hi Jomal of Emergency Medicine Vol 5 pp 197 -208. 1987 Pmted r the USA ?? Copyright 1987 Perqamon Journals Ltd ------iiizEzi Prehospital Care- COMPARISON OF PREHOSPITAL TRAUMA TRIAGE INSTRUMENTS IN A SEMIRURAL POPULATION Jerris R. Hedges, MD, MS, FACEP,* Stan Feero, MD,t Brian Moore, BS, EMT-P,* Dennis W. Haver, BS,* Bette Shultzt *Department of Emergency Medlclne University of Clnclnnatl College of Medlclne. tThurston County Medic I, Emergency MedIcal Services System, Olympia, WashIngton Reprint address Jerrls R Hedges MD klS FACEP Department of Emergency Medlclne, Urxverslty of Clnclnnatl College of Medtclne 234 Goodman Street, M L 769 Clnclnnatl. OH 4 17 Abstract-An essential feature of the trau- ma center concept is the rapid delivery of pa- tients with complicated injuries to a regional trauma center directly from the site of injury. A variety of triage instruments have been pro- posed to aid the prehospital personnel in mak- ing this difficult triage decision. We used a combination of prospective and retrospective analysis to evaluate and compare the perfor- mance of 11 recommended triage instruments on the same trauma population. Of the 130 patients evaluated by paramedics in a semirural area, 41 patients were considered desirable for trauma center triage. These patients were iden- tified by either the absence of vital signs in the prehospital setting, death in the emergency department, immediate surgery other than for orthopedic extremity injury, or immediate ad- mission to the intensive care unit. All sub- sequent in-hospital deaths occurred in the group of patients identified as deserving trauma center triage. Of the triage instruments, the Kane’s “revised” checklist provided the largest improvement in odds against needing a trauma center when the triage instrument is negative. Of the triage instruments with a sensitivity > 70%, the respiratory/systolic pressure/ Glasgow Coma Scale (RSG) score provided the largest improvement in odds for needing a trauma center when the triage instrument is positive. Although no triage instrument per- formed ideally, the patients missed by the triage instruments having a sensitivity >70% were hemodynamically stable. Transfer of such patients to a trauma center following determi- nation of the extent of underlying injury at a referring emergency department should he possible. U Keywords-trauma center; triage; trauma score; CRAMS scale; prehospital index; prehospital care: trauma triage Introduction Successful implementation of the trauma center concept is dependent upon the rap- id delivery of patients with complicated injuries requiring high-level surgical care Prehospital Care focuses on the issues and practices that directly affect the type and B quality of care administered by the emergency physician in the emergency department; _- and is coordinated by fe/er Ports, MD, Saint Joseph’s Hospital, Denver, Colorado. -_ RECEIVED: 28 August 1986; ACCEPTED: 21 October 1986 0736-4679/87 $3.00 +- .OO
Transcript
hi Jomal of Emergency Medicine Vol 5 pp 197 -208. 1987 Pmted r the USA ?? Copyright 1987 Perqamon Journals Ltd
------iiizEzi Prehospital Care-
COMPARISON OF PREHOSPITAL TRAUMA TRIAGE INSTRUMENTS IN A SEMIRURAL POPULATION
Jerris R. Hedges, MD, MS, FACEP,*
Stan Feero, MD,t Brian Moore, BS, EMT-P,* Dennis W. Haver, BS,* Bette Shultzt
*Department of Emergency Medlclne University of Clnclnnatl College of Medlclne. tThurston County Medic I, Emergency MedIcal Services System, Olympia, WashIngton Reprint address Jerrls R Hedges MD klS FACEP Department of Emergency Medlclne,
Urxverslty of Clnclnnatl College of Medtclne 234 Goodman Street, M L 769 Clnclnnatl. OH 4
17 Abstract-An essential feature of the trau- ma center concept is the rapid delivery of pa- tients with complicated injuries to a regional trauma center directly from the site of injury. A variety of triage instruments have been pro- posed to aid the prehospital personnel in mak- ing this difficult triage decision. We used a combination of prospective and retrospective analysis to evaluate and compare the perfor- mance of 11 recommended triage instruments on the same trauma population. Of the 130 patients evaluated by paramedics in a semirural area, 41 patients were considered desirable for trauma center triage. These patients were iden- tified by either the absence of vital signs in the prehospital setting, death in the emergency department, immediate surgery other than for orthopedic extremity injury, or immediate ad- mission to the intensive care unit. All sub- sequent in-hospital deaths occurred in the group of patients identified as deserving trauma center triage. Of the triage instruments, the Kane’s “revised” checklist provided the largest improvement in odds against needing a trauma center when the triage instrument is negative.
Of the triage instruments with a sensitivity > 70%, the respiratory/systolic pressure/ Glasgow Coma Scale (RSG) score provided the largest improvement in odds for needing a trauma center when the triage instrument is positive. Although no triage instrument per- formed ideally, the patients missed by the triage instruments having a sensitivity >70% were hemodynamically stable. Transfer of such patients to a trauma center following determi- nation of the extent of underlying injury at a referring emergency department should he possible.
Successful implementation of the trauma center concept is dependent upon the rap- id delivery of patients with complicated injuries requiring high-level surgical care
Prehospital Care focuses on the issues and practices that directly affect the type and B quality of care administered by the emergency physician in the emergency department; _- and is coordinated by fe/er Ports, MD, Saint Joseph’s Hospital, Denver, Colorado.
-_ RECEIVED: 28 August 1986; ACCEPTED: 21 October 1986 0736-4679/87 $3.00 +- .OO
198 J. R. Hedges, S. Feero, B. Moore, D. W. Haver, B. Shultz
to a trauma center. The development of emergency medical services (EMS) sys- tems with physician-directed prehospital personnel offers not only the potential for earlier prehospital initiation of trauma care, but also the means whereby sophisti- cated decisions regarding the disposition of the traumatized patient can be made.
Prehospital disposition decisions are complex for several reasons. First, the traumatized patient population is het- erogenous with respect to demographics (eg, geographic location and age), mecha- nisms of injury, physiologic response to injury, and time from injury until medical care. Disposition rules must therefore be flexible to deal with the variability in the patient population.
Second, prehospital triage is controver- sial from the hospital administrator’s per- spective. A hospital that has not been des- ignated as a “trauma center” should continue to receive patients that do not require the specialized services of a trau- ma center. Furthermore, trauma centers with a large population base could be overwhelmed and ineffective if all trauma were diverted to their facility. Unnecessary transport of patients with non-life-threat- ening injuries to regional trauma centers rather than the nearest hospital also may decrease the ability of the prehospital team to respond to other emergency calls.
Third, prehospital disposition deci- sions must be made rapidly with limited information by prehospital personnel un- der challenging conditions. Therefore, the triage criteria must be easily understood by the nonphysician. The triage criteria also must be rapidly and consistently im- plemented under a variety of inclement environmental conditions. Therefore, simplicity and objectivity in the triage in- strument are desired.
A variety of trauma triage instruments have been proposed (Appendix). These in- struments have been developed from phys- iologic measurements, anatomical inju- ries, mechanisms of injury, or some combination of these.rmL4 (Champion HR,
Sacco WJ: Personal communication, Au- gust 1986). The majority of these instru- ments were developed by retrospective da- ta analysis. Prospective comparison of the instruments has been limited. During de- velopment of the instruments, the criteria or “gold standards” used to define which patients should be triaged to a trauma center also have varied. Injury severity scores, the need for operative care, surviv- al, emergency department disposition, and combinations of these criteria have been used for analysis.
This study was designed to prospective- ly evaluate the trauma score (TS), TS and Glasgow Coma Score (GCS) combina- tion, and the prehospital personnel’s ges- talt impression of injury severity (SEV) as triage instruments for trauma center dis- position.ls2,7 With the subsequent develop- ment and recommendation of other triage instruments in the trauma literature, the study was modified to permit retrospec- tive comparison of newer triage instru- ments on the same data set. The following additional triage instruments were stud- ied: the CRAMS scale,8m10 the prehospital index (PHI),“,‘* three abbreviations of the TS (RPM, RSM, and RSG),13~‘4 mecha- nisms of injury (MOI) (alone and in com- bination with TS/GCS),3mh and Kane’s “revised” triage checklist.5 This paper com- pares the ability of these recommended prehospital triage instruments to desig- nate victims of blunt and penetrating trau- ma for trauma center triage using the same semirural population.
Methods
The Thurston County Medic I EMS sys- tem served as the prehospital care system for this study. The EMS system and the county it serves have been described in de- tail elsewhere.’ In brief, the EMS system is a tiered response system that provides pre- hospital medical and trauma care for a semirural county (714 square miles with a
Prehospltal Trauma Triage Instruments 199
population of 124,000) in Washington State. Local fire department basic-life support providers trained at the EMT (81 hour DOT course) level provide initial emergency response in the county. The EMS system uses a central dispatch with “91 1” telephone and police/fire channel access. Three paramedic units staffed by two paramedics each respond to provide advanced-life support at the requesr of the basic-life support providers and per the direction of the EMS dispatcher. All para- medics arc capable of endotracheal intu- bation, intravenous cannulation, applica- tion of pneumatic antishock garments, and administration of intravenous fluids and medications.
Prior to the initiation of this study, the EMS data form was modified to prospec- tively collect GCS, TS, and paramedic se- verity impression information directly from the paramedic record. Paramedic and hospital records of trauma cases seen by the paramedic units of the EMS system during 1982 were reviewed. Patients were initially evaluated at a single facility fol- lowing their injury.’ Patients who were transferred out of the county and for whom there was insufficient medical information to make a determination of severity of injury were excluded from the study.
Calculation of all scores was performed using the EMS data forms. Instruments requiring patient evaluation information (eg, CRAMS scale and Kane’s “revised” triage checklist) were evaluated by careful review of the EMS data sheet narrative re- port. For the CRAMS scale assessment of “abdominal/chest” injury, a score of zero was assigned if mention was made of a flail chest, penetrating injury to the abdo- men or thorax, or if the narrative used the terms rigid, tight, firm, hard, or guarded in reference to the abdominal examina- tion. A score of one was assigned if the narrative otherwise mentioned a tender abdomen or thorax or if abrasions or con- tusions to the abdomen or thorax were noted. A score of two was assigned when
no mention of abdominal or thoracic in- jury or tenderness was made.
Complete descriptions of the various triage instruments are provided in the Ap- pendix. Cut-off criteria for the triage in- struments are listed in Table 1.
Prehospital “trauma center” triage ~1s considered to have been desirable when the patient either was without vital signs in the prehospital setting, died in the emergency department, went from the emergency department to the operating room (OR) for surgery other than for an orthopedic extremity injury, or was admit- ted to the intensive care (ICU). A patient admitted directly to a regular hospital bed was not considered in need of trauma cen- ter triage. These criteria are similar to “gold standard” criteria used in other studies.‘.h.“.“.‘? Determination of trauma center desirability was made indepen- dent of and prior to correlation with tri- age instrument scores. In-hospital deaths occurring after transfer from the emergen- cy department were reviewed after deter- mination of trauma center desirability.
Patients without vital signs in the prc- hospital setting or who died while in the emergency department did not receive an autopsy. Complete patient injury infor- mation was not available on most patients transferred out of the county for tertiary care, therefore injury severity scores (ISS)” were not reported nor were they used to determine appropriateness of triage.
Sensitivity and specificity for trauma center desirability for the triage instru- ments were calculated using standard for- mulae.lh Comparison of these variables amongst triage instruments was made us- ing the two-tailed Fisher exact test on un-- tied pairs. I_ A P value of 0.05 wa!, considered statistically significant.
The triage instruments were also com- pared using likelihood ratio (LR) esti- mates.lh LR + represents the ratio of the posttest to pretest odds for need of trauma center triage given a positive result from the triage instrument. LR - represents the
200 J. R. Hedges, S. Feero, 6. Moore, D. W. Haver, 6. Shultz
Table 1. Triage Instrument Cutoffs
Criteria Send to Trauma Center
TS’,’ TS512 TSIGCS’,’ TSs12orGCSzzlO MOl= MOI = 1 (any index mechanism present) TSIGCSIMOI’-G TS~12orGCS~lOorMOI=l SEV Score7,’ Sev = 3 (serious, life-threatening)
*(Champion HR, Sacco WJ: Personal communication, August 1986) Abbreviations: TS, trauma score; GCS, TSlGlasgow Coma Scale; MOI, mechanism of injury; SEV, paramedic severity impression; CRAMS, CRAMS scale; PHI, prehospital in- dex; RSM, respiratory/systolic blood pressure/motor response score; RPM, respiratory/ pulse/motor response score; RSG. respiratory/systolic pressure/GCS score; and Kane’s revised checklist
ratio of posttest to pretest odds for need- ing trauma center triage given a negative triage instrument result. A good instru- ment has both a large LR+ and a small LR - . An LR of 1 implies that the test (triage instrument) provides no additional information. Note that for a triage instru- ment with a single cut-off, LR+ =sen- sitivity/( l-specificity), and LR - = (l-sen- sitivity)/specificity. Confidence intervals (95% CI) were calculated using standard formulas.lR
Results
During 1982 the Thurston County para- medic units evaluated 141 trauma pa- tients. One of these patients was a major thermal and electrical burn and was ex- cluded from further analysis. Sufficient data for 130 of the remaining patients were available to evaluate desirability of transfer to a trauma center. There were four patients who had no vital signs in the prehospital setting, and five others who died in the emergency department. Five additional patients died in the hospital.
Of the 130 patients reported in this pa- per, the mean age was 33.1 (f 18.3 SD)
years with a range from 2 to 87 years. There were 13 penetrating wounds or lac-
erations, with the remainder of patients sustaining blunt trauma.
On the basis of the criteria of this study, 41 (31% patients were considered desirable for trauma center triage (Group I). These patients had a mean age of 32.5 (f 17.7 SD) years with a range of 2 to 76 years. The mean initial trauma score for Group I patients was 11 .O ( f 5.0 SD). Six- teen patients went to the OR for other than orthopedic extremity injuries, 16 pa- tients went to the ICU, 5 patients died in the emergency department, and 4 patients presented without vital signs and could not be resuscitated. Subsequent analysis revealed that all five in-hospital deaths (ie, death after disposition from the emergen- cy department) occurred in the Group I patients.
There were 89 (69%) patients not desig- nated for trauma center triage (Group II). These patients had a mean age of 33.5 (f 18.1 SD) years with a range of 2 to 87 years. The initial mean trauma score for Group II patients was 15.2 (f 1.2 SD).
Emergency department disposition of the Group II patients was as follows: 47 were admitted to a regular hospital bed, 30 were released home, 9 went to the OR with or- thopedic extremity injuries, and 3 were transferred for admission to a regular bed
Prehospital Trauma Triage Instruments 201
at another hospital. No deaths were iden- tified in the Group II patients.
Sensitivity and specificity for trauma center triage for the triage instruments are shown in Table 2. Five triage instruments had sensitivities of more than 70% (PHI, TS/GCS/MOI, RSG, CRAMS [cut-off 5 81, and Kane’s checklist). Kane’s check- list and CRAMS [ 5 81 were found to be significantly more sensitive for identifi- cation of trauma center triage than the instruments with sensitivities 5 70% (P< .013 and P< .002, respectively). With respect to specificity, the RSG and PHI tests were significantly better than the other five tests (PC .03 and Pc.05, respectively).
Likelihood ratios for the five triage in- struments with sensitivities > 70% are shown in Table 3. The Kane’s checklist and CRAMS scale [I 81 instruments when negative provide the largest improvement in odds against the need for trauma center triage. The RSG and PHI instruments when positive provide the largest increase in odds for the need for trauma center triage. More specific instruments (not shown in Table 3) such as the TS and SEV score yield LR+‘s of 13.75 and 11.40, respectively.
These latter instruments have LR-‘s of 0.56 and 0.51, respectively, which sug- gest that they perform half as good as the Kane’s checklist or CRAMS scale [ 5 81 as a screen against major trauma.
More explicit descriptions of the pa- tients with life-threatening injuries who would not have been triaged to the trauma center using the five instruments with sen- sitivities > 70% are provided below and in Table 4. All patients missed by these in- struments were hemodynamically stable during their prehospital and emergency department stays.
Of the 11 patients considered in need of trauma center triage but not identified by the PHI, all had an initial TS of > 13 and an initial GCS of 2 12. Six were admitted to the ICU with multiple trauma, three went to the OR with blunt trauma, and
Table 2. Triage Criteria Performance: Sensitivity and Specificity for Trauma Center Triage
two went to the OR with penetrating inju- ries to the head. There was one in-hospital death in this group.
Of the 11 patients considered in need of trauma center triage but not identified by the RSG, all had an initial TS of 2 14 and an initial GCS of z 13. Five were admitted to the ICU with multiple trauma, four went to the OR with penetrating injuries, and two went to the OR with stable trau- ma. There was one in-hospital death in this group.
Of the nine patients considered in need of trauma center triage but not identified by the combined TS/GCS/MOI triage in- dex, all had an initial TS of 2 13 and an initial GCS of 112. Five were admitted to the ICU with multiple trauma, three went to the OR with blunt trauma, and one went to the OR with a brachial artery lac- eration. There were two in-hospital deaths in this group.
Of the six patients considered in need of trauma center triage but not identified by a CRAMS score 58, all had an initial TS of 2 15 and an initial GCS of 2 12. Three were admitted to the ICU with mul- tiple trauma, two went to the OR with blunt trauma, and one went to the OR with a penetrating injury. There was one in-hospital death in this group.
Of the six patients considered in need of trauma center triage but not identified
202 J. R. Hedges. S. Feero, B. Moore, D. W. Haver, B. Shultz
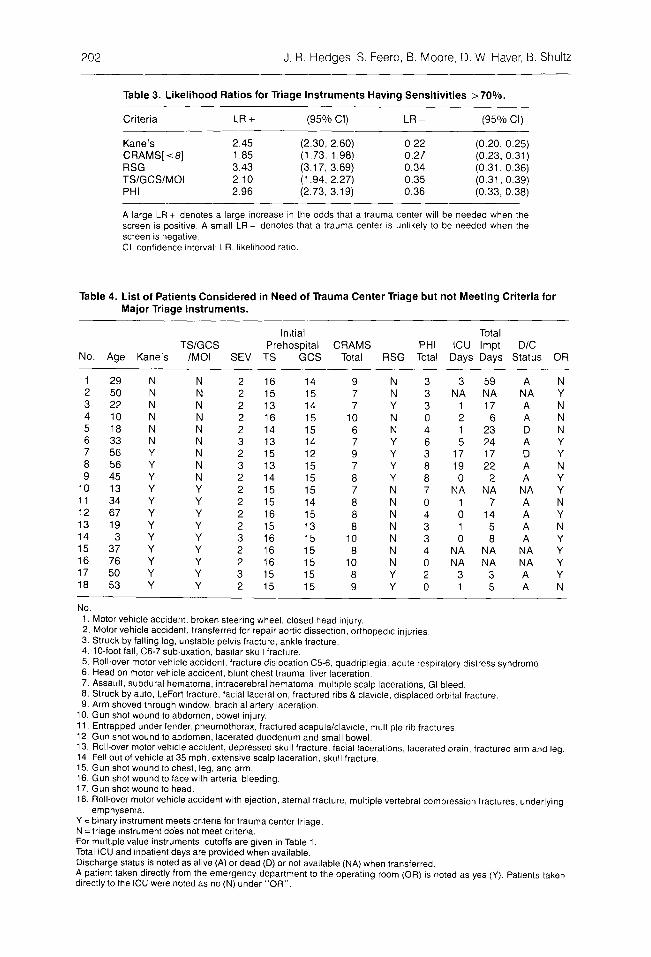
Table 3. Likelihood Ratios for Triage Instruments Having Sensitivities >70%.
A large LR + denotes a large Increase in the odds that a trauma center will be needed when the screen IS positive. A small LR - denotes that a trauma center IS unlikely to be needed when the screen IS negative Cl, confidence interval; LR, llkellhood ratio.
Table 4. List of Patients Considered in Need of Trauma Center Triage but not Meeting Criteria for Major Triage Instruments.
Initial Total TSIGCS Prehospital CRAMS PHI ICU lmpt WC
NO. Age Kane’s /MO1 SEV TS GCS Total RSG Total Days Days Status OR
1 29 N N 2 16 2 50 N N 2 15 3 22 N N 2 13 4 10 N N 2 16 5 18 N N 2 14 6 33 N N 3 13 7 56 Y N 2 15 8 56 Y N 3 13 9 45 Y N 2 14
IO 13 Y Y 2 15 11 34 Y Y 2 15 12 67 Y Y 2 16 13 19 Y Y 2 15 14 3 Y Y 3 16 15 37 Y Y 2 16 16 76 Y Y 2 16 17 50 Y Y 3 15 18 53 Y Y 2 15
14 9 N 3 3 59 A N 15 7 N 3 NA NA NA Y 14 7 Y 3 1 17 A N 15 10 N 0 2 6 A N 15 6 N 4 1 23 D N 14 7 Y 6 5 24 A Y 12 9 Y 3 17 17 D Y 15 7 Y 8 19 22 A N 15 a Y 8 0 2 A Y 15 7 N 7 NA NA NA Y 14 0 N 0 1 7 A N 15 a N 4 0 14 A Y 13 a N 3 1 5 A N 15 IO N 3 0 8 A Y 15 8 N 4 NA NA NA Y 15 10 N 0 NA NA NA Y 15 8 Y 2 3 3 A Y 15 9 Y 0 1 5 A N
No. 1. Motor vehicle accident, broken steering wheel, closed head injury. 2. Motor vehicle accident. transferred for repair aortic dIssectIon. orthopedic injuries, 3. Struck by falling log, unstable pelvis fracture. ankle fracture. 4. lo-foot fall, C6-7 subluxation, basilar skull fracture. 5. Roll-over motor vehicle accident, fracture dislocation B-6, quadnplegla. acute respiratory distress syndrome. 6. Head on motor vehicle accident, blunt chest trauma, liver laceratlon. 7. Assault, subdural hematoma, intracerebral hematoma, multiple scalp lacerations. GI bleed. 8. Struck by auto, LeFort fracture. facial laceration, fractured ribs & clavicle, displaced orbital fracture. 9. Arm shoved through window, brachlal artery laceration.
10. Gun shot wound to abdomen, bowel injury. Il. Entrapped under fender, pneumothorax, fractured scapula/clavicle, multiple rib fractures. 12. Gun shot wound lo abdomen, lacerated duodenum and small bowel. 13. Roll-over motor vehicle accident, depressed skull fracture, facial lacerattons, lacerated brain, fractured arm and leg. 14 Fell out of vehicle at 35 mph, extensive scalp laceration, skull fracture. 15. Gun shot wound to chest, leg, and arm. 16. Gun shot wound lo face with artenal bleeding. 17. Gun shot wound to head. 18. Roll-over motor vehicle accident with ejection, sternal fracture, multiple vertebral compression fractures, underlymg
emphysema. Y = bmary instrument meets criteria for trauma center triage. N = triage instrument do% not meet criteria. For multlple value instruments, cutoffs are given in Table 1. Total ICU and Inpatient days are provided when available. Discharge status is noted as alive (A) or dead (D) or not available (NA) when transferred. A patlent taken directly from the emergency department to the operatmg room (OR) is noted as yes (Y). Patients taken directly to the ICU were noted as no (N) under “OR”.
Prehospltal Trauma Triage Instruments 203
by Kane’s “revised” triage checklist, all had an initial TS of 2 13 and an initial GCS of 2 14. Four were admitted to the ICU with multiple trauma and two went to the OR with blunt trauma. There was one in-hospital death in this group.
Discussion
We have evaluated commonly recom- mended prehospital triage instruments in a semirural trauma population. Criteria used to denote desirability of transfer to a trauma center were similar to that used in other studies with the exception of exclu- sion of the injury severity scores. Al- though the data set are small, the trauma population was preselected by the EMS system and contains a high proportion of serious injuries. A number of conclusions can be made.
First, five of the triage instruments stand out with respect to their ability to identify patients in need of trauma cen- ter triage. Patients “missed” by these instruments (PHI, TS/GCS/MOI, RSG, CRAMS [I 81, and Kane’s checklist) pre- sented in a hemodynamically stable condi- tion and often were admitted to the ICU for observation. Four patients with pene- trating injuries were missed by the RSG. Performance of this score could be im- proved by including penetrating injuries of the head, neck, or torso as a screening item. Consideration for adding penetrat- ing wounds of the head and neck to the PHI and CRAMS scale should also be made. The inclusion of this mechanism of injury criterion may be necessary when paramedic response times are rapid and initial physiologic compromise minimal.
Second, of the five triage instruments showing the greatest sensitivity for pa- tients in need of trauma center triage, the RSG and PHI scores were significantly more specific. Of the five scores, the CRAMS scale [ 5 81 showed the worst spe- cificity. Using the CRAMS scale, nearly half the patients who did not require a
trauma center would have been triaged to a trauma center. With respect to overall performance (high LR + , low LR -- , the Kane’s checklist appears promising. How- ever the Kane’s checklist does not permit physiologic characterization of the trauma patient population for subsequent analy- sis of prehospital care impact upon trau- ma management.:
Third, although the paramedic’s gestalt impression of injury severity (SEV) was specific for the need for trauma center re- ferral, the SEV score was not sensitive. The SEV score correlated strongly with the TS/GCS screen, indicating that para- medics in this EMS system primarily gauge life-threat potential upon physio- logic parameters.
Fourth, the constellation of (MOI) cri- teria of this study when used in isolation of physiologic criteria represents an insen- sitive instrument for predicting need for a trauma center. Penetrating trauma to the head, neck, or torso, however, was found to be a useful indicator in this small data set.
Our results complement other studies. Although Kane et al’ used a slightly differ- ent “gold standard” to determine need for triage to a trauma center, they also found the TS to have poor sensitivity whereas the Kane’s revised checklist and CRAMS scale [ C= 81 had reasonable sensitivity (81% and 72%, respectively) and specificity (77% and 86%, respectively). They note that a perfect instrument may be impossible to develop.
Similar to our finding that physiologic scores were specific for trauma center triage need, Sharff et alh found that a pre- hospital TS 5 12 correlated with early deaths. They also found that MO1 criteria similar to ours when used in isolation were not specific for trauma center need.
Long et al” used an ISS 2 16 to deter- mine need for trauma center triage. In agreement with our results for a TS 5 12, they obtained a sensitivity of 49% and specificity of 84%. They report an im- provement in the sensitivity of MO1 crite-
204 J. R. Hedges, S. Feero, B. Moore, D. W. Haver, B Shultz
ria by the addition of physiologic (TS) in- formation. They did not report the ability of MO1 to improve the performance of the TS.
Using criteria similar to ours for evalu- ating CRAMS [ 161 scale trauma center triage, Clemmer, et alI0 report a sensitivity of 29% and a specificity of 99%. For a cutoff of 56, we found a sensitivity of 39% and a specificity of 89%.
Koehler, et all? prospectively found the PHI to be an excellent predictor of mor- tality and the need for emergency general or neurosurgical operative intervention. They found the PHI to be 85% sensitive and 94% specific for the need for emer- gency general or neurosurgical operative intervention. In our study, the PHI missed five of 16 patients who went to the OR for emergency surgery for other than man- agement of orthopedic extremity injuries. For our data, this OR “gold standard,” which is similar to that of Koehler, et al, yields a sensitivity of 69% for prediction of need for emergency OR care by the PHI. The sensitivity reported by Koehler, et al is within the 95% confidence interval (CI) of our estimate (.41, .89; 95% CI).r:
Our results are slightly at variance with those of Ornato, et al,” who found both the CRAMS [I 81 scale and TS to be infe- rior to their paramedics’ gestalt impres- sion of severity in determining death or need for urgent surgery. This difference can be, in part, explained by the differ- ence in “gold standard” used by Ornato, et al. In their study there was no separation of the indication for or type of surgery and hence we do know how many of the patients taken to the OR in their study would have been equally well managed at a hospital not designated as a trauma cen- ter. Although we used a similar scale for gestalt paramedic impression of injury se- verity (SEV), our paramedics’ SEV score closely paralleled the TS and was nor su- perior in sensitivity to other triage instru- ments.
Thus, in a community with several po- tential receiving hospitals, use of the
Kane’s checklist, the RSG, or the PHI should facilitate prehospital triage of trau- ma victims to the facility designated by the EMS system for receiving major trau- ma. Patients not meeting criteria for ma- jor trauma could otherwise be taken to the closest hospital.
Conclusions
In this study the criteria of absence of vi- tal signs in the prehospital setting, death in the emergency department, need for ur- gent operation for other than orthopedic extremity injury, and admission to the ICU designated the desirability of trauma center triage. No prehospital triage instru- ment was a perfect discriminator of the need for trauma center triage. Kane’s “re- vised” checklist, RSG, and the PHI were found to be the most promising instru- ments. These instruments appear to be compatible with rapid application and minimize subjectivity in their application. They combine good sensitivity with ac- ceptable specificity.
Patients missed by the Kane’s checklist, RSG, or PHI were hemodynamically sta- ble and should be safely transferable from a nontrauma-center receiving hospital up- on emergency department determination of significant underlying injury. Provided that individual component scores are re- corded, the RSG and PHI triage instru- ments should also provide objective means of physiologically characterizing the prehospital trauma patient population to permit subsequent evaluation of the in- fluence of prehospital care upon trauma managements.
Finally, in EMS systems with rapid re- sponse times, the RSG score may be im- proved by addition of a penetrating wound mechanism of injury criterion. Fu- ture studies should address the interobser- ver variability, the stability with time. the applicability to different trauma popula- tions, and the average time needed to score these indicies.
Prehospltal Trauma Triage Instruments 205
REFERENCES
1. Champion HR, Sacco WJ, Carnazzo AJ, et al: Trauma Score, Crit Care A4ed 1981; 9:672- 676.
trauma victims. A/?n Emerg Med 1982; 1 I : I32- 135.
2. Moreau M, Gainer PS, Champion HR, et al: Application of the trauma score in the pre- hospital setting. Ann Emerg Med 1985; 14:1049- 1054.
10. Clemmer TP, Orme JF, Thomas F, et al: Pro- spective evaluation of the CRAMS scale for triaging major trauma. J Trauma 1985; 25: I XX- 191.
3. Conference on Injury Severity Scoring and Triage. Sponsored by the U.S. Army Medical Re- search & Development Command. Contract to DAMD 17-83-G-9256 and the American Trauma Society. Washington DC, September 1983.
3. Long WB, Bachulis BL, Hynes GD: Accuracy and relationship of mechanisms of injury, trau- ma score, and injury severity score in identifying major trauma. Am JSurg 1986; 151:581-584.
5. Kane K, Engelhardt R, Celentrano .I, et al: Em- pirical development and evaluation of prehospi- tal trauma triage instruments. J Truuma 1985; 25:482-488.
II. Koehler JJ, Baer LJ, Malafa SA, et al: Prehoapt- tal index: A scoring system for field triage tract- ma victims. Ann Emerg Med 1986; 15:178-182.
12. Koehler JJ, Malafa SA, Hillesland J, et al: Pre- hospital index: A multicenter trial. ,4nn Enrerq Med 1986; 15:625-626.
13. Champion HR, Sacco WJ, Copes W: Simphfica- tion of the trauma score. J Traumu 1985; 25:680.
14. Sacco WJ, Champion HR, Henderson JV: lm plementation of severity scores in navjal casualty care. Proceedings of the 17th Annual Hawaii In- ternational Conference on System Science\. 1984, pp 292-302.
6. Sharff J, Neely K, Derr P: The ability of triage criteria to predict jnjury severity in a county- wide trauma system. Ann Emerg Med 1986; 15:626.
7. Hedges JR, Sacco WJ, Champion HR: An anal- ysis of prehospital care of blunt trauma. J Truu- tnu 1982; 22:989-993.
15. Baker SP, O’Neill B, Haddon W Jr, et al: ‘The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974; 14:187.
16. Radack K, Rouan G, Hedges JR: The likelihood ratio: an improved measure for reporting and in terpreting diagnostic test results. Arch Pa/h Ltrb Med 1986; 110:689-693.
8. Ornato J, Mlinek EJ Jr, Craren EJ, et al: Ineffec- 17. Colton T Sfafisrics in Medicine. Boston, Littlc tiveness of the trauma score and the CRAMS Brown & Co, 1974, pp 169-174. scale for accurately triaging patients to trauma 18. Miettinen OS: Estimability and estimation in centers. Ann EmergMed 1985; 14:1061-1064. case-referent studies. Am J Eprderniol 1’976;
Y. Gormican SP: CRAMS Scale: Field triage of 103:226-235.
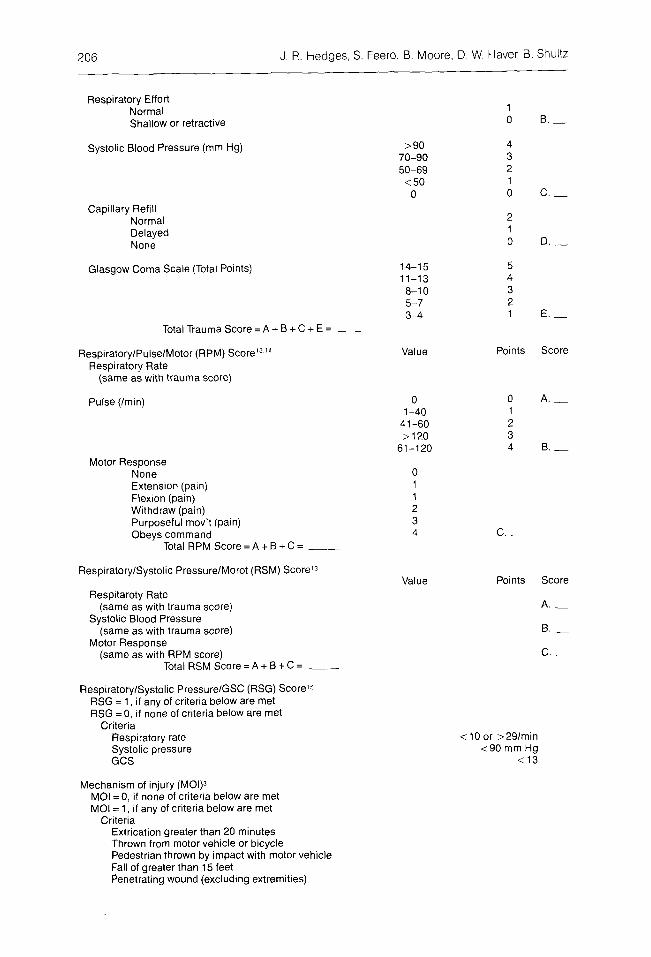
Mechanism of injury (MOl)3 MOI = 0, if none of criteria below are met MOI = 1, if any of criteria below are met
Criteria Extrication greater than 20 minutes Thrown from motor vehicle or bicycle Pedestrian thrown by impact with motor vehicle Fall of greater than 15 feet Penetrating wound (excluding extremities)
0 1
2 3 4
1 0 B. _
c. -
c. -
Prehospltal Trauma Triage Instruments 207
Severity Estimated by Paramedic (SEV)’ (Paramedics Gestalt impression of severity) Not serious Potential Life-Threatening Serious, Life-Threatening
2 3
Prehospital Index (PHI)” Systolic Pressure (mmHg)
Value >lOO
86-100 75-85 o-74
Pomts 0 1 2 5
3 0 5
Score
Pulse (bpm) 2120 51-119
<51
Respirations Normal Labored/Shallow < lO/min; lntubation
Consciousness Normal Confused/Combative Unintelligible
Penetrating chest/abdominal wound No Yes
Total PHI Score=A+B+C+D+E= __
CRAMS Scale Crrculation
Value Normal capillary refill
and BP 2 100 mm Hg Delayed capillary refill
or85 sBP<lOOmm Hg No capillary refill
orBP <85mmHg
Respirations Normal Labored or shallow cr > 351 min Absent
Abdomen/Thorax Nontender Tender Rigid abdomen or flail chest
or penetrating injury
Motor Normal Responds only to pain
(not decerebrate) No response (decerebrate)
Speech Normal Confused Unintelligible
Total CRAMS Scale Score = A + B + C + D + E = __
Kane’s Revised Triage Checklist (KANES)s KANES = 0, if none of the criteria below are present KANES = 1, If any of the criteria below are present
J R. Hedges. S Feero, 6. Moore. D. W. Haver, 8 Shultz
Penetrating abdominal injury Blunt thoracic trauma with systolic pressure <90 mm Hg Pedestrian struck by motor vehicle with abdominal injury Flail chest Motorcyclist with blunt abdominal injury Fall greater than 15 feet Age less than 5 or greater than 65 years