British Homoeopathic Journal January 1991, Vol. 80, pp. 26-33 Computer-aided case-following and diagnosis ANDREW WRIGHT, MB, CHB, DCH, MCRGP Battery testing This system of diagnosis is appropriate when there are a number of possible diagnoses in mind, of roughly equal probability. Thus it is often used by relatively inexperienced doctors (e.g. housemen) who do not have enough experience of the relative incidence of disease to adequately 'weight' the different hypotheses or to assess their utility and payoff. All the hypo- theses are tested simultaneously, the main aim of the tests being to RULE OUT the possibilities one by one, until only one remains. Case-following here requires the ability to 'pencil in' a differential diagnosis without according the different possible diagnoses the status of hard fact--i.e, to enter rubrics without coding them for the time being. Heuristic diagnosis This is the type of diagnosis usually practised by young GPs and hospital registrars. It requires a Cue 1 Hypotheses I A, B, & C t ,L 1 Test A Test B Test C False TRUE False Treatment Figure 1: Battery testing. certain level of experience, to accurately prior- itize which hypothesis to test first, and to limit the range of possibilities by ruling out very unlikely or un-utilitarian diagnoses from the beginning, so that only two or three alternatives have to be considered. Tests are chosen to RULE OUTpossibilities or to DISCRIMINATE well between alternatives where there are only two front-runners. The working hypothesis will change as the problem is worked through. Thus we need to be able to retitle problems easily, and to link them in to pre-existing problems when it becomes clear that they are in fact related; e.g. chest pain is confirmed as being angina, and the patient has a previous history of myocardial infarction. SOAP One simple time-honoured way of recording the consultation in manual notes is known by the Cue 26 A, l Test A 1 False I Hypotheses I > B, & C 1 Test B Test C 1 TRUE False Treatment Figure 2: Heuristic diagnosis.
Transcript
British Homoeopathic Journal January 1991, Vol. 80, pp. 26-33
Computer-aided case-following and diagnosis ANDREW WRIGHT, MB, CHB, DCH, M C R G P
Battery testing This system of diagnosis is appropriate when there are a number of possible diagnoses in mind, of roughly equal probability. Thus it is often used by relatively inexperienced doctors (e.g. housemen) who do not have enough experience of the relative incidence of disease to adequately 'weight' the different hypotheses or to assess their utility and payoff. All the hypo- theses are tested simultaneously, the main aim of the tests being to RULE OUT the possibilities one by one, until only one remains.
Case-following here requires the ability to 'pencil in' a differential diagnosis without according the different possible diagnoses the status of hard fact-- i .e , to enter rubrics without coding them for the time being.
Heuristic diagnosis This is the type of diagnosis usually practised by young GPs and hospital registrars. It requires a
Cue
1 Hypotheses
I
A, B, & C
t ,L 1 Test A Test B Test C
False TRUE False
Treatment Figure 1: Battery testing.
certain level of experience, to accurately prior- itize which hypothesis to test first, and to limit the range of possibilities by ruling out very unlikely or un-utilitarian diagnoses from the beginning, so that only two or three alternatives have to be considered. Tests are chosen to RULE OUT possibilities or to DISCRIMINATE well between alternatives where there are only two front-runners.
The working hypothesis will change as the problem is worked through. Thus we need to be able to retitle problems easily, and to link them in to pre-existing problems when it becomes clear that they are in fact related; e.g. chest pain is confirmed as being angina, and the patient has a previous history of myocardial infarction.
SOAP One simple time-honoured way of recording the consultation in manual notes is known by the
Cue
26
A,
l Test A
1 False
I
Hypotheses I
> B, & C
1 Test B Test C
1 TRUE False
Treatment Figure 2: Heuristic diagnosis.
Volume 80, Number 1, January 1991 27
Knowledge of what is normal for that patient.
Knowledge of their illness behaviour
Time of day Modalities Modifiers
Past history Family history Doctor's mood Epidemiology Pay-off
Cue
Hypothesis generation
"--- Weighting
Test preferred hypothesis
,l Review
1 True or False?
Diagnosis<
1 Hypothesise treatments
Weighting
Test preferred treatment
Review
1 Better or not?
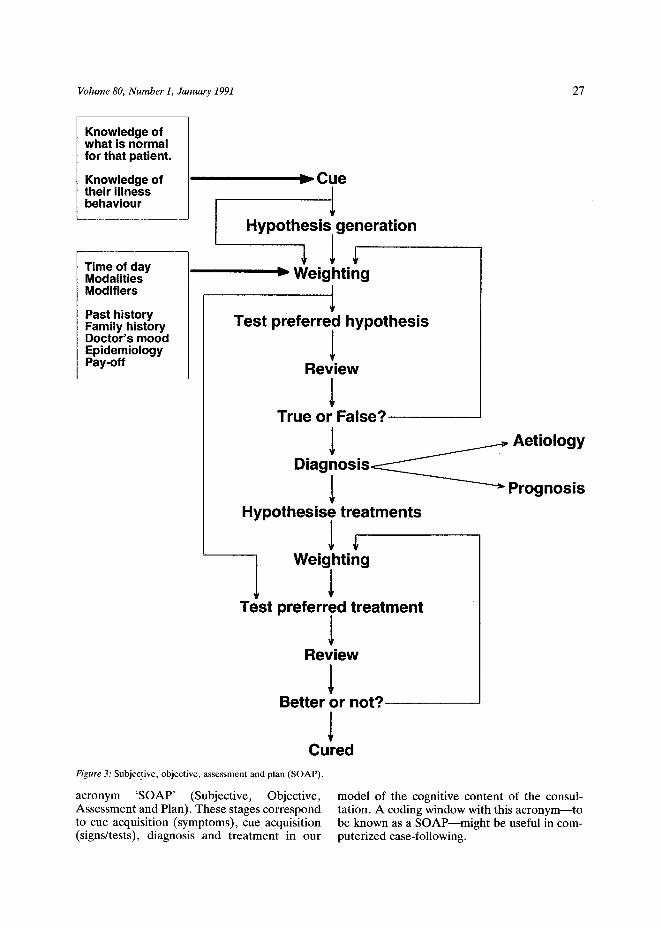
Cured Figure 3: Subjective, objective, assessment and plan (SOAP).
acronym 'SOAP' (Subjective, Objective, Assessment and Plan). These stages correspond to cue acquisition (symptoms), cue acquisition (signs/tests), diagnosis and treatment in our
Aetiology
Prognosis
model of the cognitive content of the consul- tation. A coding window with this acronym-- to be known as a SOAP--might be useful in com- puterized case-following.
28 British Hom~eopathic Journal
TeIU
100% spe~f~
100% sensitivity
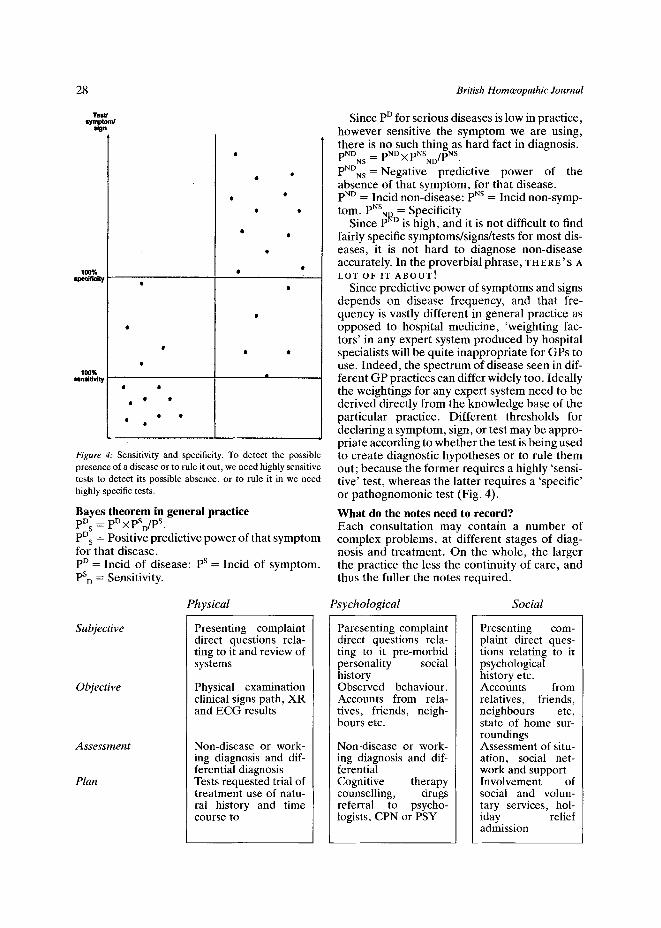
Figure 4: Sensitivity and specificity. To detect the possible presence of a disease or to rule it out, we need highly sensitive tests to detect its possible absence, or to rule it in we need highly specific tests.
Bayes theorem in general practice pD s = pD • pSD/PS" PD s = Positive predictive power of that symptom for that disease. pO = Incid of disease: pS = Incid of symptom. PS D = Sensitivity.
Since pO for serious diseases is low in practice, however sensitive the symptom we are using, there is no such thing as hard fact in diagnosis. pNDNs = pND X P~SND/pNS. PNDNs=Negative predictive power of the absence of that symptom, for that disease. pND = Incid non-disease: pUS = Incid non-symp- tom. PNSNo = Specificity
Since pND is high, and it is not difficult to find fairly specific symptoms/signs/tests for most dis- eases, it is not hard to diagnose non-disease accurately. In the proverbial phrase, T H E R E' S A L O T OF I T A B O U T !
Since predictive power of symptoms and signs depends on disease frequency, and that fre- quency is vastly different in general practice as opposed to hospital medicine, 'weighting fac- tors' in any expert system produced by hospital specialists will be quite inappropriate for GPs to use. Indeed, the spectrum of disease seen in dif- ferent GP practices can differ widely too. Ideally the weightings for any expert system need to be derived directly from the knowledge base of the particular practice. Different thresholds for declaring a symptom, sign, or test may be appro- priate according to whether the test is being used to create diagnostic hypotheses or to rule them out; because the former requires a highly 'sensi- tive' test, whereas the latter requires a 'specific' or pathognomonic test (Fig. 4).
What do the notes need to record? Each consultation may contain a number of complex problems, at different stages of diag- nosis and treatment. On the whole, the larger the practice the less the continuity of care, and thus the fuller the notes required.
Physical Psychological Social
Subjective
Objective
Assessment
Plan
Presenting complaint direct questions rela- ting to it and review of systems
Physical examination clinical signs path, XR and ECG results
Non-disease or work- ing diagnosis and dif- ferential diagnosis Tests requested trial of treatment use of natu- ral history and time c o u r s e t o
Paresenting complaint direct questions rela- ting to it pre-morbid personality social history Observed behaviour. Accounts from rela- tives, friends, neigh- bours etc.
Non-disease or work- ing diagnosis and dif- ferential Cognitive therapy counselling, drugs referral to psycho- logists, CPN or PSY
Presenting com- plaint direct ques- tions relating to it psychological history etc. Accounts from relatives, friends, neighbours etc, state of home sur- roundings Assessment of situ- ation, social net- work and support Involvement of social and volun- tary services, hol- iday relief admission
Volume 80, Number 1, January 1991 29
Example of present paper records entry 18/ 9/89 LSCS: Baby in SCBU with Oeso-
phageal Fistula 27/10/89 Came home 1/52 ago
Present problems: (1) Wound infection of LSCS
scar: Rx Amoxil/Flagyl (2) Postpartum anemia:
9.9 grn/dl. AND had retained mem- branes post LSCS! �9 still bleeding--but very reluctant to have D and C. Check FBC, Ferritin Rx Pregaday TT o.d.
(3) Can we prescribe Aptimil? Check with Chemist.
Same entry, on computer system 18/ 9/89 Lower seg caesarian sect[Oper] C 27/10/89 Post-op infection of LSCS scar c * AMOXIL 500 mg caps take one
three times a day 21 caps 0/1 M * FLAGYL 400 mg tabs take one
three times a day 21 tabs 0/1 M 27/10/89 Postpartum hemorrhage, c
:Hb :MCV :MCHC Hemoglobin low. :9.9 : : L Secondary P.P.H. Still fresh bleed- ing after 5/52 N Retained placental membranes-- post LSCS! Very reluctant to h N Serum ferritin/TIBC. Requested L
* PREGADAY tabs take two a day. 56 tabs 27/1/90 M
Problems with the computer version Absence o f visual clues to significance, time course and causal links Lower case 'c' for Caesarian. No punctuation in medication entries. Inappropriate capitals for drugs. No ability to inset lines or alter their spacing on
the page. Inappropriate level of detail in drug entries. In order to show 'tree' of causality, must enter
subsidiary problems first and then link to main problem: clumsy.
Can only show two levels of causal 'tree' 'C'x~r 'c'. Inability to show links by using 'AND'. Unable to code post-partum anemia per se: had
to use P.P.H. code. Inability to code 'Reluctant to have D and C'. Inability to code 'Serum ferritin requested'
appropriately: had to use lab code inappropriately.
One code rubric per line, clutters the page and obscures linkages�9 Reluctance to consider formulating the prob-
lem in free text seems to stem from several aspects:
- - A n ' E i t h e r . . . or' approach to the free text vs coding argument�9 BUT modern software techniques such as hypertext would allow us to use both, with the codes being 'hidden' behind any part of the free text which corresponded to a Read code rubric.
- - A feeling that causal links must be expressed in some computer-analyzable way, for sub- sequent study of these links over large groups of patients HOWEVER, even the AI experts at the meeting today acknowledged that such analysis is very difficult--and while we are waiting for this dream to come true, the simple clinical care of individual patients is being impaired and the encounter recording necessary for data col- lection therby being discouraged.
- - 'F ree text = unpredictable demands on disc space'--is this REALLY likely to be a problem? My patients' notes contain more referral let- ters than they do continuation sheets--and the software could discard the free text ver- sion of a problem after a set period, retaining the coded version.
Visual display of linkages (Fig. 5) One approach already in use in the motor indus- try, which can elucidate such links clearly, is Hypertext. In this system, pointing to a word or graphic (with a mouse) and then clicking on it using various different cursors, can show the linkages between that item and others; related information on the item (perhaps drawn from a linked database such as the Oxford Textbook o f Medicine); an explanatory note (such as the Read code linked to the word); or an associated image or graphic.
Such an approach, combining text and gra- phics, would have great advantages in terms of user friendliness. However, I am told that refreshing a bit-mapped terminal screen at any reasonable rate would require far higher baud rates than GP systems currently use; the alter- native being a costly network of workstations.
A picture is worth a thousand words A flow chart's the next best thing Numeric data such as blood pressure readings become far more usable when displayed in
30 British Hom~eopathic Journal
18/9/89 L.S.C.S.
CAME HOM 1/52 AGO
I " POST-PARTUM ANEMIA
RETAINED MEMBRANES
CONTINUED P.P.H.
Reluctant to have D & C
Figure 5: Visual display of linkages.
Check FBC, Ferritin Rx Pregaday TT o.d.
graphical form, even if only a star bar-chart like the age-sex report format, rather than true graphics.
Chronic diseases require some comparison of data from one assessment to the next, if monitor- ing is to have any purpose. This means we need some sort of flow chart into which the data from our tests and observations is autofed. Ideally we would have mini spreadsheets available within each such patients' notes, configurable to the practice's chronic disease protocol for that condition.
Prescribing for multiple problems raises the difficulty of identifying what other drugs the patient currently uses. Compliance checking is important too. Easy access to a list of current drugs is essential: better would be a bar-chart showing all current drugs, with the duration of each prescription for them plotted out against time.
Administration For pathology and imaging investigations, there are a number of stages between requesting the test and acting on the result:
Request marked in notes Patient given path forms and explanation of how
to get the test done
Nurse takes blood from patient Sample sent to Lab Lab result received Results checked daily by doctor, and marked
'normal, get notes out, see doctor' Patient rings receptionist for result and makes
appointment to see doctor to discuss results Doctor acts on results
Similar chains occur for smears, immunizations etc.
Such a chain of events contains many oppor- tunities for going astray, However, the adminis- trative codes necessary to follow the chain through without breaks, badly clutter up the clinical records with material mainly relevant to reception, not to the GP. We need a simple system to toggle such codes in and out of sight on the screen.
Implications for computerized encounter recording Codes, computers and data-purchasers like hard facts. Much encounter recording is 'soft' data which only firms up over a period of time. The codes are excellent tools to ensure uniform data entry and analysis, but are largely irrelevant to the process of working up a case because they demand firm data.
Volume 80, Number 1, January 1991 31
By requiring one fact at a time on one line at a time, coding militates against an integrated assessment of the physical, psychological and social aspects of a problem.
To overcome these problems, journal 'pages' which allow FREE TEXT entry of an UNDEFINED PROBLEM are necessary. I envisage a system
which can allow either prospective or retrospec- tive marking of important words in such a record, rather like the use of 'boxing' and high- lighter pens on manual records.
Such marked words would subsequently be automatically coded by a programme similar to a spelling checker, checking each word against an
Knowledge of what is normal
Time of day Modalities Modifiers
Past history Family history Doctor's mood Epidemiology* Pay-off
Cue
1 Hypothesis generation*
.--~ Weighting*
l Test preferred hypothesis
l Review
l True or False?
l Diagnosis*<
Hypothesize treatments*
Weighting*
l Test preferred treatment
l Review
l Better or not?
Cured
Aetiology*
--~Prognosis*
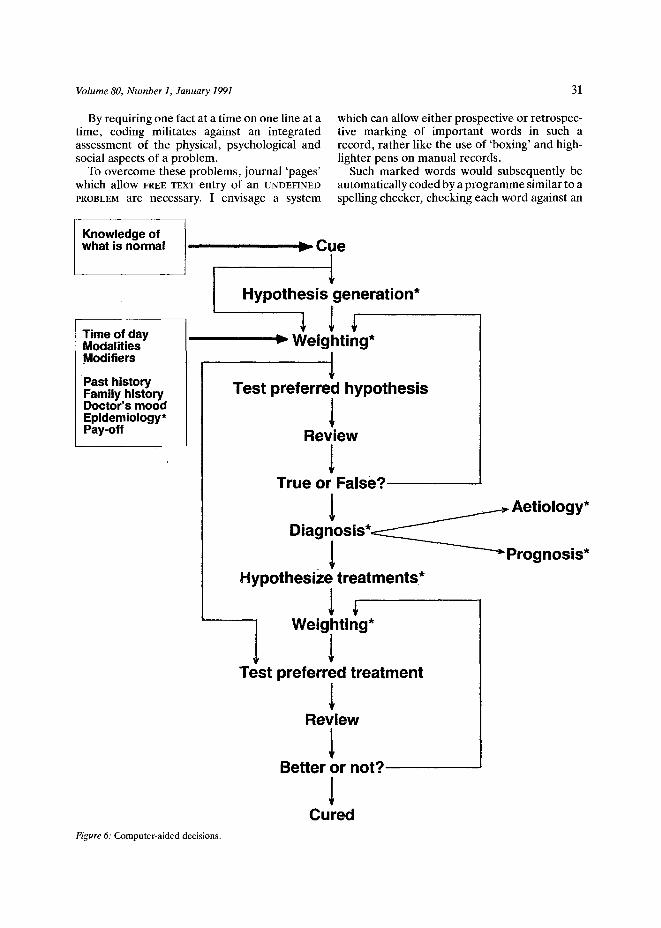
Figure 6: Computer-aided decisions.
32 British Homteopathic Journal
alphabetic list of Read codes and synonyms and if in doubt offering one various codes (with their rubrics) to choose from.
The Meditel software already has suitable software, in the form of the Lyrix spell checker. If its dictionary were replaced by the Read code rubrics, it could check any word written in capitals, for example, and offer a choice of sev- eral synonyms. The output of the spell checker would then have to be redirected into a tempor- ary on-screen window in which other aspects of the coding (such as encounter type and recall date) would be entered and the contents of the window then stored in the database, leaving only the free text on screen with the important words in capitals. To leave potential diagnoses uncoded, one would simply enter them in lower case, changing them to upper case and triggering the auto-coding system once the diagnosis was established. For those who dislike free text, a software toggle would switch between free text mode and the existing coded mode.
Another possible way to do this would be a Mouse-driven system which highlighted relevant words in inverse video. I have been told that this is technically impossible because of the variety of ways in which terminals handle inverse video. I do not know why one cannot get round this via the system's terminal definition files. I can see that it might be physically difficult to connect mice to terminals already linked both to the CPU and to a through terminal printer.
A third way would be to use a hypertext system such as Guide, as already discussed.
The present system represents a great advance in offering problem-orientated records by link- ing a number of entries to one problem title. However the true 'title' of a particular problem rarely becomes clear at the first consultation. We need to be able to create untitled problems and title or retitle them subsequently with ease. The title may need to contain more than one code, and to have several layers of subtitles to indicate complications etc.
The GP's need to record the absence of symp- toms and signs (for medico-legal reasons) and his preoccupation with the diagnosis of non- disease (e.g. 'Ca Stomach excluded') set me wondering whether each Read code shouldn't have a negative version, which would simply be the same code preceded by a minus sign and with the rubric suitably negated.
The Read codes started out as primarily a path- ological classification. Their great strengths are (a) the hierarchical structure, which allows searches at
different levels of detail, and encourages one to refine the level of detail which is coded, and (b) the integrated system of synonyms which makes the use of the codes so practical for data entry.
However, the GP is often more interested in symptomatology, health beliefs, aetiology, management and prognosis than in pathology per se. (He may be unable to reach a diagnosis at all, whilst being able to formulate a practical plan of management.) Also, much of the meaning in many consultations lies in their psychodynamics rather than their physiological content.
In so far as the codes handle these aspects at present, they do so by pragmatically locating codes for them in chapters 0-9 of the hierarchy, above the disease code chapters A-Z . It might be more logical to handle them as separate but interlinked dimensions--but how this could be done in practice I honestly do not know. The SNOMED experience is not encouraging. It would require the application of AI concepts such as 'the tangled hierarchy', etc .--but would have the potential for example to handle homeeo- pathic 'modifiers', health beliefs, etc. much more logically and to irltegrate them into the decision-making process of future medical AI systems more easily.
Computer-supported decision-making Hypothesis generation could be aided by a com- puterized 'French's Index'. Humans cannot retain more than about four different possibil- ities at once: but the very broad spectrum of ill- ness we see often requires more lateral thinking than we are capable of.
Weighting requires probabilities: both the inci- dence of that disease in your practice, and the sen- sitivities and incidence of many different symptoms, signs, and tests. Acquiring these demands long experience, and they are usually very difficult to measure and thus are used subcon- sciously-hence the older GP's gradual shift from heuristic diagnosis to pattern recognition. A national database of symptoms, signs and test results, linked to subsequent 'definitive' diag- noses, would enable us for the first time to gener- ate such sensitivities and specificities; whilst the practice's own morbidity data, or a national aver- age weighted for local incidence and the age-sex structure of one's list, could give the GP the a priori likelihood of a given disease. This would
Volume 80, Number 1, January 1991 33
enable us to use Bayes' Theorem to derive a math- ematical approach to differential diagnosis in general practice.
Diagnosis and prognosis (which latter is the patient's main concern) could then be checked by using computer databases such as the Oxford Text- book of Medicine.
Generating ideas on how to treat, could be aided in the codes relating to each chapter heading in the British National Formulary brought up on the screen a monograph about that area of treat- ment, similar to those contained in the BNF. Poss- ible drugs to be used should be checked for interactions with the patient's pre-existing medi-
cation using Philex or similar. Doctor warnings can be shown on screen, from the new Read codes drug database,
If such databases are to be used in practice, they must be easily and speedily accessible: a toggle which takes one into the relevant database at the relevant point for any given Read disease or drug code would be suitable, and it should be acti- vatable before the Read code is transcribed from the screen buffer onto the main database.
Specific conditions such as asthma, hyperlipid- aemia, diabetes, hypertension, etc. can be dealt with using computer protocols programmed to ensure full recording of particular features.
Address for correspondence Dr Andrew Wright St Johns Health Centre Oak Lane Twickenham TW1 3PA