Page 1
Competency 1 Fetal Alcohol Spectrum Disorders
Foundation
1 Description
2 Pretest
3 Learning Objectives
4 Historic Findings Related to Alcohol Use by Pregnant Women
5 Changes in US Perspectives on Alcohol Use During Pregnancy
6 Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
7 Effects of Alcohol on the Developing Embryo and Fetus
8 Effects of Alcohol on the Developing Brain
9 Relationship between Prenatal Alcohol Use and FetalInfant Death
10 Comparative Effects of Alcohol and Other Substances on the Developing Fetus
11 Issues Related to Professional Values and Ethics
12 Matching Activity
13 Posttest
14 References
Competency 1 Fetal Alcohol Spectrum Disorders
Foundation
Description
This competency describes historic findings related to alcohol use by pregnant women
US perspectives on drinking during pregnancy terminology related to fetal alcohol
spectrum disorders (FASD) prevalence rates of FASD and effects of alcohol on the
fetus It also discusses professional values and ethics related to the counselors role in
counseling women who have used alcohol during their pregnancies
Test Your Knowledge Questions Pretest
Pretests are designed to gauge your knowledge Click in the circle or box next to the
correct answer Circles indicate that only one correct answer is possible Boxes indicate
that more than one correct answer is possible A posttest is given at the end of the module
so that you can see what youve learned
1 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
2 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
3 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
4 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
5 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
6 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
7 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
8 The terms FASD and FAS are interchangeable
True
False
9 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
10 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
Submit
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
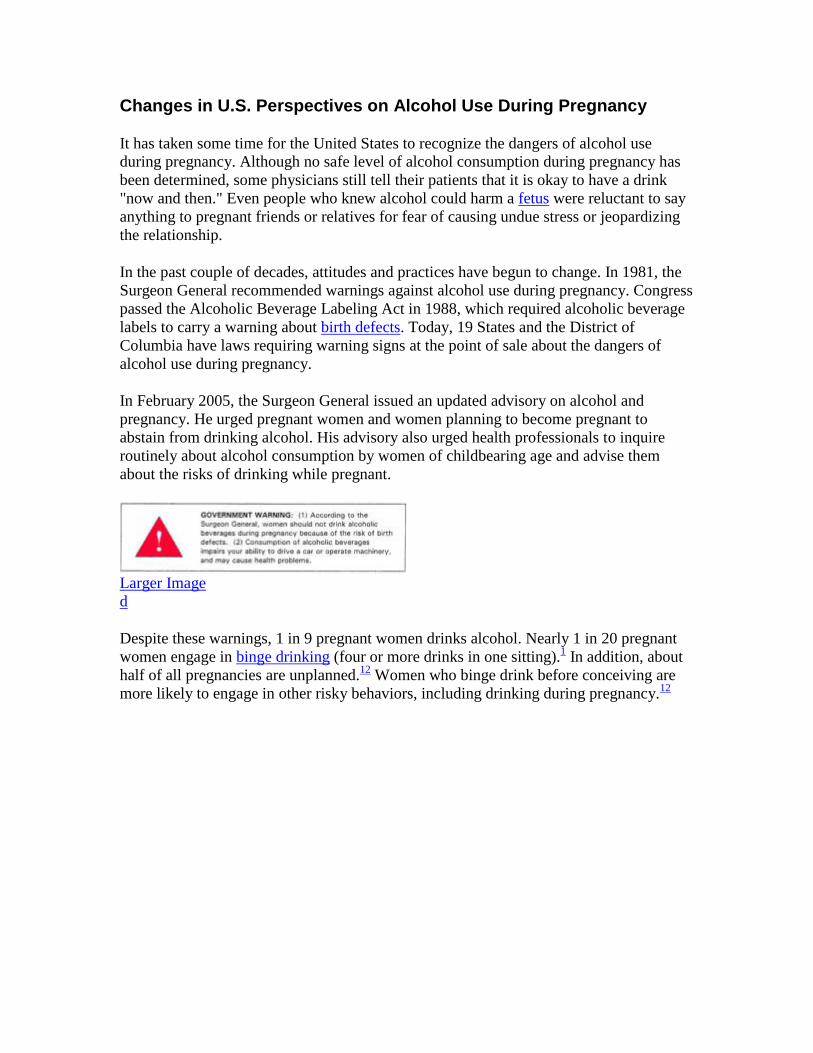
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
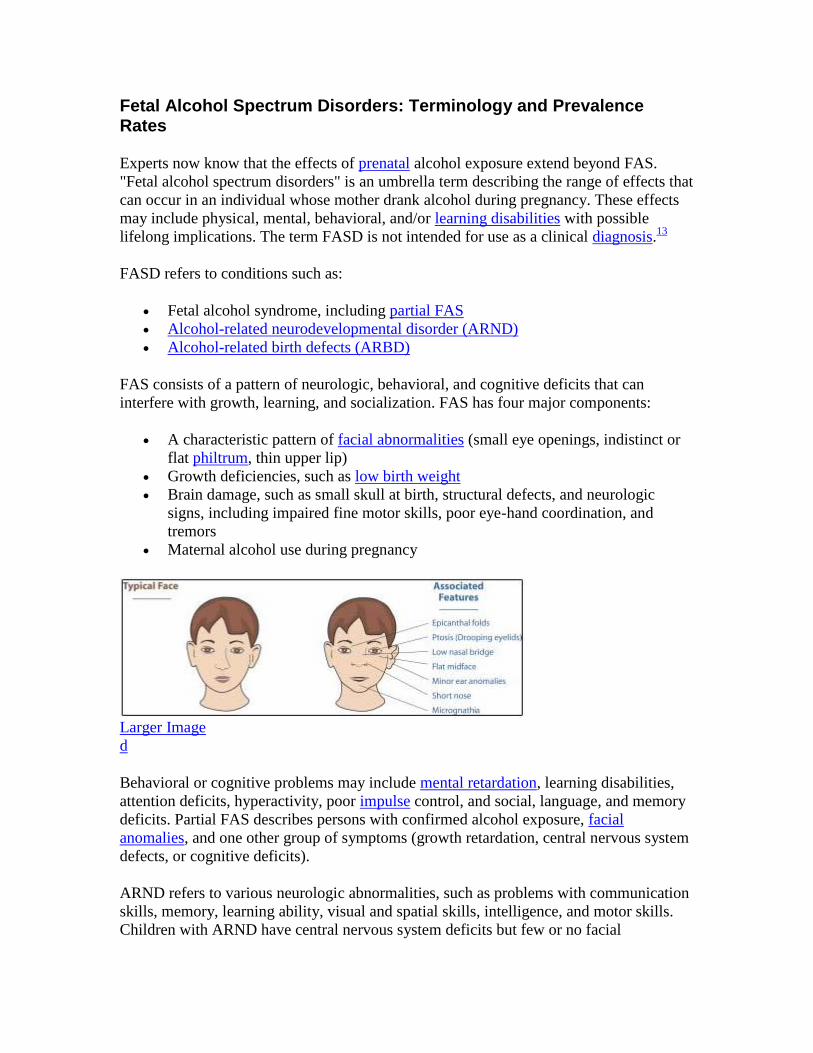
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
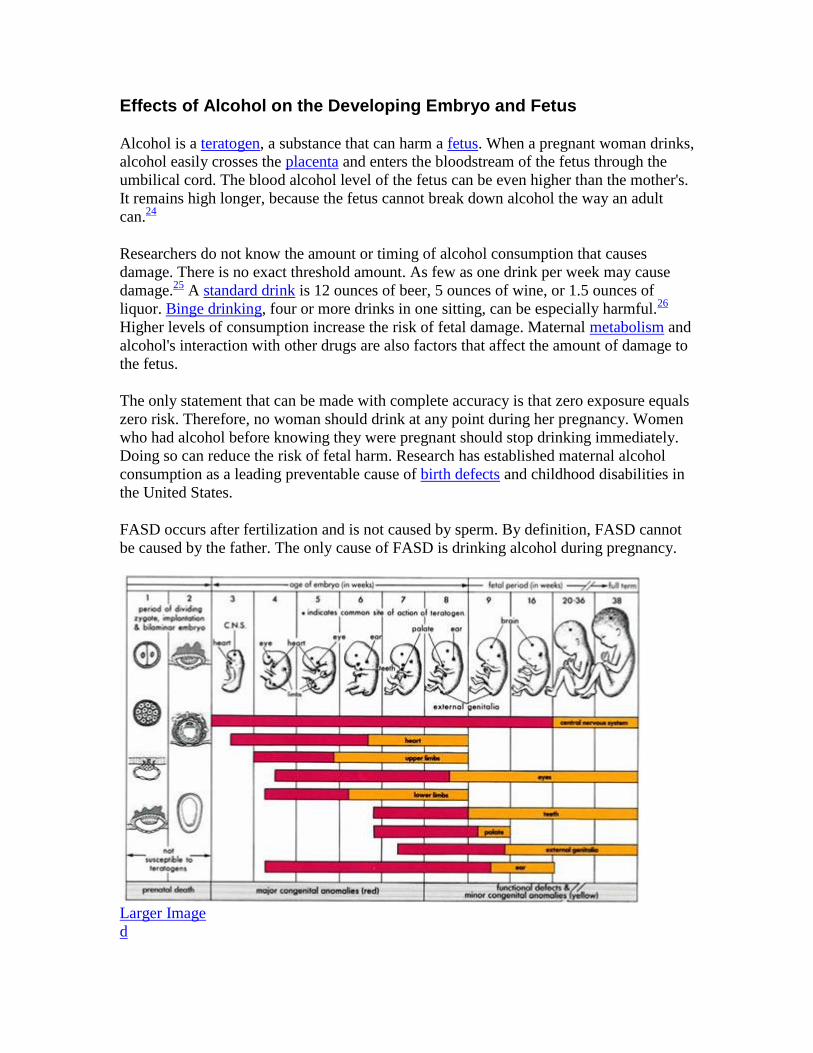
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
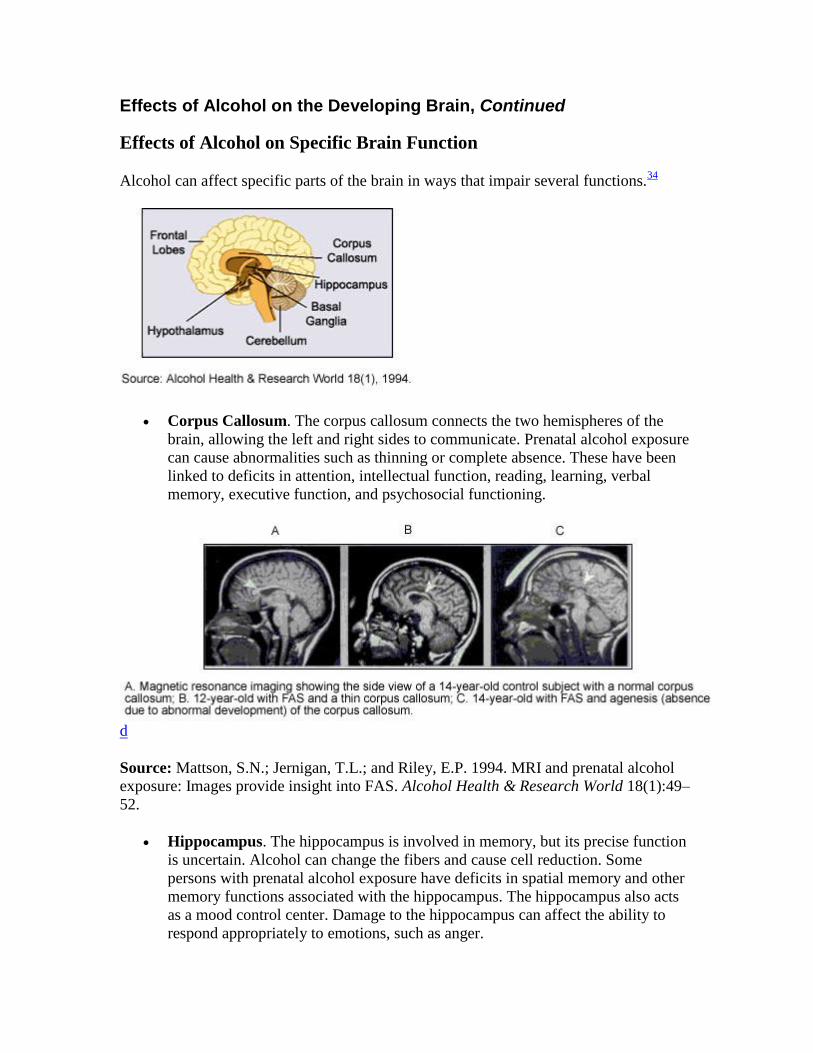
Alcohol can affect specific parts of the brain in ways that impair several functions34
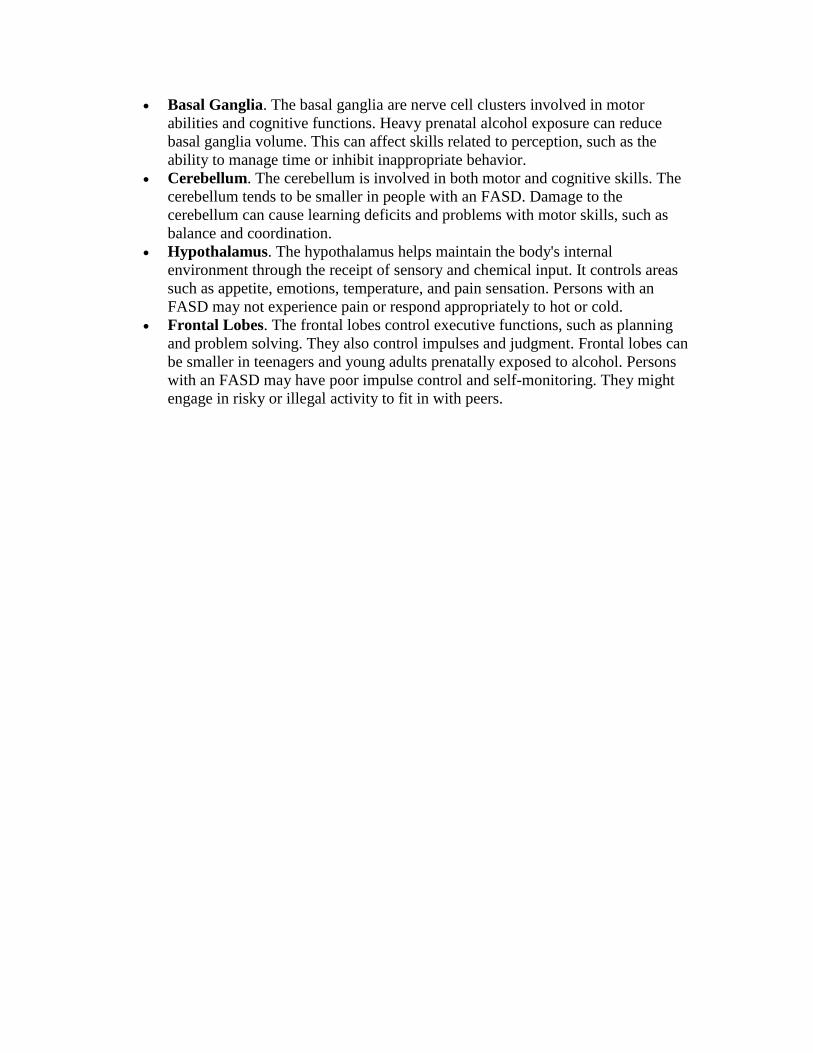
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
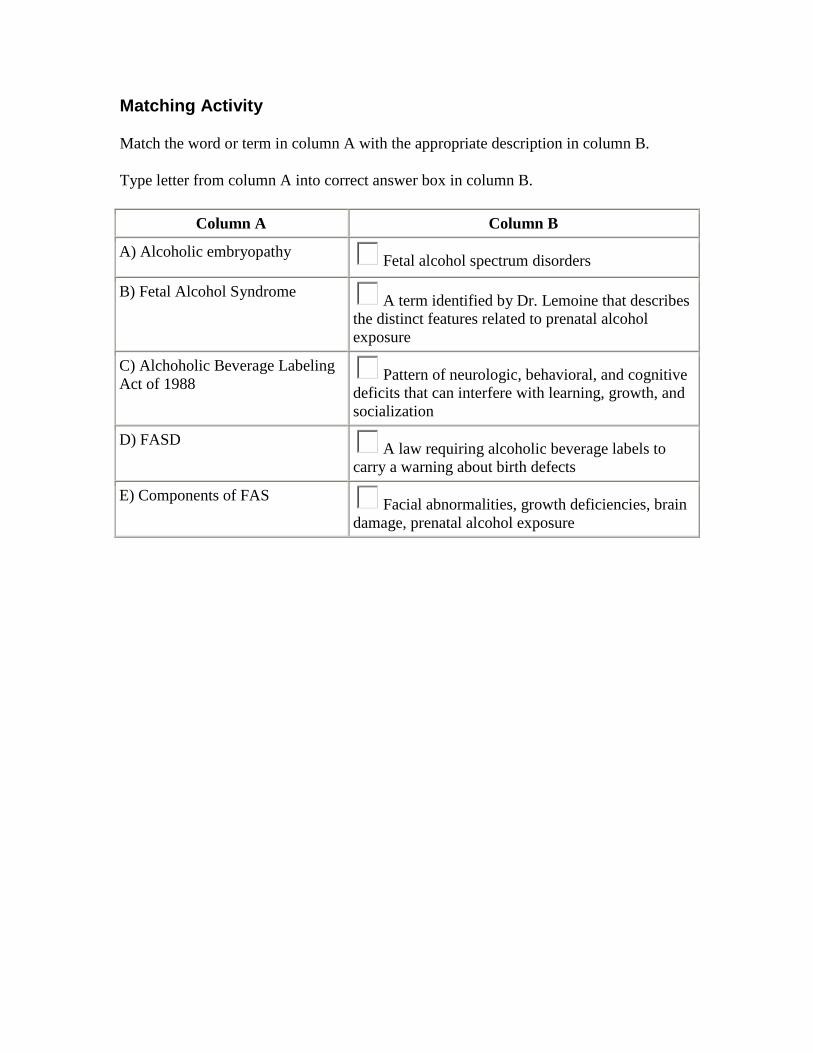
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
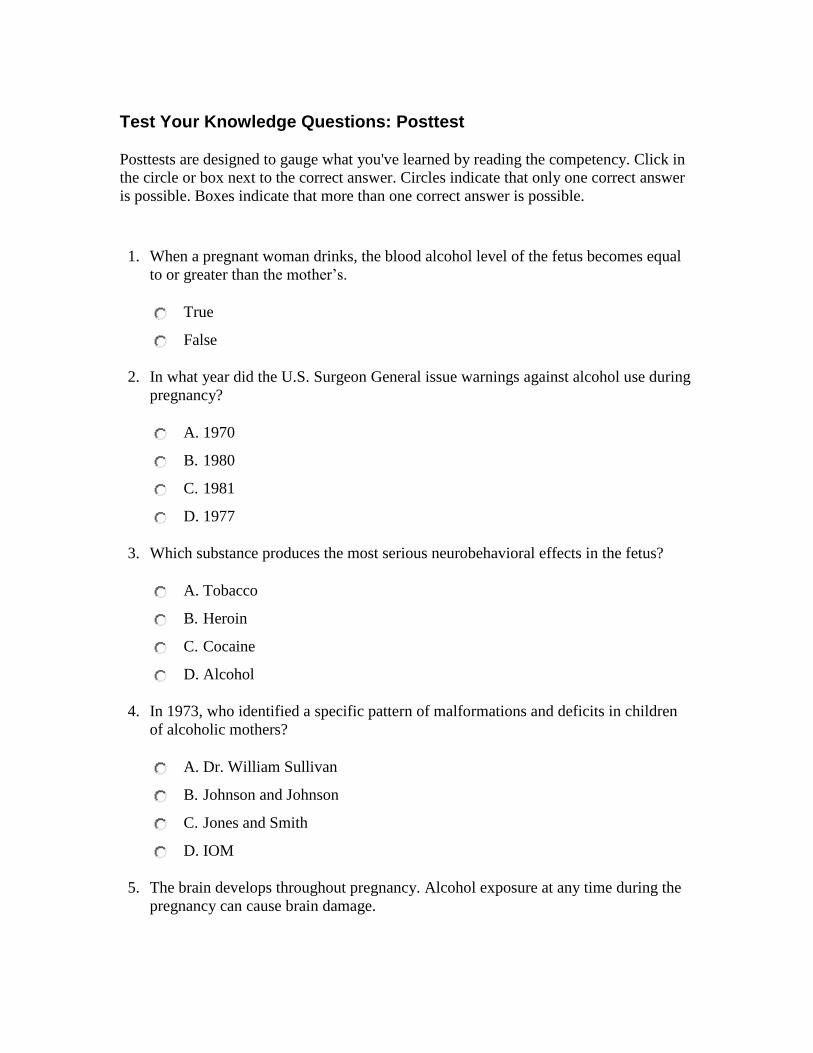
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 2
Competency 1 Fetal Alcohol Spectrum Disorders
Foundation
Description
This competency describes historic findings related to alcohol use by pregnant women
US perspectives on drinking during pregnancy terminology related to fetal alcohol
spectrum disorders (FASD) prevalence rates of FASD and effects of alcohol on the
fetus It also discusses professional values and ethics related to the counselors role in
counseling women who have used alcohol during their pregnancies
Test Your Knowledge Questions Pretest
Pretests are designed to gauge your knowledge Click in the circle or box next to the
correct answer Circles indicate that only one correct answer is possible Boxes indicate
that more than one correct answer is possible A posttest is given at the end of the module
so that you can see what youve learned
1 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
2 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
3 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
4 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
5 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
6 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
7 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
8 The terms FASD and FAS are interchangeable
True
False
9 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
10 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
Submit
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 3
Test Your Knowledge Questions Pretest
Pretests are designed to gauge your knowledge Click in the circle or box next to the
correct answer Circles indicate that only one correct answer is possible Boxes indicate
that more than one correct answer is possible A posttest is given at the end of the module
so that you can see what youve learned
1 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
2 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
3 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
4 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
5 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
6 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
7 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
8 The terms FASD and FAS are interchangeable
True
False
9 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
10 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
Submit
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 4
bifida
A Higher
B Lower
C Equal
6 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
7 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
8 The terms FASD and FAS are interchangeable
True
False
9 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
10 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
Submit
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 5
D Problems and consequences ensuing from alcohol abuse
Submit
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 6
Learning Objectives
After completing Competency 1 the learner should be able to
Understand the significance of alcohol use disorders among women
Identify areas in which alcohol use disorders in women differ from those in men
Describe the basic historic foundation of FASD
Discuss the basic terminology related to FASD and the prevalence rates
Explain the effects of maternal alcohol exposure on the developing embryo and
fetus
Compare the adverse effects of alcohol on the developing fetus to those of other
substances
Identify issues related to professional values and ethics
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 7
Historic Findings Related to Alcohol Use by Pregnant Women
Throughout history women generally have used alcohol Women now account for an
estimated one-third of Americans with alcohol abuse or alcohol dependence disorders1
Research over the last two decades shows that women respond to alcohol differently than
men do Differences are found in
Predisposing factors contributing to the development of alcohol abuse
Patterns of alcohol abuse
Context within which the alcohol abuse is initiated and maintained
Problems and consequences ensuing from alcohol abuse
Co-occurring problems and issues interacting with alcohol abuse
Based on epidemiologic factors physiologic effects and psychosocial and medical
factors women experience the damaging consequences of chronic alcohol use more
severely and rapidly than men
A major issue related to alcohol and women is alcohol use during pregnancy Drinking
during pregnancy is associated with a variety of health consequences for the woman and
her child Current estimates indicate that 5 percent of women of childbearing age are
heavy drinkers (five or more drinks on the same occasion on 5 or more days) Nearly
one-quarter of women of childbearing age engage in binge drinking (four or more drinks
on the same occasion meaning at the same time or within a couple of hours of each
other)1 Both heavy and binge drinking increase the risk of harm to a fetus
For centuries people have known that alcohol can harm a fetus In the 17th century Sir
Francis Bacon warned women against drinking alcohol while pregnant Since then
knowledge about alcohol and pregnancy has increased leading to preventive measures
such as government warnings about the dangers of alcohol use during pregnancy As far
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 8
back as the 18th century the British government recognized the impact of alcohol on
pregnancy outcomes and took steps to reverse dangerous trends
The Gin Epidemic in England in the 1700s is believed to have led to alcohol-related birth
defects When the gin tax was lifted the price went down Drinking went up and so did
infant deaths2 In 1751 the government imposed sales restrictions
In time the problem was more widely recognized In 1834 a British House of Commons
report stated that infants of alcoholic mothers often have a starved and imperfect look3
About 30 years later a French physician described children exposed to alcohol as having
small heads peculiar facial features and nervousness2
Near the end of the 19th century many researchers began to examine the effects of
alcohol on the fetus For example in 1899 Dr William Sullivan compared the pregnancy
outcomes in 120 alcoholic prisoners with 28 of their blood relatives The infant death rate
was 20 percent higher among the women with alcohol problems2 Such studies continued
into the early 20th century
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 9
Historic Findings Related to Alcohol Use by Pregnant Women Continued
Twentieth Century
For decades physicians thought that the placenta provided a protective barrier that would
prevent teratogens such as alcohol from reaching the fetus Many believed children of
alcoholics had defects related to poor genetic stock rather than alcohol exposure That
was the conclusion in a 1946 article in the Journal of the American Medical Association
French researchers began to study alcohol and pregnancy in the 1950s An unpublished
thesis reported the prenatal effects of alcohol on children born to alcoholic parents In
1968 Dr Paul Lemoine published a study of 127 children from 69 French families4
Twenty-five children had distinct features related to prenatal alcohol exposure Dr
Lemoine called this alcoholic embryopathy
A few years later Christy Ulleland a pediatric resident in Seattle became interested in
babies with failure to thrive She noticed that many had alcoholic mothers In reviewing
delivery records she found more babies that fit the pattern Her colleagues Drs David
Smith and Kenneth Jones asked to have all the children examined at one time
In 1973 Jones and Smith identified a specific pattern of malformations growth
deficiencies and central nervous system defects in 10 children of alcoholic mothers
Their study not only noted the connection between prenatal alcohol and developmental
disabilities but gave it a name fetal alcohol syndrome (FAS)5
It was originally believed that malnutrition might be responsible for these defects
However the pattern of malformation associated with FAS is not seen in children born to
malnourished women In addition alcohol has been found to be acutely toxic to the fetus
independently of the effects of malnutrition67
Similar cases were found in Germany France and Sweden8-10
As a result FAS
prevention programs were developed in the late 1970s11
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 10
Changes in US Perspectives on Alcohol Use During Pregnancy
It has taken some time for the United States to recognize the dangers of alcohol use
during pregnancy Although no safe level of alcohol consumption during pregnancy has
been determined some physicians still tell their patients that it is okay to have a drink
now and then Even people who knew alcohol could harm a fetus were reluctant to say
anything to pregnant friends or relatives for fear of causing undue stress or jeopardizing
the relationship
In the past couple of decades attitudes and practices have begun to change In 1981 the
Surgeon General recommended warnings against alcohol use during pregnancy Congress
passed the Alcoholic Beverage Labeling Act in 1988 which required alcoholic beverage
labels to carry a warning about birth defects Today 19 States and the District of
Columbia have laws requiring warning signs at the point of sale about the dangers of
alcohol use during pregnancy
In February 2005 the Surgeon General issued an updated advisory on alcohol and
pregnancy He urged pregnant women and women planning to become pregnant to
abstain from drinking alcohol His advisory also urged health professionals to inquire
routinely about alcohol consumption by women of childbearing age and advise them
about the risks of drinking while pregnant
Larger Image
d
Despite these warnings 1 in 9 pregnant women drinks alcohol Nearly 1 in 20 pregnant
women engage in binge drinking (four or more drinks in one sitting)1 In addition about
half of all pregnancies are unplanned12
Women who binge drink before conceiving are
more likely to engage in other risky behaviors including drinking during pregnancy12
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 11
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates
Experts now know that the effects of prenatal alcohol exposure extend beyond FAS
Fetal alcohol spectrum disorders is an umbrella term describing the range of effects that
can occur in an individual whose mother drank alcohol during pregnancy These effects
may include physical mental behavioral andor learning disabilities with possible
lifelong implications The term FASD is not intended for use as a clinical diagnosis13
FASD refers to conditions such as
Fetal alcohol syndrome including partial FAS
Alcohol-related neurodevelopmental disorder (ARND)
Alcohol-related birth defects (ARBD)
FAS consists of a pattern of neurologic behavioral and cognitive deficits that can
interfere with growth learning and socialization FAS has four major components
A characteristic pattern of facial abnormalities (small eye openings indistinct or
flat philtrum thin upper lip)
Growth deficiencies such as low birth weight
Brain damage such as small skull at birth structural defects and neurologic
signs including impaired fine motor skills poor eye-hand coordination and
tremors
Maternal alcohol use during pregnancy
Larger Image
d
Behavioral or cognitive problems may include mental retardation learning disabilities
attention deficits hyperactivity poor impulse control and social language and memory
deficits Partial FAS describes persons with confirmed alcohol exposure facial
anomalies and one other group of symptoms (growth retardation central nervous system
defects or cognitive deficits)
ARND refers to various neurologic abnormalities such as problems with communication
skills memory learning ability visual and spatial skills intelligence and motor skills
Children with ARND have central nervous system deficits but few or no facial
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 12
abnormalities Their problems may include sleep disturbances attention deficits poor
visual focus increased activity delayed speech and learning disabilities
ARBD describes defects in the skeletal and major organ systems Virtually every defect
has been described in some patient with FAS They may include abnormalities of the
heart eyes ears kidneys and skeleton such as holes in the heart underdeveloped
kidneys and fused bones
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 13
Fetal Alcohol Spectrum Disorders Terminology and Prevalence Rates Continued
Prevalence
Experts are unsure exactly how many individuals in the United States have an FASD
Studies by the Centers for Disease Control and Prevention have reported FAS prevalence
rates from 02 to 15 cases per 1000 births across various populations14-17
Other studies
using a variety of methods have produced estimates ranging from 05 to 20 cases per
1000 live births1819
Such rates are comparable with or above other common
developmental disabilities such as Down syndrome or spina bifida20
Some experts estimate that an FASD occurs in 10 in 1000 live births Thus of 4 million
infants born each year an estimated 40000 will be born with an FASD19
Studies of
particularly vulnerable populations yield even higher prevalence estimates For example
some Native Americans have FAS rates as high as 3 to 5 per 1000 children21-23
Because of the challenges of establishing accurate and timely prevalence information the
number of cases of fetal alcohol spectrum disorders could be greater than current data
indicate These challenges include
Lack of specific and uniformly accepted diagnostic criteria Only recently
have diagnostic guidelines been established for FAS No uniform guidelines exist
for other types of fetal alcohol spectrum disorders Thus health providers are
hampered in their efforts to screen and identify children with an FASD
FAS diagnosis based on clinical examination of features but not all children
with FAS look or act the same Because each symptom has a broad range of
possible diagnoses a clinician might miss or misdiagnose an FASD For instance
physicians are aware of the high prevalence of attention deficithyperactivity
disorders but might not link attention problems to an FASD
Lack of knowledge and misconceptions among primary care providers Many
professionals believe that an FASD can only occur if the mother is an alcoholic
poor African American or Native American Few know about the full range or
progressive nature of the neurobehavioral symptoms that result from prenatal
exposure to alcohol
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 14
Effects of Alcohol on the Developing Embryo and Fetus
Alcohol is a teratogen a substance that can harm a fetus When a pregnant woman drinks
alcohol easily crosses the placenta and enters the bloodstream of the fetus through the
umbilical cord The blood alcohol level of the fetus can be even higher than the mothers
It remains high longer because the fetus cannot break down alcohol the way an adult
can24
Researchers do not know the amount or timing of alcohol consumption that causes
damage There is no exact threshold amount As few as one drink per week may cause
damage25
A standard drink is 12 ounces of beer 5 ounces of wine or 15 ounces of
liquor Binge drinking four or more drinks in one sitting can be especially harmful26
Higher levels of consumption increase the risk of fetal damage Maternal metabolism and
alcohols interaction with other drugs are also factors that affect the amount of damage to
the fetus
The only statement that can be made with complete accuracy is that zero exposure equals
zero risk Therefore no woman should drink at any point during her pregnancy Women
who had alcohol before knowing they were pregnant should stop drinking immediately
Doing so can reduce the risk of fetal harm Research has established maternal alcohol
consumption as a leading preventable cause of birth defects and childhood disabilities in
the United States
FASD occurs after fertilization and is not caused by sperm By definition FASD cannot
be caused by the father The only cause of FASD is drinking alcohol during pregnancy
Larger Image
d
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 15
Source Moore KL and Persaud TVN 1993 The Developing Human Clinically
Oriented Embryology Philadelphia WB Saunders p 156
Findings are mixed on the effects of male alcohol use before conception Some studies
cite no discernible effects27
Others show that sons of fathers who drank alcohol have
memory deficits hyperactivity and other neurologic problems2829
There has also been
some research that suggests that alcohol use can affect the motility of sperm30
The only
way to completely avoid risk is for both parents to be alcohol free prior to conceiving a
child and for the mother to abstain from drinking alcohol throughout her pregnancy
Men may not cause FASD but they have a very important role to play in preventing
FASD They can encourage women not to drink during pregnancy They also can support
and respect a womans decision not to drink Men can also be role models for their
significant others By not drinking themselves they are modeling the safest behavior for
pregnant women Men can also help women get alcohol treatment and follow their
treatment plans These actions can help women remain alcohol free during their
pregnancies
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 16
Effects of Alcohol on the Developing Brain
Alcohol can damage the developing brain when it crosses the placenta Since the brain
develops throughout pregnancy alcohol exposure at any time can cause brain damage
Prenatal exposure to alcohol can change the brain structurally in ways that can be viewed
and measured including
Small head (microcephaly) usually below the 10th percentile
Hydrocephalus an abnormal accumulation of fluid31
that causes the brain and
skull to enlarge
Absence of the corpus callosum an area of the brain that contains nerve fibers
that bridges the two hemispheres of the brain MRIs have shown completely
missing areas of the brain in individuals with an FASD3233
Abnormal cysts or cavities in the brain
Neurologic problems such as seizures tremors and poor fine motor skills
Patterns of dysfunction on psychometric tests
Prenatal exposure to alcohol also can change the function of different parts of the brain
leading to deficits in executive functioning memory word retrieval concrete thinking
cognitive flexibility sensory integration difficulties and sleep disturbances The damage
can lead to developmental delays learning disabilities and behavior problems such as
Mental retardation
Problems with attention
Hyperactivity
Poor impulse control
Problems in social perception
Speech and language delays or deficits
Poor capacity for abstract thinking
Specific deficits in math skills
Poor judgment
Problems with cause and effect
Problems anticipating consequences
Problems changing behavior or response in different situations
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 17
Effects of Alcohol on the Developing Brain Continued
Effects of Alcohol on Specific Brain Function
Alcohol can affect specific parts of the brain in ways that impair several functions34
Corpus Callosum The corpus callosum connects the two hemispheres of the
brain allowing the left and right sides to communicate Prenatal alcohol exposure
can cause abnormalities such as thinning or complete absence These have been
linked to deficits in attention intellectual function reading learning verbal
memory executive function and psychosocial functioning
d
Source Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Images provide insight into FAS Alcohol Health amp Research World 18(1)49ndash
52
Hippocampus The hippocampus is involved in memory but its precise function
is uncertain Alcohol can change the fibers and cause cell reduction Some
persons with prenatal alcohol exposure have deficits in spatial memory and other
memory functions associated with the hippocampus The hippocampus also acts
as a mood control center Damage to the hippocampus can affect the ability to
respond appropriately to emotions such as anger
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 18
Basal Ganglia The basal ganglia are nerve cell clusters involved in motor
abilities and cognitive functions Heavy prenatal alcohol exposure can reduce
basal ganglia volume This can affect skills related to perception such as the
ability to manage time or inhibit inappropriate behavior
Cerebellum The cerebellum is involved in both motor and cognitive skills The
cerebellum tends to be smaller in people with an FASD Damage to the
cerebellum can cause learning deficits and problems with motor skills such as
balance and coordination
Hypothalamus The hypothalamus helps maintain the bodys internal
environment through the receipt of sensory and chemical input It controls areas
such as appetite emotions temperature and pain sensation Persons with an
FASD may not experience pain or respond appropriately to hot or cold
Frontal Lobes The frontal lobes control executive functions such as planning
and problem solving They also control impulses and judgment Frontal lobes can
be smaller in teenagers and young adults prenatally exposed to alcohol Persons
with an FASD may have poor impulse control and self-monitoring They might
engage in risky or illegal activity to fit in with peers
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 19
Relationship Between Prenatal Alcohol Use and FetalInfant Death
Researchers identified an association between prenatal alcohol exposure and fetal death
more than 20 years ago The likelihood of miscarriage increased directly with alcohol
consumption Risk was twice as high in women consuming 1 ounce of absolute alcohol
as infrequently as twice a week35
More recently fetal mortality was found to be 77
percent higher when alcohol was consumed during pregnancy36
Prenatal alcohol
exposure is also associated with a higher rate of infant death37
A related research finding was that siblings of children with FAS had increased risk of
death due to infectious illness and sudden infant death syndrome (SIDS) compared with
controls A diagnosis of FAS is an important risk marker for mortality in siblings of an
individual with FAS even if the siblings do not have FAS Maternal alcoholism appears
to be a useful risk marker for increased mortality risk in diagnosed cases and their
siblings38
In some populations such as Northern Plains Indians binge drinking (four or
more drinks on one occasion) in the first trimester was associated with an increased risk
of SIDS39
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 20
Comparative Effects of Alcohol and Other Substances on the Developing Fetus
Commonly abused substances include
Alcohol
Tobacco
Heroin
Methadone
Cocaine
Marijuana
Prescription drugs
Of these alcohol produces by far the most serious neurobehavioral effects in the fetus40
The table shows various effects of different substances Only alcohol can produce all of
the noted problems In addition combinations of substances (eg alcohol and tobacco)
can produce more serious effects than either substance alone Many women use multiple
substances
Alcohol Tobacco Opioids Amphetamines Cocaine Marijuana PCP
Growth deficiency X X X X X X X
Behavior
problems X X X X X X
Cognitive
problems X X X X X
Motor deficits X X X
Developmental
delays X X
Facial anomalies X X
Physical defects X X X X
Source Briggs G G Freeman R K amp Yaffe S J (2002) A reference guide to fetal
and neonatal risk Drugs in pregnancy and lactation Philadelphia PA Lippincott
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 21
Williams amp Wilkins Plessinger M A (1998 March) Prenatal exposure to
amphetamines Risks of adverse outcomes in pregnancy Obstetrics and Gynecology
Clinics of North America 25(1) 119-138 Fraser Askin D amp Diehl-Jones B (2001)
Cocaine Effects of in utero exposure on the fetus and neonate Journal of Perinatal and
Neonatal Nursing 14(4) 83-102
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 22
Issues Related to Professional Values and Ethics
The role of the counselor in addiction treatment is to provide support and education
Addiction professionals also need to use treatment approaches that help women move
from unhealthy self-defeating self-devaluing behaviors to healthy self-enhancing and
self-nurturing behaviors The counselor needs to understand the roots of alcohol abuse
among women as well as symptoms motivation problems and issues to enhance
engagement and treatment effectiveness
It is important for the addiction professional to know and believe that women do not try
to hurt their babies Cases of women drinking to induce a miscarriage or harm the baby
are very rare Most women want healthy babies but some cannot stop drinking even
when they are pregnant Addiction professionals can provide needed support and
understanding as women go through the difficult process of recovery
Clients often feel a great deal of shame associated with their addictive behaviors Some
clients may learn about FASD and realize that their children might have an FASD This
discovery can increase their guilt and shame when they realize they have harmed their
children permanently Alcohol problems already carry a tremendous stigma in our
society particularly when women drink To help resolve those feelings of shame and
guilt the counselor should encourage the client to speak honestly about her addictive
behaviors and respond to the client with honesty gentleness and care
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 23
Issues Related to Professional Values and Ethics Continued
Counselor Know Thyself
Learning about FASD can raise many issues for addiction professionals Addiction
professionals have been socialized within a society that takes punitive measures against
women who abuse alcohol during pregnancy Elements of this attitude may consciously
or subconsciously exist within the professional Perhaps they have a preconceived notion
about how pregnant women are supposed to act feel or think They may have
insufficient knowledge and skills to build relationships that are respectful and safe for
women to explore painful issues such as having a child with an FASD
It is important for counselors to be aware that their own background socialization and
experiences influence the therapeutic relationship These include their personal
experience with alcohol use disorders as well as their attitudes values and biases
Addiction professionals need to recognize the limits of their competencies and expertise
A counselors self-assessment regarding his or her knowledge of women-specific alcohol
use disorders and appropriate women-specific interventions can help in establishing a
starting point and planning strategies for building capacity and quality care
Many addiction professionals are recovering from alcohol use disorders Others have no
alcohol abuse history of their own but have been close to someone elses active addiction
This firsthand experience of addiction can add to the counseling process In some cases it
may complicate the process Counselors might recognize signs and symptoms of FASD
in their own children and have feelings of guilt and shame
When professionals have not come to grips with their own issues they sometimes project
these issues onto others Often the pain and chaos of clients lives can trigger their own
intense pain and fear It is important to seek help to resolve these feelings and to get help
for ones children Recognizing these feelings and addressing them can help the counselor
set limits and protect boundaries and avoid transferring these feelings to the client In
addition it can help the counselor avoid self-disclosure that might make clients
uncomfortable or shift the focus to the counselor The focus must always be on the
clients recovery
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 24
Matching Activity
Match the word or term in column A with the appropriate description in column B
Type letter from column A into correct answer box in column B
Column A Column B
A) Alcoholic embryopathy Fetal alcohol spectrum disorders
B) Fetal Alcohol Syndrome A term identified by Dr Lemoine that describes
the distinct features related to prenatal alcohol
exposure
C) Alchoholic Beverage Labeling
Act of 1988 Pattern of neurologic behavioral and cognitive
deficits that can interfere with learning growth and
socialization
D) FASD A law requiring alcoholic beverage labels to
carry a warning about birth defects
E) Components of FAS Facial abnormalities growth deficiencies brain
damage prenatal alcohol exposure
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 25
Test Your Knowledge Questions Posttest
Posttests are designed to gauge what youve learned by reading the competency Click in
the circle or box next to the correct answer Circles indicate that only one correct answer
is possible Boxes indicate that more than one correct answer is possible
1 When a pregnant woman drinks the blood alcohol level of the fetus becomes equal
to or greater than the motherrsquos
True
False
2 In what year did the US Surgeon General issue warnings against alcohol use during
pregnancy
A 1970
B 1980
C 1981
D 1977
3 Which substance produces the most serious neurobehavioral effects in the fetus
A Tobacco
B Heroin
C Cocaine
D Alcohol
4 In 1973 who identified a specific pattern of malformations and deficits in children
of alcoholic mothers
A Dr William Sullivan
B Johnson and Johnson
C Jones and Smith
D IOM
5 The brain develops throughout pregnancy Alcohol exposure at any time during the
pregnancy can cause brain damage
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 26
True
False
6 The terms FASD and FAS are interchangeable
True
False
7 Women respond to alcohol differently then men do These differences include
Select all that apply
A Co-occurring problems and issues interacting with alcohol use
B Patterns of alcohol abuse
C Context for the initiation and maintenance of alcohol abuse
D Problems and consequences ensuing from alcohol abuse
8 Based on which of the following factors do women experience the damaging
consequences of chronic alcohol use more severely and rapidly than men
Select all that apply
A Psychosocial
B Visual
C Medical
D Physiological
9 How does the rate for FASD compare with the rate of Down syndrome or spina
bifida
A Higher
B Lower
C Equal
10 Which of the following are major components of FAS
A Growth deficiencies such as low birth weight
B Brain damage with neurologic deficits such as impaired fine motor skills
poor eye-hand coordination and tremors
C Maternal alcohol use during pregnancy
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 27
D All of the above
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 28
References
1 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
2 Abel EL 1990 Fetal Alcohol Syndrome Oradell NJ Medical Economics
3 Warner PH and Reset HL 1975 The effects of drinking on offspring an
historical survey of the American and British literature Journal of Studies on
Alcohol 36(1)1395-1420
4 Lemoine P Harousseau H Borteyru J-P et al 1968 Les enfants de parents
alcooliques Anomalies observees A propos de 127 cas [Children of alcoholic
parents Abnormalities observed in 127 cases] Ouest Medical 21476-482
5 Jones KL and Smith DW 1973 Recognition of the fetal alcohol syndrome in
early infancy Lancet 2999-1001
6 Phillips DK Henderson GI and Schenker S 1989 Pathogenesis of fetal
alcohol syndrome Overview with emphasis on the possible role of nutrition
Alcohol Health amp Research World 13(3)219-227
7 Randall CL 1987 Alcohol as a teratogen A decade of research in review
Alcohol and Alcoholism Suppl 1125-132
8 Majewski F Bierich JR Loser H et al 1976 Clinical aspects of
pathogenesis of alcohol embryopathy (authors translation)] Munchener
Medizinische Wochenschrift 118(50)1635-1642 [Article in German]
9 Dehaene P Samaille-Villette C Crepin G et al 1977 Le syndrome
dalcoolisme foetal dans le Nord de la France La Revue de lAlcoolisme 23145-
158
10 Olegard R Sabel KG Aronsson M et al 1979 Effects on the child of
alcohol abuse during pregnancy Retrospective and prospective studies Acta
Paediatrica Scandinavica Suppl 275112-121
11 Streissguth A 1994 A long-term perspective of FAS Alcohol Health amp
Research World 18(1)74-81
12 Office of Applied Studies 2005 Results from the 2004 National Survey on Drug
Use and Health National Findings NSDUH Series H-28 DHHS Publication No
SMA 05-4062 Rockville MD Substance Abuse and Mental Health Services
Administration (SAMHSA)
13 Naimi TS Lipscomb LE Brewer RD et al 2003 Binge drinking in the
preconception period and the risk of unintended pregnancy Implications for
women and their children Pediatrics 111(5 Part 2)1136-1141
14 Bertrand J Floyd RL Weber MK et al 2004 Fetal Alcohol Syndrome
Guidelines for Referral and Diagnosis Atlanta GA Centers for Disease Control
and Prevention
15 Centers for Disease Control and Prevention (CDC) 2002 Fetal alcohol
syndromemdashAlaska Arizona Colorado and New York 1995-1997 MMWR
51433-435
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 29
16 CDC 1997 Surveillance for fetal alcohol syndrome using multiple sourcesmdash
Atlanta Georgia 1981-1989 MMWR 461118-1120
17 CDC 1995 Update trends in fetal alcohol syndromemdashUnited States 1979ndash1993
MMWR 44249-51
18 CDC 1993 Fetal alcohol syndromemdashUnited States 1979-1992 MMWR 42239-
241
19 Cordero JF Floyd RL Martin ML et al 1994 Tracking the prevalence of
FAS Alcohol Health amp Research World 1882-85
20 May PA and Gossage JP 2001 Estimating the prevalence of fetal alcohol
syndrome A summary Alcohol Research amp Health 25159-167
21 Mirkes PE ed 2003 Congenital malformations surveillance report A report
from the national birth defects prevention network Birth Defects Research 67(9)
22 Sampson PD Streissguth AP Bookstein FL et al 1997 Incidence of fetal
alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder
Teratology 56317-326
23 Egeland GM Katherin PH Gessner BD et al 1998 Fetal alcohol syndrome
in Alaska 1977 through 1992 An administrative prevalence derived from
multiple data sources American Journal of Public Health 88781-786
24 Chavez GF Cordero JF and Becerra JE 1988 Leading major congenital
malformations among minority groups in the United States 1981-1986 MMWR
37(SS-3)17-24
25 Sood B Delaney-Black V Covington C et al 2001 Prenatal Alcohol
Exposure and Childhood Behavior at Age 6 to 7 Years I Dose-Response Effect
Pediatrics 108(2) e34
26 Jacobson JL and Jacobson SW 1994 Prenatal alcohol exposure and
neurobehavioral development Where is the threshold Alcohol Health amp
Research World 1830-36
27 Jacobson JL and Jacobson SW 1999 Drinking moderately and pregnancy
Effects on child development Alcohol Research amp Health 23(1)25-30
pubsniaaanihgovpublicationsarh23-125-30pdf
28 Livy DJ Maier SE and West JR 2004 Long-term alcohol exposure prior to
conception results in lower fetal body weights Birth Defects Research Part B
Developmental and Reproductive Toxicology 71(3)135-141
29 Abel E 2004 Paternal contribution to fetal alcohol syndrome Addiction Biology
9(2)127-133 discussion 135-136
30 Jamerson PA Wulser MJ and Kimler BF 2004 Neurobehavioral effects in
rat pups whose sires were exposed to alcohol Brain Research Developmental
Brain Research 149(2)103-111
31 Dare WN Natrona CC Kusemiju OT et al 2002 The effect of ethanol on
spermatogenesis and fertility in male Sprague-Dawley rats pretreated with
acetylsalicylic acid Nigerian Postgraduate Medical Journal 9(4)194-198
32 Berg S Kinsey K Lutke J et al 1995 A Laymans Guide to Fetal Alcohol
Syndrome and Fetal Alcohol Effects Surrey BC FASE Support Network
33 Mattson SN Jernigan TL and Riley EP 1994 MRI and prenatal alcohol
exposure Alcohol Health amp Research World 18(1)49-52
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press
Page 30
34 Mattson SN and Riley EP 1995 Prenatal exposure to alcohol What the
images reveal Alcohol Health amp Research World 19(4)273-277
35 Mattson SN Schoenfeld AM Riley EP 2001 Teratogenic effects of alcohol
on brain and behavior Alcohol Research amp Health 25(3)185-191
36 King JC and Fabro S 1983 Alcohol consumption and cigarette smoking
Effect on pregnancy Clinical Obstetrics and Gynecology 26(2)437-448
37 Hoyert DL 1996 Medical and life-style risk factors affecting fetal mortality
1989ndash90 Vital and Health Statistics 20(31)
38 Faden VB Graubard BI and Dufour M 1997 The relationship of drinking
and birth outcome in a US national sample of expectant mothers Paediatric and
Perinatal Epidemiology 11(2)167-80
39 Burd L Klug M and Martsolf J 2004 Increased sibling mortality in children
with fetal alcohol syndrome Addiction Biology 9(2)179-186 discussion 187-188
40 Iyasu S Randall LL Welty TK et al 2002 Risk factors for sudden infant
death syndrome among northern plains Indians JAMA 288(21)2717-2723
41 Stratton K Howe C and Battaglia F eds 1996 Fetal Alcohol Syndrome
Diagnosis Epidemiology Prevention and Treatment Washington DC Institute
of Medicine National Academy Press