34
COMPASS-CP: An interoperable SMART on FHIR application to generate care plans Umit Topaloglu, PhD Mysha Sissine, MSPH September 2019

COMPASS-CP: An interoperableSMART on FHIR application
to generate care plans
Umit Topaloglu, PhD
Mysha Sissine, MSPH
September 2019
Outline
1. Why we need care planning?2. Design and Implementation3. COMPASS-CP evaluation and what we have
learned so far 4. SMART on FHIR as integration framework5. Demonstration 6. Sustainability and Future Direction

Health Care is Complex
Patients and
Caregivers
Therapists (PT, OT, SLP)
HospitalSystem
Primary Care
Home Health
Community

There is Growing Demand
• Demand has been escalating– Center for Medicaid and Medicare (CMS)
• Reimbursements and policies• Quality metrics
– NC Medicaid Managed Care & Pilots
• There is a need for tools to support comprehensive, timely, and quality care

What is COMPASS-CP?• “Comprehensive Post-Acute Stroke Services – Care Plan”
– Patient-centered digital application used at the point of care– Collect patient report outcomes (PRO) – Assess functional and social determinants – Patient and caregiver-reported assessments– Algorithms to create an individualized and “actionable” care plan– Includes a directory of community-based resources
• Goals– Improve patient outcomes– Increase patient satisfaction– Reduce unnecessary readmissions

DESIGN AND IMPLEMENTATION

7
• 9,000 patients• 40 hospitals and
communities
How was COMPASS-CP Developed?• Pragmatic Trial in NC• Diverse health systems• Patients discharged home after stroke, clinical
workflow, and CMS billing
COMPASS Hospitals1. Alleghany Memorial Hospital
2. Angel Medical Center
3. Ashe Memorial Hospital
4. Atrium Health Cabarrus
5. Atrium Health Carolinas Medical Center
6. Atrium Health Cleveland
7. Atrium Health Kings Mountain
8. Atrium Lincoln
9. Atrium Health Mercy
10. Atrium Stanly
11. Atrium Health Union
12. Atrium Health University City
13. Betsy Johnson Hospital
14. Blue Ridge Regional
15. Caldwell UNC Health Care
16. Carolinas HealthCare System Blue Ridge
17. Cape Fear Valley Medical Center
18. Carteret Health Care
19. Central Harnett Hospital
20. Duke Raleigh Hospital
21. FirstHealth Moore Regional
22. Frye Regional Medical Center
23. Hugh Chatham Memorial Hospital
24. Margaret R. Pardee Memorial Hospital
25. Mission Hospital
26. New Hanover Regional Medical Center
27. Northern Hospital of Surry County
28. Novant Health Huntersville Medical Center
29. Novant Health Matthews Medical Center
30. Novant Health Presbyterian Medical Center
31. Onslow Memorial Hospital
32. Rex Healthcare
33. SouthEastern Regional Medical Center
34. UNC Lenoir Health Care
35. UNC Hospital
36. UNC Rockingham Health Care
37. Vidant Duplin Hospital
38. Vidant Edgecombe Hospital
39. WakeMed Health & Hospitals
40. Wake Forest Baptist Health
41. Wake Forest Baptist Health Lexington Medical Center
42. Wake Forest Baptist Health Wilkes Medical Center
43. Washington County Hospital
COMPASS Study AimsPrimary aim • Determine the comparative effectiveness of COMprehensive
Post-Acute Stroke Service model vs usual care on stroke survivor functional status at 90 days post-stroke
Secondary aims • Assess caregiver strain at 90 days• All-cause readmissions at 30 and 90 days• Mortality, health care utilization, use of TCM billing codes
using claims data at 1 year

COMPASS Care Model
.
2 Day Call 7-14 Day Clinic Visit 30 Day Call 60 Day Call
Care Team– Advanced Practice Provider or Physician – Post-Acute Care Coordinator (Nurse)
Intervention Highlights– Patient-centered education handouts– Training modules for clinicians – Digital tool (beta-COMPASS-CP) to assess
functional and social determinants of self-management and health
– Individualized care plans – Directory of community-based resources

COMPASS Clinical Workflow

COMPASS-CP EVALUATION AND WHAT WE HAVE LEARNED SO FAR
3

What we have learned: Patients
less than half of patients could list the major risk factors for
stroke
36% did not recognize blood pressure as a
stroke risk factor
19% of patients were nonadherent with
prescribed medications

What we have learned: Clinician-users
“Makes my job easier”

“Helps identify factors impacting the patient’s
recovery that they may have otherwise missed”
What we have learned: Clinician-users

Sustainability
• The team has been working to make the solution sustainable after the completion of the COMPASS Study.
• Received funding from: Wake Forest Catalyst Innovation fund to develop the FHIR version

SMART ON FHIR AS INTEGRATION FRAMEWORK

Challenges of Multiple System/Manual Data Entry
• Erroneous and missing data (up to 56% data
unusable+)
• Resource demanding process and correspondingly,
delays.
• No single source of truth,
• Data Provenance/Reusability issues
• Compliance/Privacy related issues
18 + Frey et al

Potential Solutions
• Technology focus– Open architectures and APIs (REST, JSON LD)– Semantic Interoperability (ontologies, RDF representations)– Standards (UMLS, CDISC, HL7)
• Data Governance and MDM
• Data Provenance
• User friendly systems
19

Standards and Technologies
• Continuity of Care Document (CCD) and HL7 Clinical Document Architecture (CDA)– Header, Allergies, Problems, Procedures, Family
history, Social history, Payers, Advance directives, Medications, Immunizations, Medical equipment, Vital signs, Functional stats, Results, Encounters, Plan of care
• Integrating the Healthcare Enterprise (IHE) – Retrieve Process for Execution (RPE), Clinical Research
Process Content (CRPC), Resource Form Description (RFD)
• CDISC Operational Data Model (ODM) v2
20

HL7- Fast Healthcare Interoperability Resources (FHIR)
Fast and Easy to implement, Evolved from HL7 Version 2 and CDA, Strong foundation in Web standards– XML, JSON, HTTP, Oauth, Support for RESTful architectures, messages or documents A Human-readable wire format for ease of use by developers Solid ontology-based analysis with a rigorous formal mapping for
correctness SMART on FHIR: Structured data with FHIR, Oauth2
authorization/permission, OpenID for SSO, HTML5 for app
21

FHIR Resources;
22

Resource Content- medication
23

Resource Content- Definitions
24

FHIR Sandbox- open.epic.com
25

FHIR’s Outlook
• FDA and NIH are very interested;– Issued several RFAs
• Growing community; paradigm shift• 21st Century Cures Act and Real World
Evidence
26
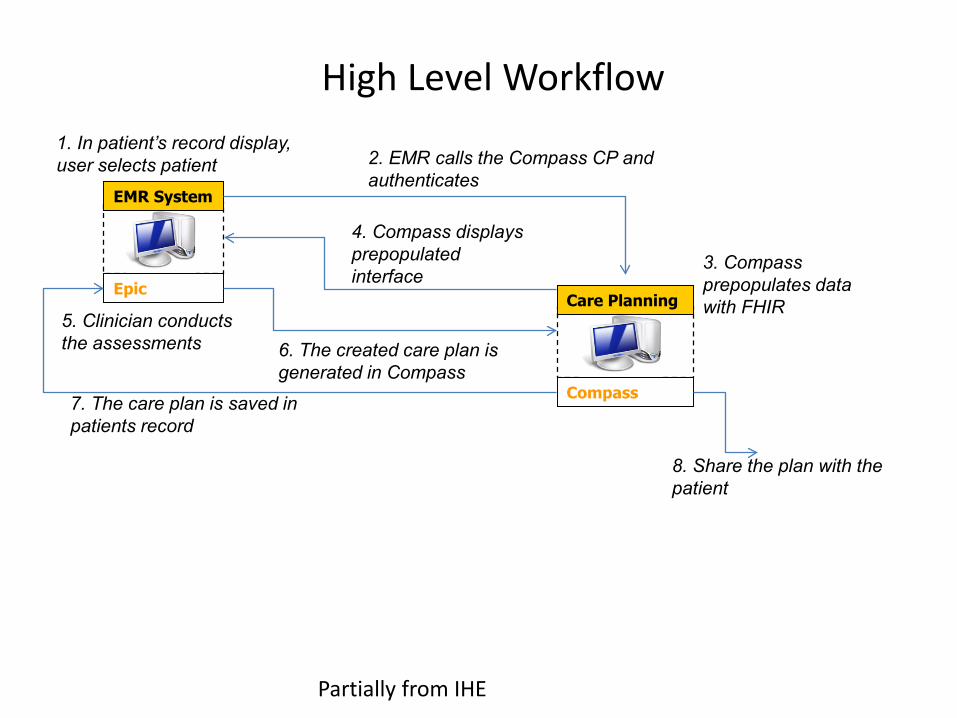
Epic
EMR System
1. In patient’s record display, user selects patient 2. EMR calls the Compass CP and
authenticates
Compass
Care Planning
3. Compass prepopulates data with FHIR
4. Compass displays prepopulated interface
5. Clinician conducts the assessments 6. The created care plan is
generated in Compass
7. The care plan is saved in patients record
8. Share the plan with the patient
High Level Workflow
Partially from IHE
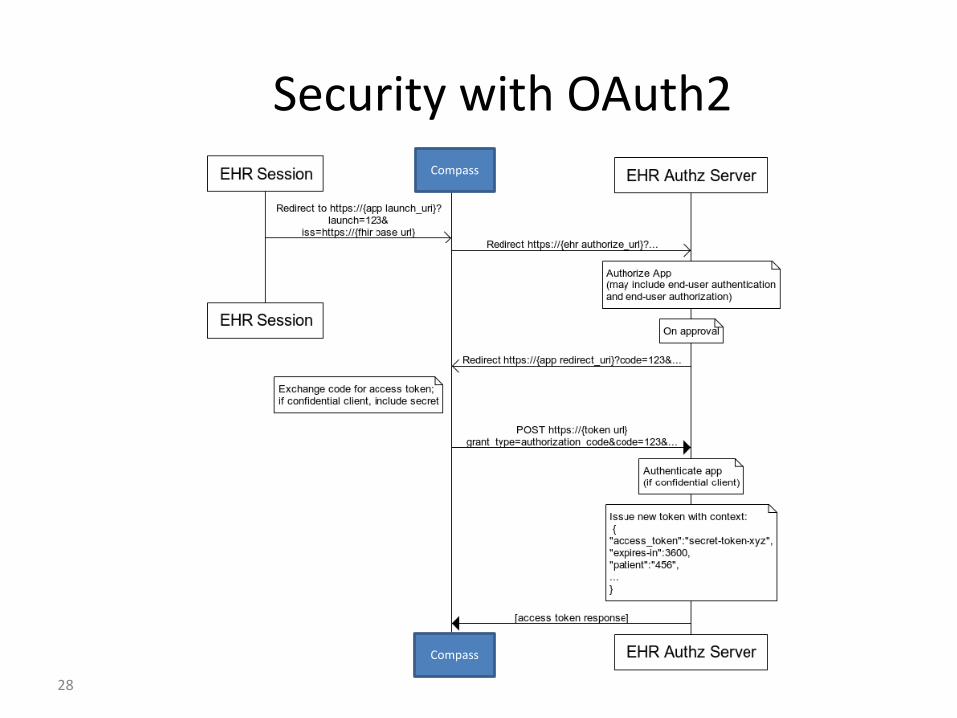
Security with OAuth2
28
Compass
Compass


DEMONSTRATION

SUSTAINABILITY AND FUTURE DIRECTION

COMPASS-CP Today
• Integrated into Wake Forest Baptist Medical Center’s EHR, Epic– Stroke and Cardiology
• COMPASS-CP is contributing to sustainable care planning for post-acute stroke patients by improving the care of patients and the efficiency of clinicians for enhanced patient engagement.
Wake Forest Innovations
Cancer
Discharge Diagnosis
Readmission Risk Scoring
Frailty & Falls
Integration with other electronic medical records, wearables, and applications
Future Enchantments

Questions?
To request a Demo of COMPASS-CP please contact: Mysha Sissine – [email protected] Leanna Grondy – [email protected] visit our website: https://www.nccompass-study.org/compasscp/

















