91 Douglas A. Graeb, M.D. William D. Robertson, M.D. Jocelyne S. Lapointe, M.D. Robert A. Nugent, M.D. Philip B. Harrison, M.D. Computed Tomographic Diagnosis of Intraventricular Hemorrhage Etiology and Prognosis1 Sixty-eight patients with intraventricular hemorrhage (IVH) diagnosed by computed tomography (CT) were reviewed retro- spectively to determine the etiology and prognosis, relationship to delayed hydro- cephalus, and effect on neurological out- come. The most common causes were a ruptured aneurysm, trauma, and hyper- tensive hemorrhage. Ruptured aneurysms of the anterior communicating artery can often be predicted from the non- enhanced CT scan. The total mortality rate was 50%; however, 21% of patients returned to normal or had only mild disability. Patients in whom no cause was identified had a better prognosis. Delayed hydrocephalus was related to the effects of subarachnoid hemorrhage rather than obstruction of the ventricular system by blood. IVH per se is seldom a major factor in the neurological outcome. Index terms: Aneurysm, cerebral. 1(71.730 #{149} Brain, hemorrhage #{149} Brain, injuries #{149} Head, computed tomography. 1[0].l211 . Hydrocephalus. 1[6].4372. Subarachnoid space. hemorrhage Radiology 143: 91-96, April 1982 I From the Department of Diagnostic Radiology. Vancouver Ceneral Hospital, Vancouver, B.C., Canada. Received May 7, 1981; accepted and revision requested Aug. 11; revision received Sept. 18. Presented in part at the Forty-third Annual Meeting of the Canadian Association of Radiologists. Montreal, Quebec, Canada, May 11-15, 1980. sjh B EFORE computed tomography (CT), the clinical diagnosis of intraventmiculam hemorrhage (IVH) was usually suggested by sudden coma followed by severe and often fatal brainstem dys- function (1-3). This so-called “classical” presentation was generally associated with massive intraventricular hemorrhage. However, CT frequently demonstrates IVH even when the “classical” clinical picture is absent. Fortunately, although it usually occurs in association with severe brain trauma, even relatively massive IVH may have a good outcome (4) (Fig. 1). While several reports have documented the ability of CT to show IVH (4-7), to our knowledge only one sizable series has been ana- lyzed, namely that of Little et a!. (8) who observed 54 patients of whom only 9 survived. Our experience suggests that the prognosis is somewhat better than these statistics indicate. We have reviewed our own cases to determine the etiology and prognosis and evaluate the mole of IVH in both delayed hydrocephalus and the neurological outcome. MATERIALS AND METHODS Of 77 cases of CT-diagnosed IVH available for study, 9 were dis- carded because of inadequate follow-up, poor scan quality, on because the IVH was postoperative, leaving 68 cases for review. Premature infants were not included. All patients had non-contrast scans on an EM! 1O1OS; contrast- enhanced scans were also obtained in 11 cases. In patients with a ruptured aneurysm, we attempted to locate it on the non-contrast scan, based on the site of hematoma formation. In 29 patients scanned more than once, ventricular size was followed up in order to deter- mine the relationship between subarachnoid and/on intraventriculam bleeding and delayed hydmocephalus, defined as an increase in ventricular size developing at least one week after the initial hem- omrhage. Any increase in size was also correlated with the presence of blood in the third and fourth ventricles and subarachnoid space. IVH was graded according to the amount of blood within each yen- tnicle (TABLE I), with a maximum score of 12: 1-4 was called mild, 5-8 moderate, and 9-12 severe. Outcome was assessed using the Glasgow scale (9), in which pa- tients are assigned to one of five categories: normal or mild disability (I), moderate disability (II), major disability (III), vegetative state (IV), or death (V). Each patient’s clinical record was also reviewed to de- termine the cause of death, on the nature of any residual neurological deficit in the case of survivors. RESULTS Age and sex distributions are shown in Figure 2. Males and females
Transcript
91
Douglas A. Graeb, M.D.
William D. Robertson, M.D.
Jocelyne S. Lapointe, M.D.Robert A. Nugent, M.D.Philip B. Harrison, M.D.
Computed Tomographic Diagnosis
of Intraventricular Hemorrhage
Etiology and Prognosis1
Sixty-eight patients with intraventricularhemorrhage (IVH) diagnosed by computedtomography (CT) were reviewed retro-spectively to determine the etiology andprognosis, relationship to delayed hydro-cephalus, and effect on neurological out-come. The most common causes were aruptured aneurysm, trauma, and hyper-tensive hemorrhage. Ruptured aneurysmsof the anterior communicating arterycan often be predicted from the non-enhanced CT scan. The total mortalityrate was 50%; however, 21% of patientsreturned to normal or had only milddisability. Patients in whom no causewas identified had a better prognosis.Delayed hydrocephalus was related tothe effects of subarachnoid hemorrhagerather than obstruction of the ventricularsystem by blood. IVH per se is seldom amajor factor in the neurological outcome.
Index terms: Aneurysm, cerebral. 1(71.730 #{149}Brain,
Vancouver Ceneral Hospital, Vancouver, B.C., Canada.Received May 7, 1981; accepted and revision requested
Aug. 11; revision received Sept. 18.Presented in part at the Forty-third Annual Meeting
of the Canadian Association of Radiologists. Montreal,Quebec, Canada, May 11-15, 1980. sjh
B EFORE computed tomography (CT), the clinical diagnosis ofintraventmiculam hemorrhage (IVH) was usually suggested by
sudden coma followed by severe and often fatal brainstem dys-function (1-3). This so-called “classical” presentation was generallyassociated with massive intraventricular hemorrhage. However, CTfrequently demonstrates IVH even when the “classical” clinicalpicture is absent. Fortunately, although it usually occurs in association
with severe brain trauma, even relatively massive IVH may havea good outcome (4) (Fig. 1).
While several reports have documented the ability of CT to showIVH (4-7), to our knowledge only one sizable series has been ana-lyzed, namely that of Little et a!. (8) who observed 54 patients of
whom only 9 survived. Our experience suggests that the prognosisis somewhat better than these statistics indicate. We have reviewed
our own cases to determine the etiology and prognosis and evaluatethe mole of IVH in both delayed hydrocephalus and the neurologicaloutcome.
MATERIALS AND METHODS
Of 77 cases of CT-diagnosed IVH available for study, 9 were dis-carded because of inadequate follow-up, poor scan quality, on becausethe IVH was postoperative, leaving 68 cases for review. Prematureinfants were not included.
All patients had non-contrast scans on an EM! 1O1OS; contrast-
enhanced scans were also obtained in 1 1 cases. In patients with aruptured aneurysm, we attempted to locate it on the non-contrast
scan, based on the site of hematoma formation. In 29 patients scannedmore than once, ventricular size was followed up in order to deter-mine the relationship between subarachnoid and/on intraventriculambleeding and delayed hydmocephalus, defined as an increase inventricular size developing at least one week after the initial hem-omrhage. Any increase in size was also correlated with the presenceof blood in the third and fourth ventricles and subarachnoid space.IVH was graded according to the amount of blood within each yen-tnicle (TABLE I), with a maximum score of 12: 1-4 was called mild, 5-8moderate, and 9-12 severe.
Outcome was assessed using the Glasgow scale (9), in which pa-tients are assigned to one of five categories: normal or mild disability
(I), moderate disability (II), major disability (III), vegetative state (IV),or death (V). Each patient’s clinical record was also reviewed to de-termine the cause of death, on the nature of any residual neurologicaldeficit in the case of survivors.
RESULTS
Age and sex distributions are shown in Figure 2. Males and females
Aneurysm
,a _.
I I I
Trauma
�rJf�
Hypertensive
f///kr/i2ffAhemorrhage0 20 40 60 80
Age
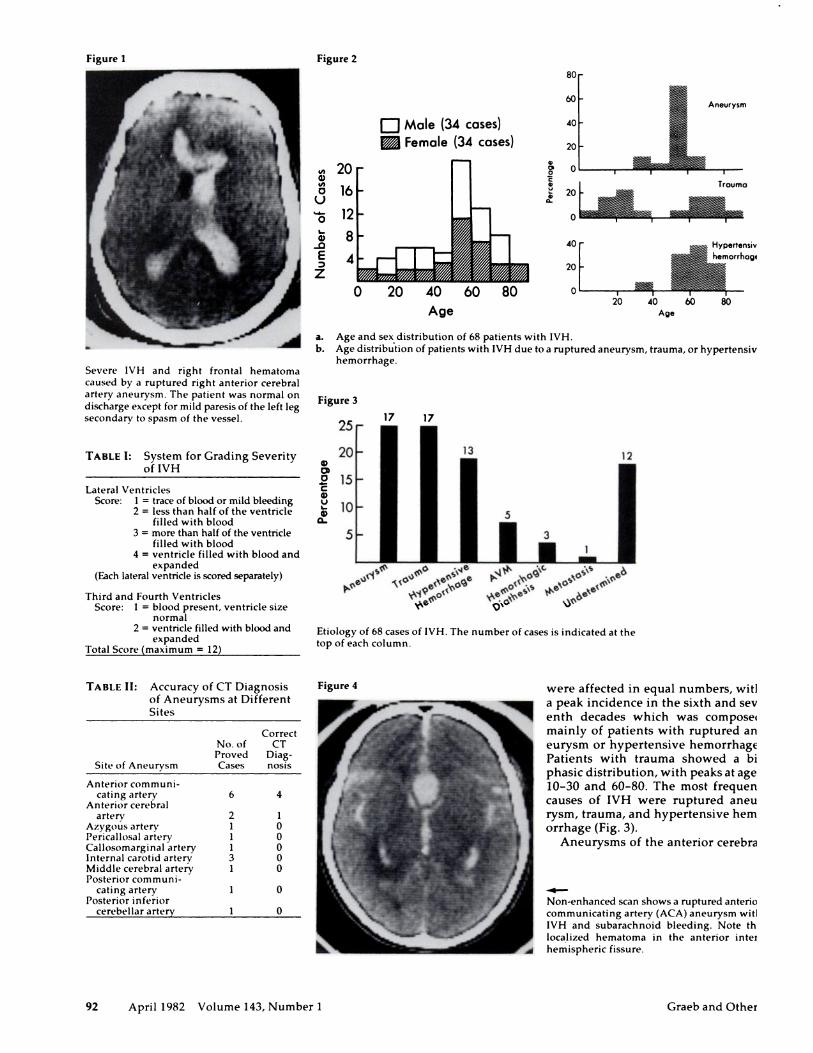
Severe IVH and right frontal hematoma
caused by a ruptured right anterior cerebral
artery aneurysm. The patient was normal on
discharge except for mild paresis of the left leg
secondary to spasm of the vessel.
80
60
U Male (34 cases) 40
� Female (34 cases) 20
20 1 #{176}
16 a� 20
12 0
8 40
4 20
0 I I I I
20 40 60 80Age
a. Age and sexdistribution of 68 patients with IVH.
b. Age distribution of patients with IVH due to a ruptured aneurysm, trauma, or hypertensive
hemorrhage.
Figure 3
25 17 17
13 12
01
0 15Ca)
c�10 5
5 3
‘S
S P’ �
-c 011�n(�O4 I#{231}�5 �t%O�OS �(%‘
- �
Etiology of 68 cases of IVH. The number of cases is indicated at the
top of each column.
Figure 4 were affected in equal numbers, with
a peak incidence in the sixth and sev-enth decades which was composed
mainly of patients with ruptured an-
eurysm on hypertensive hemorrhage.Patients with trauma showed a bi-phasic distribution, with peaks at ages10-30 and 60-80. The most frequentcauses of IVH were ruptured aneu-rysm, trauma, and hypertensive hem-
omrhage (Fig. 3).Aneurysms of the anterior cerebral
Non-enhanced scan shows a ruptured anteriorcommunicating artery (ACA) aneurysm with
IVH and subarachnoid bleeding. Note the
localized hematoma in the anterior inter-
hemispheric fissure.
Figure 1 Figure 2
92 April 1982 Volume 143, Number 1 Graeb and Others
TABLE I: System for Grading Severity
of IVH
Lateral VentriclesScore: 1 = trace of blood or mild bleeding
2 = less than half of the ventriclefilled with blood
3 = more than half of the ventriclefilled with blood
4 = ventricle filled with blood andexpanded
(Each lateral ventricle is scored separately)
Third and Fourth VentriclesScore: 1 = blood present, ventricle size
CT Diagnosis of Intraventnicular Hemorrhage NEURORADIOLOGY 93
Cerebral trauma with severe IVH (Glasgow scores: left ventricle 4; right ventricle 3; third ventricle 2; fourth ventricle 2; total 1 1)., Note the hemorrhage in the subarachnoid space and the soft tissues of the scalp and face. The dilatation of the lateral ventricles is probably
due to intraventricular obstruction of CSF flow.
artery and its branches, including theanterior communicating artery (ACA),
were the most common, constituting 11out of 17 cases (65%) (TABLE II). Onlyruptures involving the ACA could
be predicted, being seen as localizedbleeding in the anterior intenhemi-
spheric fissure, just anterior to the lam-
ma termina!is, in 4 out of 6 cases (Fig.
4).
The diagnosis of trauma was evident
from the history and physical findings
and was confirmed by autopsy in 11
out of 17 patients. Swelling on hemon-
rhage in the extracranial soft tissue was
present in 13 patients (76%). Paren-
chymal hematomas were found in 12
(71%). Additional findings included
ventricular enlargement, midline shift,
subarachnoid hemorrhage, acute sub-
dunal hematoma, cerebral contusion,
skull fracture, and intracranial air (Fig.
5).
Hypertensive hemorrhage, seen in
13 cases, was established by hyperten-
sion �180/100 (mean, 220/120) and a
deep parenchymal hematoma on the
CT scan. In 3 patients, angiographyshowed no aneurysm; 2 patients had
hypertensive hemorrhage at autopsy.
In 7 cases (54%), there was bleedinginto the thalamus or basal ganglia
b (Fig. 6). Three had bleeding into thetemporal lobe, 1 into the frontal lobe,
and 1 into the pons; another patienthad multiple hemorrhages throughout
failed to show the bleeding site, as didautopsy in 1 case. Two patients died
Figure
16
e
a 12I-)
Figure 9
Figure 10
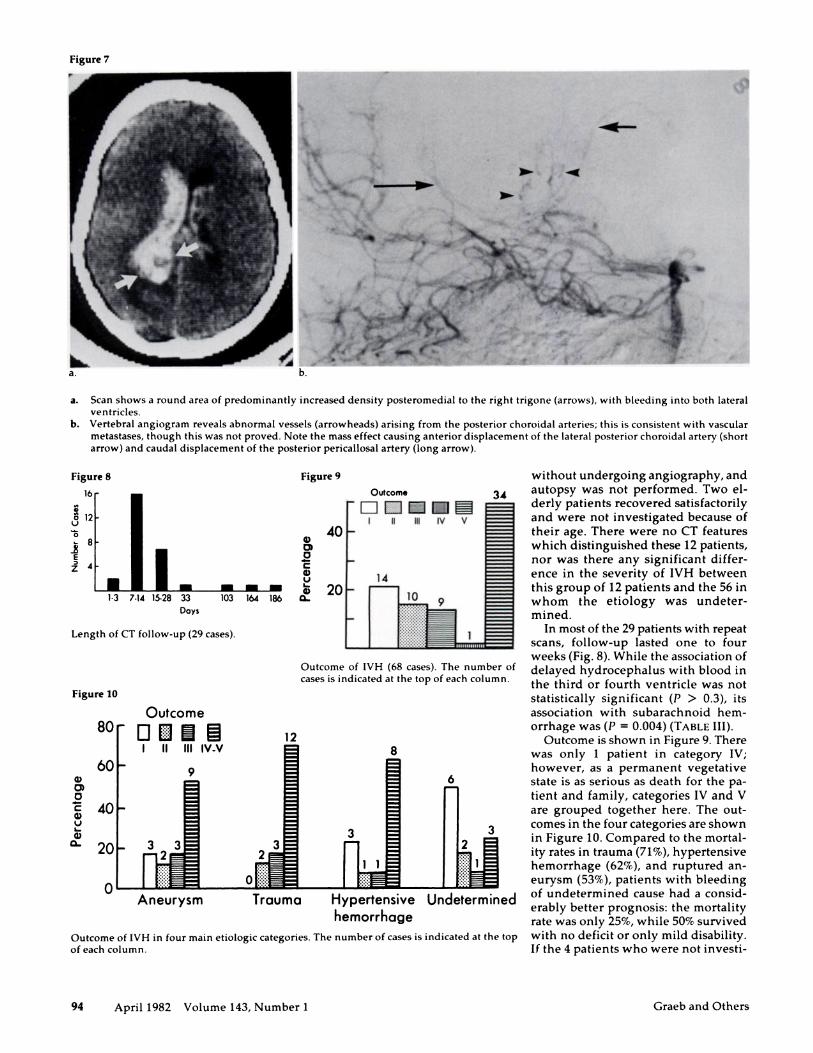
Outcome of IVH (68 cases). The number of
cases is indicated at the top of each column.
a)at0Ca)UI-
a)a-
Outcome of IVH in four main etiologic categories. The number of cases is indicated at the top
of each column.
Figure 7
94 April 1982 Volume 143, Number 1 Graeb and Others
a. b.
a. Scan shows a round area of predominantly increased density posteromedial to the right trigone (arrows), with bleeding into both lateral
ventricles.
b. Vertebral angiogram reveals abnormal vessels (arrowheads) arising from the posterior choroidal arteries; this is consistent with vascular
metastases, though this was not proved. Note the mass effect causing anterior displacement of the lateral posterior choroidal artery (short
arrow) and caudal displacement of the posterior penicallosal artery (long arrow).
1.3 7.14 15.28 33
Days
Length of CT follow-up (29 cases).
Outcome
I II IN IV V
a) 40010Ca)U 14
- - - �5 20103164186 Q� 10
without undergoing angiography, and
34 autopsy was not performed. Two el-derly patients recovered satisfactorilyand were not investigated because oftheir age. There were no CT featureswhich distinguished these 12 patients,nor was there any significant differ-ence in the severity of IVH betweenthis group of 12 patients and the 56 inwhom the etiology was undetem-mined.
In most of the 29 patients with repeatscans, follow-up lasted one to four
weeks (Fig. 8). While the association of
delayed hydrocephalus with blood in
the third on fourth ventricle was notstatistically significant (P > 0.3), its
association with subanachnoid hem-
ornhage was (P 0.004) (TABLE III).Outcome is shown in Figure 9. There
was only 1 patient in category IV;
however, as a permanent vegetativestate is as serious as death for the pa-
tient and family, categories IV and Vare grouped together here. The out-
comes in the four categories are shownin Figure 10. Compared to the mortal-
ity rates in trauma (71%), hypertensive
hemorrhage (62%), and ruptured an-
eurysm (53%), patients with bleeding
of undetermined cause had a consid-enably better prognosis: the mortalityrate was only 25%, while 50% survivedwith no deficit or only mild disability.
If the 4 patients who were not investi-
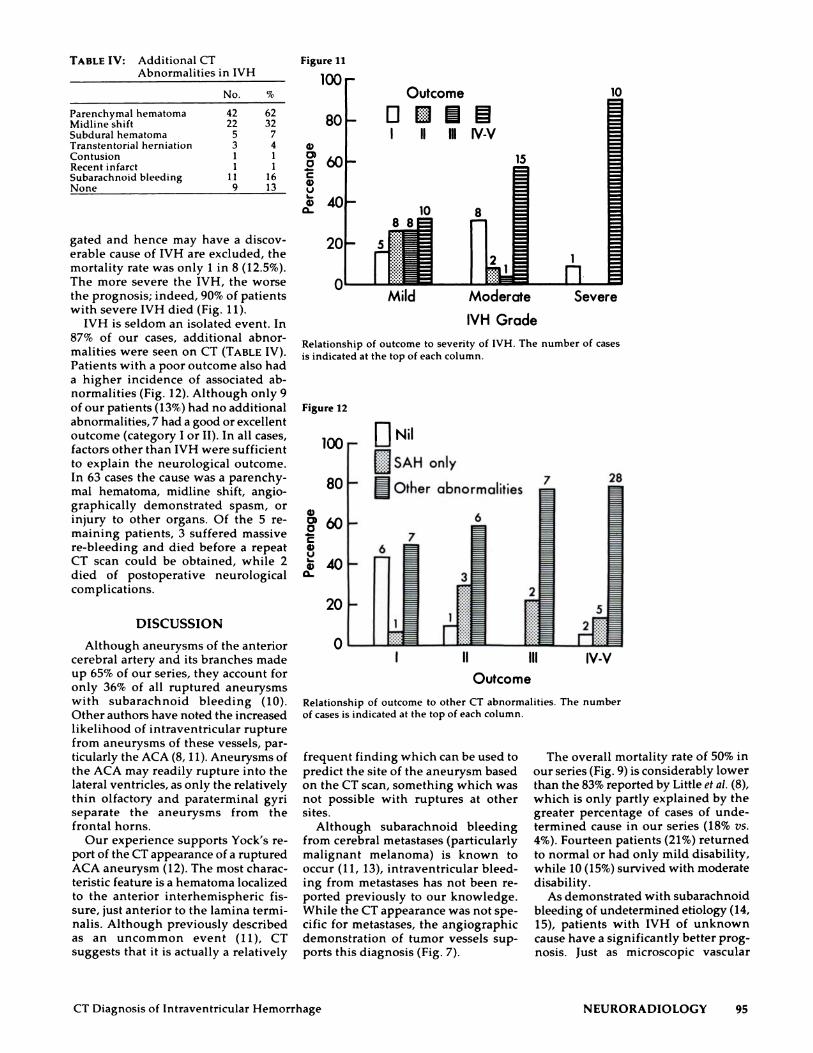
TABLE IV: Additional CT
Abnormalities in IVH
80
Outcome
I II Ill IV-V
IVH Grade
Severe
Figure 11
100
a)at0Ca)Ua)
a-
Relationship of outcome to severity of IVH. The number of cases
is indicated at the top of each column.
Figure 12
100 UNil
��.JSAH only
It �:0 0 Other abnormalities 2 � 2 � 28
I II Ill IV-VOutcome
Relationship of outcome to other CT abnormalities. The number
of cases is indicated at the top of each column.
frequent finding which can be used topredict the site of the aneurysm basedon the CT scan, something which wasnot possible with ruptures at other
sites.Although subarachnoid bleeding
from cerebral metastases (particularlymalignant melanoma) is known tooccur (11, 13), intnaventniculan bleed-ing from metastases has not been re-ported previously to our knowledge.While the CT appearance was not spe-cific for metastases, the angiographicdemonstration of tumor vessels sup-ports this diagnosis (Fig. 7).
CT Diagnosis of Intnaventniculan Hemorrhage NEURORADIOLOGY 95
gated and hence may have a discov-enable cause of IVH are excluded, themortality rate was only 1 in 8 (12.5%).The more severe the IVH, the worse
the prognosis; indeed, 90% of patientswith severe IVH died (Fig. 11).
IVH is seldom an isolated event. In87% of our cases, additional abnor-
malities were seen on CT (TABLE IV).Patients with a poor outcome also hada higher incidence of associated ab-nonmalities (Fig. 12). Although only 9of our patients (13%) had no additionalabnormalities, 7 had a good on excellentoutcome (category I on II). In all cases,factors other than IVH were sufficientto explain the neurological outcome.In 63 cases the cause was a pamenchy-mal hematoma, midline shift, angio-graphically demonstrated spasm, oninjury to other organs. Of the 5 me-maining patients, 3 suffered massivere-bleeding and died before a repeatCT scan could be obtained, while 2died of postoperative neurologicalcomplications.
DISCUSSION
Although aneurysms of the anteriorcerebral artery and its branches made
up 65% of our series, they account foronly 36% of all ruptured aneurysmswith subarachnoid bleeding (10).
Other authors have noted the increasedlikelihood of intraventniculam rupturefrom aneurysms of these vessels, par-ticulanly the ACA (8, 1 1). Aneurysms of
the ACA may readily rupture into thelateral ventricles, as only the relativelythin olfactory and panatenminal gyniseparate the aneurysms from the
frontal horns.Our experience supports Yock’s me-
port of the CT appearance of a rupturedACA aneurysm (12). The most charac-tenistic feature is a hematoma localizedto the anterior interhemisphemic fis-sure, just anterior to the lamina tenmi-nalis. Although previously describedas an uncommon event (11), CT
suggests that it is actually a relatively
The overall mortality rate of 50% inour series (Fig. 9) is considerably lowerthan the 83% reported by Little et a!. (8),
which is only partly explained by thegreater percentage of cases of unde-temmined cause in our series (18% vs.
4%). Fourteen patients (21%) returnedto normal on had only mild disability,while 10 (15%) survived with moderatedisability.
As demonstrated with subamachnoidbleeding of undetermined etiology (14,15), patients with IVH of unknowncause have a significantly better prog-nosis. Just as microscopic vascular
96 April 1982 Volume 143, Number 1 Gnaeb and Others
malformations have been postulated asa cause of subanachnoid bleeding ofundetermined etiology (16), similarmalformations adjacent to the epen-dymal lining of the ventricles may beresponsible for some cases of IVH inwhich no cause is found.
Approximately 50% of our patientshad mild enlargement of the lateralventricles on the initial CT scan. As noprevious scans were available andmany patients were at an age when at-nophy could be expected, this findingwas difficult to interpret; however, anyincrease in ventricular size on subse-quent scans was considered significant.Allcock (17) has stated that develop-ment of hydrocephalus after IVH maybe due to obstruction of the flow of#{231}erebrospinal fluid (CSF) at the foma-men of Monno or aqueduct of Sylvius;although this is likely to be true inacute cases, our study shows that hy-drocephalus which develops at leastone week after IVH can be correlatedwith subarachnoid hemorrhage on theinitial CT scan rather than with IVH inthe third on fourth ventricle. In suchcases, the hydmocephalus is more likelyto be communicating (due to oblitema-tive amachnoiditis in the posterior fossaon impaired resorption of CSF in thearachnoid granulations) than obstruc-tive (18, 19).
The effect of IVH on outcome couldperhaps be assessed most accurately ina prospective fashion by comparisonwith a control group without IVH;however, obtaining an unbiased con-trol group presents a problem in thatthe ultimate severity of brain damageis difficult if not impossible to evaluate
prospectively. Our approach was tocorrelate the clinical record and the CT
scan with outcome in each case. In ourseries, outcome was determined byassociated brain injury rather thanby IVH itself. Factors such as pamenchy-ma! hematoma, midline shift, cerebraledema, and vasospasm had predictableeffects which in each case were suffi-cient to explain the neurological out-come. Patients with IVH and no addi-tiona! CT abnormalities had a muchbetter outcome, and those in whompanenchymal damage was confined to“silent” areas of the brain (such as thefrontal lobes) also did well. Our find-ings indicate that IVH per se is seldom
a major contributor to the neurologicaloutcome in these patients.
As CT is now capable of disclosingIVH in many cases where it could notbe diagnosed clinically, this finding by
itself should not be overemphasized. In
the great majority of cases, the eventualoutcome will be determined by thepresence or absence of associated brainabnormalities. Even severe IVH neednot be cause for a gloomy prognosis
in all cases.
SUMMARY
Sixty-eight patients with CT-diag-nosed IVH were reviewed retrospec-tively. The most frequent causes werea ruptured aneurysm, trauma, and hy-pertensive hemorrhage; less frequentcauses included bleeding from an am-teriovenous malformation, a hemon-rhagic diathesis, on probable metasta-ses. In 12 patients the cause was un-
determined. Ruptured aneurysms ofthe anterior cerebral artery and itsbranches (including the ACA) causedIVH more often than other aneurysmsand could frequently be predicted bytheir appearance on non-enhancedCT scans.
The overall mortality rate was 50%.However, 21% of patients returned tonormal on had only mild disability,while 15% had only moderate disabil-ity. Patients with IVH of undeterminedcause had a much better prognosis.IVH due to cerebral trauma carried thehighest mortality mate (71%) and wouldappear to be an ominous finding. Hy-drocephalus which develops one week
or more after IVH can be correlatedwith subamachnoid bleeding on the CTscan rather than with blood in the thirdor fourth ventricle and is thereforemore likely to be communicating thanobstructive. IVH per se seldom has amajor effect on the neurological out-come.
Department of Diagnostic RadiologyVancouver General Hospital
855 W. 12th Ave.Vancouver, B.C. V5Z 1M9
Canada
References
1. Gordon A. Primary ventricular hemor-rhage. Further contribution to a character-istic symptom group. Arch Neurol Psychi-
ulating tumors of the third ventricle.Neurology 1962; 12:805-809.
3. Ojemann RG, New PFJ. Spontaneous res-
olution of an intraventricular hematoma.Report of a case with recovery. J Neurosurg
1963; 20:899-902.4. Scott WR, New PFJ, Davis KR, Schnur JA.
Computerized axial tomography of intra-cerebral and intraventricular hemorrhage.Radiology 1974; 112:73-80.
5. Jacobs L, Kinkel WR, Heffner RR Jr. Au-topsy correlations of computerized tomog-
raphy: experience with 6,000 CT scans.Neurology 1976; 26:1111-1118.
6. Baker HL Jr. Campbell JK, HouserOW, et al.Computer assisted tomography of the head.An early evaluation. Mayq Clin Proc 1974;
49:17-27.7. Paxton R, Ambrose J. The EM! scanner.
A brief review of the first 650 patients.Br J Radiol 1974; 47:530-565.
8. Little JR. Blomquist GA Jr. Ethier R. Intra-ventricular hemorrhage in adults. Surg
Neurol 1977; 8:143-149.9. Jennett B, Bond H. Assessment of outcome
after severe brain damage. Lancet 1975;1:480-484.
10. Locksley HB. Report on the cooperative
study of intracranial aneurysms and sub-arachnoid hemorrhage. Section V. Part I.
Natural history of subarachnoid hemor-rhage, intracranial aneurysms and arterio-venous malformations. Based on 6368 casesin the cooperative study. J Neurosurg 1966;
25:219-239.11. Heidrich R. Subarachnoid hemorrhage. In:
Vinken PJ, Bruyn GW, eds. Vascular diseases
of the nervous system. Part II. Handbook ofclinical neurology, Vol. 12. New York: El-
sevier, 1972:68-204.12. Yock DH Jr. Larson DA. Computed to-