Page 1
Accepted Manuscript
Comprehensive surgical management of CIMDL
Giacomo Colletti, MD Luca Autelitano, MD Matteo Chiapasco, MD Federico Biglioli,MD Federica Giovanditto, MD Marco Mandalà, MD Fabiana Allevi, MD
PII: S0278-2391(14)00326-7
DOI: 10.1016/j.joms.2014.03.013
Reference: YJOMS 56260
To appear in: Journal of Oral and Maxillofacial Surgery
Received Date: 21 January 2014
Revised Date: 8 March 2014
Accepted Date: 10 March 2014
Please cite this article as: Colletti G, Autelitano L, Chiapasco M, Biglioli F, Giovanditto F, Mandalà M,Allevi F, Comprehensive surgical management of CIMDL, Journal of Oral and Maxillofacial Surgery(2014), doi: 10.1016/j.joms.2014.03.013.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
Page 2
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Comprehensive surgical management of CIMDL
Giacomo Colletti MD1, Luca Autelitano MD,1 Matteo Chiapasco MD,2 Federico Biglioli MD,1
Federica Giovanditto MD,1 Marco Mandalà MD,3 Fabiana Allevi MD,1
1 University of Milan, Department of Maxillo facial surgery, San Paolo Hospital, Milan, Italy
2 University of Milan, Department of Oral Surgery, San Paolo Hospital, Milan, Italy
3 University of Verona, Department of Otolaryngology, Verona, Italy
Corresponding Author
Giacomo Colletti
Via di Rudinì 8,
20142 Milan, Italy
Tel.: +39281844593
Fax: +39281844704
Mail: [email protected]
Page 3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Abstract
Purpose: This article presents a review of the literature and proposes a protocol for managing
midfacial cocaine-induced acute and chronic injuries.
Methods: We report a series of four patients affected by cocaine-induced midline destructive
lesions (CIMDL). Three of the patients came to our attention after 18 months of drug
withdrawal and underwent surgical treatments to restore nasal and palatal morphology and
function, while the fourth patient was referred due to acute cocaine-induced destructive
lesions and was treated by aggressive debridement. An 18-month drug-free period is planned
before beginning any reconstructive procedures in this latter patient.
Results: Long-term follow-up showed stable results without relapse of palatal fistulas and
good esthetic nasal appearance in all three patients undergoing reconstruction. The fourth
patient did not show any disease progression and will be monitored for drug withdrawal.
Conclusion: Chronic cocaine consumption may cause multiple types of damage to the soft and
hard tissues of the midface. Acute lesions must be addressed with aggressive debridement. As
a result of chronic injury, the palate and the nose are deformed in a very complex way and the
vascularity of remaining local tissues may be compromised or inadequate for flap harvesting.
Palatal and nasal reconstructions are very delicate operations and they should be addressed
separately to maximize the predictability of the result.
Introduction
Cocaine is an alkaloid obtained from Erythroxylum coca plant leaves. The earliest known use
of cocaine was by sub-Andean Indians as a stimulant, while Koller first introduced its use in
medicine as local anesthetic in 1884.1
Page 4
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
More recently, cocaine has been used as a recreational drug because of its stimulating effects,
resulting in socioeconomic and physical damage. Cocaine is most commonly administered
intranasally, and the snorting of this drug has been associated with chronic rhinitis, epistaxis,
nasal septum perforations, lateral nasal wall destruction, and hard palate involvement with
oronasal communication.2,3 Cocaine inhalation damages the mucosal lining of the nose,
resulting in ischemia and necrosis, which lead to exposure and perforation of septal cartilage
and bones. As the disease progresses, the load-bearing structures of the nose can be lost with
consequent nasal collapse and central midface deformation.4 This is caused by a central
midfacial granulomatous destructive process, simulating other aggressive pathologies, such as
systemic lupus erythematosus, Wegener’s granulomatosis, tertiary syphilis, and
lymphoproliferative disorders, and is described in the literature as cocaine-induced midline
destructive lesions (CIMDL).5–7 A diagnosis of CIMLD is confirmed when two of the three
following signs are present: nasal septum perforation, lateral wall nasal destruction, and/or
hard palate involvement.6 Nasal septum perforation represents the most common
complication in cocaine abuse, affecting 5% of abusers.8 These adverse physical effects were
first described by Owens in 1912.9 Cocaine abuse has become a growing public health
problem, because of the rarity of short-term medical adverse effects and the poor
socioeconomic level of most abusers.1
Several methods have been reported for reconstructing the nose and palate damaged by
repeated cocaine inhalation. This article presents a series of four patients affected by CIMDL
who underwent surgical treatments for acute cocaine-induced granulomatous lesions in one
case and to restore nasal and palate morphology and function in three cases.
Page 5
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMaterials and Methods
Due to the retrospective nature of this study, an exemption was granted by the internal IRB of
our institution. This study was performed in adherence to the World Medical Association
Declaration of Helsinki.
Patient 1
Patient 1 was a 43-year-old man who was referred to our surgical department because of
severe cocaine-related midfacial destructive lesions. He reported prolonged cocaine abuse
lasting 10 years, but he stopped this habit 2 years before the first visit, which was confirmed
by serial urine analysis.
The patient presented wide midline destructive lesions, characterized by extensive oronasal
communication, with posterior hard palate defect, absence of nasal septum, and collapse of
the nasal pyramid. He complained of rhinolalia and oronasal regurgitation of solids and
liquids (Figs. 1–5).
Preoperative computed tomography (CT) showed complete absence of the nasal septum, the
lateral nasal walls, and the hard palate. The patient underwent two surgical procedures over
the last 2 years. The first surgery was performed for closure of the oronasal communication
using a partially deepithelialized radial fasciocutaneous free flap10 (Fig. 6). During the second
surgery, we performed an open rhinoplasty approach and freed the external soft tissues of the
nose. At the end of this phase, it was decided that the available soft tissues were sufficient and
therefore only reconstruction of the skeletal support of the nose was required. A costal
osteochondral cantilever graft was harvested, placed in the soft tissue pocket, and fixed with a
Kirschner wire (Figs. 7–10).
After 24 months, no relapse of the fistula was detected and the nasal reconstruction was
stable with good esthetic results.
Page 6
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Patient 2
Patient 2 was a 46-year-old woman who came to our attention because of severe nasal
pyramid collapse following an intense period of cocaine abuse lasting 9 years. She presented a
wide cutaneous fistula of the left nasal ala and marked oronasal communication (Figs. 11–13).
On first examination, she reported that she had stopped abusing cocaine 2 years previously,
which was confirmed by multiple urine analysis. She was unable to breathe through her nose
because of complete collapse of the dorsum-ala complex. As she was unhappy with her
esthetic condition and complained of the passage of liquid and food in the nose, she sought
medical attention and underwent surgery to reconstruct the hard palate and nasal pyramid.
She underwent the first surgery to reconstruct the hard palate with a partially
deepithelialized radial fasciocutaneous free flap10 (Fig. 14). In a second surgery, the borders of
the nasal ala fistula was incised, all of the synechiae of the internal lining were freed, and the
defect was covered with an island melolabial flap. Three months later, we created a pocket
between the newly created internal lining and the external skin with an open rhinoplasty
approach. A costochondral graft was harvested and placed as a cantilever graft to reconstruct
the dorsum and the tip. The graft was secured in place with a Kirschner wire. Fifteen months
after the last surgery, the results were stable: no residual fistula was noted and the esthetic
results of nasal reconstruction had not changed over time (Figs. 15,16).
Patient 3
Patient 3 was a 36-year-old woman who was referred to our surgical department due to wide
oronasal communication and nasal pyramid collapse caused by cocaine abuse. The patient’s
main complaints were the inability to breathe through the nose and the nasal regurgitation of
Page 7
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
solids and liquids. She confirmed a 5-year history of cocaine abuse and complete drug
withdrawal lasting 18 months, which was confirmed by urine analysis. First, she underwent
surgery to reconstruct the hard palate with a radial fasciocutaneous free flap.10 Then, surgery
was performed to reconstruct the nasal pyramid. A first session was needed to reconstruct
the internal lining. This was performed with a grafted forehead pericranial flap, rotated
through a soft tissue tunnel at the level of the glabella. Three months later, with open
rhinoplasty access, a pocket was created in which a costochondral graft was placed and
secured to the nasal bones with a Kirschner wire.
Thirteen months after the second procedure, the palatal and nasal results are stable and the
patient no longer shows oronasal regurgitation.
Patient 4
Patient 4 was a 39-year-old woman who was referred to our institution because of CIMDL
after 10 years of cocaine abuse. The patient had not ceased drug consumption at the time of
referral. Acute lesions on the nasal septum, columella, nostrils, premaxilla, and palate were
clearly evident. These areas were characterized by the presence of granulation tissue and pus.
Bone, cartilage, and soft tissues of the nasal septum and lateral nasal wall were missing, and a
wide palatal fistula was present (Figs. 17,18).
These chronic inflammatory lesions endured for months despite conservative treatment with
antibiotics and gentle debridement. Then it was decided to perform aggressive debridement
and all of the areas involved by the process were surgically removed under general
anesthesia. No signs of new acute lesions were found several months after the operation (Figs.
19,20). The patient has since reported complete drug withdrawal. Urine analysis is performed
Page 8
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
every 2 months to confirm withdrawal, and an 18-month drug-free period is planned before
commencement of any reconstructive procedures.10
Discussion
Midfacial osteocartilaginous lesions as a result of cocaine abuse were first reported in 1988.11
Cocaine abuse is becoming increasingly common in Western countries, and cocaine use is
being seen among younger and younger people.10 Snorted cocaine induces intense
vasoconstriction, which in turn leads to severe ischemic necrosis of the affected tissues
associated with osteomyelitis and chondritis, with eventual destruction of the sinonasal and
midfacial bones and soft tissues.2 Necrosis of nasal tissues is caused by the added effects of
cocaine and topical decongestant; the caustic effects of adulterants such as talc, amphetamine,
and lidocaine; and the anesthetic effects of the drug resulting in trauma and thermal injuries,
favoring local infections. The midfacial complications of cocaine abuse are well documented.
Approximately 5% of cocaine abusers show nasal septal perforation, which is the most
frequent local complication of intranasal cocaine use.1 All of the surrounding structures, i.e.,
the lateral nasal wall and hard and soft palate, then show progressive damage, until reaching a
condition described as CIMDL.
Nasal septal perforation is usually well tolerated by these patients, while they are usually
troubled by external nasal collapse and by the oronasal fistulas that cause rhinolalia and
passage of liquids and food into the nose.
In 2005, Goodger et al. suggested that women may be more susceptible to wide palatal
necrosis and connective tissue disorders than men.2 In addition to cocaine abuse, multiple
other conditions can induce midfacial destructive lesions, including tertiary syphilis, tumors,
traumas, chronic infections (actinomycosis and tuberculosis), Wegener’s granulomatosis,
Page 9
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
systemic lupus erythematosus, and midline granulomas, often caused by angiocentric T-cell
lymphoma.1,2 In patients who do not admit to cocaine abuse, the differential diagnosis
between Wegener’s granulomatosis and cocaine-induced midfacial osteocartilaginous lesions
may be difficult because both diseases are c-ANCA-positive and show vascular lesions. The
absence of renal and pulmonary involvement does not exclude limited Wegener’s
granulomatosis; therefore, histopathology represents the gold standard for obtaining a
reliable diagnosis. Nonspecific histopathological changes are more frequent in cocaine-
induced lesions than in Wegener’s disease; fibrinoid necrosis, leukocytoclastic vasculitis,
perivenulitis, and microabscesses in the vascular wall are usually present in both pathologies;
and extravascular changes such as stromal granulomas with giant cells, microabscesses, and
deeply localized necrosis are pathognomonic features of Wegener’s granulomatosis that are
not present in CIMDL.12–14
Drug abusers are difficult patients as they are prone to lie regarding their condition and often
show poor compliance. However, there is little information in the literature regarding the
general treatment of these patients.
Several aspects must be taken into consideration in the management of CIMDL. The first is the
management of acute lesions. As seen in patient 4, these are essentially caused by areas of
nonviable tissue that form crypts where many toxic substances can accumulate if the patient
continues using the drug. The complex of necrotic tissue and harmful substances causes a
mixed acute and chronic inflammatory reaction. Medications such as antibiotics and “light”
debridement will not help in such cases, and meticulous and thorough curettage is needed to
eliminate all of the foci. This surgical step is essential for the tissue to heal, but complete and
definitive withdrawal of the drug is required to avoid relapse.
Page 10
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
The second aspect to consider in the management of CIMDL is reconstruction. Soft and hard
tissues of the nose, maxilla, and the soft and hard palate of cocaine abusers are frequently
destroyed. These anatomical structures are completely lost or left with a complex three-
dimensional deformity in cocaine users. Moreover, the vascularity of the affected areas is
frequently unreliable and therefore local flaps are prone to failure. An integrated
reconstructive protocol will rely on many delicate surgical procedures, which could easily fail
if the patient resumes drug abuse. To ascertain patient motivation to undergo this complex
course of treatment, an 18-month period of drug withdrawal, confirmed by serial urine
analysis, is considered mandatory.15
Comprehensive reconstructive management of CIMDL must address the palatal fistula and the
nasal deformity. In the past, severe hard palate defects were rehabilitated using prosthetic
obturators, with moderate results in term of speech and swallowing. Several disadvantages of
such devices have recently been described, including the lack of stability and retention in
edentulous patients and sensory impairment that leads to problems with mastication,
deglutition, and speech.16
Many surgical techniques have been proposed for reconstruction of nasal and palatal tissues.
However, both local and regional tissue transfer have limitations in cocaine users: oronasal
communication often presents as a wide fistula that cannot be treated with local tissues
(palatal or lingual flap), because of the large size of the fistula and the unreliable results in
terms of flap survival in infected and poorly vascularized donor and recipient beds.
Furthermore, local tissues are often quantitatively unavailable as local flap donors because of
their involvement in drug-induced necrosis.
However, there have been some reports of the successful treatment of small CIMDL palatal
fistulas with palatal or tongue flaps.1,17 The use of temporalis muscle flaps was proposed, but
Page 11
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
cocaine abusers usually present with median palatal defects, which are difficult to reach with
a temporalis muscle flap that requires a very large fenestration through the maxilla.16,18 Even
more complex procedures, such as Le Fort I osteotomy and buccal fat pad flaps, have
occasionally been tried. The validity of such procedures, however, remains to be determined
as only single case reports have been described.19 In 2003, Marshall and colleagues first
described the use of the forearm fasciocutaneous free flap to reconstruct cocaine-related
oronasal fistulas.20 The forearm free flap is a thin versatile flap with a long vascular pedicle
that allows it to reach the cervical region to make use of facial vessels for vascular
anastomosis. Should the facial vessel be inadequate, the length of the pedicle allows switching
to more distant vessels, such as the internal jugular vein and the carotid artery. In patients 1
and 2 in the present study, the facial artery was anastomosed with the radial artery of the flap,
while the facial vein was too small so we used the internal jugular vein to facilitate safe
venous drainage. In patient 3, facial vessels were adequate for microvascular anastomoses.
The use of free flaps in reconstructing CIMDL is particularly suitable because they allow
repair of the defect with abundant reliable well-vascularized soft tissue without tension; in
addition, they yield reliable long-term results. In experienced hands, with a double team
approach, a forearm free flap is not more invasive and does not require more operative time
than harvesting and rotating a temporalis muscle flap.
Cocaine abuse causes severe and extremely complex changes in nasal morphology. The entire
process is initiated by necrosis of the nasal mucosa of the septum. When the cartilage is
exposed, it rapidly becomes necrotic, giving rise to septal perforation. The loss of septal
support causes collapse of the dorsum with a typical resulting saddle nose. The same process
afflicts the entire mucosa, and the areas where this mucosa is thinner are more rapidly
compromised. Immediately after the septum, the area that is injured next corresponds to the
internal valve and to the caudal limit of the nasal bones. These areas with time become
Page 12
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
retracted as a consequence of the loss of internal lining, resulting in cephalic migration of the
tip with columellar exposure. In contrast, the area of the ala cartilage is covered by skin and
thus becomes affected only at the very end of the process. Moreover, the deformity is often
asymmetrical as cocaine abusers usually use their dominant hand to introduce the drug and
thus the detrimental effect accumulates more on that side. As a result, there is a worse
contracture of the nose corresponding to the patient’s dominant side and the entire nose
becomes deviated to that side. Often, there is some columellar retraction that pulls the tip
dorsally.21 Reconstructive rhinoplasty of CIMDL must take all of these aspects of the disease
into account.
The first to consider is the internal lining. Although various procedures have been proposed,
no surgical technique is yet available to reconstruct a sufficiently thin soft tissue envelope for
a new nasal septum. The role of microvascular reconstruction of the nasal septum, which ends
with a bulky mass inside the nasal cavity, is questionable and until new techniques are
discovered such procedures are better avoided.22
However, there have been reports of successful reconstruction of the internal lining using free
flaps.23–26 This is required only where there is an almost complete absence of the internal
lining and it is therefore seldom indicated in CIMDL nasal reconstruction.
On the other hand, despite a single report of excellent results obtained with local flaps from
the remaining internal lining,22 other authors have relied on locoregional flaps, typically an
island melolabial flap, to rebuild the lost mucosa.4 While local flaps have the undoubted
advantage of being very thin and thus do not affect respiration, their vasculature can be
unreliable and therefore the results may not be maintained over the long term. Conversely,
melolabial flaps are bulky and may require additional thinning, but they have superior
Page 13
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
vasculature. In our institute, we have used for the second option for internal lining
reconstruction with rotation of an island melolabial flap.
The other aspect of nasal reconstruction for CIMDL is the skeletal framework. The aim is to
rebuild support for the dorsum, the tip, and the ala, and various different approaches have
been reported. Some authors have used composite free flaps containing skin and cartilage,27
while others have transferred prefabricated composite skin-cartilage flaps.23 Again,
considering the general poor color and texture match of distant flaps, these are a second
choice and should be used only if local tissues are truly unavailable.
The best option for reconstruction of CIMDL nasal defects is an open rhinoplasty approach
where the inner lining is carefully preserved. Any breach must be repaired immediately with
watertight sutures.22 When the entire inner lining has been separated then the outer soft
tissues must be widely freed. The tip must be moved anteriorly and downward, and the
surgeon checks the amount of movement obtained while exerting gentle traction on these
outer soft tissues. If there is any tension, then more soft tissue mobility must be obtained by
undermining in the frontoglabellar region and within the cheeks. When a sufficient degree of
freedom has been obtained in the soft tissues, structural skeletal grafting is required. The rib
is acknowledged as the best donor site for major nasal reconstruction,4,22 but some other
grafts are seldom used, such as calvarial bone.28 The technique of skeletal reconstruction with
costochondral grafts in CIMDL is equivalent to the same procedure used in other
circumstances, such as in posttraumatic defects or even in syphilis or leprosy.4 The quality of
local nasal soft tissues, even if injured by many years of chronic drug abuse, is not an issue
and we have not observed any exposure or infection of the grafts, consistent with other
reports in the literature.4,22
Page 14
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTConclusions
Chronic cocaine abuse may cause a wide range of damage to the soft and hard tissues of the
midface. The aim of acute management is aggressive removal of infected crypts where
injurious substances and bacteria can accumulate. Reconstruction of the affected structures
can be initiated when an 18-month period of drug withdrawal can be confirmed. The palate
and nose are damaged in a very complex way, and the vascularity of remaining local tissues
can be compromised or inadequate to allow for flap harvesting. Palatal and nasal
reconstructions are very delicate, and they should be addressed separately to maximize the
predictability of the result.
Page 15
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
References
1 – Marì A, Arranz C, Gimeno X, Lluch J, Pericot J, Escuder O, Monner A, Piulachs P: Nasal
cocaine abuse and centrofacial destructive process: report of three cases including treatment.
Oral surg Oral Med Oral Pathol Oral Radiol Endod 93(4): 435-9, 2002
2 – Goodger NM, Wang J, Pogrel MA: Palatal and nasal necrosis resulting from cocaine misuse.
Br Dent J 198(6): 333-4, 2005
3 – Messinger E: Narcotic septal perforations due to drug addiction. J Am Med assoc 179: 964,
1962
4 – Millard DR, Mejia FA: Reconstruction of the nose damaged by cocaine. Plast Reconstr Surg
107(2): 419-24, 2001
5 – Brusati R, Carota F, Mortini P, Chiapasco M, Biglioli F: A peculiar case of midface
reconstruction with four free flaps in a cocaine-addicted patient. J Plast Reconstr Aesthet Surg
62(2): e33-40, 2009
6 – Seyer BA, Grist W, Muller S: Aggressive destructive midfacial lesion from cocaine abuse.
Oral surg Oral Med Oral Pathol Oral Radiol Endod 94: 465-70, 2002
7 – Smith JC, Kacker A, Anand VK: Midline nasal and hard palate destruction in cocaine
abusers and cocaine’s roles in rhinologic practice. Ear Nose Throat 81: 172-77, 2002
8 – Schwarz RH, Estroff T, Fairbanks DNF, Hoffman NG: Nasal symptoms associated with
cocaine abuse during adolescence. Arch Otolaryngol Head Neck Surg 115: 63-64, 1989
9 – Owens WD: Signs and symptoms presented by those addicted to cocaine. J.A.M.A. 58: 329,
1912
10 – Colletti G, Allevi F, Valassina D, Bertossi D, Biglioli F: Repair of cocaine-related oronasal
fistula with forearm radial free flap. J Craniofac Surg 24(5): 1734-8, 2013
11 – Becker GD, Hill S: Midline granuloma due to illicit cocaine use. Arch Otolaryngol Head
Neck Surg 114: 90-1, 1988
Page 16
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12 – Trimarchi M, Mortini P: Cocaine-induced midline destructive lesion and Wegener
granulomatosis. Neurosurgery 70(5): E1339, 2012
13 – Trimarchi M, Gregorini G, Facchetti f, Morassi ML, Manfredini C, Maroldi R, Nicolai P,
Russell KA, McDonald TJ, Specks U: Cocaine-induced midline destructive lesions: clinical,
radiographic, histopathologic and serologic features and their differentiation from Wegener
granulomatosis. Medicine (Baltimore) 80(6): 391-404, 2001
14 – Armstrong Jr M, Shikani AH: Nasal septal necrosis mimicking Wegener’s granulomatosis
in cocaine abuser. Ear Nose Throat J 75: 623-27, 1996
15 – Preuss UW, Bahlmann M, Koller G, Soyka M:Treatment of cocaine dependence.
Intoxication, withdrawal and prevention of relapse. Fortschr Neurol Psychiatr 68(5): 224-38,
2000
16 – Di Cosola M, Turco M, Acero J, Navarro-Vila C, Cortelazzi R: Cocaine-related syndrome
and palatal reconstruction: report of a series of cases. Int J Oral Maxillofac Surg 36(8): 721-7,
2007
17 – Posnick JC, Getz SB: Surgical closure of end-stage palatal fistulas using anteriorly-based
dorsal tongue flaps. J Oral Maxillofac Surg 45: 907, 1987
18 – Cordeiro P, Wolfe SA: The temporalis muscle flap revisited on its centennial: advantages,
newer uses and disadvantages. Plast Reconstr Surg 98: 980-87, 1996
19 – Pelo S, Gasparini G, Di Petrillo A, Tassiello S, Longobardi G, Boniello R: Le Fort I
osteotomy and the use of bilateral Bichat bulla adipose flap: an effective new technique for
reconstructing oronasal communications due to cocaine abuse. Ann Plast Surg 60(1): 49-52,
2008
20 – Marshall DM, Amjad I, Wolfe A: Use of the radial forearm flap for deep, central, midfacial
defects. Plast Reconstr Surg 111: 56-64, 2003
Page 17
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21 – Silvestre FJ, Perez-Herbera A, Puente-Sandoval A, Bagan JV: Hard palate perforation in
cocaine abusers: a systematic review. Clin Oral Investig 14(6): 621-8, 2010
22 – Guyuron B, Afrooz PN: Correction of cocaine-related nasal defects. Plast Reconstr Surg
121(3): 1015-23, 2008
23 – Walton RL, Burget GC, Beahm EK: Microsurgical reconstruction of the nasal lining. Plast
Reconstr Surg 115(7): 1813-29, 2005
24 – Menick FJ: Nasal reconstruction. Plast Reconstr Surg 125(4): 138-150, 2010
25 – Menick FJ, Salibian A: Microvascular repair of heminasal, subtotal and total nasal defects
with a folded radial forearm flap and a full-thickness forehead flap. Plast Reconstr Surg
127(2): 637-51, 2011
26 – Menick FJ: Complex nasal reconstruction: a case study: composite defect. Facial Plast
Surg Clin North Am 19(1): 197-211, 2011
27 – Castello JR, Taglialatela Scafati S, Sanchez O: Bilateral nasal ala reconstruction of the
cocaine-injured nose with 2 free reverse-flow helical rim flaps. Ann Plast Surg, Epub ahead of
print, 2013
28 – Shipchandler TZ, Chung BJ, Alam DS: Saddle nose deformity reconstruction with a split
calvarian bone L-shaped strut. Arch Facial Plast Surg 10(5): 305-11, 2008
Page 18
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Legends
Figure 1: Preoperative picture showing a typically foreshortened nose with right deviation:
the patient is right-handed; the tip is underprojected and deepened nasolabial sulci are
evident. Frontal view.
Figure 2: Preoperative three-quarter view of the same patient showing collapse of the nasal
pyramid caused by CIMDL.
Figure 3: Preoperative lateral view of the same patient: the tip is cranially and dorsally
retracted as a result of the collapsed nasal pyramid.
Figure 4: Preoperative worm’s eye view showing an asymmetric nasal deformity
characterized by tip deviation and collapse of the dorsum.
Figure 5: Preoperative picture showing extensive oronasal communication.
Figure 6: Postoperative result: closure of the oronasal communication was obtained with a
partially deepithelialized fasciocutaneous radial free flap.
Figure 7: Frontal view showing the postoperative result obtained with an open rhinoplasty
approach, a costal osteochondral cantilever graft fixed with a Kirschner wire.
Figure 8: A three-quarter view showing the postoperative result of the same patient:
eumorphic nasal pyramid and nasolabial sulci were obtained.
Figure 9: Lateral view of the same patient where a normally projected tip and a 105° naso-
labial angle are detected.
Figure 10: Postoperative worm’s eye view showing a good symmetry of the tip and nasal alae.
Page 19
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 11: Preoperative picture showing a patient with a severe nasal pyramid collapse
following intense cocaine abuse lasting 9 years (lateral view).
Figure 12: Preoperative picture showing a patient with a severe nasal pyramid collapse
following intense cocaine abuse lasting 9 years (three-quarter view).
Figure 13: Preoperative picture showing a wide oronasal communication.
Figure 14: Postoperative picture showing the closure of the oronasal communication obtained
by a partially deepithelialized radial fasciocutaneous free flap.
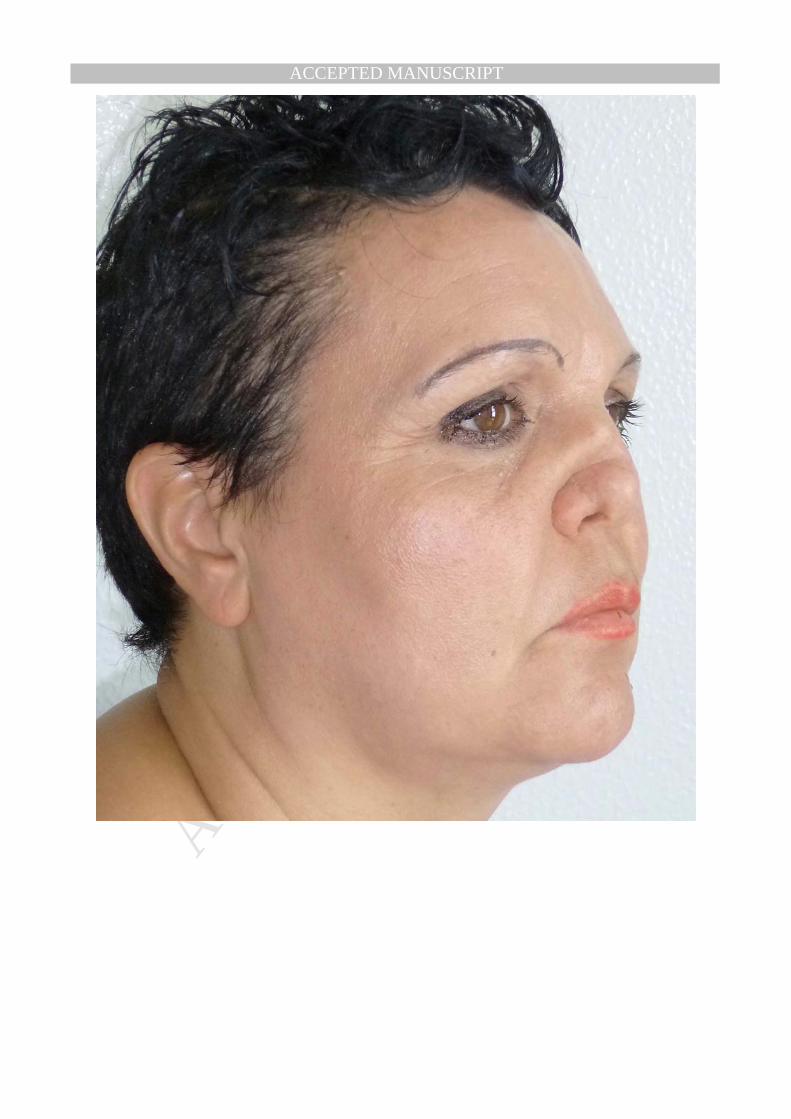
Figure 15: Postoperative picture showing the result obtained after two-step surgery: first, we
freed all of the retractions of the inner lining and reconstructed the resulting defect with an
island melolabial flap; second, a costochondral cantilever graft was placed to reconstruct the
dorsum and the tip (lateral view).
Figure 16: Postoperative three-quarter view of the same patient. A dorsum with good tip
projection and nasolabial angle was obtained.
Figure 17: Frontal view of the fourth patient, affected by acute lesions on the nasal septum,
columella, nostrils, and premaxilla. These areas were characterized by the presence of
granulation tissue and pus. Bone, cartilage, and soft tissue of the nasal septum and lateral
nasal wall were already missing.
Figure 18: Intraoral picture of the fourth patient affected by a wide palatal fistula.
Figure 19: Frontal view of the fourth patient after aggressive debridement: under general
anesthesia all of the areas involved by the process were surgically cleared.
Figure 20: Intraoral picture after aggressive debridement: the resulting severe collapse of the
lower two-thirds of the nose is evident.
Page 20
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 21
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 22
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 23
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 24
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 27
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 28
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 29
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 30
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 31
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 32
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 33
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 34
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 35
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 36
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 37
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 38
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 39
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT