree cats at best, are fascinating, intriguing creatures; at worst, they can suffer from a whole range of problems either intentionally or unintentionally selected for during breeding programmes, which cause suffering for the afflicted individuals and expensive veterinary bills for their owners.
Dog breeds were created over decades of selective breeding to “fix” physical or behavioural traits desirable to fulfil specific purposes, such as hunting, herding or as lap-dogs, resulting in the development of the well known breeds. In contrast, historically cats have chosen their own sexual partners and have thus remained a heterogeneous population. In fact, the breeding of pedigree cats is a very recent phenomenon, starting just over 150 years ago, and some of the
most recognisable breeds are surprisingly recent additions to the pedigree stable.
The Burmese cat was first recognised in the UK in 1952, and full British recognition was only given to the Balinese cat in the 1980’s. New breeds are in continual development, with breeders focusing on individuals with “desirable” characteristics, whether that be as simple as coat colour or length or as complex as body shape.
New breeds on the blockAs an example, the short-legged Munchkin breed originated when two extremely short-legged black cats were found living under a trailer in Louisiana in 1983. One cat was pregnant and half of her kittens were born short-legged. One of these kittens became the father of a breeding programme that established the Munchkin breed in North America. Munchkin cats are now regularly crossed with other breeds such as Persians or Siamese to result in a short-legged version of these more recognised breeds.
In fact, the genetic defect causing the Munchkin phenotype is inherited in an autosomal dominant fashion with the homozygous genotype being embryonically lethal, and so breeding of affected individuals with normal cats is vital to ensure a consistent proportion of the offspring are short-legged.
This selection for an albeit naturally occurring mutation, resulting in pseudoachondroplasia, has resulted in a breed which appears to have an increased incidence of pectus excavatum and spinal lordosis, both problems commonly seen in human patients with pseudoachondroplasia. Similarly, anecdotally Munchkin cats are
companion | 7
8 | companion
PEDIGREE CATS
reported to be prone to degenerative joint disease as are their human counterparts.
So a short-legged cat may look cute, but is it fair to deliberately create a breed which is suspected to be likely to develop joint problems, pain and arthritis? This controversy has resulted in The Governing Council of the Cat Fancy in the UK (GCCF), refusing to recognise the Munchkin breed but some other breed associations have had no such qualms.
In other cases, selection for a particular characteristic can result in a breed which needs more attentive care than the norm to prevent disease. The hairless Sphynx needs regular baths to remove the oil that would otherwise be absorbed by hair, and they must be kept indoors because of the dual risks of sunburn in the summer and hypothermia in the winter.
Disease predisposition as a diagnostic aidThankfully most cat breeds have been bred for characteristics which are not in and of themselves a threat to the health of the individual. However selecting for “desirable” characteristics, and the intensive breeding involved, results in an increase in the incidence of undesirable mutations within the breed. In the canine world this has resulted in the spectrum of breed-specific inherited diseases and breed disease predispositions with which the practicing veterinary surgeon is so familiar. As pedigree cats gain in popularity, vets in practice increasingly need to keep themselves up-to-date with the inherited disorders and breed dispositions of the feline world.
One such disease recently surveyed in the UK Somali cat population is pyruvate kinase deficiency. Affected cats suffer from anaemia, both chronically and as dramatic acute bouts, as a result of the reduced lifespan of their erythrocytes. This inherited disease occurs in the DSH but the selective breeding during development of the Somali and Abyssinian breeds unwittingly increased the incidence of the autosomal recessive trait.
Development of a reliable test now allows early identification of affected individuals, and in fact the incidence of the mutant allele was found to be 24% in the sampled population of UK Somalis. The development of this test has allowed the GCCF to put a testing programme in place so that carrier cats are not mated and breeders can take an active role in the control of the disease incidence.
Unfortunately, not all breed-associated diseases are as well understood, nor do they result from single gene mutations; however,
as the increased incidence of specific diseases becomes well characterised in feline breeds, this can provide useful information during the diagnostic process. For example, it has been demonstrated that Siamese cats are at an increased risk of suffering from intestinal adenocarcinoma, being 3–8 times more likely to suffer from this condition than DSH cats. Similarly, the knowledge that Burmese cats are over-represented amongst cats with type 2 diabetes may help clinicians during diagnosis.
Know your stuffThankfully there are numerous resources, which can help the practicing vet. One such source is the FAB website – www.fabcats.org – which provides a treasure-trove of feline information, including more information on the conditions discussed above. One section of the website is dedicated to confirmed and suspected inherited disorders of cats. Many pedigree breeds are listed and within each breed section, the various inherited disorders are colour-coded into those in which:
CAT BREEDS – TROPHIES WITH HIDDEN PROBLEMS?
8 | companion
companion | 9
PEDIGREE CATS
a) The genetics of the condition has been confirmed and/or a genetic test is available.
b) A breed predisposition is recognised and the condition is strongly suspected to be, but as not proven to be, inherited.
c) A potential breed predisposition is possible but evidence is either ancedoctal or based on a single case report.
An expert’s viewSuch databases, of course, need to be interpreted with caution and despite the increased incidence of a given disease within pedigree cats, the majority of cases encountered in veterinary practice will still be DSH or DLH. In fact Dr David Sargan, from the University of Cambridge adds some useful provisos for vets who are newcomers to the FAB list of inherited problems. “In order for veterinary surgeons to give advice on the possible presence or severity of inherited diseases they need to have access to accurate breed-related information and they need to be able to understand the connection between inbreeding and disease incidence.
In addition, they need to recognise that all such lists are unsatisfactory as a means of assessing the genetic health of a particular breed. This is because the length of any breed-related list will depend to a great degree on the level of surveillance within the breed, and vary with the breed’s long term popularity or special factors such as a breed’s usage in medical research. It would be wrong to contend that, for example, the Burmese breed is hugely less healthy than the Tonkinese simply because a higher number of inherited conditions are contained on the FAB list. It is simply that the former is more numerous and has an
active and vigilant breed club, while the latter is less numerous and less studied.
In fact, much of our information would suggest that in very general terms, the less popular a breed, the smaller the available gene pool and the more likely it is (per cat) that there will be inherited disease problems. On the other hand, many (and potentially all) of the inherited diseases known in pedigree breeds may also be found in mixed breed cats but usually with a lower prevalence. Where a breed has had a sudden rise in popularity, there may also be an increased incidence in heritable disease because novice breeders are attracted to the breed and sell kittens for breeding without paying due heed to health.”
Breeding dataDr Sargan goes on to make the point that with the exception of diseases for which open registries or health schemes exist, there is little data on the prevalence of potentially inheritable conditions in different cat breeds, nor on the severity of the disease’s effect on the welfare for the animals. Such data are very hard to collect. There are a few clear examples where abnormalities of conformation or severe inherited conditions have such a high prevalence and/or such severe effects on welfare and morbidity that they constitute a clear reason to counsel prospective cat owners against those breed lines. Indeed Dr Sargan feels strongly that vets should be cautious about making sweeping statements against a particular breed.
However, in most cases the best course of action is to take a less extreme approach. If a breeder has an animal that develops a problem which might be heritable, they should be advised
to withdraw the affected cat from breeding, along with its parents and close relatives.
Vets should counsel prospective owners to check with breeders as to whether or not their breed of cat has a history of heritable conditions, and to request information about possible clinical and/or DNA-based testing schemes. The FAB website and others offer vets, breeders and the purchasing public a useful tool in the effort to achieve a healthy cat population.
The future looks bright given that pedigree cat breeding is becoming popular at the same time as veterinary science embraces molecular medicine and when the breed societies and public alike are increasingly conscious of the ethics and moralities of breeding.
The responsible control of inherited diseases and breed predispositions as pure-bred cats are increasingly seen in the clinic relies on the successful utilisation of all available resources. ■
companion | 9
PEDIGREE CATS
to withdraw the affected cat from breeding,
10 | companion
CLINICAL CONUNDRUM
CLINICALCONUNDRUM
Case PresentationA 6-year-old male neutered Great Dane was presented with a history of lethargy, vomiting and anorexia of 3 days’ duration, and of passing very dark discoloured urine for the previous 24 hours. The dog was ambulatory but lethargic. Abnormalities detected on clinical examination included pyrexia, tachycardia, pale mucous membranes and tachypnoea with mildly increased effort on inspiration. The abdomen was tense and distended, with moderate discomfort on palpation. A urine sample supplied by the owners was a deep red to brown colour (Figure 1).
Ronan Doyle of Davies Veterinary Specialists describes problem-solving in a Great Dane with discoloured urine and abdominal pain
Assimilate a problem list from the clinical history and physical examination
Lethargy■■
Vomiting■■
Anorexia■■
Pyrexia■■
Tachycardia■■
Pale mucous membranes■■
Tachypnoea■■
Abdominal pain■■
Abdominal distension■■
Urine discoloration (red/brown)■■
Clinical signsThe majority of these clinical signs are non-specific and could relate to a wide variety of diseases in a range of organ systems. However, urine discoloration and abdominal distension have a defined number of differential diagnoses, and problem-solving on these aspects of the patient’s presentation is therefore likely to be most fruitful for achieving a diagnosis.
What are the possible causes of the urine discoloration and how can the underlying cause be further ascertained?
The presence of red, brown or black ■■
urine suggests the presence of blood, free haemoglobin, myoglobin or bilirubin. It is important to remember that urine
dipsticks do not differentiate between myoglobin, haemoglobin and blood.Spinning the sample and assessing the ■■
urine sediment will help differentiate blood from free haemoglobin, myoglobin or bilirubin. Spinning a haematuria sample will result in the sample separating, and large numbers of red blood cells should be evident in the sediment on microscopy.
If the urine is still discoloured after ■■
spinning, assessment of the plasma colour will help differentiate the cause further.Pink plasma is suggestive of ■■
haemoglobinaemia and yellow plasma is suggestive of bilirubinaemia. In myoglobinuria the plasma will be clear, as myoglobin is not significantly protein-bound and is filtered by the kidneys. Another possibility if the plasma is clear is haemoglobinuria due to lysis of red blood cells in an old urine sample.
Figure 1: Discoloured free-catch urine sample
companion | 11
CLINICAL CONUNDRUM
In this case, assessment of the urine and ■■
plasma indicated a haemoglobinaemia causing the haemoglobinuria (Figure 2). Haemoglobinaemia results from intravascular haemolysis, which is associated with immune-mediated haemolytic anaemia, parasite-mediated haemolysis, drug-mediated haemolysis, haemolysis as a result of hypophosphataemia, inherited membrane disorders and microangiopathic haemolysis.Further refinement of this differential ■■
diagnoses list requires haematological and biochemical evaluation.
What are the possible causes for the abdominal distension and how can this be further evaluated?
The abdomen can be distended by fat, ■■
fluid, gas or organ enlargement. Fat accumulation may be due to obesity.Fluid and gas accumulation may be ■■
intraperitoneal (as with septic peritonitis) or intraluminal (as with gastric dilatation and volvulus, GDV).Solid organ enlargement can be a ■■
consequence of neoplastic conditions or due to congestion, as with hepatomegaly with right-sided heart failure.Further evaluation is by physical ■■
examination (palpation of a fluid wave or an enlarged mass) and abdominal radiography and/or ultrasonography, possibly followed by abdominocentesis or fine-needle aspiration.
Laboratory and diagnostic imaging resultsHaematology revealed a regenerative anaemia with a haematocrit of 28% (just below bottom of the reference range) and a
moderate neutrophilia. The plasma was pink, consistent with intravascular haemolysis. A Coombs’ test and an in-saline agglutination test to assess for antierythrocyte antibodies (seen in immune-mediated haemolytic anaemia) were negative.
Platelet numbers were adequate, and prothrombin and activated partial thromboplastin (clotting) times were normal. Serum biochemical testing revealed moderate elevations of a number of parameters but interpretation of these was complicated by the haemolysis, which impairs the ability of automated biochemistry machines to measure blood analytes using colorimetric methods.
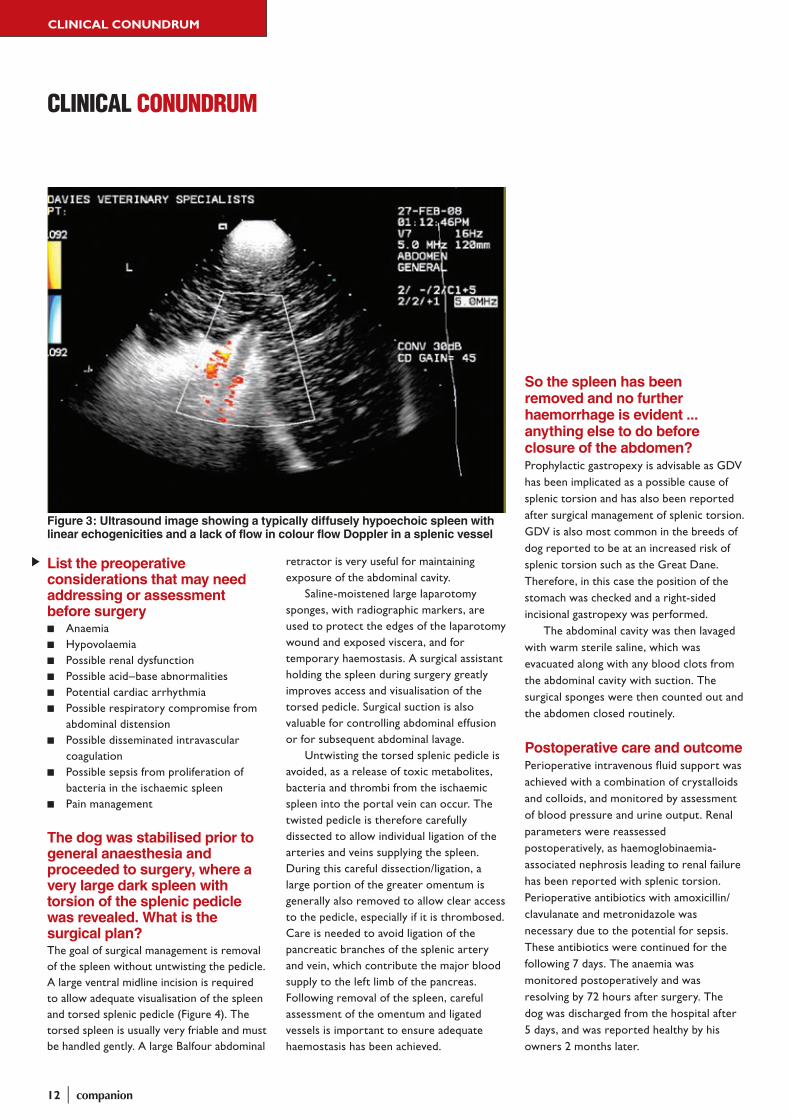
Abdominal radiographs were not taken but abdominal ultrasonography was performed. This revealed a markedly enlarged hypoechoic spleen with linear echogenicities (often described as ‘lacy’ appearing parenchyma). No flow was detected in the hilar splenic vessels on Doppler assessment (Figure 3). The mesentery in the hilar region was hyperechoic. There was a minimal amount of free abdominal fluid present.
A presumptive diagnosis of a splenic torsion causing intravascular haemolysis was made and a plan was formulated to stabilise the dog prior to exploratory midline laparotomy.
Figure 2: Spun urine (left) and blood (right) samples in microhaematocrit tubes. Note the pink colour of the plasma on the right, indicative of haemoglobinaemia and therefore haemoglobinuria
12 | companion
CLINICAL CONUNDRUM
CLINICAL CONUNDRUM
List the preoperative considerations that may need addressing or assessment before surgery
coagulationPossible sepsis from proliferation of ■■
bacteria in the ischaemic spleenPain management■■
The dog was stabilised prior to general anaesthesia and proceeded to surgery, where a very large dark spleen with torsion of the splenic pedicle was revealed. What is the surgical plan?The goal of surgical management is removal of the spleen without untwisting the pedicle. A large ventral midline incision is required to allow adequate visualisation of the spleen and torsed splenic pedicle (Figure 4). The torsed spleen is usually very friable and must be handled gently. A large Balfour abdominal
retractor is very useful for maintaining exposure of the abdominal cavity.
Saline-moistened large laparotomy sponges, with radiographic markers, are used to protect the edges of the laparotomy wound and exposed viscera, and for temporary haemostasis. A surgical assistant holding the spleen during surgery greatly improves access and visualisation of the torsed pedicle. Surgical suction is also valuable for controlling abdominal effusion or for subsequent abdominal lavage.
Untwisting the torsed splenic pedicle is avoided, as a release of toxic metabolites, bacteria and thrombi from the ischaemic spleen into the portal vein can occur. The twisted pedicle is therefore carefully dissected to allow individual ligation of the arteries and veins supplying the spleen. During this careful dissection/ligation, a large portion of the greater omentum is generally also removed to allow clear access to the pedicle, especially if it is thrombosed. Care is needed to avoid ligation of the pancreatic branches of the splenic artery and vein, which contribute the major blood supply to the left limb of the pancreas. Following removal of the spleen, careful assessment of the omentum and ligated vessels is important to ensure adequate haemostasis has been achieved.
So the spleen has been removed and no further haemorrhage is evident ... anything else to do before closure of the abdomen?Prophylactic gastropexy is advisable as GDV has been implicated as a possible cause of splenic torsion and has also been reported after surgical management of splenic torsion. GDV is also most common in the breeds of dog reported to be at an increased risk of splenic torsion such as the Great Dane. Therefore, in this case the position of the stomach was checked and a right-sided incisional gastropexy was performed.
The abdominal cavity was then lavaged with warm sterile saline, which was evacuated along with any blood clots from the abdominal cavity with suction. The surgical sponges were then counted out and the abdomen closed routinely.
Postoperative care and outcomePerioperative intravenous fluid support was achieved with a combination of crystalloids and colloids, and monitored by assessment of blood pressure and urine output. Renal parameters were reassessed postoperatively, as haemoglobinaemia-associated nephrosis leading to renal failure has been reported with splenic torsion. Perioperative antibiotics with amoxicillin/clavulanate and metronidazole was necessary due to the potential for sepsis. These antibiotics were continued for the following 7 days. The anaemia was monitored postoperatively and was resolving by 72 hours after surgery. The dog was discharged from the hospital after 5 days, and was reported healthy by his owners 2 months later.
Figure 3: Ultrasound image showing a typically diffusely hypoechoic spleen with linear echogenicities and a lack of flow in colour flow Doppler in a splenic vessel
companion | 13
CLINICAL CONUNDRUM
DiscussionSplenic torsion occurs when the spleen rotates around its vascular pedicle, leading to obstruction of the splenic veins and severe splenic congestion. The splenic arteries subsequently become thrombosed, leading to infarction and ischaemic necrosis of the spleen.
Although most commonly occurring in association with GDV, splenic torsion can also occur as an isolated event. Isolated splenic torsion usually develops in large deep-chested breeds, especially the Great Dane and German Shepherd Dog, with a predominance of males over females. The pathogenesis of isolated splenic torsion is unclear but it is thought that it may be secondary to repeated episodes of gastric
dilatation and partial volvulus, which may cause splenic congestion or splenic hypermobility. Increased physical activity may accentuate this displacement, leading to torsion.
Splenic torsion can be an acute condition with significant abdominal discomfort and major systemic signs, or can present as a more chronic condition with non-specific signs such as vomiting, anorexia, depression, intermittent abdominal pain, abdominal distension, polyuria and polydipsia, and weight loss.
Haemoglobinuria is commonly reported with splenic torsion, possibly as a consequence of intrasplenic or intravascular haemolysis, although the exact mechanism for this is unclear. A potential complication
Figure 4: Intraoperative view of the enlarged dark spleen covered in omentum with torsion of the splenic pedicle
associated with haemoglobinaemia is the development of renal failure due to a haemoglobinuric nephrosis.
Haematological abnormalities include anaemia, leucocytosis with neutrophilia and thrombocytopenia. Biochemical findings are non-specific, with elevations in serum alkaline phosphatase most common. Elevated pancreatic enzymes are also possible if there is compromise to the pancreatic branches of the splenic artery.
Abdominal radiography findings include: a mid-abdominal mass; absence of a normal splenic silhouette; displacement of other abdominal organs; decreased abdominal detail (secondary to abdominal effusion); and intrasplenic gas accumulation (from proliferating bacteria).
Ultrasonography of the abdomen is an excellent tool and can be used to confirm splenic torsion. Typical findings include generalised splenomegaly, distended splenic veins and a diffuse hypoechoic pattern.
Doppler ultrasonography can demonstrate the absence of blood flow through the splenic vessels of the hilus (see Figure 3). Hyperechoic mesentery is usually evident at the hilus, extending between the hilar vessels and the parenchyma.
Surgical management by splenectomy without untwisting the pedicle is necessary. These patients may require aggressive stabilisation prior to surgery with fluid therapy supplemented by colloids or blood products as necessary. As with other procedures involving the spleen, careful monitoring for cardiac arrhythmias perioperatively is necessary with institution of antiarrhythmic treatment if clinically relevant problems develop. Dogs with appropriately managed splenic torsion should carry a good prognosis. ■
14 | companion
HOW TO…
USE A DIRECT OPHTHALMOSCOPE
HOW TO…
In theory, the direct ophthalmoscope is simple to use. It provides an upright, magnified and real image. Its primary use
is for examination of the ocular fundus, although it also allows magnified examination of anterior ocular structures, including the vitreous, lens, anterior segment, ocular surface and eyelids.
In practice, however, many veterinary surgeons lack confidence when using a direct ophthalmoscope. This is in part due to perceived difficulties in distinguishing normal from abnormal findings. In addition, there is unfamiliarity with the instrument itself. The aim of this article is to summarise the main features of a direct ophthalmoscope and to review its use in clinical practice.
Choice of modelThere are a number of manufacturers of direct ophthalmoscopes, including Welch-Allyn, Neitz and Keeler. Rechargeable or battery options are available. The choice of direct ophthalmoscope is primarily one of personal preference, and as such it may be helpful to ‘road test’ a few models prior to purchase.
Key featuresFigure 1 shows the observer and patient aspects of a typical direct ophthalmoscope head. Its main features include the following:
A brow rest – the head of a direct ■■
ophthalmoscope is ergonomically designed to fit comfortably against the observer’s orbital rim. Whenever a direct ophthalmoscope is in use, the brow rest should always be in contact with the observer’s brow. Compare looking through the eyepiece of the ophthalmoscope with looking through a keyhole; the closer you get, the greater the field of viewAn eyepiece – in which lenses of varying ■■
strengths (dioptres) can be inserted by means of a flywheelFilters – to supply white, red-free and ■■
cobalt blue light
– White light is used for most applications
– ‘Red-free’ light (which appears green in colour) is designed to filter out red light, allowing the examiner to distinguish retinal haemorrhage from pigment. Blood appears black under the red-free light; pigment brown
– Cobalt blue enhances fluorescence after application of fluorescein dye
Variable aperture settings – the variety ■■
of settings depends on the model, but may include wide, intermediate and narrow beam, graticule and slit beam (Figure 2)
David Gould, Head of Ophthalmology at Davies Veterinary Specialists, describes the proper use of this often ignored piece of equipment
Figure 1: Observer and patient aspects of a direct ophthalmoscope head. 1 = brow rest; 2 = eyepiece/illumination mirror and dust cover; 3 = filter settings; 4 = aperture settings; 5 = flywheel/ lens magazine; 6 = quick-step swing (+/– 20D); 7 = rheostat
companion | 15
HOW TO…
– A wide beam is most commonly used in practice, and maximises the field of view through the ophthalmoscope
A narrow beam is useful for small pupils, ■■
to reduce light reflection from the irisThe graticule can be used to roughly ■■
size a fundic lesion by comparing it to the size of the optic nerve headThe slit beam is useful for determining ■■
whether a fundus lesion is a depression (e.g. coloboma, optic disc cupping) or an elevation (e.g. retinal detachment, optic disc swelling). It can also be used to assess anterior chamber depth, and to identify aqueous flareA lens magazine – this provides lenses ■■
of varying focusing powers, usually by means of a flywheel– Zero dioptres (0D) is the default lens
setting, assuming that both examiner and patient are emmetropic (i.e. have normal eyesight)
– Positive dioptre lenses (typically +1 to +20D) are typically represented by black or green numbers and allow the examiner to focus progressively anteriorly, usually in single dioptre steps
– Negative dioptre lenses (–1 to –20D) are typically represented by
red numbers and allow the examiner to focus progressively posteriorly, usually in single dioptre steps. They are used for identifying optic disc cupping or colobomata
– Some models have an additional ‘quick step’ swing of ± 20D. This is not used commonly in clinical veterinary practice, although the +20D lens can be useful when examining for the eyelids, where it provides approximately 2X magnification. This can aid visualisation of small eyelid lesions such as distichia or ectopic cilia
A light source and rheostat – the light ■■
source is reflected out of the eyepiece towards the patient, directly along the direction of view, by means of a mirror within the eyepiece. The rheostat allows variation in light intensity
Distant direct ophthalmoscopyThis technique is mostly used for identifying cataracts, and for distinguishing cataract from age-related nuclear sclerosis. However, it will identify any opacity in the visual axis. This includes mucus and hairs on the cornea, corneal ulcers and other corneal lesions, and opacities within the vitreous.
Set the ophthalmoscope lens magazine ■■
to zero dioptres (0D), stand an arm’s length away from the patient and look at the tapetal reflection through the ophthalmoscope (Figure 3). Remember to use the brow rest. Any opacities will appear black against the tapetal reflection (Figure 4)You can localise lesions within the eye ■■
using the technique of parallax: whilst viewing the opacity through the ophthalmoscope, move to the left and then to the right and observe whether the opacity appears to move with you or against you. Anterior opacities (e.g. corneal lesions, anterior capsular cataracts) will appear to move in the opposite direction to you, whilst posterior opacities (e.g. posterior cataracts, vitreal opacities) will appear to move in the same direction
Close direct ophthalmoscopyClose direct ophthalmoscopy is primarily used to examine the ocular fundus. It provides around 15X magnification but at the expense of a small field of view (around 5–10 degrees). The small field of view means that performing a thorough fundus examination can prove challenging. Some tips to aid visualisation are as follows:
Before you use it to examine a patient, ■■
check that the ophthalmoscope is in good working order. Switch it on, turn the rheostat to maximum, set the lens magazine to zero dioptres (0D) and set the aperture to the wide angle setting. A bright, circular beam of light should be emitted (sometimes the flywheel can catch midway between lenses, cutting off a portion of light, or the dust cover may partly obstruct the light beam).
1 2 3 4 5Figure 2: Aperture settings for a direct ophthalmoscope. 1. Wide angle 2. Intermediate angle 3. Small angle 4. Graticule 5. Slit
Figure 3: Distant direct ophthalmoscopy
Figure 4: With distant direct ophthalmoscopy, cataracts appear dark when viewed against the bright tapetal reflex
16 | companion
HOW TO…
USE A DIRECT OPHTHALMOSCOPE
Look through the eyepiece, ensuring that the brow rest is used. The view through the ophthalmoscope should be clear – use it to look around the roomApply a mydriatic eye drop to dilate the ■■
pupil of the patient prior to examination. Tropicamide 1% is effective within around 10 minutes, has a maximum effect around 30 minutes and lasts 2–3 hours. Atropine should be avoided, especially in cats, in which it induces excess salivationPerform ophthalmoscopy in a darkened ■■
room to minimise light reflectionSet the rheostat to low or mid intensity ■■
when examining the fundus – using a low intensity of illumination will maximise patient comfort and cooperationUse the brow rest■■
Get close to the patient (‘looking ■■
through a keyhole’). The ophthalmoscope should be around 1–2 cm from the patient’s eye. Ideally, use your right eye to examine the patient’s right eye, and your left eye to examine the patient’s left eye. This will help to avoid obstruction of view by the patient’s nose (Figure 5)Try to perform an organised ■■
examination of the fundus:1. Identify the optic nerve head. In most
patients it is located marginally below the midline, and slightly medial. If the optic nerve head appears out of focus then rotate the lens magazine clockwise or anticlockwise in single dioptre steps until the image becomes clear.
Assess size, shape and colour of the optic nerve head, and compare left and right sides. Note that there is significant normal variation in the dog, less so in the cat
2. Examine the superficial retinal blood vessels. In general, the venules are wider and darker than the arterioles.The normal canine fundus contains 15–20 arterioles and 3–5 venules that drain into a venous circle on the optic nerve head (Figure 6). In the feline fundus, three major pairs of arterioles and venules emerge from the edge of the optic nerve head (Figure 7). In the dog, there is considerable normal variation in the degree of blood vessel tortuosity, much less so in the cat
3. Examine the tapetal fundus, located dorsal to the optic nerve head. Using a low intensity of illumination will allow easier identification of abnormalities such as tapetal hyper- or hyporeflectivity
4. Examine the dark non-tapetal fundus, located ventral to the optic nerve head. Abnormalities may include areas of hypo- or hyperpigmentationRemember that the small field of view ■■
through the ophthalmoscope means that a thorough fundus examination takes some timeIf you are myopic or hyperopic (short- ■■
or long-sighted, respectively) then adjusting the lens magazine to your prescription will allow you to use the ophthalmoscope without having to wear your glasses. For example, if you are –2D myopic then adjust the lens magazine to –2DAttempting an ophthalmic examination ■■
on a patient under general anaesthetic is seldom rewarding. Rotation of the globes under anaesthesia makes intraocular visualisation particularly difficult. A combination of patience and gentle restraint is usually sufficient to allow ophthalmoscopy in the vast majority of patients.
Examining anterior ocular structuresThe direct ophthalmoscope can also be used to examine structures anterior to the retina, by utilising the positive dioptre setting on the lens magazine. Approximate
Figure 7: The normal feline ocular fundus
Figure 6: The normal canine ocular fundus
settings for examining structures of the canine eye are as follows:
Posterior lens: +8D■■
Anterior lens: +12D■■
Cornea and eyelids: +20D■■
SummaryThe direct ophthalmoscope is a versatile piece of equipment that is perhaps underused in general veterinary practice. As well as using it for detailed fundus examination, it is also helpful for identification and localisation of opacities in the visual axis, most notably cataracts. In addition it allows magnified examination of structures anterior to the retina, including the lens, cornea and eyelids. Familiarising yourself with the functions of your direct ophthalmoscope, and regular practice with its use, should increase your confidence in examining eyes and in diagnosing ophthalmic abnormalities. ■
Figure 5: Close direct ophthalmoscopy
companion | 17
CONGRESS
The full social programme will be revealed in November’s edition of companion. The Advanced Programme is available online now at www.bsava.com
AN EXTRA SPECIAL SPEAKER
The BSAVA Congress Lecture for 2009 is being presented by a doctor who is as comfortable on the comedy circuit and presenting his own television show as he is in his surgery
The list of Congress speakers for the special BSAVA lecture includes some difficult acts to follow. In recent
years Tanni Grey-Thompson, Simon King and, most recently, Susan Greenfield have entertained Congress delegates on Thursday afternoon with inspirational, fascinating and revealing stories of their own experiences.
However, for 2009 BSAVA has invited a man with his own very special take on medicine, someone who has been described by the Guardian newspaper as “One of the most entertainingly subversive people on the planet.”
Phil Hammond is a GP, writer, journalist, broadcaster, campaigner and comedian. He is also Lecturer in Medical Communication at Bristol Medical School.
After an education at Eastbourne College, Hammond qualified as a doctor in 1987 from St Thomas’ Hospital Medical School, University of London.
He first came into the public spotlight writing for The Independent, where he emphasised patients’ rights and gave away some of the ‘below-stairs’ secrets of the NHS. As well as appearing on Channel 4’s longest running programme, Countdown, Hammond has written Private Eye’s medical column, ‘Doing the Rounds’, since 1992 under the pseudonym ‘MD’.
As a campaigning journalist, he was first to expose the problems of paediatric heart surgery in Bristol, which led to the largest Public Inquiry in British medical history. Hammond gave evidence to both phases of the Inquiry, and has exposed many other examples of patchy quality care as a journalist and as a presenter of BBC2’s award-winning and highly controversial programme Trust Me I’m a Doctor. His comedy credentials include being twice selected for the Perrier Pick of the Fringe in Edinburgh.
All delegates are invited to hear Phil Hammond’s talk on Thursday in the ICC where prizes will also be presented to the winners of the Petsavers photography competition. ■
BSAVA Congress 20092–5 April ICC/NIA BirminghAm
A AA A A
18 | companion
VIN
Discussion CreatorPepper is a 2 year old St. Bernard who was shot in the face at point blank range with bird shot; the result of a neighbourly dispute over a few chickens. The blast obliterated the lateral wall of her nose, hitting the hard palate, with most of the pellets ricocheting off over the hard palate into her nose, soft palate and throat. Part of the hard palate, from the first incisor to the 4th premolar was fractured. The 4th premolar was also blown to bits.
After stabilization with pain control and IV fluids I removed the root fragments of her PM4 and wired the hard palate back in place and closed the oronasal defects with gingival flaps. I did not try to reconstruct her nose yet as it was not clear which tissue was still viable. Now, one week later, a large portion of her nose has sloughed off leaving a big open defect. My palatal repair is holding, although a few areas of my flaps also dehisced and will need to be redone.
The question is: how do I rebuild her nose in such a way that air passage is not impeded and the end result is cosmetically acceptable to her owners? The problem is that much of the frontal/nasal bone was obliterated. I was wondering if it would be possible to incise her lip along the gingival margin. Split it so the oral mucosa could form the new nasal mucosa, insert a titanium mesh for support and use the outside of the lip to close the skin on top of the mesh over her nose? Other suggestions are welcome.
The Veterinary Information Network brings together veterinary professionals from across the globe to share their experience and expertise. At vin.com users get instant access to vast amounts of up-to-date veterinary information from colleagues, many of whom who have specialised knowledge and skills. In this regular feature, VIN shares with companion readers a small animal discussion that has recently taken place in their forums
.comGRAPEVINEheard on the
companion | 19
VIN
All content published courtesy of vin.com. The names of participants have been removed from this feature. For more details about the Veterinary Information Network visit vin.com. As VIN is a global veterinary discussion forum not all diets, drugs or equipment referred to in this feature will be available in the UK, nor do all drug choices necessarily conform to the prescribing rules of the Cascade. Discussions may appear in an edited form.
Reply 2These cases do remarkably well by themselves. In that the left nostril is functional, I would not do anything drastic until secondary healing has taken place (in about two months) then consider reopening a new “nostril” if indicated.
Discussion CreatorUpdate on Pepper: after all your input I was able to convince her owners to hang in there for another 2 weeks. Pepper is doing much better after we removed most of the dead tissue. She is eating with gusto, drinking, wagging her tail and is almost back to normal except for the gaping hole in her head. The owners now want to wait a few more weeks before deciding where to go with further surgery. Thank you all for your input, much appreciated.
Reply 5I would definitely wait until all the “die back” has settled down so you know what you’re working with before trying flaps. If the dog is functional, the owners should be encouraged to cope with the appearance and you should just leave things nasal alone. Otherwise I would do the pedicle flap to close. Let your palatal stuff settle/heal and then try to close any defects. Make sure there isn’t non-vital bone underneath. And no tension on the sutures!
Reply 4An end result that is cosmetically acceptable to her owners? The owners may need to adjust their expectations. They should be thrilled that their pet survived a full-face blast from a shot gun – that in itself seems miraculous. And no ocular damage! Wow. I would say anything that results in a live pet at the end of it should be considered a successful outcome. Anything beyond that is a bonus. I would be hesitant to get too aggressive trying to re-create a face as you may end up compromising a great
deal more tissue with a much larger defect in the end.
Discussion CreatorThank you for all your suggestions. There’s a recommendation to wait two months before attempting a further repair of the nose, but I assume this does not apply for the oro-nasal defects that are still present? When I wired the palate back in place I did create flaps to close these defects. Most of my flaps held, but small areas dehisced. Does everyone agree the suggestion to wait two months or go for a repair once debridement is complete? Her owners are quite grossed out by the way the wound looks and would like something done ASAP.
Reply 3I agree with the suggestion for a cheek advancement flap. Be careful when working around the maxillary bone – leave the periosteum alone since you need it to heal that large crack in the palate – which looks like it exits through the alveolar ridge distal to the canine tooth. Warn the owner about sunburn in the next few months – while the skin is healing it will be susceptible.
Reply 1The easiest way to get skin coverage there, I think, would be to advance a flap from the muzzle/cheek. It’ll mess up her colour scheme, I’m afraid, but it’ll give you what you need. For the first layer I would do what you’re thinking about: elevate a mucosal flap from inside the lip over the
premaxilla, with the base of the flap located dorsally. Make an incision where the lip meets what’s left of the bottom of the nasal cavity on that side so that you can rotate the flap up to suture to the tissue at the top of the open nasal cavity. Then advance the skin flap over that. If you use the titanium mesh, it would go between the two layers.
20 | companion
PUBLICATIONS
GREAT BUSTARDS
John Chitty, co-editor of the BSAVA’s avian manuals, reports on a programme to reintroduce one of Britain’s most impressive birds
Bustard Group (GBG) was formed 10 years ago to attempt this reintroduction and to assist in Great Bustard research and conservation throughout Europe.
From Russia with chicksProbably the largest population is near the southern Russian city of Saratov, close to the border with Kazakhstan. There are many problems with bird losses due to powerline collisions and nest disturbance during cultivation. Various methods have been tried to save them (e.g. covering nests, leaving strips of uncultivated land around them) yet all failed, with the nests being predated by corvids or foxes within 48 hours.
The local Institute of Ecology is licensed to take a limited number of eggs from disturbed nests for captive rearing. Rearing is performed using isolation rearing techniques similar to those used in the Whooping Crane projects, to prevent the birds becoming
imprinted on humans. For the last five years the GBG has been allowed to take chicks hatched from eggs from disturbed nests for reintroduction to the UK. The impact on the Russian population is zero, since the eggs that are taken would have been predated. It is hoped that enough chicks will be brought in each year to enable a self-sustaining population to become established in the UK.
The chicks enter quarantine for a compulsory 30-day period before being placed in a release pen. This should mirror their natural behaviour where birds have a home patch where they hatch. They will then disperse before returning each year for breeding. Great Bustards are a lekking species: males and females congregate, males put on a spectacular display together and the females then choose the best.
Veterinary consultantMy role is to see that the imported birds will be fit for release. Also, they must not bring in infectious diseases that could cause problems to wild or captive birds in the UK.
I travel to Russia each year to check the chicks prior to import. The chicks are reared in a biosecure unit at the Institute’s Field Station in a village called Diakovka. This small village is slightly closer to the Kazakhstan border than to Saratov and it takes a 4-hour flight to Moscow, then an 18-hour train journey before a 3-hour drive to get there.
Post-mortem examinations are performed on any eggs that have failed to hatch as well as on any chicks that have died – we must be very careful to ensure that problems do not develop through introduced infection or through management failures. Generally, the only major problem is embryonic death due to
The Great Bustard (Otis tarda) is the world’s heaviest flying bird – older males may weigh over 25 kg.
Although traditionally found in the UK, they became extinct here in 1832. While changes in agriculture were partly to blame, a major reason was shooting – partly for food but mainly for taxidermy. Males in breeding condition are spectacular, and the quickest way to destroy a species is to wipe out one sex.
Although the Great Bustard is not rare (it is still found in Spain, Germany, Hungary and Russia), the populations are under threat. The setting up of new populations, therefore, provides an additional ‘safety net’ for the species.
The main UK population was on the open grassland of Salisbury Plain. Because of army use and conservation, the Plain is essentially the same now as it was in 1832. As a result, attempts have been made to reintroduce the birds there. The Great
temperature changes or excessive movement of the egg after taking – not surprising given bumpy roads and temperatures frequently over 40°C. Nonetheless hatch rates are usually very high (an exception was 2007 when Spring temperatures during the breeding season reached over 50°C and few local birds bred successfully).
I also check the live chicks, rejecting any birds that appear to be unlikely to be fit for release into the wild. Very few birds have problems – the only major worry occurring in 2005 when a change in feeding resulted in angel wing in many birds (heavy fast-growing flight feathers pull and twist soft growing bones, resulting in deformation of the wings). Birds are tested for avian influenza and paramyxovirus and we are eternally grateful to Ruth Manvell from VLA Weybridge who accompanies us on these trips and undertakes the virological testing.
The other major veterinary task is organising the annual Diakovka barbecue! Food hygienists may be appalled by the facilities and cooking methods, and the Russians are always mystified by the English need to take perfectly good pieces of meat and cremate them in open air, but with liberal quantities of beer and vodka the evening normally goes well and no-one has been ill … yet!
QuarantineThe chicks are brought to the UK after obtaining the necessary CITES and importation licences. They then enter quarantine where they undergo further disease testing – compulsory tests for avian influenza and paramyxovirus, and also faecal tests for parasites, mycobacteria, Chlamydophila, and other potential
pathogens. Other haematological and serological tests are done as deemed necessary. Very few abnormalities have been encountered thus far.
SightingsPrior to release, wing tags and tracking devices are attached. In the first year problems were encountered with the harness fittings: the birds’ flying ability was restricted and we had increased losses due to hitting fences. A few simple adjustments have since been made and the birds have really benefitted and started dispersing as anticipated.
In the second year, birds reached France – the furthest being sighted south of Toulouse (that bird has returned and there have been many sightings of it across southern England). Within the UK there have been bird sightings in Somerset, Gloucester and Cambridge. As the number of released birds increase, so small same-sex flocks have started forming as they would in the wild. This is a huge advantage to the younger birds – as they are released they are recruited into one of these flocks, which considerably reduces their chances of being predated.
In the last two years birds have started moving back to the release site area in Spring and lekking behaviours have been observed. In each of the last two years, one of the females has laid eggs (the first in the UK for over 170 years!). Sadly these have been infertile – unsurprising given how young the males are.
So, things are progressing well and with increasing numbers of birds coming in (we hope to bring back 26 this year) we hope to see this success continue.
The ‘dehumanising’ suit. Hands and feet are covered and the brown and white pattern is designed to reflect the colour distribution on a female bustard. The aim is that young bustards do not associate humans with food. When handling the birds for testing or examination such suits are not worn – therefore bustards should develop aversion to humans rather than imprinting on them
Avian Medicine from BSAVA
International cooperationFor a vet brought up on the edge of Salisbury plain, it has been wonderful to be part of the effort to bring back this bird. Many others are working on this project, both in Russia and the UK, all playing vital roles in rearing, releasing and monitoring.
The Russian people have been extremely friendly, indeed we are probably among the first Brits to visit the area and so achieve near-celebrity status for a brief period each year. The birdwatching round Diakovka is excellent. If anyone would like to know more about the project or make a visit, please visit www.greatbustard.com ■
22 | companion
Improving the health of the nation’s pets
PETSAVERS
PET PICTURES WIN PRIZES
CARDS THAT MAKE A DIFFERENCE
Petsavers will once again be inviting entries to its popular annual photo competition. The theme is ‘Pets at
Holiday Time’ to illustrate how animals are cherished members of the family and enjoy the various seasonal celebrations, such as summer holidays and Christmas, as much as we do.
The competition is open to 3 age ranges: 11 years and under, 12–16 years, and adults over 16. Entry to the competition is through the Petsavers
The festive season is nearer than you think, and this is a great time to consider supporting your favourite
charities, whether it’s buying Christmas cards, gifts or making a donation. Petsavers certainly benefits from our generous supporters at this time – and what ever you do, remember, it all makes a difference in helping the charity carry on its important work to find treatments for diseases of our pets.
The popular Petsavers photographic competition invites submissions from vets and their clients from 3 November – 23 February
Christmas cardsThe Petsavers Christmas cards have some great designs and are popular with both practices and individuals every year. Cards are available in packs of 10 at £4.50 or £7.50 for a selection pack.
Making a donationAn alternative to sending cards is to make a donation to the charity instead of weighing down the postman – just let everyone know your intention and they might think about
doing the same – as well as saving you all that writing and postage.
Placing your orderYou can buy Petsavers Christmas cards as well as our range of notelets by calling 01452 726700 and providing your credit or debit card details, or by visiting the Petsavers website at www.petsavers.org.uk to find out more and download an order form. ■
website at www.petsavers.org.uk from the beginning of November. Enter one photo per person for the chance to win a prize of up to £250 worth of vouchers. The closing date is Monday 23 February.
Telling your clients about the competition and getting them to enter their own images is a great way to introduce them to the charity that supports research into the health problems which affect small animals – and perhaps even their own pets.
Remember – Petsavers studies do not
WIN PRIZES
MAKE A DIFFERENCE
The popular Petsavers photographic competition invites submissions from vets and their clients from
doing the same – as well as saving you all that writing and postage.
from the beginning of November. Enter one photo per person for the chance to win a prize of up to £250 worth of vouchers. The closing
use experimental animals.On Thursday 2 April finalists of the
Petsavers Photo Competition will be invited to BSAVA Congress to be awarded their prizes. The winners in each age group will be announced at Congress, and photos by the finalists will be displayed at the ICC and in the NIA. ■
companion | 23
WSAVA NEWS
DUBLIN CONGRESS HIGHLIGHTS
This year’s WSAVA Congress was held at the Royal Dublin Society (RDS), which was founded in 1731 to
promote the development of agriculture, arts, science and industry in Ireland, and housed on grounds that cover 40 acres in the heart of Dublin. Ireland, the United Kingdom, the USA, Australia, Canada, France and Germany sent more than 100 delegates each, and Eastern Europe was also very well represented.
WSAVA scienceThe scientific programme included 235 Congress lectures (including four State-Of-The-Art Lectures) presented by 75 world-renowned veterinary scientists, covering over 20 disciplines. Oral or poster abstract presentations and three pre-Congress meetings covering veterinary emergency and critical care, feline, and avian medicine complemented the programme. The Animal Welfare track continues as a WSAVA Congress highlight, attracting more attendees each year, with an additional track on hereditary diseases
The beautiful city of Dublin, Ireland, welcomed 2870 attendees representing 86 countries during the 33rd WSAVA Congress in August
organised by the WSAVA Committee, and an update on the tremendous accomplishments of the GI Standardization Group, presented by Dr Robert Washabau.
WSAVA SocialThere was plenty of variety on offer at the lively social events. The Opening Ceremony took place on Thursday at the RDS and featured the dynamic Irish musical group Electric Ceili, opening addresses from a
variety of dignitaries, presentation of the WSAVA Awards, and a parade of Irish dog breeds. A cocktail party followed on the RDS grounds whilst enjoying a live sheepdog trial demonstration and a display from the Irish Pony Club.
Friday night played host to the Gala Evening, which began with a champagne reception in the airy conservatory overlooking the lake on the leafy grounds of the University College Dublin campus, followed by a 5-course banquet at O’Reilly Hall. After-dinner festivities included the passing of the Presidential chain of office from outgoing President Brian Romberg to incoming President David Wadsworth, and culminated in a lively evening of dancing to the sound of ‘Boogie Nights’, Ireland’s top party band.
Attendees of the WSAVA Dublin Congress Gala dinner dance to the sounds of Boogie Nights
24 | companion
DUBLIN CONGRESS HIGHLIGHTS
WSAVA NEWSWSAVA NEWS
WSAVA ASSEMBLY MEETING
The President provided assembly members with updates from a very active WSAVA leadership, including
the Executive Board and various committees, which he highlighted in his Congress Message (featured in September companion).
Team changeIn addition to the passing of the presidential chain of office and retirements of Drs Anne Sorensen as Honorary Secretary, Larry Dee as Immediate Past-President, and Anjop Venker-van Haagen as Scientific Advisory Committee Chair, an election of officers was also held that saw the new WSAVA Executive Board affirmed. The new Board includes (pictured from left to right) Dr Brian Romberg (Immediate Past-President; South Africa), Dr Luis Tello (Vice President; Chile), David Wadsworth (President; UK), Dr Jolle Kirpensteijn (President Elect; Netherlands), Dr Di Sheehan (Honorary Treasurer; Australia)
and Dr Walt Ingwersen (Honorary Secretary; Canada).
New associationsThe assembly members voted in favour of accepting two new full member associations
that included the Montenegro Association of Small Animal Practitioners (MASAP) and the Federation of Indian Small Animal Veterinary Associations (FISAVA; made possible by the membership withdrawal of the Pet Practitioners of Mumbai, who are now members of FISAVA). Also, the Veterinary Emergency and Critical Care Society was voted in as an affiliate member. A number of associations had their membership revoked for lack of subscription dues payment.
WSAVA President Dr Brian Romberg welcomed the Assembly members after a 12-month hiatus since the last assembly meeting in Sydney, Australia on August 19, 2007
On Saturday night, attendees were treated by event sponsor Mérial to a traditional evening of Irish food and Celtic music on the grounds of the historic Trinity College, home of the famous Book of Kells. Guests mingled in an eclectic mix of rooms with their dramatic gothic architecture and decor.
The Closing Ceremony wrapped up
the Congress on Sunday afternoon and featured an engaging presentation highlighting next year’s Brazil Congress, featuring Brazilian dancers.
Great successThe Dublin Congress was a tremendous event, complemented by Congress tours arranged by the Organizing Committee, all
of which will have left attendees with fond and lasting memories.
For more information on the 2008 WSAVA Congress, including a photo gallery, visit www.wsava.org. WSAVA Prime Partner Hill’s and Partners Fort Dodge, Nestle Purina, Pfizer, Novartis and Bayer, who joined the 135 exhibitor strong Exhibition Hall, supported the Congress. ■
WSAVA Executive Board 2008
companion | 25
WSAVA NEWS
WSAVA AWARD WINNERSFull details of award winners are available on the WSAVA website
WSAVA/Waltham International Award for Scientific AchievementThis award is based on outstanding contributions by a veterinarian who has had a significant impact on the advancement of knowledge concerning the cause, detection, cure and/or control of disorders of companion animals. This went to Professor Peter Moore, Department of Pathology, Microbiology and Immunology, School of Veterinary Medicine, University of California, USA.
WSAVA Intervet/Schering Plough International Award for Service to the ProfessionThis award is presented to a person who has given exemplary service in fostering and enhancing the exchange of scientific and cultural ideas throughout the veterinary
small animal world. This went to Professor Marion Horzinek, Department of Infectious Diseases and Immunology, Faculty of Veterinary Medicine, Utrecht University, the Netherlands.
WSAVA/Hill’s Mobility AwardThis award is presented to recognise the outstanding work of a clinical researcher in the field of canine and feline orthopaedic medicine and surgery. Through improvements in the mobility and quality of life of pets, this person’s research has contributed significantly to the well being of pets’ lives and to the human–animal bond worldwide. This went to Professor David Bennett, Institute of Comparative Medicine, University of Glasgow Veterinary Faculty, Bearsden, Glasgow, Scotland.
WSAVA/Hill’s Excellence in Veterinary Healthcare AwardThis award recognises the outstanding work of veterinarians in promoting companion animal healthcare and the family pet–veterinary bond through a special sensitivity
Future WSAVA Congress datesSão Paulo, Brazil – July 21–24, 2009Geneva, Switzerland – June 2–5, 2010Jeju, South Korea – 2011Birmingham, UK – 2012
Dr Hans Klaus Dreier (right) receives the inaugural President’s Award from WSAVA President Dr Brian Romberg at the 2008 Assembly meeting
2012 Congress in UKWSAVA Congress will be back in the UK in the country’s Olympic year, as Birmingham was chosen as the site for the 2012 WSAVA Congress – hosted by the British Small Animal Veterinary Association.
Assembly highlights:Past WSAVA President Dr Hans Klaus ■
Dreier was presented with the inaugural President’s Award for his past and ongoing significant contributions to the WSAVA and international veterinary medicineThe Treasurer’s report acknowledged a ■
difficult 2007 financial year, due in large part to unpaid revenues from member association subscriptions, lack of payment of Congress revenue from Mexico, and loss of sponsorship for some WSAVA Awards. However, with the recently announced Hill’s Prime
Partner sponsorship agreement, 2008 is enjoying healthier financial stability. The revised and more equitable fee structure, voted in at the 2007 Assembly meeting, was readily implemented, with an additional 4.5% subscription increase for 2008 to account for cost-of-living increasesAnnouncement of Hill’s as a long-term ■
Prime Partner providing over 1.5 million dollars in sponsorship over 3 years for a multitude of WSAVA projects and initiatives, including the Congress, various WSAVA Standardization Projects and www.wsava.orgA Continuing Education Committee ■
report thanked industry and member association sponsors and celebrated the past and ongoing successes of WSAVA-sponsored CE in various regions around the world
David Wadsworth presented the ■
results of the WSAVA Strategic Planning sessions, together with time the following morning dedicated for WSAVA member association input and hosted by WSAVA Board members.
Assembly Minutes are available at www.wsava.org ■
to both clients and patients using cutting edge clinical nutrition and advanced medical and surgery techniques.
This went to Professor Carl Osborne, University of Minnesota and Co-Director of the Minnesota Urolith Center, Minnesota, USA. ■
26 | companion
companion INTERVIEW
Kim Hamilton was born and brought up in Coventry where she attended Barr’s Hill Girls Grammar School. After various jobs she went to Citibank, intending to save for a trip around Europe; however, Kim remained there for 22 years. After deciding on a move into the voluntary sector Kim undertook a Sloan Fellowship MSc course at the London Business School, before taking the position of Chief Operating Office at the National Association for the Care and Resettlement of Offenders (Nacro). She has recently been appointed as the new Chief Executive of The Blue Cross
THEcompanionINTERVIEW
Working in the finance and then with ex-offenders seems a long way from animal welfare. What motivated you to work with the Blue Cross?Whilst I can sympathise with the objectives of many charities who do very worthwhile work, there are only a few whose mission I can truly identify and empathise with – The Blue Cross is one of those charities. Their mission of enhancing both animal and human lives through companionship is something I feel very strongly about, therefore the chance to work in this field, and with The Blue Cross in particular, is a once in a lifetime opportunity that I had to explore.
What do you consider to be your most significant achievement?It would be the contribution that I made at Nacro by turning its financial fortunes around and introducing a culture change. The most rewarding aspect is seeing individuals meet their potential when they are given the opportunity to look to the future and be ambitious and brave.
What particular goals have you set yourself at the Blue Cross?To visit all centres and activities within the first few months and meet as many staff on the ground as possible in order to understand the organisation from all perspectives. To clarify what differentiates
The Blue Cross from other animal welfare charities and how we can leverage that to meet the needs of more companion animals, horses and the people that care for them.
Who has been the most inspiring influence on your professional career?My boss in my early days at Citibank, Mike Rice, who taught me about taking chances and risk. He lived by the premise that regret is a feeling experienced when you don’t take an opportunity when it is presented to you and you then wonder what would have happened – whilst if you take an opportunity, you may make mistakes but if so, the consequences are a learning experience.
What is the most significant lesson you have learned so far in life?That life is too short and that during our time here, we should cherish our family and friends because you can never have enough time with them.
What is your most important possession?If, God forbid, my home were burning down, my first thought would be for my partner and our dogs. However, if I had to nominate my most important material possession, it would be my mother’s wedding ring.
What has been your main interest outside work?My main interest outside of work is my family and friends – I never seem to have enough time to spend with them. In recent years I have begun to learn how to fly helicopters; however, as I have not flown for over a year now, I need to find the time to re-take the exams before flying again and gaining a private licence.
If you were given unlimited political power, what would you do with it?Forgive third world debt and introduce global free trade agreements – the combination would go a long way to eradicating global poverty.
What would you like to have done if you hadn’t gone into banking?As a teenager my ambition was to be a PE teacher; however, if I look back now and could choose a different early career path, I would have liked to go into law and perhaps become a barrister. ■
www.bluecross.org.uk
The Blue Cross mission: Provide
care, promote companionship
– enhance animal and human lives.
CPD DIARY
companion | 27
CPDDIARY
6 NovemberThursday
Exploring the true potential of cytologySpeaker Andrew TorranceAfternoon meeting at the Potters Herron Hotel, Romsey. Southern Region.Details from Michelle Stead, telephone 01722 321185, email [email protected]
6 NovemberThursday
Raptor medicineSpeaker Nigel Harcourt-Brown (co-editor of Psittacine Birds)Evening meeting at the Swallow Hotel, Preston. North West Region.Details from Simone der Weduwen, email [email protected]
12 NovemberWednesday
Rabbits – it’s not the teeth or gut, what next?Speaker John Chitty (co-editor of Raptors)Evening meeting at the Park Inn, Llanederyn, Cardiff. South Wales Region.Details from the Chairman or Secretary email [email protected]
12 NovemberWednesday
CPD Road Show: surgical emergencies Speakers Karen Tobias and John Williams (co-editor of Wounds 2e and Abdominal Surgery)Day meeting at Stirling Management Centre, situated within the grounds of the University of Stirling campus. Scottish Region.Details from BSAVA Customer Services, telephone 01452 726700, email [email protected]
13 NovemberThursday
LA calls for SA vets: from pygmy goats to pot-bellied pigsSpeaker Graham DuncansonEvening meeting at the Russell Hotel, Maidstone. Kent Region.Details from Hannah Perrin, email [email protected]
13 NovemberThursday
BVDA CPD – rabbit dentistrySpeaker BVDA Day meeting at Myerscough College, Bilsborrow, Preston. North West Region.Details from Alex Smithson (BVDA), telephone 07887650812, email [email protected]
14 NovemberFriday
CPD Road Show: surgical emergencies Speakers Karen Tobias and John Williams (co-editor of Wounds 2e and Abdominal Surgery)Day meeting at the Cadbury House Hotel, Congresbury, Somerset. South West RegionDetails from BSAVA Customer Services, telephone 01452 726700, email [email protected]
14 NovemberFriday
BVDA CPD – oral surgerySpeaker BVDA Day meeting at Myerscough College, Bilsborrow, Preston. North West Region.Details from Alex Smithson (BVDA), telephone 07887650812, email [email protected]
16 NovemberSunday
Coughing cats and dogsSpeaker Anne FrenchDay meeting at The Novotel, Newcastle. North East Region.Details from Karen Goff, telephone 01924 275249, email [email protected]
16 NovemberSunday
Immune-mediated diseaseSpeakers Nat Whitley and Oliver GardenDay meeting at the Cambridge Belfry, Cambourne. East Anglia Region.Details from Graham Bilbrough, email [email protected]
17 NovemberMonday
CPD Road Show: surgical emergencies Speakers Karen Tobias and John Williams (co-editor of Wounds 2e and Abdominal Surgery)Day meeting at the Holiday Inn, Gatwick. Surrey and Sussex Region.Details from BSAVA Customer Services, telephone 01452 726700, email [email protected]
18 NovemberTuesday
Top 10 tips to avoid being suedSpeaker Julian WellsEvening meeting at the Glasgow Pond Hotel, Great Western Road (Glasgow). Scottish Region.Details from Ross Allan, telephone 07786 653371, email [email protected]
19 NovemberWednesday
CPD Road Show: surgical emergencies Speakers Karen Tobias and John Williams (co-editor of Wounds 2e and Abdominal Surgery)Day meeting at the Bellhouse Hotel, Beaconsfield, Buckinghamshire. Metropolitan Region.Details from BSAVA Customer Services, telephone 01452 726700, email [email protected]
20 NovemberThursday
Recent developments in feline orthopaedicsSpeaker Harry ScottEvening meeting at the Potters Heron Hotel, Romsey. Southern Region.Details from Michelle Stead, telephone 01722 321185, email [email protected]
25 NovemberTuesday
SA endocrinology IISpeaker Ian RamseyBSAVA Modular course Day meeting at BSAVA, Woodrow House. Organised by BSAVA.Details from BSAVA Customer Services, telephone 01452 726700, email [email protected]
Musculoskeletal Disorders
Your comprehensive guide to joints and lameness
British Small Animal Veterinary AssociationWoodrow House, 1 Telford Way,
Waterwells Business Park, Quedgeley, Gloucester GL2 2AB
ArthritisArthritis is an important orthopaedic condition and is considered in-depth in this Manual. Topics covered include: general approach and diagnostics; osteoarthritis; immune mediated arthritis; and infective arthritis.
LamenessThis common presenting complaint is discussed in detail in this Manual. Chapters dedicated to the approach to the lame patient and the neurological causes of lameness help provide a comprehensive review.
Joint surgeryStep-by-step Operative Techniques accompany the surgical chapters in this Manual. Surgery of the shoulder, the elbow, the hip and the stifl e are all covered here. The equipment and principles of arthroscopy are covered in-depth.