Université de Bourgogne UFR des Sciences de Santé Circonscription Médecine ANNEE 2017 N° Comparaison de différentes modalités de recueil en tomographie par cohérence optique Spectral-Domain dans la détection de pathologies maculaires et de l’interface vitréorétinienne : l’étude MONTRACHET THESE présentée à l’UFR des Sciences de Santé de Dijon Circonscription Médecine et soutenue publiquement le 4 octobre 2017 pour obtenir le grade de Docteur en Médecine par Ghislaine ASSAD Née le 20 janvier 1986 A Paris 14 ème
Transcript
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
ANNEE 2017
N°
Comparaison de différentes modalités de recueil en tomographie
par cohérence optique Spectral-Domain dans la détection de
pathologies maculaires et de l’interface vitréorétinienne : l’étude
MONTRACHET
THESE
présentée
à l’UFR des Sciences de Santé de Dijon
Circonscription Médecine
et soutenue publiquement le 4 octobre 2017
pour obtenir le grade de Docteur en Médecine
par Ghislaine ASSAD
Née le 20 janvier 1986
A Paris 14ème
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
AVERTISSEMENT
Ce document est le fruit d’un long travail approuvé par le jury de soutenance et mis à la
disposition de la communauté universitaire élargie.
Il est soumis à la propriété intellectuelle de l’auteur.
Ceci implique une obligation de citation et de référencement dans la rédaction de vos travaux.
D’autre part, toutes contrefaçons, plagiats, reproductions illicites encourt une poursuite
pénale.
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
ANNEE 2017
N°
Comparaison de différentes modalités de recueil en tomographie
par cohérence optique Spectral-Domain dans la détection de
pathologies maculaires et de l’interface vitréorétinienne : l’étude
MONTRACHET
THESE
présentée
à l’UFR des Sciences de Santé de Dijon
Circonscription Médecine
et soutenue publiquement le 4 octobre 2017
pour obtenir le grade de Docteur en Médecine
Par Ghislaine ASSAD
Née le 20 janvier 1986
A Paris 14èm
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
Année Universitaire 2017-2018
au 1er Septembre 2017
Doyen : M. Frédéric HUET
Assesseurs : M. Marc MAYNADIE M. Pablo ORTEGA-DEBALLON
PROFESSEURS DES UNIVERSITES – PRATICIENS HOSPITALIERS
Discipline
M. Marc BARDOU Pharmacologie clinique M. Jean-Noël BASTIE Hématologie - transfusion M. Emmanuel BAULOT Chirurgie orthopédique et traumatologie M. Yannick BEJOT Neurologie M. Alain BERNARD Chirurgie thoracique et cardiovasculaire Mme Christine BINQUET Epidémiologie, économie de la santé et prévention M. Bernard BONIN Psychiatrie d’adultes M. Philippe BONNIAUD Pneumologie M. Alain BONNIN Parasitologie et mycologie M. Bernard BONNOTTE Immunologie M. Olivier BOUCHOT Chirurgie cardiovasculaire et thoracique M. Belaid BOUHEMAD Anesthésiologie - réanimation chirurgicale M. Alexis BOZORG-GRAYELI ORL M. Alain BRON Ophtalmologie M. Laurent BRONDEL Physiologie Mme Mary CALLANAN Hématologie type biologique M. Patrick CALLIER Génétique M. Jean-Marie CASILLAS-GIL Médecine physique et réadaptation Mme Catherine CHAMARD-NEUWIRTH Bactériologie - virologie; hygiène hospitalière M. Pierre-Emmanuel CHARLES Réanimation M. Pascal CHAVANET Maladies infectieuses M. Nicolas CHEYNEL Anatomie M. Alexandre COCHET Biophysique et médecine nucléaire M. Luc CORMIER Urologie M. Yves COTTIN Cardiologie M. Charles COUTANT Gynécologie-obstétrique M. Gilles CREHANGE Oncologie-radiothérapie Mme Catherine CREUZOT-GARCHER Ophtalmologie M. Frédéric DALLE Parasitologie et mycologie M. Serge DOUVIER Gynécologie-obstétrique Mme Laurence DUVILLARD Biochimie et biologie moléculaire M. Olivier FACY Chirurgie générale Mme Laurence FAIVRE-OLIVIER Génétique médicale Mme Patricia FAUQUE Biologie et Médecine du Développement Mme Irène FRANCOIS-PURSSELL Médecine légale et droit de la santé M. Pierre FUMOLEAU Cancérologie M. François GHIRINGHELLI Cancérologie M. Claude GIRARD Anesthésiologie – réanimation chirurgicale M. Vincent GREMEAUX Médecine physique et réadaptation
(Mise en disponibilité du 12 juin 2017 au 11 juin 2018) M. Frédéric HUET Pédiatrie M. Pierre JOUANNY Gériatrie
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
M. Sylvain LADOIRE Histologie M. Gabriel LAURENT Cardiologie M. Côme LEPAGE Hépato-gastroentérologie M. Romaric LOFFROY Radiologie et imagerie médicale M. Luc LORGIS Cardiologie M. Jean-Francis MAILLEFERT Rhumatologie M. Cyriaque Patrick MANCKOUNDIA Gériatrie M. Sylvain MANFREDI Hépato-gastroentérologie M. Laurent MARTIN Anatomie et cytologie pathologiques M. David MASSON Biochimie et biologie moléculaire M. Marc MAYNADIE Hématologie – transfusion M. Marco MIDULLA Radiologie et imagerie médicale M. Thibault MOREAU Neurologie M. Klaus Luc MOURIER Neurochirurgie Mme Christiane MOUSSON Néphrologie M. Paul ORNETTI Rhumatologie M. Pablo ORTEGA-DEBALLON Chirurgie Générale M. Jean-Michel PETIT Endocrinologie, diabète et maladies métaboliques M. Christophe PHILIPPE Génétique M. Lionel PIROTH Maladies infectieuses Mme Catherine QUANTIN Biostatistiques, informatique médicale M. Jean-Pierre QUENOT Réanimation M. Patrick RAT Chirurgie générale M. Jean-Michel REBIBOU Néphrologie M. Frédéric RICOLFI Radiologie et imagerie médicale M. Paul SAGOT Gynécologie-obstétrique M. Emmanuel SAPIN Chirurgie Infantile M. Henri-Jacques SMOLIK Médecine et santé au travail M. Éric STEINMETZ Chirurgie vasculaire Mme Christel THAUVIN Génétique M. Benoit TROJAK Psychiatrie d’adultes ; addictologie M. Pierre VABRES Dermato-vénéréologie M. Bruno VERGÈS Endocrinologie, diabète et maladies métaboliques M. Narcisse ZWETYENGA Chirurgie maxillo-faciale et stomatologie
PROFESSEURS EN SURNOMBRE
M. Roger BRENOT Chirurgie thoracique et cardiovasculaire
(Surnombre jusqu’au 31/08/2018) M. Philippe CAMUS Pneumologie
(Surnombre jusqu’au 31/08/2018) M. Maurice GIROUD Neurologie
(Surnombre jusqu’au 21/08/2018)
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
MAITRES DE CONFERENCES DES UNIVERSITES
PRATICIENS HOSPITALIERS DES DISCIPLINES MEDICALES
Discipline Universitaire
Mme Lucie AMOUREUX BOYER Bactériologie M. Sylvain AUDIA Médecine interne Mme Shaliha BECHOUA Biologie et médecine du développement M. Benjamin BOUILLET Endocrinologie Mme Marie-Claude BRINDISI Nutrition M. Jean-Christophe CHAUVET-GELINIER Psychiatrie, psychologie médicale Mme Marie-Lorraine CHRETIEN Hématologie Mme Vanessa COTTET Nutrition M. Alexis DE ROUGEMONT Bactériologie-virologie ; hygiène hospitalière M. Hervé DEVILLIERS Médecine interne Mme Ségolène GAMBERT-NICOT Biochimie et biologie moléculaire Mme Marjolaine GEORGES Pneumologie Mme Françoise GOIRAND Pharmacologie fondamentale M. Charles GUENANCIA Cardiologie Mme Agnès JACQUIN Physiologie M. Alain LALANDE Biophysique et médecine nucléaire M. Louis LEGRAND Biostatistiques, informatique médicale Mme Stéphanie LEMAIRE-EWING Biochimie et biologie moléculaire M Maxime SAMSON Médecine interne M. Paul-Mickaël WALKER Biophysique et médecine nucléaire
PROFESSEURS EMERITES M. Laurent BEDENNE (01/09/2017 au 31/08/2020) M. Jean-François BESANCENOT (01/09/2017 au 31/08/2020) M. François BRUNOTTE (01/09/2017 au 31/08/2020) M. Jean FAIVRE (01/09/2015 au 31/08/2018) M. Patrick HILLON (01/09/2016 au 31/08/2019) M. François MARTIN (01/09/2015 au 31/08/2018) M. Pierre POTHIER (01/09/2015 au 31/08/2018) M. Pierre TROUILLOUD (01/09/2017 au 31/08/2020)
PROFESSEURS DES UNIVERSITES DE MEDECINE GENERALE M. Jean-Noël BEIS Médecine Générale
PROFESSEURS ASSOCIES DE MEDECINE GENERALE M. Didier CANNET Médecine Générale M. Gilles MOREL Médecine Générale M. François MORLON Médecine Générale
MAITRES DE CONFERENCES ASSOCIES DE MEDECINE GENERALE Mme Anne COMBERNOUX -WALDNER Médecine Générale M. Clément CHARRA Médecine Générale M. Rémi DURAND Médecine Générale M. Arnaud GOUGET Médecine Générale
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
MAITRES DE CONFERENCES DES UNIVERSITES M. Didier CARNET Anglais M. Jean-Pierre CHARPY Anglais Mme Catherine LEJEUNE Pôle Epidémiologie M. Gaëtan JEGO Biologie Cellulaire
PROFESSEURS DES UNIVERSITES Mme Marianne ZELLER Physiologie
PROFESSEURS CERTIFIES Mme Anaïs CARNET Anglais M. Philippe DE LA GRANGE Anglais Mme Virginie ROUXEL Anglais (Pharmacie)
PROFESSEURS DES UNIVERSITES – PRATICIENS HOSPITALIERS DES DISCIPLINES
PHARMACEUTIQUES M. François GIRODON Sciences biologiques, fondamentales et cliniques
Mme Evelyne KOHLI Immunologie
MAITRES DE CONFERENCES DES UNIVERSITES
PRATICIENS HOSPITALIERS DES DISCIPLINES PHARMACEUTIQUES M. Mathieu BOULIN Pharmacie clinique M. Philippe FAGNONI Pharmacie clinique M. Frédéric LIRUSSI Toxicologie M. Marc SAUTOUR Botanique et cryptogamie M. Antonin SCHMITT Pharmacologie
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
L’UFR des Sciences de Santé de Dijon, Circonscription Médecine, déclare que les opinions
émises dans les thèses qui lui sont présentées doivent être considérées comme propres à
leurs auteurs, et qu'elle n'entend ne leur donner ni approbation, ni improbation.
COMPOSITION DU JURY
Président : Madame le Professeur Catherine CREUZOT-GARCHER
Membres : Monsieur le Professeur Alain-Marie BRON
Monsieur le Docteur Hervé DEVILLIERS
Madame le Docteur Clémence DESCHASSE
A notre Président et Directeur de thèse,
Madame le Professeur Catherine CREUZOT-GARCHER,
Nous vous remercions de l’honneur que vous nous faites en acceptant de présider
notre jury.
Votre détermination, vos connaissances et votre dextérité chirurgicale nous ont
toujours inspiré une grande admiration.
Nous saluons votre persévérance, votre optimisme et votre patience dans la
recherche et la formation des internes, qui sont pour nous un magnifique exemple
à suivre.
Nous sommes très fières d’avoir été votre élève et nous vous remercions pour
votre aide et votre soutien tout au long de ces années.
Soyez assurée de notre sincère reconnaissance et notre plus profond respect.
A notre juge,
Monsieur le Professeur Alain BRON,
Nous vous remercions de l’honneur que vous nous faites en acceptant de juger
notre travail.
Nous admirons votre détermination et votre travail de longue haleine qui a permis
au service de Dijon de devenir une école prestigieuse de l’ophtalmologie.
Votre savoir immense et votre sens de la rigueur nous ont servi de modèle dans
l’apprentissage de l’ophtalmologie. Cela aura été un grand honneur d’avoir pu
apprendre à vos côtés.
Veuillez recevoir ici l’expression de notre gratitude et de notre plus profond
respect.
A notre juge,
Monsieur le Docteur Hervé DEVILLIERS,
Soyez vivement remercié de l’honneur que vous nous avez fait en acceptant de
juger notre travail.
Vos connaissances dans tous les domaines de la médecine, votre capacité de
travail et votre dynamisme nous épatent et font de vous un futur grand Professeur.
Nous vous remercions pour votre enseignement pendant ces quelques mois dans
le service de médecine interne et pour votre précieuse collaboration avec le
service d’ophtalmologie.
Veuillez recevoir l’expression de notre reconnaissance et de notre plus profond
respect.
A notre juge,
Madame le Docteur Clémence DESCHASSE,
Soyez vivement remerciée de l’honneur que vous nous avez fait en acceptant de
juger notre travail.
Nous saluons vos connaissances débordantes dans tous les domaines de
l’ophtalmologie. Neuro-ophtalmolgie, uvéite, rétine, paupière, glaucome, plus rien
ne vous arrête.
Nous vous remercions infiniment pour vos enseignements et votre patience au
bloc opératoire. Vous avez su nous transmettre la passion de la chirurgie de la
paupière. Nous avons beaucoup appris chirurgicalement, toujours avec un fond
musical de Disney ou Dalida. Votre bonne humeur, votre humour, vos playlists et
chorégraphies improbables ont fait de la « team-paupiette » un duo magique gravé
dans l’histoire du bloc.
Vous êtes devenue une amie et confidente précieuse. Nous sommes
reconnaissantes de vos conseils et votre soutien en toute circonstance. Nous
sommes ravies de partager encore des moments formidables à vos côtés.
Soyez assurée de notre reconnaissance et de notre profonde amitié.
Un grand MERCI à …
A mes anciens chefs et co-interne
Denis (#DD) : Mon premier mentor de la paupière, toujours speed et dynamique, tu m’impressionnes à
chaque bloc opératoire. En un tour de main et un peu de coagulation, tu viens à bout de toutes les
chirurgies de paupière. Je te remercie pour tout ce que tu m’as appris et je te souhaite plein de réussite
dans votre tout nouveau cabinet.
Yann et Philippe (#PK) : Merci pour vos enseignements et votre partage de l’amour de la rétine qui
m’ont beaucoup apporté au début de mon internat. Je vous souhaite que du bonheur et de la réussite
pour la suite, vous êtes la jeunesse florissante de l’ophtalmologie de ville.
Olivier (#Oliv’) : Toujours le sourire aux lèvres et de bonne humeur, tu as toujours plein de bons plans
et de belles idées de voyage. Je te remercie pour ton aide dans mes débuts de chirurgie réfractive.
J’espère aussi que tu pourras m’accompagner pour cette 2ème année du DU de paupière et continuer
avec la secte de la paupière cosmopolite.
Arthur (#Arthuro) : Quand je t’ai rencontré la première fois à Nevers, tu étais déjà très impliqué et
soigneux dans le travail et tu as continué à être un formidable cornéologue dans le service. Ton sourire,
ta bonne humeur et ton accent toulousain nous manquent. Je te souhaite une belle réussite dans ta
nouvelle vie parisienne.
Aurore, Rodica, Arnaud, Till, JC : Je n’ai malheureusement pas eu la chance de travailler avec vous,
mais c’est toujours un plaisir de vous revoir notamment à la SFO.
A mes chefs actuels
Cyril (#CM) : Que dire à part un immense merci. On ne souligne pas assez l’implication que tu as dans
le service, le bloc et le soutien envers tous les internes. Merci pour m’avoir toujours soutenue depuis
mon premier semestre au CHU où je me noyais dans les urgences du lundi matin jusqu’à la relecture
de ma thèse aujourd’hui. Merci pour ta patience et tes conseils au bloc au prix de nombreux spasmes
coronariens. Merci de m’avoir redonné confiance en moi et de m’avoir permis de réaliser ma première
cataracte. Merci pour tous ces fous rires et bons moments. Tu es une personne entière, sincère, pleine
de vie, forte et fragile à la fois, je suis heureuse de t’avoir rencontré.
Firas (#DucDeSemur #MercrediEtVendrediC’estSacré)
Charlotte : Je te remercie pour ta détermination et ton sérieux dans l’organisation du service et la
formation des externes. Tu es notre pilier de l’ophtalmologie pédiatrique et je suis fière d’apprendre à
tes côtés pendant encore quelques temps même si tu devras nous abandonner pour un magnifique
évènement. Je te souhaite une vie pleine de bonheur avec Julien et votre futur petit bout de chou
(j’espère que tu le mettras très tôt à la course à pied).
Jacques (#Jacky) : Je t’ai toujours connu calme, soigné et travailleur, mais aussi drôle et sympathique,
avec une petite touche d’humour bien placée et un sens de la répartie inégalée. C’est un réel plaisir de
travailler avec toi, ne change rien. Je te souhaite pleins de bonheur et de réussite avec Perrine.
A mes co-internes : les « vieux » et « moyens vieux »
Aurélie : Très sérieuse, impliquée et rigoureuse, tu as contribué à développer la contactologie dans le
service et je t’en félicite. Je te souhaite une belle continuation à Chalon et un bel épanouissement avec
Maxime dans ta future nouvelle grande maison.
Louis (#Luigi) : J’apprécie beaucoup ton calme et ta sérénité en toute circonstance, pour preuve, tu as
réussi à convaincre la troupe de remanger à l’internat sans effusion de sang, chapeau ! Je te félicite
surtout pour avoir eu le courage de rallonger cette aventure d’une année, mais je suis sure que le jeu
en valait la chandelle. Je te souhaite une belle réussite pour la suite.
Pierre-Henry (#PH #Pitch) : Grand et élancé, cheveux grisonnants bien peignés, une curiosité
débordante, une humilité indéniable et une touche d’humour pour couronner le tout…il n’y a aucun
doute, tu as toutes les qualités du futur Professeur Mamour de l’ophtalmologie dijonnaise. Tu es devenu
un véritable ami, je te souhaite tout le bonheur et une vie heureuse avec Clem et bientôt mini-PH.
Youssef (#Youyou) : Sérieux, travailleur, toujours de bonne humeur et parfois même taquin sur les
bords, tu es toujours là pour soutenir et aider les jeunes internes. Tu es devenu un grand ami et mon
acolyte des révisions EBO. On ne compte plus les week-end et soirées passées ensemble dans le
service et les appels mutuels de soutien et de motivation. Je suis heureuse de continuer cette route
avec toi.
Edouard (#Edou) : Tu fais partie d’une de mes meilleures rencontres de cette aventure. Ta
détermination et ta rigueur dans le travail, ton sens de la perfection et tes accès maniaques, ta
générosité, ta bonne humeur et tes coups de gueule font de toi une personne entière et un ami précieux.
Je te souhaite le meilleur mon Edou.
Sophia : J’ai rarement vu une fille aussi déterminée, volontaire et travailleuse. Deuxième jeune mariée
de la troupe, tu aimes ta vie planifiée et ordonnée. Mais derrière cette femme de caractère, se cache
une jeune fille aimante, sensible, pleine de bonté et de générosité. Je suis heureuse de t’avoir
rencontrée et je te souhaite une vie paisible avec Jocelyn.
Julie (#Juju #JB) : Ma Juju, on a passé des moments merveilleux à la fois joyeux, festifs et tristes en
sillonnant la Bourgogne ensemble de Macon à Nevers. Tu pourrais être juste grande blonde et jolie,
mais tu es aussi intelligente, travailleuse, impliquée dans ton travail (notamment les plannings) et tu
sais profiter de la vie autour d’une bière. Tu es devenue une amie et confidente qui m’est chère et sur
qui on peut compter. Tout plein de bonheur pour François et toi.
Elsa (#Kitty #PetiteBiche) : Toujours élégante, dynamique et consciencieuse, tu seras sans nul doute
une cornéologue redoutable. Tu vas pouvoir approfondir tes connaissances à Lyon le semestre
prochain, mais ta bonne humeur et ta joie de vivre vont nous manquer. Reviens nous vite !
Florian (#Flo) : Premier jeune marié et papa de la troupe, j’admire ton courage et ton aisance pour
assimiler à la fois ta vie de famille, ton implication sans faille à la recherche et ton dévouement en
contactologie. Petit génie de l’informatique, tu réponds toujours présent pour nous aider à maitriser
Excel et les statistiques. Tu reviens enfin après un an d’exil…welcome home !
A mes co-internes : les « jeunes » et « les piou-piou »
Solenne (#Soso) et Lucie (#NoFilter) les nouvelles pionnières de l’ophtalmo-pédiatriques, Mélanie
(#Mel) bosseuse mais chat noir, tu es bannie des urgences le prochain semestre, Lolita (#chikita) ma
future jeune Padawan de la paupière? Martin (#Martine) courage tu auras bientôt un vrai bloc, en
attendant rdv tous les jours même tram, même heure... Ines (#Nénès) la bosseuse de l’ombre, dernière
sortie du service, ton nouveau look te va à ravir !
Aux nouveaux piou-piou Alicia, Déa, Marc-Antoine, Chloé, Victoire, Mohammed : bon courage,
soyez fort, plein de nouvelles aventures vous attendent!
Aux secrétaires :
Françoise (perdue au combat), Annick (The boss), Anna et Emilie (merci pour tous les bonbons et
sucreries qui nous réconfortent en fin de journée), Amandine, Audrey, Aude, Christine : un grand
merci pour gérer tous ces appels incessants et ces rdv, désolée pour toutes ces consultations
déplacées. Vous êtes un des piliers du service.
Aux infirmières du service :
Anne-Claude (ironwoman, je rêverai pouvoir courir comme toi), Sarah (pas plus d’un verre!), Fabienne
(la grande Fafa, toujours souriante et de bonne humeur), Christelle (c’est toi avec moi aux angios ?),
Ghislaine VACHON (future ex-cadre d’ophtalmo, je vais perdre mon homonyme !) : un grand grand
merci pour toutes ces explos faites sans même ronchonner, vous êtes au top (#Oct mac et fibres svp
merci).
Aux aides-soignantes
Pascale (Pascalou, impératrice des IVT, mascotte du service et des patients, profites bien de ta
nouvelle vie de retraitée amplement méritée, tu vas nous manquer), Fabienne (la petite Fafa, au top,
promis on arrêtera d’embêter les jeunes internes).
Aux orthoptistes :
Aurélie (# Ça va ? Tu veux la vraie réponse ou la standard), Magalie, Clémence, Sophie et tous les
étudiants orthoptistes : un grand merci pour tous les champs-visuels, les multiples explos et les pré-
consults.
Aux ARCSs :
Emmanuella (#Manu#TenuesColorées), Hélène et Perrine : vous formez une équipe de choc ! La
petite carte des protocoles aux couleurs tendances est une très bonne idée !
A l’équipe de basse vision : Monique, Anne, Aline et Aurélie.
Aux filles de l’UPOC : Bénédicte, Emilie, Rachida, Jeanne, Valérie, Laetitia et Marie-Brigitte.
Aux filles de l’UCA : Babeth, Cindy, Véro, Pascale, Karine et les autres (# quelqu’un peut monter en
UCA faire la sortie ? Le taxi est là). Un grand merci pour les préparations des patients et les mydriasert).
Au bloc opératoire :
Nath (#17077, merci pour ton implication infaillible au bloc), Séverine (#On est bon pour l’implant ?),
Marie (#T’as un gaviscon ou un zophren pour Clemy ?), Delphine (# T’as fait ma tarte ?), Sophie (#Tu
me prêtes un stylo stp?), Cécile (#Tablette serrée à fond !), Sandrine et Marie-Claude (#Tic et Tac,
notre duo de choc, merci pour vos gâteaux entre deux blocs), Danielle (#Tablette de chocolat en douce
dans la poche) : un grand merci pour votre bonne humeur tous les matins, c’est un réel plaisir de
travailler avec vous.
Au service d’ophtalmologie de Mâcon :
Au Dominique REVY, merci d’avoir été le premier à m’enseigner l’ophtalmologie et d’avoir initié mes
premières cataractes, vous êtes un vrai modèle pour moi. A Jérome, Corinne, Julien, Isabelle,
Eléonore et les belles sécrétaires bien-sûr, un grand merci pour votre accueil et votre gentillesse.
Au service d’ophtalmologie de Nevers :
A Akram, Louhay, Martine et Aziz merci pour votre confiance au bloc et en consultation. A Marie-Thé
et Marie-France, vous êtes au top les filles ! Au trio de choc de secrétaires : Michèle, Sophie et Cécile.
Au service de médecine interne :
Au Professeur BESANCENOT, Géraldine, Alin, Hervé, Jean-Baptiste et Philip. Un grand merci pour
votre aide précieuse et désolée pour les comptes-rendus non transférés sur DxCare !
Au service de radiologie :
Au Professeur RICOLFI, aux Docteurs Martine COUDERT, Nathalie BAUDOUIN, Adrien
CHAVENT, Marie-Charlotte LELAURIN ROCHE. Un grand merci pour m’avoir fait découvrir le monde
L’examen par cohérence optique Spectral-Domain (SD-OCT) permet d’examiner, avec précision,
chacune des couches de la rétine. Il est devenu un outil diagnostique et de suivi essentiel des
pathologies maculaires et de l’interface vitréorétinienne dans la pratique ophtalmologique courante.
Cependant les appareils SD-OCT proposent de multiples modalités de recueil mais aucune étude n’a
permis de définir un protocole standardisé d’acquisition et d’analyse approprié dans la détection et le
suivi des pathologies rétiniennes. Le but de cette étude était de comparer différentes modalités de
recueil en SD-OCT pour détecter des pathologies maculaires et vitréorétiniennes rencontrées en
pratique clinique.
Deux-mille trois cent six yeux de 1153 patients d’âge moyen de 82,2 ± 3,8 ans ont été inclus dans
l’étude de MONTRACHET (Maculopathy, Optic Nerve, nuTRition, neurovasCular and HEarT diseases).
Chaque patient a bénéficié d’un examen SD-OCT incluant différentes modalités de recueil : le cube
maculaire (19 B-scans) considéré comme examen de référence, ainsi qu’une ligne horizontale et une
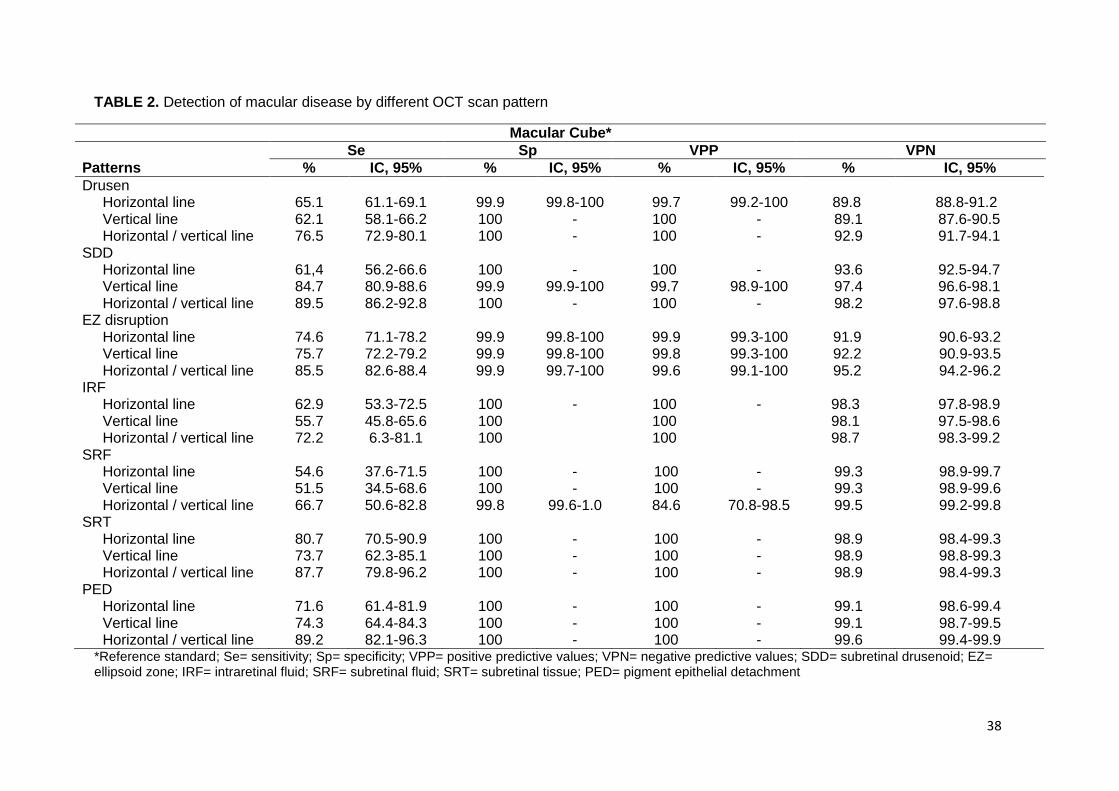
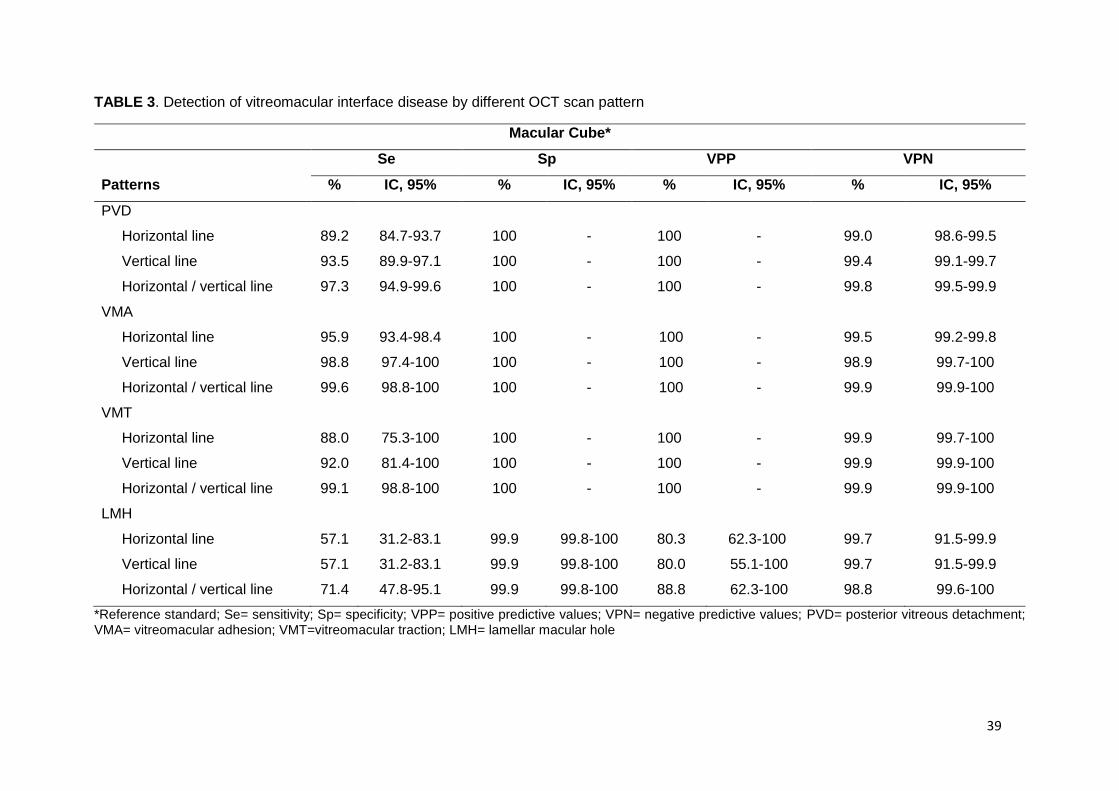
ligne verticale, toutes deux centrées sur la fovea. La détection des pathologies maculaires et
vitréorétiniennes était meilleure avec l’association d’une ligne horizontale/verticale rétrofovéolaire
qu’avec une ligne horizontale rétrofovéolaire. L’association d’une ligne horizontale/verticale
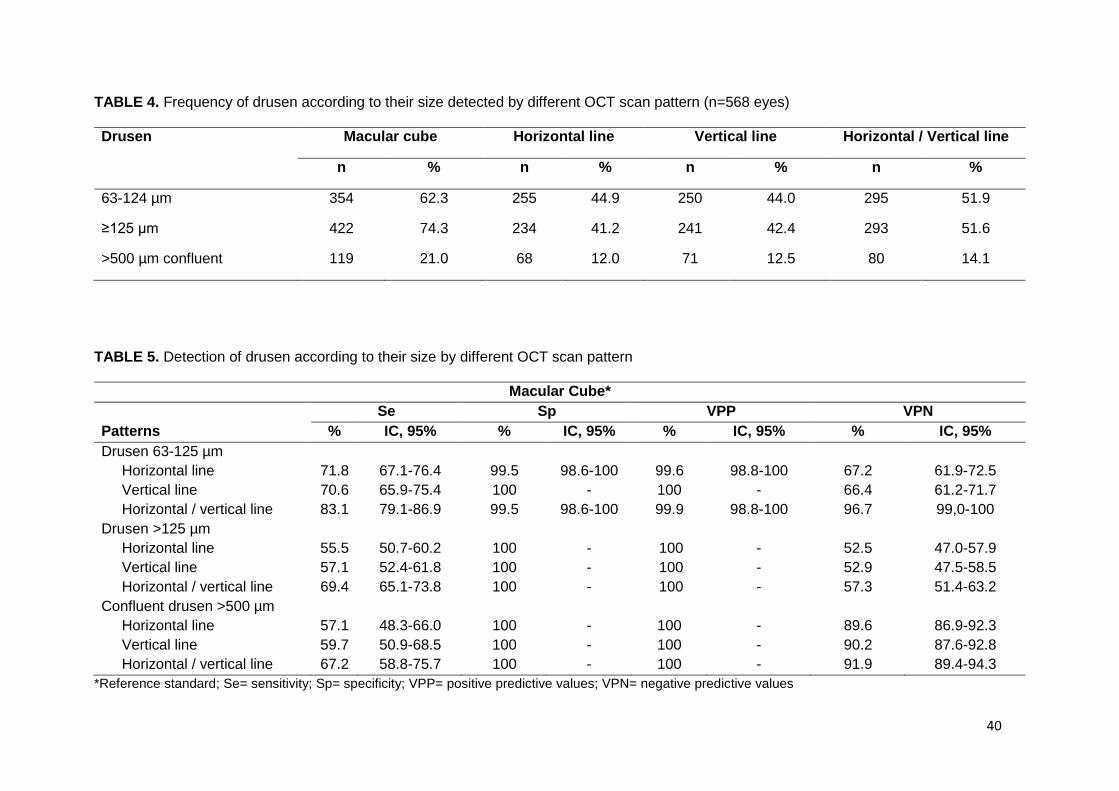
rétrofovéolaire a détecté les pathologies maculaires comme les pseudodrusens réticulés, les
décollements de l’épithélium pigmentaire, les drusens et les œdèmes intrarétiniens avec une sensibilité
de 90%, 89%, 76% et 72%, respectivement. Les pathologies de l’interface vitréorétinienne comme les
adhésions et tractions vitréomaculaires et les membranes épirétinienne ont été détectées avec une
sensibilité de 99%, 99% et 91% respectivement.
Cette étude a montré que l’association d’une ligne horizontale/verticale rétrofovéolaire en SD-OCT est
fortement corrélée au modèle de référence du cube maculaire dans la détection de pathologies
maculaires et vitréorétiniennes. Elle permet une analyse simple et rapide des clichés SD-OCT avec une
bonne qualité d’image.
43
References
1. Hoerster R, Muether PS, Hermann MM, et al. Subjective and functional deterioration in recurrences of neovascular AMD are often preceded by morphologic changes in optic coherence tomography. Br J Ophthalmol. 2011;95:1424-1426. 2. Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol. 2009;148:43-58 e41. 3. Comparison of Age-related Macular Degeneration Treatments Trials Research G, Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119:1388-1398. 4. Stalmans P, Benz MS, Gandorfer A, et al. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367:606-615. 5. Schneider EW, Todorich B, Kelly MP, Mahmoud TH. Effect of optical coherence tomography scan pattern and density on the detection of full-thickness macular holes. Am J Ophthalmol. 2014;157:978-984. 6. Kiernan DF, Mieler WF, Hariprasad SM. Spectral-domain optical coherence tomography: a comparison of modern high-resolution retinal imaging systems. Am J Ophthalmol. 2010;149:18-31. 7. Ferris FL, Davis MD, Clemons TE, et al. A simplified severity scale for age-related macular degeneration: AREDS Report No. 18. Arch Ophthalmol. 2005;123:1570-1574. 8. Zweifel SA, Imamura Y, Spaide TC, Fujiwara T, Spaide RF. Prevalence and significance of subretinal drusenoid deposits (reticular pseudodrusen) in age-related macular degeneration. Ophthalmology. 2010;117:1775-1781. 9. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120:2611-2619. 10. Meuer SM, Myers CE, Klein BE, et al. The epidemiology of vitreoretinal interface abnormalities as detected by spectral-domain optical coherence tomography: the beaver dam eye study. Ophthalmology. 2015;122:787-795. 11. Major JC, Jr., Wykoff CC, Mariani AF, et al. Comparison of spectral-domain and time-domain optical coherence tomography in the detection of neovascular age-related macular degeneration activity. Retina. 2014;34:48-54. 12. Sayanagi K, Sharma S, Kaiser PK. Comparison of retinal thickness measurements between three-dimensional and radial scans on spectral-domain optical coherence tomography. Am J Ophthalmol. 2009;148:431-438. 13. Sayanagi K, Sharma S, Yamamoto T, Kaiser PK. Comparison of spectral-domain versus time-domain optical coherence tomography in management of age-related macular degeneration with ranibizumab. Ophthalmology. 2009;116:947-955. 14. De Bats F, Mathis T, Mauget-Faysse M, et al. Prevalence of Reticular Pseudodrusen in Age-Related Macular Degeneration Using Multimodal Imaging. Retina. 2016;36:46-52. 15. Curcio CA, Messinger JD, Sloan KR, et al. Subretinal drusenoid deposits in non-neovascular age-related macular degeneration: morphology, prevalence, topography, and biogenesis model. Retina. 2013;33:265-276. 16. Schmitz-Valckenberg S, Alten F, Steinberg JS, et al. Reticular drusen associated with geographic atrophy in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:5009-5015. 17. Freeman SR, Kozak I, Cheng L, et al. Optical coherence tomography-raster scanning and manual segmentation in determining drusen volume in age-related macular degeneration. Retina. 2010;30:431-435. 18. Gregori G, Wang F, Rosenfeld PJ, et al. Spectral domain optical coherence tomography imaging of drusen in nonexudative age-related macular degeneration. Ophthalmology. 2011;118:1373-1379.
44
19. Courtney RJ, McClintic JI, Ehlers JP. Comparison of Spectral Domain Optical Coherence Tomography Scan Patterns and Clinical Review Strategies in Neovascular Age-Related Macular Degeneration. Retina. 2015;35:1315-1322. 20. Baranano AE, Keane PA, Ruiz-Garcia H, Walsh AC, Sadda SR. Impact of scanning density on spectral domain optical coherence tomography assessments in neovascular age-related macular degeneration. Acta Ophthalmol. 2012;90:e274-280. 21. Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149:371-382 e371. 22. Mojana F, Cheng L, Bartsch DU, et al. The role of abnormal vitreomacular adhesion in age-related macular degeneration: spectral optical coherence tomography and surgical results. Am J Ophthalmol. 2008;146:218-227. 23. Shao L, Xu L, You QS, et al. Prevalence and associations of incomplete posterior vitreous detachment in adult Chinese: the Beijing Eye Study. PLoS One. 2013;8:e58498. 24. Wilkins JR, Puliafito CA, Hee MR, et al. Characterization of epiretinal membranes using optical coherence tomography. Ophthalmology. 1996;103:2142-2151. 25. Romano MR, Cennamo G, Amoroso F, et al. Intraretinal changes in the presence of epiretinal traction. Graefes Arch Clin Exp Ophthalmol. 2017;255:31-38. 26. Sakamoto A, Hangai M, Yoshimura N. Spectral-domain optical coherence tomography with multiple B-scan averaging for enhanced imaging of retinal diseases. Ophthalmology. 2008;115:1071-1078 e1077. 27. Spaide RF. Enhanced depth imaging optical coherence tomography of retinal pigment epithelial detachment in age-related macular degeneration. Am J Ophthalmol. 2009;147:644-652.
Université de Bourgogne
UFR des Sciences de Santé
Circonscription Médecine
TITRE DE LA THESE : Comparaison de différentes modalités de recueil en tomographie par
cohérence optique Spectral-Domain dans la détection de pathologies maculaires et de l’interface
vitréorétinienne : l’étude MONTRACHET
AUTEUR : Ghislaine ASSAD
RESUME
Objectifs : Comparer différentes modalités de recueil en tomographie par cohérence optique Spectral-
Domain (SD-OCT) pour détecter des pathologies maculaires et vitréorétiniennes rencontrées en
pratique courante.
Méthodes : Les patients de l’étude MONTRACHET (Maculopathy, Optic Nerve, nuTRition,
neurovasCular and HEarT diseases) ont bénéficié d’un examen SD-OCT maculaire incluant différentes
modalités de recueil : le cube maculaire (19 B-scans) ainsi qu’une ligne horizontale et une ligne verticale,
toutes deux centrées sur la fovea. L’analyse des clichés SD-OCT recherchait la présence de drusens
et pseudo-drusens réticulés (PDR), d’œdème intrarétinien (OIR), de décollement de l’épithélium
pigmentaire (DEP), d’adhésion vitréomaculaire (AVM) ou de traction vitréomaculaire (VMT) et de
membrane épirétinienne (MER).
Résultats : Deux-mille trois cent six yeux de 1153 patients ont été inclus. L’âge moyen était de 82,2 ±
3,8 ans. Le cube maculaire était considéré comme modèle de référence. La ligne horizontale
rétrofovéolaire a détecté les PDR, les DEP, les drusens et les OIR avec une sensibilité de 61%, 72%,
65% et 63%, respectivement. Les AVM, les TVM et les MER étaient détectées avec une sensibilité de
96%, 88% et 82% respectivement. L’association d’une ligne horizontale/verticale rétrofovéolaire a
détecté les PDR, les DEP, les drusens et les OIR avec une sensibilité de 90%, 89%, 77% et 72%,
respectivement. Les AVM, les TVM et les MER étaient détectées avec une sensibilité de 99%, 99% et
91% respectivement.
Conclusion : L’association d’une ligne horizontale/verticale rétrofovéolaire en SD-OCT est fortement
corrélée au modèle de référence du cube maculaire dans la détection de pathologies maculaires et
vitréorétiniennes, tout en permettant une bonne qualité d’image et une interprétation simple et rapide.
MOTS-CLES : tomographie par cohérence optique Spectral-Domain, pathologie maculaire, pathologie