PATHOLOGICA 2016;108:110-119 REVIEW Computed tomography - histology correlations of unusual lung tumors N. LANDINI 1 , G. MILANESE 2 , E. ZAMBRINI 2 , I. ARIOZZI 2 , L. GNETTI 3 , A. CARLONI 4 , F. NOSENZO 5 , M. SILVA 2 , N. SVERZELLATI 2 1 Department of Experimental and Clinical Biomedical Sciences, Radiology, University of Florence, Italy; 2 Division of Radiology, Department of Surgical Sciences, University of Parma, Italy; 3 Department of Biomedical, Biotechnological, and Translational Sciences (S.Bi.Bi.T.), University of Parma, Italy; 4 Hospital of Terni “Santa Maria”, Radiology, Terni, Italy; 5 Department of Radiology, University of Genova, Italy Key words Pulmonary neoplasms • Computed tomography • Histopathology Summary Correspondence Nicola Sverzellati, Padiglione Barbieri, Azienda Ospedaliero- Universitaria di Parma, via Gramsci 14, 43126 Parma, Italy - Tel. +39 052 1702417 - E-mail: [email protected]A large variety of rare benign and malignant tumors may spo- radically affect the lung. Computed tomography (CT) findings of unusual primary lung tumors are often nonspecific. However, there are some rare pulmonary tumors with imaging features overlapping those of other conditions, thus making radiologic diagnosis chal- lenging. The aim of this review was to correlate CT and histopatho- logical features of a variety of unusual lung tumors to better clarify when and to what extent radiological diagnosis is reliable. Introduction The most unusual primary lung tumors do not generally show specific findings at computed tomography (CT). Indeed, they manifest as nodules, masses, overlapping the CT features of more common forms. However, a number of unusual lung tumors may show some peculiar CT features (e.g. density-texture, high iodinated contrast uptake etc.) that help radiologists suggest the diagnosis firstly. These tumors may have either epithelial or mes- enchymal origin. In addition, there are some rare cystic tumors with CT features that may overlap some intersti- tial non-neoplastic lung disorders. The aim of this review was to match histologic and CT features of the rarest epithelial and mesenchymal tumors to narrow the diagnostic role of CT (Tabs. I-V, Figs. 1, 2). Epithelial tumors of the lung Tumors with airways involvement Because of their typical localization, some rare tumors involving the airways can be promptly recognized at chest CT. Tab. I. Summary of airway-centered neoplasms along with their common CT features. Airways lesions CT typical/common features Tracheobronchial gland tumors Solitary soft tissue nodule or mass with smooth, lobulated or polypoid margins that may demonstrate mild enhancement and punctate calcifications. They are located within segmental bronchi (Mucoepidermoid Carcinoma) or more proximally in distal trachea (with extratracheal component), or lobar bronchi (Adenoid Cystic Carcinoma). Tracheobronchial papillomatosis Multiple, small, confluent, tracheal and endobronchial nodules (preadolescent children); solitary polyploid nodule, typically within the lobar or segmental bronchus (middle-aged adults). Carcinoid Solitary, well-defined,oval or lobulated, 1–3 cm in size,soft tissue nodule. Typical carcinoid are mainly located within the large airways; atypical carcinoids are usually peripheral.Both may show an extraluminal component (e.g. the so-called “iceberg lesions”), high contrast enhancement and calcification.
Transcript
PATHOLOGICA 2016;108:110-119
Review
Computed tomography - histology correlations of unusual lung tumors
N. LANDINI1, G. MILANESE2, E. ZAMBRINI2, I. ARIOZZI2, L. GNETTI3, A. CARLONI4, F. NOSENZO5, M. SILVA2, N. SVERZELLATI2
1 Department of Experimental and Clinical Biomedical Sciences, Radiology, University of Florence, Italy; 2 Division of Radiology, Department of Surgical Sciences, University of Parma, Italy; 3 Department of Biomedical, Biotechnological, and Translational Sciences (S.Bi.Bi.T.), University of Parma, Italy; 4 Hospital of Terni “Santa Maria”, Radiology, Terni, Italy; 5 Department of
A large variety of rare benign and malignant tumors may spo-radically affect the lung. Computed tomography (CT) findings of unusual primary lung tumors are often nonspecific. However, there are some rare pulmonary tumors with imaging features overlapping
those of other conditions, thus making radiologic diagnosis chal-lenging. The aim of this review was to correlate CT and histopatho-logical features of a variety of unusual lung tumors to better clarify when and to what extent radiological diagnosis is reliable.
Introduction
The most unusual primary lung tumors do not generally show specific findings at computed tomography (CT). Indeed, they manifest as nodules, masses, overlapping the CT features of more common forms. However, a number of unusual lung tumors may show some peculiar CT features (e.g. density-texture, high iodinated contrast uptake etc.) that help radiologists suggest the diagnosis firstly. These tumors may have either epithelial or mes-enchymal origin. In addition, there are some rare cystic tumors with CT features that may overlap some intersti-tial non-neoplastic lung disorders.
The aim of this review was to match histologic and CT features of the rarest epithelial and mesenchymal tumors to narrow the diagnostic role of CT (Tabs. I-V, Figs. 1, 2).
Epithelial tumors of the lung
Tumors with airways involvement
Because of their typical localization, some rare tumors involving the airways can be promptly recognized at chest CT.
Tab. I. Summary of airway-centered neoplasms along with their common CT features.
Airways lesions CT typical/common features
Tracheobronchial gland tumors
Solitary soft tissue nodule or mass with smooth, lobulated or polypoid margins that may demonstrate mild enhancement and punctate calcifications. They are located within segmental bronchi (Mucoepidermoid Carcinoma) or more proximally in distal trachea (with extratracheal component), or lobar bronchi (Adenoid Cystic Carcinoma).
Tracheobronchial papillomatosisMultiple, small, confluent, tracheal and endobronchial nodules (preadolescent children); solitary polyploid nodule, typically within the lobar or segmental bronchus (middle-aged adults).
Carcinoid
Solitary, well-defined,oval or lobulated, 1–3 cm in size,soft tissue nodule.Typical carcinoid are mainly located within the large airways; atypical carcinoids are usually peripheral.Both may show an extraluminal component (e.g. the so-called “iceberg lesions”), high contrast enhancement and calcification.
111COMPUTED TOMOGRAPHY - HISTOLOGY CORRELATIONS OF UNUSUAL LUNG TUMORS
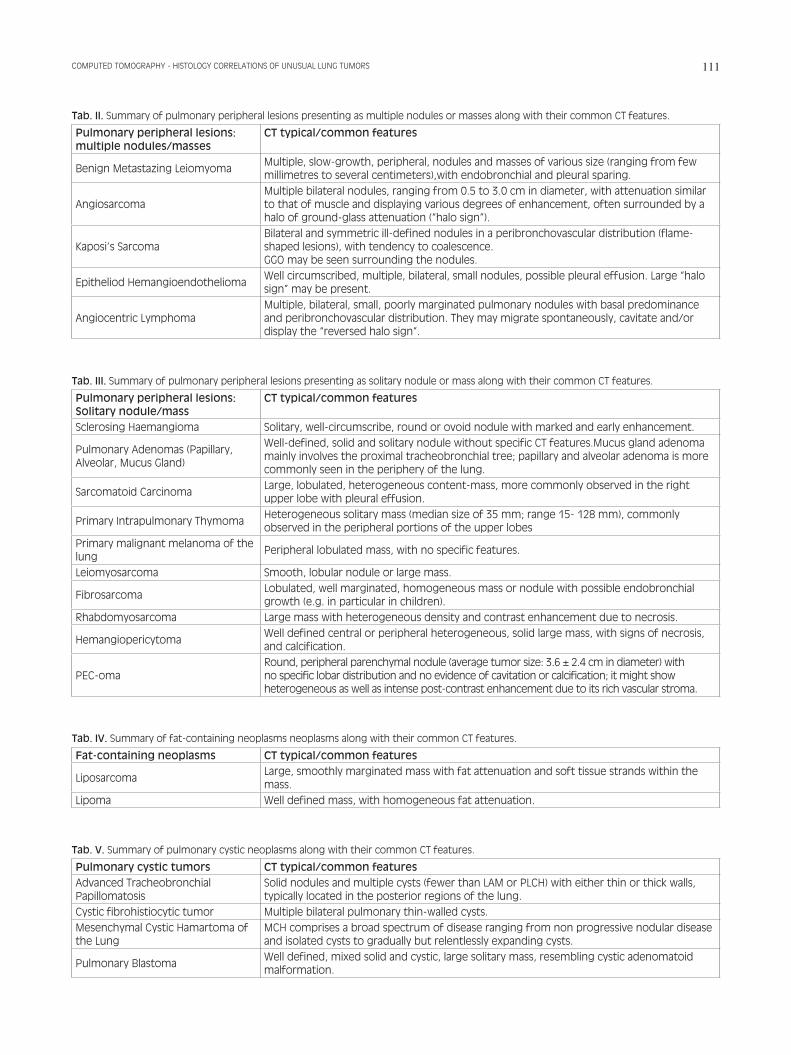
Tab. II. Summary of pulmonary peripheral lesions presenting as multiple nodules or masses along with their common CT features.
Benign Metastazing LeiomyomaMultiple, slow-growth, peripheral, nodules and masses of various size (ranging from few millimetres to several centimeters),with endobronchial and pleural sparing.
AngiosarcomaMultiple bilateral nodules, ranging from 0.5 to 3.0 cm in diameter, with attenuation similar to that of muscle and displaying various degrees of enhancement, often surrounded by a halo of ground-glass attenuation (“halo sign”).
Kaposi’s SarcomaBilateral and symmetric ill-defined nodules in a peribronchovascular distribution (flame-shaped lesions), with tendency to coalescence.GGO may be seen surrounding the nodules.
Epitheliod HemangioendotheliomaWell circumscribed, multiple, bilateral, small nodules, possible pleural effusion. Large “halo sign” may be present.
Angiocentric LymphomaMultiple, bilateral, small, poorly marginated pulmonary nodules with basal predominance and peribronchovascular distribution. They may migrate spontaneously, cavitate and/or display the “reversed halo sign”.
Tab. III. Summary of pulmonary peripheral lesions presenting as solitary nodule or mass along with their common CT features.
Well-defined, solid and solitary nodule without specific CT features.Mucus gland adenoma mainly involves the proximal tracheobronchial tree; papillary and alveolar adenoma is more commonly seen in the periphery of the lung.
Sarcomatoid CarcinomaLarge, lobulated, heterogeneous content-mass, more commonly observed in the right upper lobe with pleural effusion.
Primary Intrapulmonary ThymomaHeterogeneous solitary mass (median size of 35 mm; range 15- 128 mm), commonly observed in the peripheral portions of the upper lobes
Primary malignant melanoma of the lung
Peripheral lobulated mass, with no specific features.
Leiomyosarcoma Smooth, lobular nodule or large mass.
FibrosarcomaLobulated, well marginated, homogeneous mass or nodule with possible endobronchial growth (e.g. in particular in children).
Rhabdomyosarcoma Large mass with heterogeneous density and contrast enhancement due to necrosis.
HemangiopericytomaWell defined central or peripheral heterogeneous, solid large mass, with signs of necrosis, and calcification.
PEC-omaRound, peripheral parenchymal nodule (average tumor size: 3.6 ± 2.4 cm in diameter) with no specific lobar distribution and no evidence of cavitation or calcification; it might show heterogeneous as well as intense post-contrast enhancement due to its rich vascular stroma.
Tab. IV. Summary of fat-containing neoplasms neoplasms along with their common CT features.
Fat-containing neoplasms CT typical/common features
LiposarcomaLarge, smoothly marginated mass with fat attenuation and soft tissue strands within the mass.
Lipoma Well defined mass, with homogeneous fat attenuation.
Tab. V. Summary of pulmonary cystic neoplasms along with their common CT features.
Solid nodules and multiple cysts (fewer than LAM or PLCH) with either thin or thick walls, typically located in the posterior regions of the lung.
Cystic fibrohistiocytic tumor Multiple bilateral pulmonary thin-walled cysts.Mesenchymal Cystic Hamartoma of the Lung
MCH comprises a broad spectrum of disease ranging from non progressive nodular disease and isolated cysts to gradually but relentlessly expanding cysts.
Pulmonary BlastomaWell defined, mixed solid and cystic, large solitary mass, resembling cystic adenomatoid malformation.
N. LANDINI ET AL.112
Tracheobronchial papillomatosisAirways papillomatosis is usually related to Human Pap-illoma Virus (HPV) infection, commonly via vertical transmission during birth. It is characterized by benign lesions in the larynx, trachea and bronchi, with limited lung involvement. It may show an aggressive pattern of growth, producing multiple and extensive endobronchial lesions. Malignant transformation has been described 1.The involvement of lung parenchyma (so called Pul-monary Advanced Papillomatosis) occurs as a severe complication of tracheobronchial papillomatosis in less than 1% of cases. It can develop after many years of latency following the onset of laryngeal disease. Such complication carries a poor prognosis, because of exten-sive parenchymal infiltration. Patients with pulmonary papillomatosis are prone to recurrent infections and suf-fer of an increased risk of development of squamous cell carcinoma 2.
Histologic findingsTracheobronchial papillomatosis is well differentiated at histology without cytological anaplastic features, de-spite his aggressive pattern of growth. Single, regular-layered arrangements of keratin resembling keratotic plugs may be specific 1.
CT findingsTracheal and endobronchial papillomas usually manifest as multiple, small, sessile or pedunculated, nodules protruding into the tracheal lumen. As opposed to other airways tumors, nodules may aggregate in papillomatosis. Sometimes papil-lomas may appear as smooth thickening of airway wall 3. In Pulmonary Advanced Papillomatosis, CT findings usually consist of solid nodules and multiple cysts (few-er than in LAM or PLCH) with thin or thick walls, which often predominate in the posterior regions of the lung. In some cases, large papillomas of the airways may cause post-obstructive atelectasis, or pulmonary infections 4-7. Coexisting or previously documented laryngeal disease may help radiologists suggest the correct diagnosis 2.The lesions of respiratory papillomatosis are well dif-ferentiated at histology, which is reflected on CT by smoothly marginated homogenous nodules, without per-ilesional ground-glass (Figs. 3, 4).
Adenoid cystic carcinomaAdenoid cystic carcinoma (ACCs) is the second com-monest primary tumor of the trachea after squamous cell carcinoma. It is a mucous gland tumor, as well as tracheobronchial mucous gland adenoma and mucoepi-dermoid carcinoma. As it typically grows in central air-ways lumen, ACC may determine signs and symptoms of obstruction, for instance hemoptysis 8.
Histologic findingsThe adenoid cystic carcinoma is composed of small-sized cells with scant cytoplasm and hypercromatic
Fig. 1. Mucoepidermoid carcinoma (high grade): the tumor shows mucus secreting cells, squamous cells and intermediate type cells in a dense lymphoplasmacytic infiltrate.
Fig. 2. Leiomyosarcoma: the lesion shows a fascicular growth pattern with a palisading of spindle cells with eosinophilic fibrillary cytoplasm. Mitotic figures are common.
Fig. 3. Tracheobronchial papillomatosis: the lesion shows a prolifera-tive well-differentiated squamous epithelium overlying fibrovascular cores with koilocytotic change and mild dysplasia.
113COMPUTED TOMOGRAPHY - HISTOLOGY CORRELATIONS OF UNUSUAL LUNG TUMORS
nuclei, showing frequent perineural invasion and infre-quent mitosis.Three different growth patterns are described (i.e. crib-riform, the most characteristic, tubular and solid), which may coexist 9. The differential diagnosis includes car-cinoid tumors, small cell carcinoma and basaloid squa-mous cell carcinoma; those tumors are typically distin-guished by immunohistochemical staining.
CT findingsACC usually grows in the distal tract of the trachea, but can also develop in the lobar bronchi. It appears like an intraluminal mass of soft-tissue attenuation with com-mon extra-tracheal extension, unlike mucoepidermoid carcinoma and mucous gland adenoma that typically grow within the airway. ACC is frequently misdiag-nosed as carcinoid tumors because of its extra-tracheal pattern of growth, however it rarely has calcification and lower contrast enhancement 2 8 (Fig. 5).
CarcinoidCarcinoid tumor derives from neuroendocrine cells of the bronchial mucosa and is classified into two main histologic subtypes: typical (80-90%) and atypical (10-20%) 10 11. Pulmonary carcinoid tumor is rarely hormon-ally active and even more rarely cause ectopic ACTH-dependent Cushing’s syndrome as compared to the car-cinoid tumors from other organs. Main to subsegmental bronchi are the principal location of pulmonary carci-noid (85%), mean age at presentation is 45 years.
Histologic findingsTypical and atypical carcinoids are distinguished by his-tologic features: (a) mitotic activity, (b) cytologic pleo-morphism and nuclear-to-cytoplasmic ratios, (c) tissue cellularity and architectural distorsion, and (d) areas of tumor necrosis. Both categories appear as small nests or interconnect-
ing trabeculae of uniform cells separated by a prominent vascular stroma with thin-walled blood vessels. Typical carcinoid shows less than 2 mitoses per 10 high-power fields (HPFs) (or 2 mm2) of viable tumor, notably with-out areas of necrosis and with high intensity of neurose-cretory granules.Atypical carcinoids show 2-10 mitoses per 10 HPFs (or 2 mm2) and/or foci of necrosis. Cytoplasmatic chromogranin A and synaptophysin, and membrane CD56 are the neuroendocrine hallmark of both typical and atypical carcinoid 12. Peripheral carci-noid can variably express TTF-1, however it is quite un-common and non-specific. Moreover, Ki-67 has minor prognostic value in both categories of carcinoid, and can be used to differentiate between carcinoid (low labeling index < 10-20%) and small cell lung carcinoma (high labeling index > 50%) 13.
CT findingsSolitary, spherical or ovoid solid nodule or mass, with well-defined and slightly lobulated margins is the most common CT appearance of carcinoid, in both subtypes. Atypical carcinoids are usually larger in size than the typical ones (11). Calcifications occur in up to 30% of carcinoids with both diffuse and spotty appearance (11). Rarely, tumors are irregular or ill-defined 11 12 14-17. Both subtypes of carcinoid typically show high contrast enhancement (> 30HU) due to the abundant vascular stroma 11 12 14-17. Endobronchial lesions often display a large extraluminal component, hence carcinoids are also termed ‘iceberg’ lesions. Notably, narrowing or obstruc-tion of the bronchus are frequently observed in associa-tion with atelectasis or obstructive pneumonia 18. Typi-cal carcinoids are often located within the main, lobar, or segmental airways (85%). Conversely, atypical carci-noids are usually peripheral and more commonly associ-ated with adenopathy (40%) (Figs 6, 7).
Fig. 4. Tracheobronchial papillomatosis: the lesion shows a prolifera-tive well-differentiated squamous epithelium overlying fibrovascular cores with koilocytotic change and mild dysplasia.
Fig. 5. Adenoid cystic carcinoma in lung: a solid pattern of microcystic spaces containing mucin is surrounded by small tumor cells; in this specimen there are pseudocyst, intercellular spaces, basal lamina and true glandular lumens.
N. LANDINI ET AL.114
Tumors with parenchymal involvement
Sclerosing hemangiomaSclerosing hemangioma is a rare benign epithelial tu-mor 19 that occurs predominantly in middle-aged wom-en. On CT its diagnosis may be challenging, though it displays some specific features.
Histologic findingsThe name sclerosing hemangioma reflects the pres-ence of sclerosis and dilated vascular spaces, which are deemed secondary changes within the epithelial neo-plasm. The tumor is composed by two cell types (e.g. sur-face cells and round cells) variably assembled into four architectural patterns (e.g. papillary, sclerotic, solid, and hemorrhagic). Both cell types can display moderate to marked nuclear atypia with rare mitoses and scant pleo-morphism, and without necrosis. Immunohistochemical
profile is used to differentiate between the two cell types and to apportion each component. Markers are thereafter reported according to the specific representation:• vimentin, progesterone receptor, estrogen receptor
(rarely, weak) are positive in round cell component;• CK7, CKAE1/3, napsin and surfactant are positive in
surface cells, variable/weak in round cells;• EMA and TTF-1 are positive in both surface and in
synaptophysin, CD34, HMB45, calretinin, HBME1, CK5/6 and WT-1 are negative in both cell types.
More than one architectural pattern coexist in all scle-rosing hemangiomas, with the papillary, sclerotic, and solid ones being the most frequent 19.
CT findingsSolitary rounded or ovoid solid nodule is the most fre-quent CT finding of sclerosing haemangioma 20-22. It is usually located in the peripheral parenchyma, especially in a subpleural location, with slight predominance for the right lung. Bilateral multiple lesions have also been reported, though less common 20-22. The entity and pattern of contrast enhancement depends on the proportion of each histological component. No-tably, vascular component is associated with early overt enhancement.In a recent study, four main features of the tumor were described 23, as follows:• “marginal pseudocapsule” sign (50%) due to the fo-
cal compressed parenchyma next to tumor;• “overlying vessel” sign (26.3%) related to small
feeding or draining vessel adjacent to the tumor or even displaced by the mass effect, also described like a tumor ‘tail-like’ projection 23;
• “air-gap” sign (2.6%) caused by the proliferation and hyaline degeneration of undifferentiated alveolar mesenchymal cells around the bronchus. Such archi-tectural abnormality causes the expansion of the far-end edge of the airway with associated on set of air gap. Such finding can mimic the air crescent sign, which is more commonly related to mycetoma;
• “halo” sign (17.1%) is caused by the shrinkage of the coating membrane and the tumor. The shrinkage typically happens with different timing between the two components and is associated with bleeding and seen on CT as GGO.
Soft tissue and mesothelial tumors
Fat-containing tumorsThe identification of fat density tissue within a pulmo-nary lesion is probably the most reliable CT feature to narrow the differential diagnosis 2. Fat-containing lesions maybe either intra-parenchymal or endobron-chial.
Fig. 6. Typical carcinoid: HRCT showing a sharply demarked round nodule located in the airway lumen of a sub-segmental bronchus of the left upper lobe (white arrow).
Fig. 7. Atypical carcinoid. CT obtained before (A) and after (B) contrast media injection, showing intense contrast enhancement.
115COMPUTED TOMOGRAPHY - HISTOLOGY CORRELATIONS OF UNUSUAL LUNG TUMORS
LiposarcomaPrimary liposarcoma of the lung is one of the rarest va-rieties among lung sarcomas 24 25. Histologic findingsThoracic liposarcoma shows the same histological fea-tures seen in other districts, with lipoblasts characterized by malignant features such as nuclear pleomorphism and signs of neoangiogenesis 26.
CT findingsLiposarcoma usually appears as a large, smoothly margin-ated, heterogeneous mass of fat attenuation. It should be dif-ferentiated from other fat-containing lesions such as pulmo-nary lipoma, hamartoma, and exogenous lipoid pneumonia
27-30. The presence of soft tissue strands in a fat containing mass should suggest the possibility of liposarcoma.However, there are other entities with a fat attenuation component. Coexisting “popcorn” calcification within an intrapulmonary nodule is virtually diagnostic of ham-artoma, especially in lesions less than 2.5 cm in diam-eter 31-35. Bilateral consolidations with fat attenuation, predominantly in the lower lobes, in patients with his-tory of aspiration of oily-substances are the CT features of lipoid pneumonia (Figs. 8, 9) 36.
LipomaLipoma is extremely rare in the lung, despite it is the most common benign neoplasms. In most of these cas-es, it originates in the trachea or mainstem bronchi 37.
Histologic findingsLipomas consist of well-circumscribed, yellowish nod-ules composed of mature adipose cells, indistinguish-able from normal fat.
CT findingsPulmonary lipoma appears as a well defined, fat attenu-ation mass (about -100 HU).
Intrapulmonary lesions are surrounded by aerated lung tissue. Intrabronchial neoplasm may be peduncolat-ed 38 39. The lack of nodules or of tissue strands in a predominant fatty lesion is highly indicative of pulmonary lipoma.
Mesenchimal tumors of myomatous origin
Benign metastazing leiomyomaBenign metastazing leiomyoma (BML) of the lung ex-clusively occurs in middle-aged women with history of benign uterine leiomyoma. It is hypothesized that hema-togenous spread of tumor cells is aused by surgical ma-nipulation of the uterus. However, BML is a rare condi-tion despite the high prevalence of uterine leiomyomas treated by hysterectomy 40.
Histologic findingsHistologic examination reveals connected fascicles of smooth muscle cells without anaplasia or vascular inva-sion, with entrapped respiratory epithelium or cysts. Uniform, bland and cohesive spindle cells, without signs of mitosis are organized in clusters, however the cyto-logic pattern of the lesion is non-specific and without atypia or necrosis. The low Ki-67 index (< 5%) and the absence of high cellularity support the low proliferative state, consistent with a benign lesion. Positive immuno-histochemical markers such as desmin, smooth muscle actin, and caldesmin confirm the mesenchymal deriva-tion 41. The presence of estrogen and progesterone receptors suggests the derivation from the female genital tract 42.
CT findingsBenign metastatizing leiomyoma appears as multiple, slow-growth, non calcified, peripheral, nodules and masses (ranging from few millimeters to several cen-timeters), with endobronchial and pleural sparing. As compared to lung metastases from other tumors, benign
Fig. 8. Well differentiated liposarcoma with abrupt transition to dedif-ferentiated (high grade) morphology.
Fig. 9. Well differentiated liposarcoma with abrupt transition to dedif-ferentiated (high grade) morphology.
N. LANDINI ET AL.116
metastatizing leiomyoma does not show contrast en-hancement. Cavitation of the nodule or mass, and con-sequent pneumothorax have also been described on CT, but extremely uncommon 43-45. In patients with an history of surgical manipulation of the uterus and CT findings of heterogenous lesion with central necrosis, radiologists may suggest the degen-eration toward leyomiosarcomatous tissue; in such case scenario, a further histologic examination is recom-mended (Figs. 10, 11).
Mesenchimal tumors of vascular origin
AngiosarcomaMalignant vascular tumors represent less than 2% of all sarcomas. Metastases from primary angiosarcoma of heart, pulmonary arterial trunk, and extrathoracic (tegument, liver and breast) are relatively more fre-quent than primary pulmonary angiosarcoma 46 47. Primary angiosarcoma usually occurs in middle-aged adults and can be suspected in relation with hemop-tysis, usually prolonged, without response to therapy, variably associated with chest pain and cough. It usu-ally presents with multiple foci, but solitary primary pulmonary angiosarcoma has also been reported 48.
Histologic findingsPrimary pulmonary angiosarcoma shows similar fea-tures of angiosarcoma in other sites.Intra-arterial and periarteriolar involvement as well as extensive recent and old hemorrhage suggest primary pulmonary angiosarcoma in spite of metastatic lesions. Positive immunohistochemical stains for CD31, ERG or CD34 (not specific) confirm vascular origin of tumors. The differential diagnosis of angiosarcoma include Ka-posi’s sarcoma, diffuse pulmonary lymphangioleyo-miomatosis, pulmonary capillary hemangiomatosis, metastatic artery sarcoma and primary and metastatic spindle cell carcinoma 49.
Kaposi sarcoma showed nuclear staining for HHV-8, whereas the cases of angiosarcoma and benign vascular lesions were negative for HHV-8.
CT findingsMultiple solid nodules or masses (5-30 mm in diameter), with density similar to that of muscle are the most com-mon CT finding along with variable degrees of enhance-ment. The tumor frequently spreads through the thorax with invasion of the mediastinum and chest wall 47. Both pleural and pericardial effusion may be present. Local invasion and erosion of bronchi associated with alveolar perilesional hemorrhage have been described. Indeed, characteristic CT appearance of angiosarcoma consists of a central area of soft tissue attenuation surrounded by a halo of ground-glass attenuation (“halo sign”). Note-worthy, the “halo sign” is a quite aspecific finding on CT because it is quite common in infectious abnormali-ties such as angioinvasive aspergillosis, tuberculoma associated with hemoptysis, candidiasis, and infections from cytomegalovirus, herpes simplex virus, or coc-cidioidomycosis. Non-infectious causes of the halo sign include granulomatosis with polyangiitis and Kaposi’s sarcoma 2 46-48.
Cystic lung tumors
Lung cysts in the adult population can be detected in a wide variety of diseases including idiopathic prolifera-tive disorders and tumors 4 50. Lung cysts commonly appear on chest CT as round parenchymal lucencies surrounded by a thin wall (< 2 mm) 51. Primary cystic tumors are very uncommon, with those of mesenchymal origin being the most common type. However, non-mesenchymal tumors have been de-scribed in association with cystic CT pattern. Notably, multiloculated cysts may be seen in lepidic adenocar-
Fig. 10. Benign metastazing leiomyoma: bilateral, multiple nodules of various size.
Fig. 11. Benign metastazing leiomyoma: Leiomuscolar well-differen-tiated proliferation with interstitial growth. The specimen does not show signs of cytologic atypia, necrosis, significant mitotic activity or atypical mitosis.
117COMPUTED TOMOGRAPHY - HISTOLOGY CORRELATIONS OF UNUSUAL LUNG TUMORS
cinoma 52 53. The differential diagnosis of cystic tumors includes non-neoplastic disease associated with cys-tic lesions of the lung, such as pulmonary Langerhans cell histiocytosis (PLCH), lymphangioleiomyomatosis (LAM), lymphoid interstitial pneumonia (LIP), infec-tious pneumatoceles (Pneumococcus, Escherichia Coli, Klebsiella, Staphylococcus and Pneumocystis), coc-cidiomycosis, hydatid disease, immunologic disorders (granulomatosis with polyangiitis and rheumatoid nod-ules) and congenital pulmonary airway malformation 4. Multiple thin-walled cystic lesions, referred as “cheerios in the lung” pattern, can be seen in metastatic involve-ment of the lung from a variety of extrapulmonary ma-lignancies.Extrathoracic mesenchymal tumors (e.g. sarcomas, squamous cell cancer, transitional cell carcinoma of the bladder, and melanoma) and gastro-intestinal or genito-urinary adenocarcinomas are more frequently associated with cystic pattern. Cystic metastases may appear het-erogeneous in size with basal predominance 50. The diagnosis is hardly based on the sole imaging be-cause similar features overlap in different diseases. Therefore demographic data (i.e. age) are helpful to nar-row the differential diagnosis 54.
Pulmonary blastomaPulmonary blastoma often occurs at an early stage, with a median age of 2 years at presentation. It accounts for 0.25-0.5% of primary lung malignancies.
Histologic findingsGrossly the lesion is peripheral, solitary, well circum-scribed and large.Histological specimen usually shows early embryologi-cal lung features from immature malignant epithelial and mesenchymal tissues 55 56.
CT findingsOn CT scans, pulmonary blastoma appears as an het-erogeneous mass with combined solid and cystic com-ponents. The mass size is generally large (from 15 mm up to over 10 cm). Furthermore, an heterogeneous en-hancement of the solid component is seen after contrast agent injection 56 57. Pleural effusion has been reported as the sole finding in the most atypical cases (i.e. with undetectable lung lesion) 57. Pulmonary blastoma may also manifest as a branching opacity with a “gloved fin-ger” appearance, thus mimicking fungal infection 58 59. Pulmonary blastoma of the childhood may be seen in association with pre-existing benign cystic lesion, nota-bly, cystic adenomatoid malformation and bronchogenic cyst of the lung. Complete opacification of one hemitho-rax with mediastinal shift is a possible manifestation of the pediatric variant 60 61.
Pulmonary mesenchimal cystic hamartoma (MCH)Pulmonary mesenchimal cystic hamartoma is an ex-tremely rare subtype of pulmonary hamartoma 62.
Histologic findingsMCH is hystologically characterized by parenchymal nodules of primitive mesenchymal cells that gradually increase in size and then become cystic.
CT findingsTypical CT findings of MCH include multiple cysts that may be associated with pulmonary nodules, both are extremely variable in size (1-10 cm). The cysts and/or nodules can slowly increase in size and number over time 54 63.
Cystic fibrohistiocytic tumorCystic fibrohistiocytic tumor is an exceptionally rare neoplasm, which is usually caused by metastatic lo-calization from a benign or low-grade cellular fibrous histiocytoma of the skin. Nevertheless, primary localiza-tions have been described, too.
Histologic findingsThin-walled cystic airspaces delimited by cuboidal epi-thelium with underlying layer of mildly pleomorphic spindle cells and inflammatory cells are the usual pre-sentation of this rare tumor 64.
CT findingsBilateral solid nodules and masses with cavitation into cystic lesions are the typical CT findings of both the pri-
mary and secondary involvement (Fig. 12).
Tumors associated with congenital cystic adenomatoid malformation (CCAM)Congenital cystic adenomatoid malformations have been recently considered as part of congenital pulmo-nary airway malformation (CPAM).CCAM is a congenital developmental deformity that oc-curs in newborn and small children, with variable prog-nosis according to the subtype of malformation.
The five types of the Stocker classification describe the af-fected portion of the airway, the diameter of the cysts and the epithelial changes, reflecting the different CT findings that may be shown, like large cysts (3-10 cm) for type 1 and very small cysts (< 0.2 cm) for type 3 (Fig. 13) 65.
Pulmonary advanced papillomatosis
Pulmonary advanced papillomatosis is a rare complica-tion of tracheobronchial papillomatosis (less than 1% of cases), with extensive parenchymal involvement.It is associated with poor prognosis, recurrent infections, and increased risk of squamous cell carcinoma 2.In patients with solid nodules and multiple cysts (fewer than in LAM or PLCH) with thin or thick walls in the posterior regions of the lung, a known history of tracheo-bronchial papillomatosis may suggest the diagnosis.
Conclusions
Unusual lung tumors represent a broad range of histologi-cal types that have a large spectrum of CT features. These tumors cannot usually be distinguished from the more common primary lung malignancies, nevertheless, the combination of CT findings such as the tracheobronchial location, the presence of fat and the pattern of enhance-ment after injection of contrast agent can occasionally suggest a specific diagnosis of an unusual lung tumor.
References
1 Weingarten J. Cytologic and histologic findings in a case of tra-cheobronchial papillomatosis. Acta Cytologica 1981;25:167-70.
2 Bhatia K, Ellis S. Unusual lung tumours: an illustrated review of CT features suggestive of this diagnosis. Cancer Imaging 2006;6:72-82.
3 Jamjoom L, Obusez EC, Kirsch J, et al. Computed tomography correlation of airway disease with bronchoscopy-part II: tracheal neoplasms. Curr Probl Diagn Radiol 2014;43:278-84.
4 Cantin L, Bankier AA, Eisenberg RL. Multiple cystlike lung le-sions in the adult. AJR Am J Roentgenol 2010;194:W1-W11.
5 Basheda SG, Mehta AC, De Boer G, et al. Endobronchial and pa-renchymal juvenile laryngotracheobronchial papillomatosis. Ef-fect of photodynamic therapy. Chest 1991;100:1458-61.
6 Smith L, Gooding CA. Pulmonary involvement in laryngeal papil-lomatosis. Pediatr Radiol 1974;2:161-6.
7 Lui D, Kumar A, Aggarwal S, et al. CT findings of malignant change in recurrent respiratory papillomatosis. J Comput Assist Tomogr 1995;19:804-7.
8 Kwak SH, Lee KS, Chung MJ, et al. Adenoid cystic carcinoma of the airways: helical CT and histopathologic correlation. AJR Am J Roentgenol 2004;183:277-81.
9 Ernst A, Cagle PT, Allen TC, et al. Adenoid Cystic Carcinoma. In: Fraire AE, Cagle PT, Irwin RS, eds. Atlas of Neoplastic Pulmonary Disease. New York: Springer 2010, pp. 43-45.
10 Travis WD, Linnoila RI, Tsokos MG, et al. Neuroendocrine tumors of the lung with proposed criteria for large-cell neuro-endocrine carcinoma. An ultrastructural, immunohistochemi-cal, and flow cytometric study of 35 cases. Am J Surg Pathol 1991;15:529-53.
11 Rosado de Christenson ML, Abbott GF, Kirejczyk WM, et al. Tho-racic carcinoids: radiologic-pathologic correlation. Radiograph-ics 1999;19:707-36.
12 Chong S, Lee KS, Chung MJ, et al. Neuroendocrine tumors of the lung: clinical, pathologic, and imaging findings. Radiographics 2006;26:41-57.
13 Pelosi G, Rindi G, Travis WD, et al. Ki-67 antigen in lung neuro-endocrine tumors: unraveling a role in clinical practice. J Thorac Oncol 2014;9:273-84.
14 Yi CA, Lee KS, Kim EA, et al. Solitary pulmonary nodules: dy-namic enhanced multi-detector row CT study and comparison with vascular endothelial growth factor and microvessel density. Radi-ology 2004;233:191-9.
15 Koo CW, Baliff JP, Torigian DA, et al. Spectrum of pulmonary neuroendocrine cell proliferation: diffuse idiopathic pulmonary neuroendocrine cell hyperplasia, tumorlet, and carcinoids. AJR Am J Roentgenol 2010;195:661-8.
16 Arrigoni MG, Woolner LB, Bernatz PE. Atypical carcinoid tumors of the lung. J Thorac Cardiovasc Surg 1972;64:413-21.
17 Jeung MY, Gasser B, Gangi A, et al. Bronchial carcinoid tumors of the thorax: spectrum of radiologic findings. Radiographics 2002;22:351-65.
18 Meisinger QC, Klein JS, Butnor KJ, et al. CT features of pe-ripheral pulmonary carcinoid tumors. AJR Am J Roentgenol 2011;197:1073-80.
19 Keylock JB, Galvin JR, Franks TJ. Sclerosing hemangioma of the lung. Arch Pathol Lab Med 2009;133:820-5.
20 Im JG, Kim WH, Han MC, et al. Sclerosing hemangiomas of the lung and interlobar fissures: CT findings. J Comput Assist Tomogr 1994;18:34-8.
21 Neuman J, Rosioreanu A, Schuss A, et al. Radiology-pathology conference: sclerosing hemangioma of the lung. Clin Imaging 2006;30:409-12.
22 Khoury JD, Shephard MN, Moran CA. Cystic sclerosing haeman-gioma of the lung. Histopathology 2003;43:239-43.
23 Shin SY, Kim MY, Oh SY, et al. Pulmonary sclerosing pneumocy-toma of the lung: CT characteristics in a large series of a tertiary referral center. Medicine 2015;94:e498.
24 Lee KH, Song KS, Kwon Y, et al. Mesenchymal tumours of
Fig. 13. HRCT of a Patients with type 1 CCAM showing a large cysts with air-fluid level; coexists a lepidic growing tumor.
119COMPUTED TOMOGRAPHY - HISTOLOGY CORRELATIONS OF UNUSUAL LUNG TUMORS
the thorax: CT findings and pathological features. Clin Radiol 2003;58:934-44.
25 Sawamura K, Hashimoto T, Nanjo S, et al. Primary liposarcoma of the lung: report of a case. J Surg Oncol 1982;19:243-6.
26 John R, Goldblum SWW, Folpe AL. Enzinger and Weiss’s Soft Tissue Tumors. Saunders 2014, pp. 484-523.
27 Krygier G, Amado A, Salisbury S, et al. Primary lung liposar-coma. Lung Cancer 1997;17:271-5.
28 Ruiz-Palomo F, Calleja JL, Fogue L. Primary liposarcoma of the lung in a young woman. Thorax 1990;45:298-9.
29 Ibe T, Otani Y, Shimizu K, et al. Pulmonary pleomorphic liposar-coma. TJpn J Thorac Cardiovasc Surg 2005;53:443-7.
30 Achir A, Ouadnouni Y, Smahi M, et al. Primary pulmonary lipo-sarcoma-a case report. Thorac Cardiovasc Surg 2009;57:119-20.
31 van den Bosch JM, Wagenaar SS, Corrin B, et al. Mesenchymoma of the lung (so called hamartoma): a review of 154 parenchymal and endobronchial cases. Thorax 1987;42:790-3.
32 Poirier TJ, Van Ordstrand HS. Pulmonary chondromatous ham-artomas. Report of seventeen cases and review of the literature. Chest 1971;59:50-5.
33 Darke CS, Day P, Grainger RG, et al. The bronchial circulation in a case of giant hamartoma of the lung. Br J Radiol 1972;45:147-50.
35 Tomashefski JF. Benign endobronchial mesenchymal tumors: their relationship to parenchymal pulmonary hamartomas. Am J Surg Pathol 1982;6:531-40.
36 Gaerte SC, Meyer CA, Winer-Muram HT, et al. Fat-containing lesions of the chest. Radiographics 2002;22 Spec No:S61-78.
37 Politis J, Funahashi A, Gehlsen JA, et al. Intrathoracic lipomas. Re-port of three cases and review of the literature with emphasis on endobronchial lipoma. TJ Thorac Cardiovasc Surg 1979;77:550-56.
38 Baris YI, Kalyoncu AF, Aydiner A, et al. Intrathoracic lipomas demonstrated by computed tomography. Respiration 1990;57:77-80.
39 Kuhlman JE, Bouchardy L, Fishman EK, et al. CT and MR imaging evaluation of chest wall disorders. Radiographics 1994;14:571-95.
40 Takemura G, Takatsu Y, Kaitani K, et al. Metastasizing uterine leiomyoma. A case with cardiac and pulmonary metastasis. Pa-thology Res Prac 1996;192:622-9;discussion 30-3.
41 Chen S, Liu RM, Li T. Pulmonary benign metastasizing leiomyoma: a case report and literature review. J Thorac Dis 2014;6:E92-8.
42 Ki EY, Hwang SJ, Lee KH, et al. Benign metastasizing leiomyoma of the lung. World J Surg Oncol 2013;11:279.
43 Shin MS, Fulmer JD, Ho KJ. Unusual computed tomographic man-ifestations of benign metastasizing leiomyomas as cavitary nodu-lar lesions or interstitial lung disease. Clin Imaging 1996;20:45-9.
44 Osadchy A, Zehavi T, Zissin R. Pulmonary benign metastasising leiomyomas presenting as fluid-containing masses on CT in a pa-tient with two unrelated malignancies. Br J Radiol 2005;78:639-41.
45 Maredia R, Snyder BJ, Harvey LA, et al. Benign metastasizing leiomyoma in the lung. Radiographics 1998;18:779-82.
46 Patel AM, Ryu JH. Angiosarcoma in the lung. Chest 1993;103:1531-5.47 Kojima K, Okamoto I, Ushijima S, et al. Successful treatment of
primary pulmonary angiosarcoma. Chest 2003;124:2397-400.48 Suster S. Primary sarcomas of the lung. Semin Diagn Pathol
1995;12:140-57.49 Pandit SA, Fiedler PN, Westcott JL. Primary angiosarcoma of the
lung. Ann Diagn Pathol 2005;9:302-4.50 Ryu JH, Swensen SJ. Cystic and cavitary lung diseases: focal and
diffuse. Mayo Clin Proc 2003;78:744-52.51 Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society:
glossary of terms for thoracic imaging. Radiology 2008;246:697-722.52 Prichard MG, Brown PJ, Sterrett GF. Bronchioloalveolar carci-
noma arising in longstanding lung cysts. Thorax 1984;39:545-9.53 Yoshida T, Harada T, Fuke S, et al. Lung adenocarcinoma present-
ing with enlarged and multiloculated cystic lesions over 2 years. Respir Care 2004;49:1522-4.
54 Zhu H, Huang S, Zhou X. Mesenchymal cystic hamartoma of the lung. Ann Thorac Surg 2012;93:e145-7.
55 Larsen H, Sorensen JB. Pulmonary blastoma: a review with spe-cial emphasis on prognosis and treatment. Cancer Treat Rev 1996;22:145-60.
56 Ohara N, Tominaga O, Oka T, et al. Pulmonary blastoma: report of a case. Surg Today 1999;29:385-8.
57 Walker RI, Suvarna K, Matthews S. Case report: pulmonary blas-toma: presentation of two atypical cases and review of the litera-ture. Br J Radiol 2005;78:437-40.
58 Wang J, Sun H, Bai R, et al. Pulmonary blastoma with endobron-chial growth. J Thorac Oncol 2009;4:543-4.
59 Lee HJ, Goo JM, Kim KW, et al. Pulmonary blastoma: radiologic findings in five patients. Clin Imaging 2004;28:113-8.
60 Dehner LP. Pleuropulmonary blastoma is THE pulmonary blas-toma of childhood. Semin Diagn Pathol 1994;11:144-51.
61 Senac MO, Wood BP, Isaacs H, et al. Pulmonary blastoma: a rare childhood malignancy. Radiology 1991;179:743-6.
62 Mark EJ. Mesenchymal cystic hamartoma of the lung. N Engl J Med 1986;315:1255-9.
63 Souza FF, Chen E. Mesenchymal cystic hamartoma of the lung: MRI and PET/CT appearance. J Thorac Imaging 2009;24:52-5.
64 Osborn M, Mandys V, Beddow E, et al. Cystic fibrohistiocytic tu-mours presenting in the lung: primary or metastatic disease? His-topathol 2003;43:556-62.
65 Fowler DJ, Gould SJ. The pathology of congenital lung lesions. Semin Pediatr Surg 2015;24:176-82.