Introduction: Fractures of distal tibia are usually due to high velocity injuries with extensive damage tothe soft tissue. The best modality of method of management for distal tibial fracture is one that achieves agood reduction and stability and minimizes soft tissue compromise as well as devascularization of the bonyfragments. The aim of our study is to compare, analyse and individualize the best modality of treatment formanagement of distal tibial fractures.Materials and Methods: This study of 30 patients of distal tibial fractures, was conducted at Dr. D.Y.Patil Medical College and Research Center, Pimpri, Pune, from September 2018 - August 2020. Requiredconsents from all the patients and ethical committee clearance was taken before conducting the study.Necessary data was collected from all the patients during their hospital stay and regular follow-up wasrecorded.Results: Patients treated with Intra-Medullary Nail had mean AOFAS (American Orthopaedic Foot andAnkle Society) score of 75.2, while patients treated with External Fixator and MIPO (Minimally InvasivePercutaneous Osteosynthesis) had mean AOFAS(American Orthopaedic Foot and Ankle Society) score71.5 and 87.1 respectively.Conclusion: In our study, we have analysed overall results including functional recovery, radiologicalassessment in terms of malalignment and complications related to different modalities of treatment ofdistal tibial fractures.
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative CommonsAttribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build uponthe work non-commercially, as long as appropriate credit is given and the new creations are licensed underthe identical terms.
In non-fatal road traffic injuries, fractures are thecommonest injuries. Bones of the lower extremity arecommonly involved in road traffic accidents. Gravitationalforce and velocity of the vehicle at the time of trauma hasshown to play a major role in such types of injury.
The commonest long bone fractured and most commonopen one is tibia. According to the location in the tibia bone;distal tibia has 2nd highest incidence of the fracture.1
Fractures of distal tibia are usually due to high velocityinjuries with extensive damage to the soft tissue. Surgeonsface a dilemma over whether to give importance to softtissue healing or to anatomic reduction and articularcongruity while managing these fractures.
Orthopaedicians have been challenged with problemslike mal-union, delayed union, non-union and wounddehiscence due to poor soft tissue coverage, reducedvascularity of distal tibia region and associated soft tissueinjury.
Anatomic reduction of the articular surface, restorationof fracture alignment, proper soft tissue handling and earlyankle mobilization has shown effective results in managing
202 Solanki et al. / Indian Journal of Orthopaedics Surgery 2021;7(3):201–206
distal tibial fractures.Ruedi and Allgower2 presented their landmark paper in
1969, in which at 4 years follow up 74% patients had goodfunctional outcome, revolutionized the treatment protocol ofdistal tibia fractures.
Then, the decades of 1970’s and 1980’s saw extensiveuse of the principles of open reduction and internal fixationin the treatment of distal tibia fractures but shockingly it wasassociated with high rate of complications like non-union,superficial infection, osteomyelitis, arthrodesis, below kneeamputation, post-traumatic osteoarthritis, and malunion.3,4
Due to these complications Surgeons realised theimportance of soft tissue management in distal tibialfractures. In another analysis5 by Ruedi and Allgower inwhich they showed good results at 9 years of follow up, butmost of the patients they studied had low-energy injuries sostandard protocol for these types of injuries could not set.
In 1979 Ruedi and Allgower came up with another studyin which patients had high energy injuries and came to theconclusion that the overall results were better in low energyinjuries compared to high energy injuries.6 Appropriatesoft tissue management along with fixation of fracture gavebetter results.7,8
Open reduction and internal fixation, joint spanningexternal fixator, hybrid external fixator, ilizarov fixatorapplication, closed reduction and internal fixation withintra medullary nailing, biological minimally invasiveplate osteosynthesis (MIPO) are the various modalities oftreatment in these types of fractures.
Method selected for stabilization should be sufficientenough to maintain the reduction.
The best modality of method of management for distaltibial fracture is one that achieves a good reduction andstability and minimizes soft tissue compromise as well asdevascularization of the bony fragments.
Choosing a modality of treatment method for distal tibiafracture remains difficult and controversial because the finalresults depends upon multiple factors like the status of softtissue,degree of comminution and involvement of articularsurface. We aimed to attain anatomic reduction of articularsurface and at the same time providing stability to thefracture. This aim should be attained using methods whichdecreases bone and soft tissue devascularisation.
Usually distal tibial fractures occur due to high velocitytrauma and it presents with extensive soft tissue damage. So,it creates a dilemma whether to give priority to soft tissue orarticular congruity and anatomic reduction.
Advanced surgical methods have developed over theyears with improvement in understanding of biomechanics,biology and biomaterials which have finally led to betterfunctional outcome for patients. Initially more weightagewas given to anatomical reduction and rigid fixation to attainstability. Damage to soft tissue surrounding the fracture sitehas led to increased rate of delayed union and non-union
making this method discouraging.Thus, technique which gave more weightage to biology
than stability emerged and evolved with the time.The aim of our study is to compare, analyse and
individualize the best modality of treatment for managementof distal tibial fractures.
2. Materials and Methods
This study of 30 patients of distal tibial fractures, wasconducted at Dr. D.Y. Patil Medical College and ResearchCenter, Pimpri, Pune, from September 2018 - August2020. Required consents from all the patients and ethicalcommittee clearance was taken before conducting the study.During above mentioned period total 30 patients weretreated for distal tibial fracture using different modalitiesaccording to the fracture pattern and skin condition.Necessary data was collected from all the patients duringtheir hospital stay and regular follow-up was recorded.
2.1. Inclusion & exclusion criteria
Patient presenting with distal tibia fracture, patients with agegroup of 15-64 years and
patients who were fit for the surgery were included inthe study while patients below 15 years and above 65years, patients with crush injuries having neurovascularimpairment and pre-existing deformity of concerned partwere excluded.
2.2. Factors considered for choosing different treatmentmodalities
IM nail as a fixation method was chosen in cases wherethere was minimal soft tissue injury, less comminution andno articular involvement. MIPO technique was preferred incases with minimal soft tissue injury, severe comminutionand fracture location above the articular suface.ExternalFixation was chosen in cases with extensive soft tissuedamage and extended articular comminution.
2.3. Functional outcome estimation
To estimate the functional outcome in our study we haveused The American Orthopaedic Foot and Ankle Societyscore.
2.4. Post-operative protocol
On Post-Operative day 12 or 14th depending upon the statusof the wound, sutures were removed. And weight bearingwas started once the radiographic evidence of bone unionwas seen and then then weight bearing was progressed astolerated by the patients. Average time of starting partialweight bearing was 8-10 weeks except in cases with MIPOplating where it was delayed and started by 12-14 weeks. On
Solanki et al. / Indian Journal of Orthopaedics Surgery 2021;7(3):201–206 203
average partial weight bearing was started by 8-10 weeksexcept in cases treated with MIPO where weight bearingwas delayed and started by 12-14 weeks.
3. Observations and Results
Table 1: Number and percentage of patients belonging todifferent age groups
Age group Number Percentage11-20 1 3.321-30 8 26.731-40 7 23.341-50 5 16.751-60 6 20.0>60 3 10.0Total 30 100.0
Table 2: Shows prevalence of Gustilo Anderson (GA) type offractures among the patients
Type Number Percentage1 4 13.32 1 3.33A 5 16.7No GA type 20 66.7Total 30 100.0
Table 3: Shows distribution of the patients according to AOclassification
AO classification Number PercentageA1 8 26.7A2 2 6.7A3 15 50.0B1 1 3.3C1 1 3.3C2 1 3.3C3 2 6.7Total 30 100.0
4. Discussion
In our study around 33.3% of the patients had openinjuries which delayed the definitive surgical proceduresand managed initially by calcaneal pin traction till thehealing of the wound. Calcaneal pin traction procedure hasbeen immensely helpful to us in our set up to temporarystabilization of the fracture while we await soft tissue to behealed before going for a definitive surgery.
In between September 2018-August 2020 we treatedtotal 30 patients from which 30% of patients (9 patients)were with IM nail, while 20% patients (6 patients) weretreated with external fixator and 50% of patients (15patients) were treated with MIPO. The average age of
Fig. 1: Case 1
Fig. 2: Case 1
Fig. 3: Case 2
204 Solanki et al. / Indian Journal of Orthopaedics Surgery 2021;7(3):201–206
Table 4: Number and percentage of different modalities in different AO type of fracture among the patients
AO Type IM Nail Ext.Fix MIPO p -valueNumber % Number % Number %A1 6 75.0 0 0 2 25.0
*One patient with Ext.Fix had both wound discharge and ankle stiffness# Percentages are calculated for each column
Table 7: Number and percentage of Varus and Valgus deformity in different modality of treatment
Complications IM Nail Ext Fix* MIPO Total; p -valueNumber % Number % Number %Varus deformity 2 22.2 1 16.7 0 0 3 0.178Valgus deformity 2 22.2 4 66.7 2 13.3 8 0.042
# Percentages are calculated for each column
patients with such injuries in our study was 40.5 years(Range 18 to 64 years) which is comparable to that of otherstudies and around 66% patients being in the range of 21to 50 years which suggest high energy trauma as a leadingcause for such fractures. This is comparable with a studyconducted by Cory Colling et al.9 in his study the averageage of patients with was 43, ranging from 17 to 62 yearsand Vallier et al.10 had patients with average age of 39.1year ranging from 16 to 77 years.
Our Study had 33.3% patients with open injuries and66.7% with closed injuries.This was comparable with thestudies done by Heather A Vallier et al; his study had 30%open injuries and 70% closed injuries. Study conducted byHazarika et al11 had 40% open fractures and 60% closedfractures.
Patients treated with IM nail had mean AOFAS score of75.2, while patients treated with External Fixator and MIPO
had mean AOFAS score 71.5 and 87.1 respectively. ThisAOFAS score was comparable to study conducted by PierreJoveniaux et al.12 where mean AOFAS score of externalfixations and limited internal fixation (MIPO) was 67.7 and85.2 respectively.
5. Conclusion
In our study treatment was individualized based on the type,nature of the wound, time of presentation, associated injuryand the available facilities of treatment.
In our study we have found that choosing a treatmentmethod which considers soft tissue status and fracturepattern yields better results.
In cases where soft tissue injury is minimal, lesscomminution is present and when there is no articularinvolvement; IM nail gives better result and it has advantage
Solanki et al. / Indian Journal of Orthopaedics Surgery 2021;7(3):201–206 205
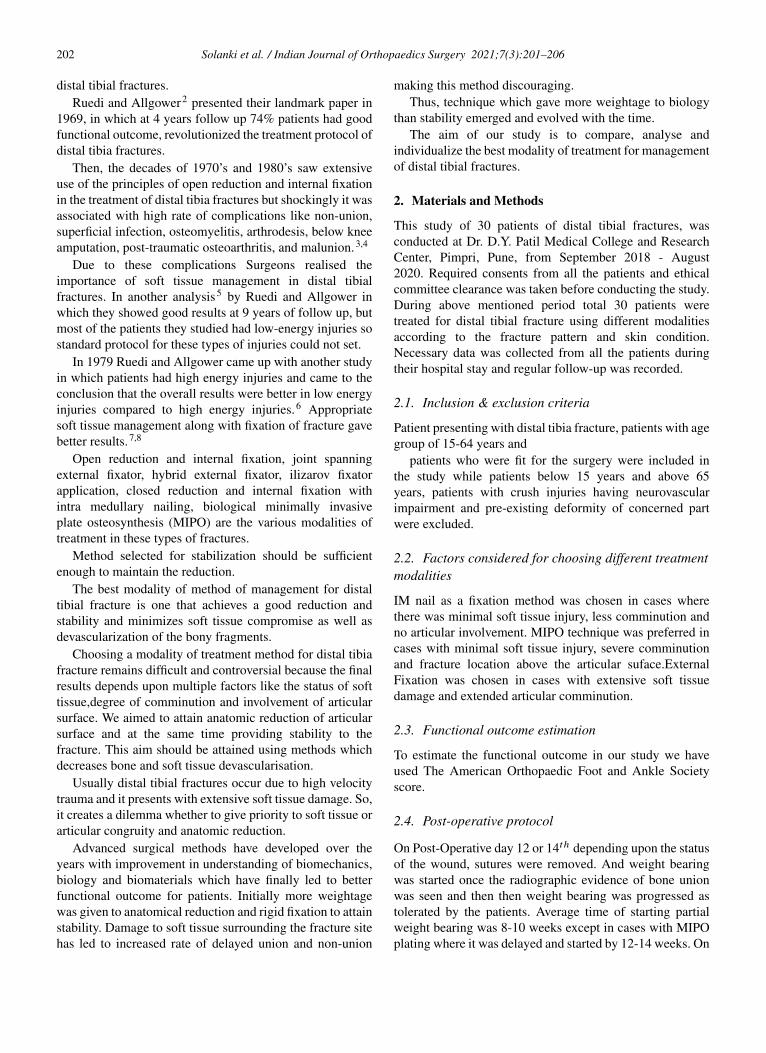
Fig. 4:
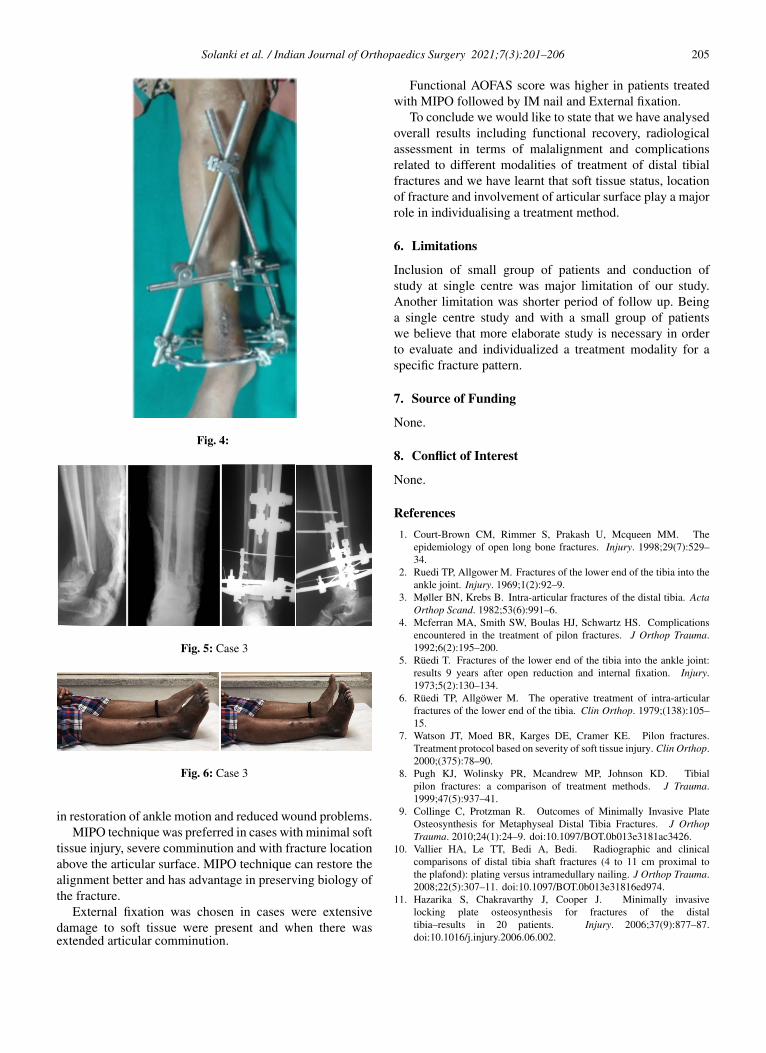
Fig. 5: Case 3
Fig. 6: Case 3
in restoration of ankle motion and reduced wound problems.MIPO technique was preferred in cases with minimal soft
tissue injury, severe comminution and with fracture locationabove the articular surface. MIPO technique can restore thealignment better and has advantage in preserving biology ofthe fracture.
External fixation was chosen in cases were extensivedamage to soft tissue were present and when there wasextended articular comminution.
Functional AOFAS score was higher in patients treatedwith MIPO followed by IM nail and External fixation.
To conclude we would like to state that we have analysedoverall results including functional recovery, radiologicalassessment in terms of malalignment and complicationsrelated to different modalities of treatment of distal tibialfractures and we have learnt that soft tissue status, locationof fracture and involvement of articular surface play a majorrole in individualising a treatment method.
6. Limitations
Inclusion of small group of patients and conduction ofstudy at single centre was major limitation of our study.Another limitation was shorter period of follow up. Beinga single centre study and with a small group of patientswe believe that more elaborate study is necessary in orderto evaluate and individualized a treatment modality for aspecific fracture pattern.
7. Source of Funding
None.
8. Conflict of Interest
None.
References1. Court-Brown CM, Rimmer S, Prakash U, Mcqueen MM. The
epidemiology of open long bone fractures. Injury. 1998;29(7):529–34.
2. Ruedi TP, Allgower M. Fractures of the lower end of the tibia into theankle joint. Injury. 1969;1(2):92–9.
3. Møller BN, Krebs B. Intra-articular fractures of the distal tibia. ActaOrthop Scand. 1982;53(6):991–6.
4. Mcferran MA, Smith SW, Boulas HJ, Schwartz HS. Complicationsencountered in the treatment of pilon fractures. J Orthop Trauma.1992;6(2):195–200.
5. Rüedi T. Fractures of the lower end of the tibia into the ankle joint:results 9 years after open reduction and internal fixation. Injury.1973;5(2):130–134.
6. Rüedi TP, Allgöwer M. The operative treatment of intra-articularfractures of the lower end of the tibia. Clin Orthop. 1979;(138):105–15.
7. Watson JT, Moed BR, Karges DE, Cramer KE. Pilon fractures.Treatment protocol based on severity of soft tissue injury. Clin Orthop.2000;(375):78–90.
8. Pugh KJ, Wolinsky PR, Mcandrew MP, Johnson KD. Tibialpilon fractures: a comparison of treatment methods. J Trauma.1999;47(5):937–41.
9. Collinge C, Protzman R. Outcomes of Minimally Invasive PlateOsteosynthesis for Metaphyseal Distal Tibia Fractures. J OrthopTrauma. 2010;24(1):24–9. doi:10.1097/BOT.0b013e3181ac3426.
10. Vallier HA, Le TT, Bedi A, Bedi. Radiographic and clinicalcomparisons of distal tibia shaft fractures (4 to 11 cm proximal tothe plafond): plating versus intramedullary nailing. J Orthop Trauma.2008;22(5):307–11. doi:10.1097/BOT.0b013e31816ed974.
11. Hazarika S, Chakravarthy J, Cooper J. Minimally invasivelocking plate osteosynthesis for fractures of the distaltibia–results in 20 patients. Injury. 2006;37(9):877–87.doi:10.1016/j.injury.2006.06.002.
206 Solanki et al. / Indian Journal of Orthopaedics Surgery 2021;7(3):201–206
12. Joveniaux P, Ohl X, Harisboure A. Distal tibia fractures: managementand complications of 101 cases. Int Orthop (SICOT). 2010;34:583–8.
Author biography
Raviraj Solanki, Junior Resident
Rahul M Salunkhe, Professor
Ishan R Shevate, Assistant Professor
Ashwin Deshmukh, Associate Professor
Anirudh Kumar Singh Kandari, Senior Resident
Cite this article: Solanki R, Salunkhe RM, Shevate IR, Deshmukh A,Kandari AKS. Comparison between outcome of various modalities ofmanagement of distal tibia fractures. Indian J Orthop Surg2021;7(3):201-206.