Page 1
3/28/2016
1
Compliant
RA Coding
and the EHRSheri Poe Bernard, CCS-P, CPC, COC, CPC-I
2
Consider factors that brought us to the EHRs we are
coding from today, and what a “compliant” EHR is
Explore benefits of taking a proactive approach to EHR
compliance issues and policies in the RA workplace
Learn to discern difference between good and bad data
within an EHR
Discuss impact of EHRs on diagnosis support and
reporting
Today’s goals
Page 2
3/28/2016
2
3
Office of the National Coordinator for Health
Information Technology (ONC):
EHR goals: Improve quality, safety, efficiency, and reduce health disparities
Engage patients and family
Improve care coordination, and population and public health
Maintain privacy and security of PHI
Ultimately, it is hoped it will result in:
• Better clinical outcomes
• Improved population health outcomes
• Increased transparency and efficiency
• Empowered individuals
• More robust research data on health systems
Meaningful use
4
CMS: Pressured for implementation of certified plans with $$$
Certifiers: Standards ignored coding/documentation compliance
HHS and Office of National Coordinator of HIT: Did not publish
coding/documentation guidance for EHRs
Med Schools: Clinical documentation addressed without any focus on
EHR platforms, compliance and coding is barely mentioned
Software vendors: Promised time and personnel cutting, advised to
omit coders from selection process
Providers and facilities: Drank the Kool-Aid, often did NOT involve
coding staff in purchase decisions
Group practices and facilities: Impose productivity standards
RA auditors: Usually do not have access to providers and bounce
between many different EHR platforms
A Perfect Storm
Page 3
3/28/2016
3
5
Electronic health records
Feature-by-feature review
What is CMS’ position
Affect on RA compliance
Unintended consequences
6
EHR may not include all elements of eSignature
requirements
Name, credential, date, “electronically signed by”
eSignature at beginning of record
Identifying author doesn’t “authenticate” record
CMS’ position
Most of what CMS has to say about electronic signatures is
regarding safeguards of access to the electronic record, and
identification of authorship. An e-signature should be dated and the
author’s credentials should be included.
RA compliance
Communicate to clients any system-wide shortcomings
eSignature issues
Page 4
3/28/2016
4
7
Differentiating between authorship and approval
eSignature issues
8
EHR doesn’t differentiate among documentation
authors, line by line or entry by entry
CMS’ position
“Abuse” describes incidents or practices that may not be fraudulent
but are not consistent with accepted medical or business practices or
may result in unnecessary costs. Some such incidents directly relate
to EHR software features, such as allowing multiple providers to
add text to the same progress note but not allowing each provider to
sign, making it impossible to verify the actual service provider or
the amount of work performed by each provider.
RA compliance
Policy to ensure authorship issues are flagged
Policy to alert clients when EHRs have faulty software features
Authorship errors
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-provider-booklet-overview.pdf
Page 5
3/28/2016
5
9
EHR doesn’t date problem list or med list
CMS’ position
Defaulting or copying and pasting clinical information with previous
existing documentation from other patient encounters in a different
health record facilitates billing at a higher level of service than was
actually provided.
RA compliance
Policy to accept only dated or referenced med lists
Policy to omit all problem lists, or accept only dated or referenced
problem lists
Authorship errors
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-provider-booklet-overview.pdf
10
Check boxes instead of free text
Templates: Using predefined text and text options to document the
patient visit within a note
Macros: Expanding text associated with abbreviations or specific
keystrokes
Populating via Default: Generating content without positive action
or selection by author
CMS’ position
Some EHR systems use templates that complete forms by checking a
box, macros that fill in information by typing a key word, or auto-
population of text when it is not entered. Problems can occur if the
structure of the note is not a good clinical fit and does not
accurately reflect the patient’s condition and services. These
features may encourage over-documentation even when services are
not medically necessary or are never delivered.
Moving to Documentation…
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-provider-booklet-overview.pdf
Page 6
3/28/2016
6
11
Check boxes instead of free text
Templates: Using predefined text and text options to document the
patient visit within a note
CMS’ position
Policy should require providers to modify templates so that
documentation clearly reflects specific conditions and observations
unique to the service, and to clearly identify the services provided.
Policy should also require the physician to provide additional
information to describe the patient in the specific episode of illness.
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
12
Sample
Checked BoxesIn a “template,”
the boxes are
blank.
Page 7
3/28/2016
7
13
Check boxes instead of free text
Macros: Expanding text associated with abbreviations or specific
keystrokes. Macros allow users to generate a lot of documentation
with one click. This practice is also referred to as charting by
exception
Populating via Default: Generating content without positive action
or selection by author
CMS’ position
Policy should require the provider to verify the validity of
information on entry.
Providers should incorporate policies and control structures that
require the addition of free text when auto-population methods are
used.
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
14
Check boxes instead of free text
Templates: Using predefined text and text options to document the
patient visit within a note
Macros: Expanding text associated with abbreviations or specific
keystrokes
Populating via Default: Generating content without positive action
or selection by author
RA compliance
Create policies addressing “good clinical fit” and “accurately reflect
patient’s condition”
Train coders to understand auto-generation of text and macros so
they can interpret documentation better
Do not use anything populated by default as support (if you can
detect the methodology)
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-provider-booklet-overview.pdf
Policy should require the provider to modify copied information to be patient-specific and related to the current visit.
Page 8
3/28/2016
8
15
Click boxes to complete system reviews
Designed after old templates like those produced by T Systems
Templates do not reflect the complexity of the diagnosis or
medical decision making
Qualitative data missing:
Chest pain (intermittent, with exercise, constant, debilitating)
Cough (at night, productive, dry, reactive, crouplike)
Type 2 diabetes (affecting daily living, managed with diet, with oral
meds, in a confident or unconfident patient)
RESULT: Support often missing when ROS/PE is templated list
Unintended consequences: template
16
Patient presents with nausea, vomiting and abdominal pain
Before EHRPHYSICAL EXAM: VITALS; BP 136/82, P 76, R 16, afebrile. W 178, RBS 96. HEART: regular rate and rhythm
without murmur or gallops. LUNGS: clear to auscultation all fields without rales, rhonchi or wheezing. ABDOMEN:
soft with active bowel sounds, no muscle guarding, lower left abdominal tenderness noted, no palpable mass or
organomegaly noted. EXTREMITIES: no edema
After EHRPHYSICAL EXAM: This is a well-developed, well-nourished male in no acute distress. VITALS: BP 138/74, P 62, W
164, P02 95 R 16 RBS 99 BMI 32. TEMP 98.6 HEAD: Normocephalic, atraumatic, no visible or palpable masses,
depressions or scaring. PERRLA. TMs translucent and mobile. Remainder of the ENT exam is unremarkable. NECK:
Supple. Euthyroid with no lymphadenopathy and nontender. Carotid pulses equal bilaterally. No bruits noted. LUNGS:
Clear to auscultation and percussion. HEART: Regular rate and rhythm. There are no murmurs or gallops noted. No
cardiomegaly or thrills. ABDOMEN: soft, lower left abdominal tenderness noted. There are no masses noted. There is
no hepatosplenomegaly noted. Active bowel sounds. EXTREMITIES: There is no edema, clubbing or cyanosis noted.
Peripheral pulses are +2 bilaterally. NEUROLOGIC: CN 2-12 normal. Deep tendon reflexes are +2 bilaterally.
Strength 5/5 and symmetrical. Babinski negative, no clonus, gait normal. PSYCHIATRIC: oriented x3, judgment and
insight good, normal mood and affect. Recent and remote memory intact.
Unintended consequences: template
Page 9
3/28/2016
9
17
Check boxes instead of free text
CMS’ position
Some EHR systems use templates that complete forms by checking a
box, macros that fill in information by typing a key word, or auto-
population of text when it is not entered. Problems can occur if the
structure of the note is not a good clinical fit and does not
accurately reflect the patient’s condition and services. These
features may encourage over-documentation even when services are
not medically necessary or are never delivered.
RA compliance
Seek support of any checked diagnosis boxes elsewhere in the
documentation
Identify those documents in which free text is permitted with
checked boxes. This may provide support.
Data-entry shortcuts
18
Automated narrative function (template translated
into documentation narrative)
Data-entry shortcuts
Page 10
3/28/2016
10
19
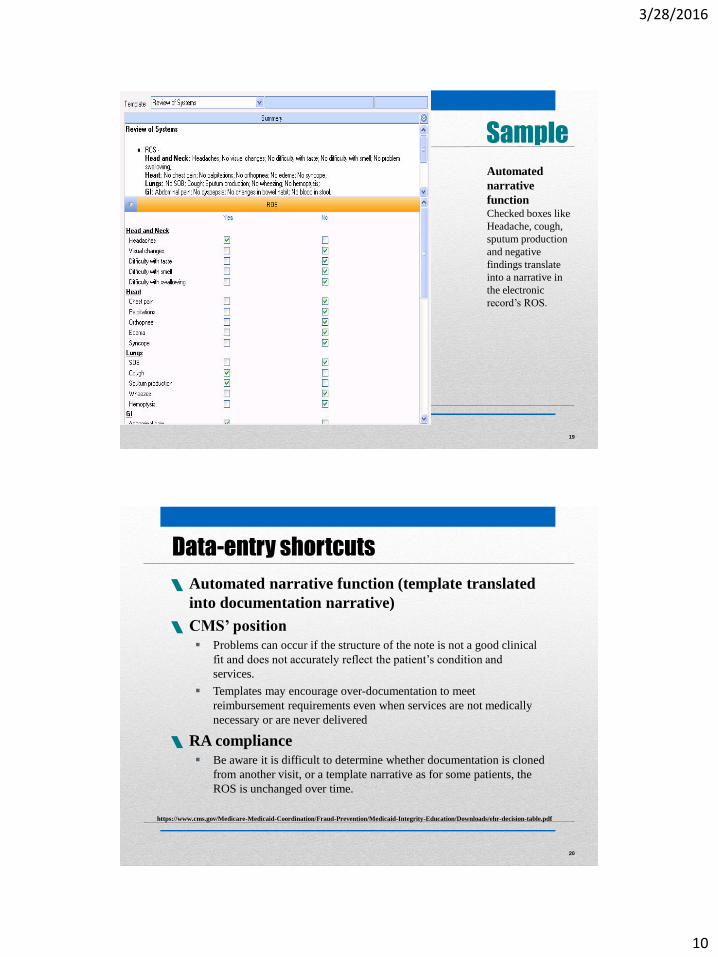
Sample
Automated
narrative
functionChecked boxes like
Headache, cough,
sputum production
and negative
findings translate
into a narrative in
the electronic
record’s ROS.
20
Automated narrative function (template translated
into documentation narrative)
CMS’ position
Problems can occur if the structure of the note is not a good clinical
fit and does not accurately reflect the patient’s condition and
services.
Templates may encourage over-documentation to meet
reimbursement requirements even when services are not medically
necessary or are never delivered
RA compliance
Be aware it is difficult to determine whether documentation is cloned
from another visit, or a template narrative as for some patients, the
ROS is unchanged over time.
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
Page 11
3/28/2016
11
21
Auto-forward of clinical data
System pulls details of last visit (H&P, med list, past medical history,
etc.) into today’s encounter to streamline documentation
CMS’ position
This can affect the quality of care and can cause improper payments
due to:
• Potentially false impression of services provided to the patient
• Coding from old or outdated information that may lead to “upcoding”
Policy should require the provider to modify copied information to
be patient-specific and related to the current visit.
RA compliance
Internal policies should address how to handle pull-forward
information and when it can be reported with support, or used as
support
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
22
Auto-forward of clinical data
Data-entry shortcuts
Page 12
3/28/2016
12
23
Cloning
Copy and Paste: Selecting data from one location and reproducing it
in another; also called “cloning,” “cookie cutter,” “copy forward,”
and “cut and paste.” Clinical plagiarism occurs when a physician
copies and pastes information from another provider and calls it his
or her own
CMS’ position
Policy should require the provider to modify copied information to
be patient-specific and related to the current visit.
Copied information should include proper notation and clear
attribution.
Best Practices: Providers must recognize each encounter as a stand-
alone record, and ensure the documentation for that encounter
reflects the level of service actually provided and meets payer
requirements for billing and reimbursement.
Data-entry shortcuts
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/Downloads/ehr-decision-table.pdf
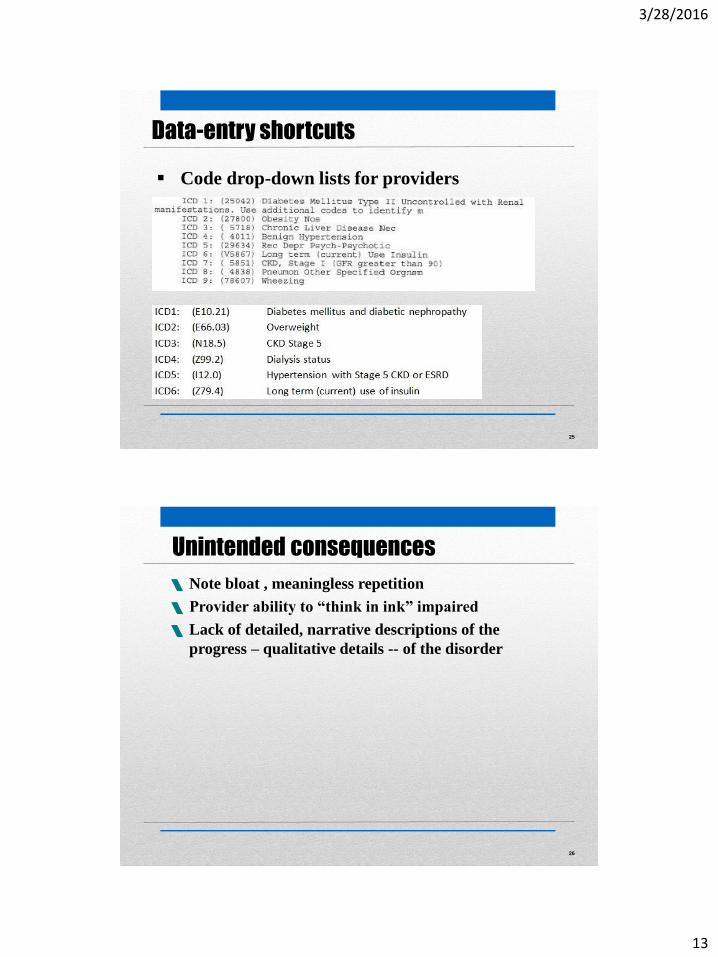
24
Code drop-down lists for providers
Often list unspecified first
May have truncated definitions
Don’t include guidance
CMS’ position
Begin in the Index. Then access the code in the
Tabular section and read all guidance there.
RA compliance
Display may not include narrative diagnosis, only code
Display may include code and truncated description
Data-entry shortcuts
Page 13
3/28/2016
13
25
No links between etiology and manifestation
Data-entry shortcuts
Code drop-down lists for providers
26
Note bloat , meaningless repetition
Provider ability to “think in ink” impaired
Lack of detailed, narrative descriptions of the
progress – qualitative details -- of the disorder
Unintended consequences
Page 14
3/28/2016
14
27
UTI
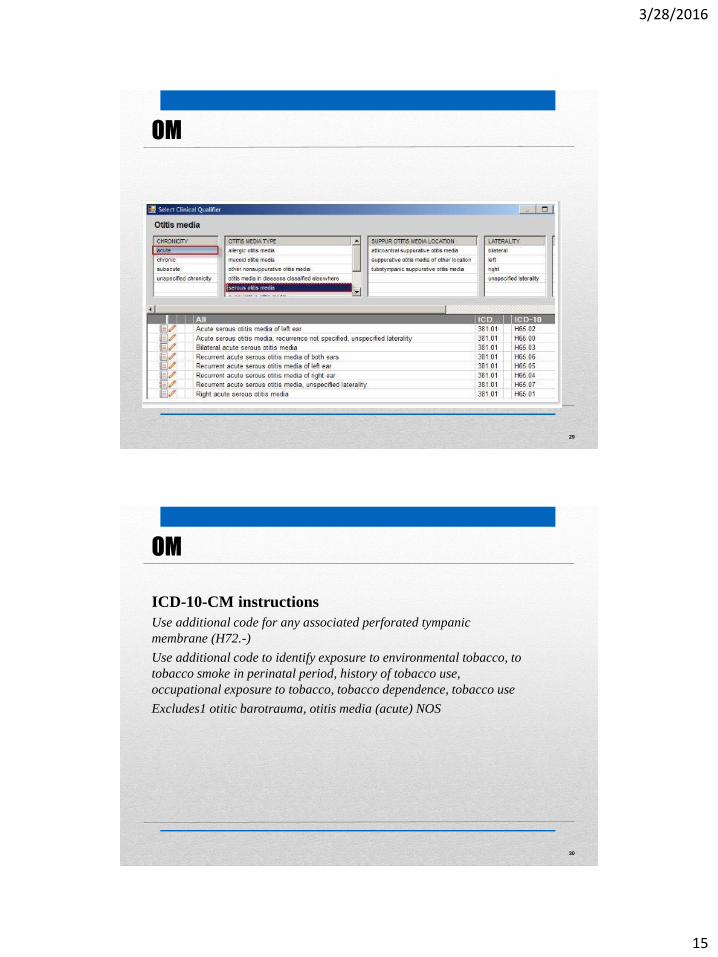
28
Incomplete pulldown menus of diagnoses
Otitis media in ICD-10
OM
Page 15
3/28/2016
15
29
Incomplete pulldown menus of diagnoses
Otitis media in ICD-10
OM
30
ICD-10-CM instructions
Use additional code for any associated perforated tympanic
membrane (H72.-)
Use additional code to identify exposure to environmental tobacco, to
tobacco smoke in perinatal period, history of tobacco use,
occupational exposure to tobacco, tobacco dependence, tobacco use
Excludes1 otitic barotrauma, otitis media (acute) NOS
OM
Page 16
3/28/2016
16
31
Unintended consequences
32
OIG
“ICD–9–CM codes reported on the health insurance claims form
should be supported by documentation.” … “In addition to facilitating
high quality patient care, a properly documented medical record
verifies and documents precisely what services were actually
provided. The medical record may be used to validate: (a) The site of
the service; (b) the appropriateness of the services provided; (c) the
accuracy of the billing; and (d) the identity of the care giver (service
provider)”
-- The OIG Compliance Program for Individuals and
Small Group Physician Practices (Federal
Register, Oct 5 2000, Page 59440)
Coding from codes
Page 17
3/28/2016
17
33
Guidelines
“The importance of consistent, complete documentation in the
medical record cannot be overemphasized. Without such
documentation accurate coding cannot be achieved.”
-- ICD Official Guidelines for Coding and Reporting
Coding from codes
34
Actual example of provider coding
“30-week multigravida seen today for an uncomplicated
OB office visit. Diagnoses: V22.2 Intrauterine pregnancy
and V45.89 History of cesarean section.”
V22.2 Pregnant state, incidental
V45.89 Other postprocedural status
Correct code:
654.23 Previous cesarean delivery, antepartum
Unintended consequences: Codes
Page 18
3/28/2016
18
35
Written policy for when the system goes down
And what happens when the system goes back up to
recreate the documentation?
Written policy on what is considered the legal medical
record.
Once was all the paper in the chart. Now, it could have
wider scope. What will you exclude from a request for a
medical record?
• Audio dictation files; audio patient telephone files
• Nursing reports
• Videorecordings of procedures
• Recorded telemedicine consults
Other issues to consider
36
https://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/electronic-health-records.html
Or Google:
CMS EHR toolkit program integrity 2015
EHR Toolkit from CMS
Page 19
3/28/2016
19
37
Decision Table
38
Page 20
3/28/2016
20
39
Monitoring and Auditing
40
Expand your policies and procedures
Keep vigil on evolving compliance requirements
Consider clinical as well as coding implications of EHR flaws
Download CMS EHR Toolkit athttps://www.cms.gov/Medicare-Medicaid-Coordination/Fraud-Prevention/Medicaid-Integrity-Education/electronic-health-records.html
Your takeaway
Page 21
3/28/2016
21
Thank you
Contact information
Sheri Poe Bernard, CPC, CPC-I, CCS-P
Phone 801-582-7000
Email [email protected]