SM Journal of Pediatrics Gr up SM How to cite this article Nasibova EM and Polukhov RS. Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children. SM J Pediatr. 2018; 3(1): 1015. OPEN ACCESS Introduction e rapid development of surgery was a powerful stimulus for the further expansion and improvement of the methods of anesthesia. Transrectal resection of the large intestine in Hirschsprung’s disease in young children is a new approach to solving this problem in this category of patients. Children of early age due to anatomical and physiological characteristics belong to the group of high anesthetic risk due to the rapid development and progression of pathological conditions. erefore, when choosing an anesthetic benefit in children of this age, it is necessary to seek to minimize the negative properties of the methods used. Given the trend of a multimodal approach to anesthesia, regional anesthesia has become increasingly prevalent in recent years. Currently, among the regional methods of anesthesia, caudal anesthesia in pediatric practice [1-3] is the most popular. e present concept of “balanced regional anesthesia” considers regional blockades not as an alternative to general anesthesia, but as a component of the latter, allowing a significant reduction in the concentration of both inhalation and non inhalation anesthetics, narcotic analgesics and muscle relaxants. It should be noted that the methods of central anesthesia provide an exceptionally effective postoperative analgesia with preservation of consciousness, motor activity and low risk of respiratory depression. Acute pain in the postoperative period increases the rigidity of the muscles of the chest and anterior abdominal wall, which leads to a decrease in the respiratory volume, vital capacity of lungs, functional residual capacity and alveolar ventilation. e consequence of this is the collapse of the alveoli, hypoxemia and decreased blood oxygenation. Activation of the autonomic nervous system against the background of pain syndrome increases the tone of the smooth musculature of the intestine with a decrease in peristaltic activity and the development of the postoperative paresis. us, on the basis of modern clinical and experimental studies, it has been established that general anesthesia, by eliminating the perception of pain, does not provide a blockade of the Research Article Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children Nasibova EM* and Polukhov R Sh Department of Pediatric Surgery, Azerbaijan Medical University, Azerbaijan Article Information Received date: Jan 26, 2018 Accepted date: Jan 30, 2018 Published date: Feb 15, 2018 *Corresponding author Nasibova EM, Department of Pediatric Surgery, Azerbaijan Medical University, Brazil, Email: [email protected]Distributed under Creative Commons CC-BY 4.0 Keywords General Anesthesia; Caudal Block; Naropin; Promedol Abstract Currently, among the regional methods of anesthesia, caudal anesthesia is most popular in pediatric practice in young children. Objective: To improve the safety of patients and improve the effectiveness of anesthetic protection of young children with Hirschsprung disease in transrectal resection of the large intestine by comparing various methods of anesthesia and creating an effective and safe anesthesia regimen. Material and methods of research: The study included 25 children with Hirschsprung disease who underwent transrectal resection of the large intestine. All investigated patients are divided into 2 groups depending on the chosen method of anesthesia. In I clinical group (n = 13) multicomponent endotracheal anesthesia with high doses of fentanyl was selected by anesthesia, in II clinical group (n = 12), operative interventions were performed under general anesthesia combined with caudal block. Results of the study: The level of cortisol in patients of the II group at the 2 nd stage of the study significantly decreased by 22%, which indicated the adequacy of this technique of anesthesia. Also in patients of this group at the 4 th stage of the study, the level of cortisol and glucose did not change. And in Group I patients who underwent multicomponent general anesthesia with high doses of fentanyl, at the 4 th stage of the study there was a significant increase in the level of cortisol and glucose by 35% and 24%, respectively. And this indicates the appearance of severe pain 24 hours after the operation. Conclusion: 1. Caudal anesthesia combined with general anesthesia provides a reliable analgesic effect and miorelaxation in transrectal resection of the colon in Hirschsprung disease in young children. 2. The combined administration of promedol with naropin into the caudal canal prolongs the analgesic effect up to 24 hours, which was confirmed by the stability of the indices of central hemodynamics and stress markers.
Transcript
SM Journal of Pediatrics
Gr upSM
How to cite this article Nasibova EM and Polukhov RS. Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children.
SM J Pediatr. 2018; 3(1): 1015.OPEN ACCESS
IntroductionThe rapid development of surgery was a powerful stimulus for the further expansion and
improvement of the methods of anesthesia. Transrectal resection of the large intestine in Hirschsprung’s disease in young children is a new approach to solving this problem in this category of patients. Children of early age due to anatomical and physiological characteristics belong to the group of high anesthetic risk due to the rapid development and progression of pathological conditions. Therefore, when choosing an anesthetic benefit in children of this age, it is necessary to seek to minimize the negative properties of the methods used. Given the trend of a multimodal approach to anesthesia, regional anesthesia has become increasingly prevalent in recent years. Currently, among the regional methods of anesthesia, caudal anesthesia in pediatric practice [1-3] is the most popular.
The present concept of “balanced regional anesthesia” considers regional blockades not as an alternative to general anesthesia, but as a component of the latter, allowing a significant reduction in the concentration of both inhalation and non inhalation anesthetics, narcotic analgesics and muscle relaxants. It should be noted that the methods of central anesthesia provide an exceptionally effective postoperative analgesia with preservation of consciousness, motor activity and low risk of respiratory depression. Acute pain in the postoperative period increases the rigidity of the muscles of the chest and anterior abdominal wall, which leads to a decrease in the respiratory volume, vital capacity of lungs, functional residual capacity and alveolar ventilation. The consequence of this is the collapse of the alveoli, hypoxemia and decreased blood oxygenation. Activation of the autonomic nervous system against the background of pain syndrome increases the tone of the smooth musculature of the intestine with a decrease in peristaltic activity and the development of the postoperative paresis. Thus, on the basis of modern clinical and experimental studies, it has been established that general anesthesia, by eliminating the perception of pain, does not provide a blockade of the
Research Article
Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young ChildrenNasibova EM* and Polukhov R ShDepartment of Pediatric Surgery, Azerbaijan Medical University, Azerbaijan
Article Information
Received date: Jan 26, 2018 Accepted date: Jan 30, 2018 Published date: Feb 15, 2018
*Corresponding author
Nasibova EM, Department of Pediatric Surgery, Azerbaijan Medical University, Brazil, Email: [email protected]
Distributed under Creative Commons CC-BY 4.0
Keywords General Anesthesia; Caudal Block; Naropin; Promedol
Abstract
Currently, among the regional methods of anesthesia, caudal anesthesia is most popular in pediatric practice in young children.
Objective: To improve the safety of patients and improve the effectiveness of anesthetic protection of young children with Hirschsprung disease in transrectal resection of the large intestine by comparing various methods of anesthesia and creating an effective and safe anesthesia regimen.
Material and methods of research: The study included 25 children with Hirschsprung disease who underwent transrectal resection of the large intestine. All investigated patients are divided into 2 groups depending on the chosen method of anesthesia. In I clinical group (n = 13) multicomponent endotracheal anesthesia with high doses of fentanyl was selected by anesthesia, in II clinical group (n = 12), operative interventions were performed under general anesthesia combined with caudal block.
Results of the study: The level of cortisol in patients of the II group at the 2 nd stage of the study significantly decreased by 22%, which indicated the adequacy of this technique of anesthesia. Also in patients of this group at the 4th stage of the study, the level of cortisol and glucose did not change. And in Group I patients who underwent multicomponent general anesthesia with high doses of fentanyl, at the 4th stage of the study there was a significant increase in the level of cortisol and glucose by 35% and 24%, respectively. And this indicates the appearance of severe pain 24 hours after the operation.
Conclusion: 1. Caudal anesthesia combined with general anesthesia provides a reliable analgesic effect and miorelaxation in transrectal resection of the colon in Hirschsprung disease in young children.
2. The combined administration of promedol with naropin into the caudal canal prolongs the analgesic effect up to 24 hours, which was confirmed by the stability of the indices of central hemodynamics and stress markers.
Citation: Nasibova EM and Polukhov RS. Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children. SM J Pediatr. 2018; 3(1): 1015. Page 2/4
Gr upSM Copyright Nasibova EM
passage of nociceptive impulses, even at the suprasegmental level, not to mention the spinal level [4-6]. Narcotic analgesics introduced into the blood do not provide sufficient blockade of the opiate receptors of the horn of the spinal cord. Numerous studies show that the degree of adequacy of anesthesia today is determined by the quality of the protection of the spinal cord. Therefore, regional anesthesia with complete blockage of afferent nociceptive impulses in one form or another should be mandatory and the main component of general anesthesia for intraoperative protection. The search for the most effective and improvement of known, and most importantly safe methods of anesthetic protection of young children with transrectal resection of the large intestine in Hirschsprung disease determines the urgency of this problem.
Objective
To improve the safety of patients and improve the effectiveness of anesthetic protection of young children with Hirschsprung disease with transrectal resection of the large intestine by comparing various methods of anesthesia and creating an effective and safe anesthesia regimen.
Material and Methods of ResearchThe study was conducted in different surgical bases of the
Department of Pediatric Surgery of AMU between 2014 and 2018. The study included 25 children with Hirschsprung disease who underwent transrectal resection of the large intestine. The age of the patients varied from 3 months to 5 years. The duration of the operation was from 2 to 3 hours. All investigated patients are divided into 2 groups depending on the chosen method of anesthesia. In the 1st clinical group (n = 13), multicomponent endotracheal anesthesia with high doses of fentanyl was selected by anesthesia, in II clinical group (n = 12), operative interventions were administered under general anesthesia combined with caudal block. In the preoperative service, children only older than 6 months were premedicated, which in both groups was standard. In the presence of parents, these children intravenously administered propofol in a dose of 2 mg/kg and then the child in a half-awake state was delivered to the operating unit. On the operating table, all patients underwent standard monitoring. Patients of group I (n = 13) had multicomponent endotracheal anesthesia with high doses of fentanyl. Introductory anesthesia in this group was carried out using O2: Air = 1:1 in combination with sevorane 6-8% and fentanyl at a rate of 3 μg/kg. After administering 0.6 mg/kg of rocuronium bromide, the patient was intubated and switched on to the ventilator. Basis anesthesia was carried out with sevorane 2% and
high doses of fentanyl 8-10 μg/kg/h. Total myoplegia was performed with maintenance doses of rocuronium bromide at a rate of 0.1 mg/kg as needed. Group II patients underwent general anesthesia with caudal block. Induction of anesthesia in patients of this group was carried out using propofol at a rate of 3 mg/kg. After the patient completely fell asleep, rocuronium bromide was administered intravenously at a rate of 0.6 mg/kg, and after irrigation of the vocal cords with an aerosol of 10% lidocaine, intubation of the trachea was performed. Maintenance of anesthesia was performed with an inhalational anesthetic of isoflurane 0.6-0.8% by volume. All patients underwent mechanical ventilation in normocapnia mode (EtCO2 36-40 mm Hg) using the Drager Fabius apparatus. After induction into anemia, the patient was transferred to the left block to perform the caudal block. With a satisfactory caudal block, patients of this group did not need fentanyl and muscle relaxant throughout the operation.
The total score for the CRIES scale is calculated as the sum of the scores for all five criteria. The maximum score is 10, the minimum score is 0, the higher the score, the greater the pain.
Technique for Conducting the Caudal Block In our daily practice in the implementation of the caudal block,
we lay patients on the left side without strong bending of the legs in the knee joints. Depending on the age, we used epikan needles for the caudal block. In young children, the sacrum gap is easily determined, since the anatomical landmarks are more superficial. The sacral slit has the shape of an inverted U and is covered with a sacrococcygeal ligament. Puncture is performed between the two horns in the upper third of the sacrococcygeal ligament, since there it has the maximum thickness and gives a noticeable “click” when the needle passes. The puncture needle is guided initially at an angle of 90° to the surface of the skin, followed by a 30-40° turn in the cranial direction, its cut is directed ventrally, and after passing through the ligament the needle is redirected 3-4 mm into the caudal canal. In our daily practice, we use the “no turn technique” technique, which consists in puncturing the sacrococcygeal ligament at an angle of 60° without holding the needle into the caudal canal. After the aspiration test, if blood and liquor are not aspirated, then narupin is administered at the rate of 3 mg/kg in a volume of 1.2 ml/kg in dilution with saline and promedol 0.2 mg/kg for 60-90 seconds (Tables 1 and 2).
To determine the adequacy of our anesthesia techniques for transrectal resection of the large intestine, we studied the indices of central hemodynamics and stress markers (cortisol and glucose in the blood) in 4 stages of the study: stage 1- the beginning of the operation (skin incision), stage 2- the most traumatic stage of the operation, the
Table 1: Dynamics of indices of central hemodynamics.
Group of patients Stages of research Heart rate, sec-1 BPaver. mm.Hg Cardiac Index, l / (min × m2)
I (general anesthesia without caudal block)
I stage (skin incision) 147,5±7,1 51,2±2,9 3,59±0,14
II stage (traumatic moment of operation) 182,3±6,4 66,2±3,2 4,47±0,09
III stage (end of operation) 172,5±8,9 62,1±2,13 4,52±0,16
II (general anesthesia with caudal block)
IV stage (24 hours after surgery) 193,4±7,5 69,8±3.1 5,2±0,12
I stage (skin incision) 140,8±6,2 49,5±2,5 3,21±0,22
II stage (traumatic moment of operation) 126,7±5,8 46,6±1,7 3,18±0,11
III stage (end of operation) 121,6±5,2 48,7±2,2 3,42±0,12
IV stage (24 hours after surgery) 140,5±5,8 49,2±2,3 3,19±0,24
Citation: Nasibova EM and Polukhov RS. Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children. SM J Pediatr. 2018; 3(1): 1015. Page 3/4
Gr upSM Copyright Nasibova EM
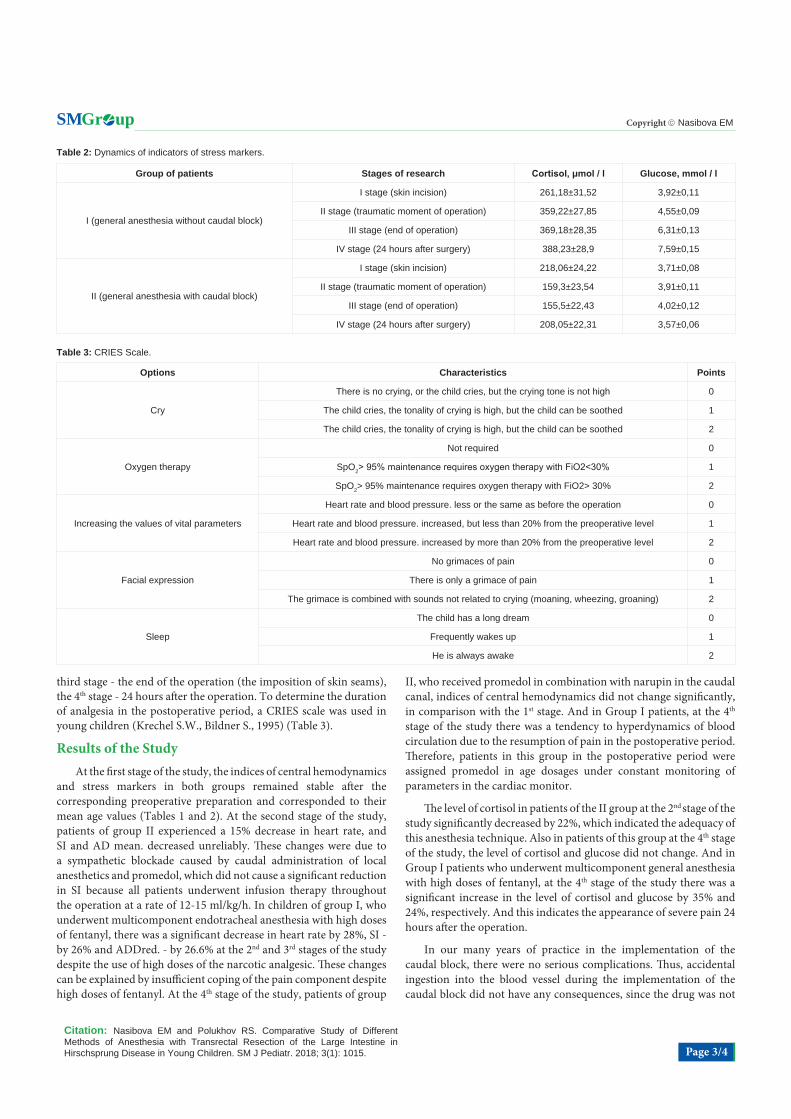
third stage - the end of the operation (the imposition of skin seams), the 4th stage - 24 hours after the operation. To determine the duration of analgesia in the postoperative period, a CRIES scale was used in young children (Krechel S.W., Bildner S., 1995) (Table 3).
Results of the StudyAt the first stage of the study, the indices of central hemodynamics
and stress markers in both groups remained stable after the corresponding preoperative preparation and corresponded to their mean age values (Tables 1 and 2). At the second stage of the study, patients of group II experienced a 15% decrease in heart rate, and SI and AD mean. decreased unreliably. These changes were due to a sympathetic blockade caused by caudal administration of local anesthetics and promedol, which did not cause a significant reduction in SI because all patients underwent infusion therapy throughout the operation at a rate of 12-15 ml/kg/h. In children of group I, who underwent multicomponent endotracheal anesthesia with high doses of fentanyl, there was a significant decrease in heart rate by 28%, SI - by 26% and ADDred. - by 26.6% at the 2nd and 3rd stages of the study despite the use of high doses of the narcotic analgesic. These changes can be explained by insufficient coping of the pain component despite high doses of fentanyl. At the 4th stage of the study, patients of group
II, who received promedol in combination with narupin in the caudal canal, indices of central hemodynamics did not change significantly, in comparison with the 1st stage. And in Group I patients, at the 4th stage of the study there was a tendency to hyperdynamics of blood circulation due to the resumption of pain in the postoperative period. Therefore, patients in this group in the postoperative period were assigned promedol in age dosages under constant monitoring of parameters in the cardiac monitor.
The level of cortisol in patients of the II group at the 2nd stage of the study significantly decreased by 22%, which indicated the adequacy of this anesthesia technique. Also in patients of this group at the 4th stage of the study, the level of cortisol and glucose did not change. And in Group I patients who underwent multicomponent general anesthesia with high doses of fentanyl, at the 4th stage of the study there was a significant increase in the level of cortisol and glucose by 35% and 24%, respectively. And this indicates the appearance of severe pain 24 hours after the operation.
In our many years of practice in the implementation of the caudal block, there were no serious complications. Thus, accidental ingestion into the blood vessel during the implementation of the caudal block did not have any consequences, since the drug was not
Table 2: Dynamics of indicators of stress markers.
Group of patients Stages of research Cortisol, μmol / l Glucose, mmol / l
I (general anesthesia without caudal block)
I stage (skin incision) 261,18±31,52 3,92±0,11
II stage (traumatic moment of operation) 359,22±27,85 4,55±0,09
III stage (end of operation) 369,18±28,35 6,31±0,13
IV stage (24 hours after surgery) 388,23±28,9 7,59±0,15
II (general anesthesia with caudal block)
I stage (skin incision) 218,06±24,22 3,71±0,08
II stage (traumatic moment of operation) 159,3±23,54 3,91±0,11
III stage (end of operation) 155,5±22,43 4,02±0,12
IV stage (24 hours after surgery) 208,05±22,31 3,57±0,06
Table 3: CRIES Scale.
Options Characteristics Points
Cry
There is no crying, or the child cries, but the crying tone is not high 0
The child cries, the tonality of crying is high, but the child can be soothed 1
The child cries, the tonality of crying is high, but the child can be soothed 2
Oxygen therapy
Not required 0
SpO2> 95% maintenance requires oxygen therapy with FiO2˂30% 1
SpO2> 95% maintenance requires oxygen therapy with FiO2> 30% 2
Increasing the values of vital parameters
Heart rate and blood pressure. less or the same as before the operation 0
Heart rate and blood pressure. increased, but less than 20% from the preoperative level 1
Heart rate and blood pressure. increased by more than 20% from the preoperative level 2
Facial expression
No grimaces of pain 0
There is only a grimace of pain 1
The grimace is combined with sounds not related to crying (moaning, wheezing, groaning) 2
Sleep
The child has a long dream 0
Frequently wakes up 1
He is always awake 2
Citation: Nasibova EM and Polukhov RS. Comparative Study of Different Methods of Anesthesia with Transrectal Resection of the Large Intestine in Hirschsprung Disease in Young Children. SM J Pediatr. 2018; 3(1): 1015. Page 4/4
Gr upSM Copyright Nasibova EM
administered. The expected puncture of the dura mater occurs usually due to excessive penetration of the needle into the caudal canal due to improper caudal blocking techniques. This complication was not observed in any patient.
Conclusion1. Caudal anesthesia combined with general anesthesia provides a
reliable analgesic effect and miorelaxation in transrectal resection of the colon in Hirschsprung disease in young children.
2. The combined administration of promedol with narupin into the caudal canal prolongs the analgesic effect up to 24 hours, which was confirmed by the stability of the indices of central hemodynamics and stress markers.
References
1. Sichkar S Yu. Epidural analgesia in newborns in the perioperative and postoperative period. Anesthesiology and resuscitation. 2015; 3: 65-68.