402 IEEE TRANSACTIONS ON TERAHERTZ SCIENCE AND TECHNOLOGY, VOL. 3, NO. 4, JULY 2013
Conceiving THz Endometrial Ablation:Feasibility,Requirements and Technical Challenges
Perambur S. Neelakanta and Bharti Sharma, Student Member, IEEE
Abstract—Shallow-ablation of endometrial lining using mi-crowaves has been traditionally indicated as a minimally invasivetreatment option for dysfunctional uterine bleeding (DUB).Known as microwave endometrial ablation (MEA), relevantprocedure is used as an alternative to hysterectomy considering itssafety, simplicity and effectiveness. In lieu of the prevailing MEAtechniques, it is attempted in this study to foresee the possibility ofconceiving an alternative and a newer option on endometrial ab-lation using mm-wave/THz frequencies. Commensurate with thismotivated impetus, objectively considered are merits and designissues of using electromagnetic (EM) spectrum of mm-wave/THzregion toward optimal conversion of EM energy into a thermalablative source so that, the basal layer of endometrium can beeffectively destroyed in surgical contexts as necessary. Hence,the feasibility of designing appropriate TEA applicators forcontrolled and safe procedures so as to ablate just the unwantedtissues within a localized zone of energy field is addressed. Lastly,a quantitative analysis on the interaction of THz EM-energyversus the lossy dielectric characteristics of endometrial mediumis indicated to model the underlying (THz-energy)-to-(thermalenergy) transduction. Relevant prospects of conceiving TEA andthe associated pros and cons are identified specific to the prospectsof feasibility, requirement considerations and technical challenges.
Index Terms—Endometrial ablation, medical application ofTHz-band, similitude principle, terms- mm-wave/THz spectrum.
I. INTRODUCTION
T HE scope of this paper is to foresee the possibility of con-ceiving a newer option of using electromagnetic (EM) en-
ergy at mm-wave/THz frequencies for ablation procedures per-tinent to the endometrial lining in the uterus.Ablation literally implies removal of material from the
surface of an object. Classically, surgical ablation has beenthe strategy in clinical contexts involving scalpel-and-scis-sors with cut-and-sew procedures; and, relevant Cox–Mazetechnique [1] involved incisions that were technically difficultto perform with added risks due to the extended time on analready time-consuming surgery (such as in open-heart bypassprocedure). Hence, it resulted in a limited use and alterna-tive methods like, using laser (laser ablation) to vaporize thetissue without surgery as well as other invasive applicationsof low-temperature cooling (cryoablation), chemical (ethanolablation) or heat induced via high-frequency electromagnetic
Manuscript received October 02, 2012; revised March 19, 2013; acceptedMarch 21, 2013. Date of publication April 15, 2013; date of current versionJune 27, 2013.The authors are with the Department of Computer and Electrical Engineering
and Computer Science, Florida Atlantic university, Boca Raton, FL 33431 USA(e-mail: [email protected]; [email protected]).Color versions of one or more of the figures in this paper are available online
at http://ieeexplore.ieee.org.Digital Object Identifier 10.1109/TTHZ.2013.2255049
(EM) energy (called radio-frequency (RF) ablation). All suchefforts focus on eradicating or substantially destroying thepathogenic tissue at desired anatomical sites.With the advent of developments in microwave technology,
more advanced methods of using EM energy to induce local-ized-heating (at desired locations in the tissue-medium) alsocame into existence. Known as microwave ablation, the under-lying technique uses EMwaves at compatible frequencies in thespectrum ranging from 900 to 2500 MHz [2]; hence, a varietyof clinical indications on successful use of microwave ablationhave emerged. Patient’s option, tissue-sparing, multiple tumorsyndrome or previous organ resection are precursors in adoptingsuch microwave ablation as a selective procedure; and, it is indi-cated as a viable candidate typically directed at anatomical siteslike, liver, lung, kidney, prostate, bone, breast, thyroid, brain,spleen, cardiac/arterial region, endometrial lining, collagenoustissues, varicose veins, esophagus, etc.The considerations in using microwaves in the ablation
procedure and the associated conceivable drawbacks are asfollows. 1) At the working microwave frequency (like 2.45GHz), the depth of penetration of EM energy is in the range 1–3cm in biological tissues. As such, the heating precision maynot be as exquisite vis-à-vis the associated energy absorption.2) Rapid heating and high temperature realization across alarge volume are critical posing relevant safety evaluations inmonitoring standpoint, when rapid heating might be difficult tocapture without real-time imaging. 3) Feeding the applicatorwith microwave energy drawn from a generator via a cablingsystem may cause overheating of the cable and resulting in aloss of power supplied to the applicator. In order to offset suchcable-loss and reduction in efficiency, adjunct cable-coolingmay be required. 4) Further, the undesirable heating of tissuesalong the transmission-line (cable) is also feasible unless, it iscounter-measured. 5) The critical part of microwave ablationdesign is concerned with the applicator-antenna. It requiresa tradeoff between the required heating-profile, the extent ofpermissible invasion of the applicator at the ablation site (inpercutaneous devices), power-handling capability, efficiencyof EM-to-thermal energy transduction and cost-effectiveness.Further, the prevailing antenna designs largely produce elon-gated ablations that may not be desirable in certain contexts.Notwithstanding the developments and practice of mi-
crowave ablation as narrated above, the scope of the presentstudy is to consider newer options of using upper mm-waveband through THz spectrum of EM energy for ablation purposesin lieu of the existing RF/microwave ablation techniques. Themotivation thereof stems from the following considerations.• Futuristic EM applications are seriously sought to explorethe unused windows of mm waveband and the unallocated
NEELAKANTA AND SHARMA: CONCEIVING THz ENDOMETRIAL ABLATION 403
regime of THz band. These spectral windows can accom-modate a broadband of EM energy yielding variety andflexibility toward ablation system designs. Though, rele-vant EM spectra are sparsely known in terms of the under-lying EM wave interaction characteristics with the mediasuch as biological substances, indicated, nevertheless, inthe present study are certain merits that can be foreseen inadopting these spectra (either in supplanting or when usedin conjunction with microwaves) for specific ablation ap-plications and anatomical sites.
• To implement the proposed ablation method with EMenergy spanning 30 GHz through terahertz spectrum,corresponding details on dielectric dissipation-loss char-acteristics (in the lossy biological medium) and theassociated thermal energy realized are not per se avail-able; and, almost little known efforts have been reportedin designing relevant ablation techniques deploying suchmillimeter and/or micrometer wavelengths of EM spec-trum. As such, unique considerations are required toformulate fresh algorithms and compute details pertinentto: 1) lossy dielectric characteristics of biological media atthe test mm/THz band [3]; 2 ) elucidating the transductionaspects of (EM energy)-to-(thermal energy); 3) deducingrelevant heat energy proliferation and convection profiles[4]–[7]; 5) formulating the associated dynamics of rate ofheat absorption and convection details; and 6) identifyingthe steady-state thermal conditions conducive for thedesired ablation at a specific site.
• The extremely high-frequency test-band of mm-wave/THzEM spectrum being considered also implies concurrently,a significantly lower wavelength (relative to traditionalmicrowaves) falling in millimeter through micrometerregime. Hence, the feasible ablation designs would corre-spond to the possibility of: 1) Conceiving “scaled-down”(miniaturized) applicator structures vis-à-vis the wave-lengths of interest; 2) selecting highly-localized andcritically specific, spotty ablation sites for precision pro-cedures (consistent with the site-dimension and zone ofablation being comparable to the wavelengths involved);and 3) constraining/restricting deep-body heating at thelocalized ablation site, inasmuch as the depth-of-penetra-tion (skin-depth) of EM energy in the dissipative mediumis an inverse function of frequency; as such, unnecessaryheat pervasiveness to other proximal anatomical regionscan be avoided.
• With super high frequencies of THz band and corre-sponding dielectric losses, the intratumoral temperaturescan be driven consistently higher. This may enable con-ceiving spotty-to-extended zones of ablation with easeand considerably less treatment time.
• Relatively small and miniaturized applicator feed-shaft di-mensions (prorated to the wavelength involved) may re-duce the risk of shaft-related abnormal heating/burning oftissues at the feeding-end.
• Physically small antenna dimensions (consistent withmm m wavelengths) would permit an array of dis-tributed framework of antenna elements leading to thechoice of ablation zones to be small or large on ad hocbasis.
• With the physical size of antenna/shaft paraphernaliascaled-down, appropriate cooling system can also bedesigned and housed conveniently.
Hence reviewed in this paper is the feasibility aspect ofknowing whether mm-wave/THz band spectrum of EM energycould be a possible candidate for medical ablation procedures.A specific case thereof in realizing endometrial ablation usingthe test band of EM spectrum of interest is investigated iden-tifying the pros and cons relevant to the requirements andunderlying challenges.
II. EM-ENERGY BASED SHALLOW-ABLATION OFENDOMETRIAL SURFACE
Traditional method of shallow-ablation or “scouring” ofendometrium with thermal source induced via MEA, is broadlydiscussed in [8]–[10]. In all such studies however, the scopeof MEA is described largely in qualitative details concerningsystem development, applicator design and modeling, exper-imental/clinical trials and treatment dynamics (pertinent todysfunctional uterine bleeding, or DUB, also known as menor-rhajia).The present study as stated earlier, proposes an alternative
method parallel to MEA to conceive THz endometrial ablation(TEA); and, attempted thereof are foreseeable considerationsto evaluate the efficacy of the proposed suite on feasibility as-pects, requirements and technical challenges. Hence, evolved isa comprehensive modeling of (EM energy)-to-(thermal energy)conversion at the mm-wave/THz-band frequencies vis-à-vis theTEA applications as detailed below.In modeling the phenomenon of interaction of EM energy
versus a biological locale in the human-body and deducing theassociated thermal considerations (such as, heat generated, rateof heating, heat absorbed by the medium, conduction of the heatacross the zone(s) of interest and the dynamics of associatedtemperature profile across the zone), it is necessary to first con-sider the following parameters: Frequency/wavelength of EMexcitation, geometry of the region being exposed to EM energy,associated EM parameters (such as, complex permittivity) andthermal characteristics of the bio-medium.One of the authors has comprehensively studied elsewhere (in
different bioelectromagnetic contexts), relevant interaction as-pects of EM-energy versus bio-medium, specific to ocular lensin human eye [4], human embryo in uterus [5], frozen red-bloodcells [6] and rewarming of human limbs [7]. The prior knowl-edge from such efforts is invoked in this study to gather a hostof details on EM-to-thermal energy transduction (across a bio-medium) and apply them to the heating of endometrial liningspecific to TEA considerations. The EM and thermal consider-ations toward modeling the TEA are outlined below.Assuming a normal uterus, it typically has the size and shape
of an upside-down pear weighing approximately six ounces(170 g). Its dimension is about 8–10 cm 6 mm Further,the wall thickness of the uterus is approximately 1 cm [5].Available in [3] are electromagnetic and thermal constants ofa typical tissue medium. For analysis proposes, the uterus canbe modeled as a thin-walled pouch excited by a current source(depicting an intravaginal applicator).Further, inasmuch as, the uterine wall gets thickened with a
smear of heavy blood during DUB, the EM power applied while
404 IEEE TRANSACTIONS ON TERAHERTZ SCIENCE AND TECHNOLOGY, VOL. 3, NO. 4, JULY 2013
ablation procedure should be adequate to increase the endome-trial surface temperature with the presence of blood. So, energyabsorption due to blood-content should also be duly consideredin deciding the EM power source required.
III. ELECTROMAGNETIC HEATING OF THE BIO-MEDIUM
In order to estimate the steady-state thermal conditions andtemperature distribution profile in the interior lining of theuterus pouch, relevant model will involve the thermal parame-ters of a tissue medium [3], the body temperature (in C) andthe flux density of conducted heat energy, (in joules s/m ).Further, the intravaginal applicator facilitated for EM excitationof the endometrium can be assumed as a current source.Now, considering any point within the uterus-wall
medium subjected to EM ablation, the heat-flux density (undera steady-state condition) along the three coordinates canbe written as follows: ( ; ;and, where depicts the heat conductivity(in calories m C s). Further, under steady-state conditions, itis assumed that the heat diverging from an infinitesimal volumeat any point of observation (x, y, z) must be equal to the heatgenerated due to EM absorption within that volume. Therefore,if is the electrical conductivity (in S/m) of the bio-medium and
is the electric intensity at the point of consideration,then conforms to the following gradient relation:
(1)
Hence, it follows that
(2)
The Poisson’s (2) has the following solution:
(3)
where U(x, y, z) denotes an auxiliary potential function (at thepoint of observation in the medium) and denotes aconstant potential function. Further,and, the setrepresents the electric field intensity components excitedas a result of EM energy applied. Hence, explicitly (2) can bewritten as follows:
(4)
However, (Laplace equation) for a potential func-tion at any point in the medium free of heat-source. As such,
(5)
Further, assuming , the tem-perature gradients can be deduced from (3):
; and.
However, the temperature gradients tangential to theendometrium can be reasonably neglected within the short-du-
ration of ablation procedure involved. That is, along theboundary surface of the endometrial-lining, the temperaturegradient would consequently vanish, provided is presumedas the conductor potential, namely, the bio-medium being fairlyconductive.The initial rise of temperature at an -point
in the medium due to EM absorption will depend mainly on theheat capacity of the medium; and as a function of time,t is determined from the relation: .Hence, it follows that
(6)
where is a constant, which can be taken as the initial condi-tion of body-temperature prior to ablation procedure.Suppose specifies the electric-field intensity per ampere in-
duced as a result of the current source (depicting the applicator)supporting I amperes; then, the incremental temperaturecan be specified via (6) as follows:
(7)
where denotes the scalar potential function at the pointunder consideration; and denotes the resistance
(in ohms) to the high-frequency current-flow in the medium.Further, accounting for the curved feature of the endome-trial-lining surface having a radius of curvature m , thefollowing explicit details can also be specified.Typically, would vary as a function of as follows. As-
suming a remote source of excitation, the electric field as afunction of can be written in terms of microscopic Ohm’slaw via the associated current-density, as follows:
. Further, inasmuch as denotes theresistance of the medium along the curved surface, it is ap-proximately equal to ( therefore, it can be written that
Relevantly, for a homogenous, isotropic medium depictingthe endometrial surface, it is reasonable to assume the near-surface temperature (neglecting convection and radiation heattransfers) as ; with an initial temperature. Therefore
(8)
And, the increase in temperature is given by:
(9)
Corresponding near-surface temperature can be deducedas follows:
(10)
where is the excitationmagnetic-field intensity due to the cur-rent source, is the free-space intrinsic impedanceand depicts the dielectric constant of the medium.
NEELAKANTA AND SHARMA: CONCEIVING THz ENDOMETRIAL ABLATION 405
IV. EM POWER DISSIPATION IN THE ENDOMETRIUM AND
CALCULATION OF TEMPERATURE RISE
When a bio-medium is exposed to EM energy, a specific ab-sorption rate (SAR in W/kg) can be defined to quantify the rateat which energy is absorbed by the medium. Thus, SAR can becalculated in terms of the electric field within the bio-mediumas follows: , where
is the density of the sample at the spatial variable, r of the samplegeometry.Suppose a comparison is made between MEA and TEA on
their bioelectromagnetic aspect of ablation with the traditionalmicrowave frequency adopted specified as Hz. Let the fre-quency envisaged in the proposed TEA be . Then, the fol-lowing explicit relations can be derived:
(11)
where is the incremental surface temperature (in C) anddenotes the time-involved
(in seconds) in heating the medium.In order to evaluate the relative performance of TEA versus
MEA, relevant frequency-scaling can be imposed on the abla-tion-related parameters. For this purpose, the concept of Buck-ingham’s similitude principle [11] can be used. Relevant con-siderations are as follows:Knowledge on lossy-dielectric and related thermal character-
istics of various biological media in the lower strata of radio-fre-quency (RF) band has been fairly comprehended [3]; however,pertinent details across the submillimeter wave-band and THzspectrum are rather sparse. Hence, indicated in this study is amethod of judiciously sharing “similarity” details of bio-mediaalready available as “models” in the traditional, lower-side EMspectrum, (namely, VLF through micro/mm-wave) so as to de-duce the “inferential prototypes” that represent EM propertiesof biological media at submillimeter/THz frequencies. For thispurpose, the principle of similitude due to Buckingham [11] canbe adopted to obtain the model-to-(inferential) prototype trans-formations on generic dielectric and conducting properties ofbiological materials, which can be used to make a comparisonon the relative efficacy of MEA versus TEA. The computationaldetails using the model indicated above for endometrial ablationare presented below.
V. MEA/TEA RELATED COMPUTATIONAL DETAILS ONENDOMETRIAL HEATING
Endometrial ablation implies heating uterus-lining so as to“ablate” the underlying myometrium to an extent of 6 to 8 mm.That is, the heating enabled by EM energy is confined to a su-perficial zone dictated by the depth of penetration (skin-depth,in m) of the EM waves applied. This skin-depth, (in m)
is given by: where f is the frequency in Hz,(in S/m) denotes the electrical conductivity of the medium and
is the permeability of the medium; further, isthe relative permeability, (which is equal to 1 for the tissuemedium) and H m depicts the free-spacepermeability. Suppose the value of of a tissue-medium (suchas, endometrium) is known across the spectrum of microwave
Fig. 1. Electrical conductivity , dielectric constant and the ratioof a typical (wet) tissue medium versus frequency.
through THz band. Then, the skin-depth can be evaluated as afunction of frequency.In the literature [3], versus frequency of tissue medium (wet
with water-content) is available over 1 MHz through 1GHzrange along with corresponding values of dielectric constant asillustrated in Fig. 1.In terms of the assigned frequency for MEA namely, (in
Hz) and the assumed test frequency of TEA as , as indicatedearlier, (11) can be rewritten as follows:
(12a)
In other words, the similitude ratio of: (temperature-rise atin C )/(temperature-rise at in C ) is given by:
(12b)
That is, (12) implies a scaled up “prototype” at relative toa “model” at written in terms of the so-called dimensionlessBuckingham’s -format. It thus specifies the temperature-rise(in C s) in the prototype-structure of TEA being conceived atin terms of the corresponding temperature-rise in the known
model-structure of MEA for a given EM power-level of excita-tion. It can be noted that, heating involved in TEA will be a pro-rated value observed in MEA and the prorating coefficient is asimple ratio, namely, . Thus, using thepattern of as a function of frequency ( ) as illustrated inFig. 1, the principle of similitude permits deducing the heating
406 IEEE TRANSACTIONS ON TERAHERTZ SCIENCE AND TECHNOLOGY, VOL. 3, NO. 4, JULY 2013
performance (expressed in terms of temperature-rise in C s) inTEA procedure relative to corresponding results in MEA.
VI. OBSERVATIONS AND DISCUSSIONS
In endometrial ablation, the anticipated design optimizationsinclude: 1) realizing consistently high myometrium tempera-tures; 2) enabling desirable heat conduction profiles; 3) accom-modating large ablation regions (viewed in terms of the surfacearea and depth of the endometrium to be ablated; 4) facilitatingfaster ablation times toward quick procedure; and 5) achievingreduced procedural complexity via less painful ablation methodset compatible for the anatomical site in question.The concept designs and experiments of EM-energy based
ablation envisaged in practice [12] mostly offer qualitative de-tails on basic physics concerning EM interactions with the tissueand corresponding conversion of EM (RF/microwave) energyinto thermal energy; and, the method of applying EM-energyusing an applicator (made of a feed plus antenna combination) isemphasized vis-à-vis the focused ablation site. Commensuratewith the associated thermodynamics of heat patterns generatedspecific to achieve an effective ablation via (EM energy)-to-(biomedia) interactions, designing a proper applicator is a pri-mary design objective. It should be consistent with related de-tails on EM power generation, effective feeding of EM energyto the site of ablation (via a transmission-line such as a coaxialcable) and applying the EM-field to the zone of interest with acontrolled proliferation. Safe transduction of (EM energy)-to-(thermal energy) without hot-spots, overheating and/or failures,cooling the antenna/feeding structure as necessary so as to avoidunnecessary heating of zones en route and achieving efficientablation are desired features in the design optimizations.As indicated before, techniques traditionally developed for
various ablations use designated frequencies like 915 MHz and2.45 GHz (ISM band). Notwithstanding the existence of suchMEA, the transition design being proposed here refers to iden-tifying the pros and cons of using upper EM spectrum spanningmm-wave through THz band (in lieu of RF/microwaves). In thiscontext, the feasibility aspects, transition design issues and tech-nical challenges vis-à-vis clinical requirements are reviewed inthe following subsections as regard to the proposed TEA.
A. TEA: Feasibility Considerations
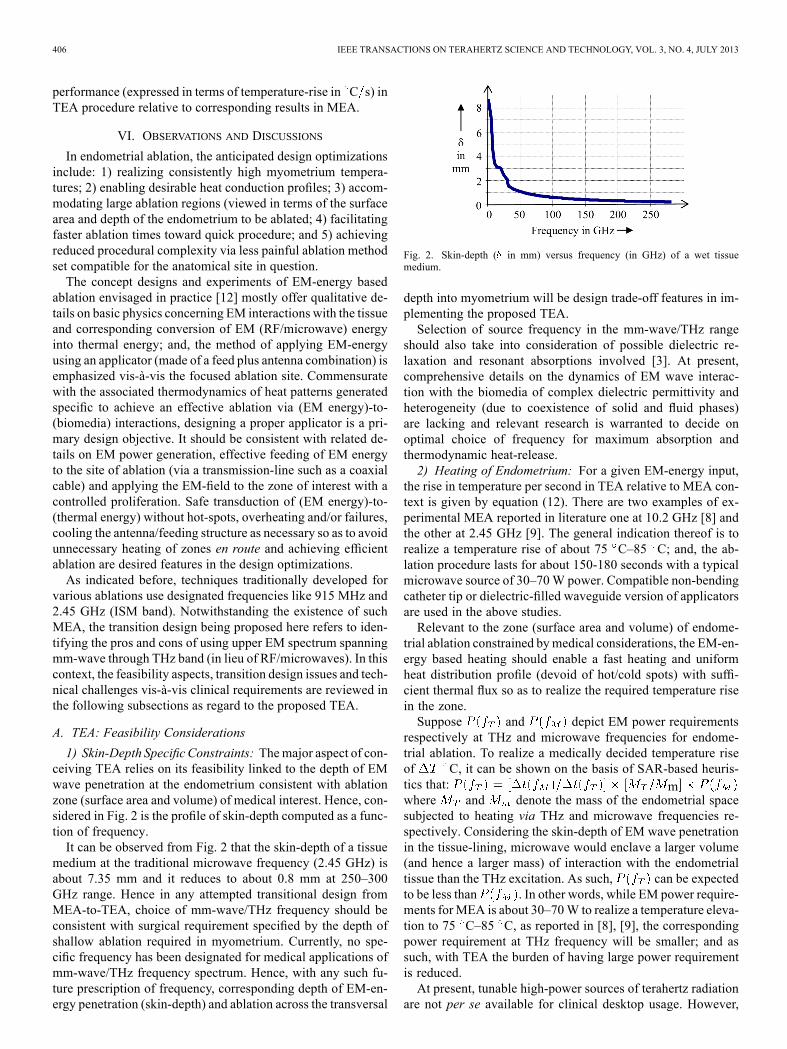
1) Skin-Depth Specific Constraints: Themajor aspect of con-ceiving TEA relies on its feasibility linked to the depth of EMwave penetration at the endometrium consistent with ablationzone (surface area and volume) of medical interest. Hence, con-sidered in Fig. 2 is the profile of skin-depth computed as a func-tion of frequency.It can be observed from Fig. 2 that the skin-depth of a tissue
medium at the traditional microwave frequency (2.45 GHz) isabout 7.35 mm and it reduces to about 0.8 mm at 250–300GHz range. Hence in any attempted transitional design fromMEA-to-TEA, choice of mm-wave/THz frequency should beconsistent with surgical requirement specified by the depth ofshallow ablation required in myometrium. Currently, no spe-cific frequency has been designated for medical applications ofmm-wave/THz frequency spectrum. Hence, with any such fu-ture prescription of frequency, corresponding depth of EM-en-ergy penetration (skin-depth) and ablation across the transversal
Fig. 2. Skin-depth ( in mm) versus frequency (in GHz) of a wet tissuemedium.
depth into myometrium will be design trade-off features in im-plementing the proposed TEA.Selection of source frequency in the mm-wave/THz range
should also take into consideration of possible dielectric re-laxation and resonant absorptions involved [3]. At present,comprehensive details on the dynamics of EM wave interac-tion with the biomedia of complex dielectric permittivity andheterogeneity (due to coexistence of solid and fluid phases)are lacking and relevant research is warranted to decide onoptimal choice of frequency for maximum absorption andthermodynamic heat-release.2) Heating of Endometrium: For a given EM-energy input,
the rise in temperature per second in TEA relative to MEA con-text is given by equation (12). There are two examples of ex-perimental MEA reported in literature one at 10.2 GHz [8] andthe other at 2.45 GHz [9]. The general indication thereof is torealize a temperature rise of about 75 C–85 C; and, the ab-lation procedure lasts for about 150-180 seconds with a typicalmicrowave source of 30–70W power. Compatible non-bendingcatheter tip or dielectric-filled waveguide version of applicatorsare used in the above studies.Relevant to the zone (surface area and volume) of endome-
trial ablation constrained bymedical considerations, the EM-en-ergy based heating should enable a fast heating and uniformheat distribution profile (devoid of hot/cold spots) with suffi-cient thermal flux so as to realize the required temperature risein the zone.Suppose and depict EM power requirements
respectively at THz and microwave frequencies for endome-trial ablation. To realize a medically decided temperature riseof C, it can be shown on the basis of SAR-based heuris-tics that: mwhere and denote the mass of the endometrial spacesubjected to heating via THz and microwave frequencies re-spectively. Considering the skin-depth of EM wave penetrationin the tissue-lining, microwave would enclave a larger volume(and hence a larger mass) of interaction with the endometrialtissue than the THz excitation. As such, can be expectedto be less than . In other words, while EM power require-ments forMEA is about 30–70W to realize a temperature eleva-tion to 75 C–85 C, as reported in [8], [9], the correspondingpower requirement at THz frequency will be smaller; and assuch, with TEA the burden of having large power requirementis reduced.At present, tunable high-power sources of terahertz radiation
are not per se available for clinical desktop usage. However,
NEELAKANTA AND SHARMA: CONCEIVING THz ENDOMETRIAL ABLATION 407
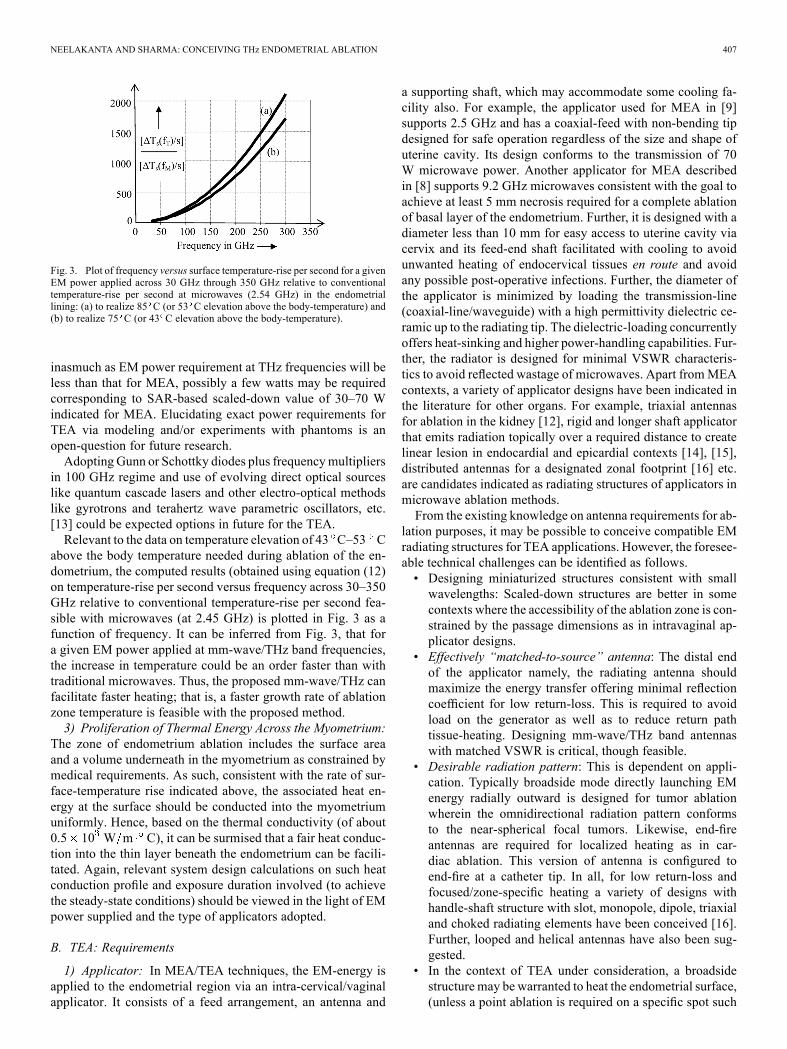
Fig. 3. Plot of frequency versus surface temperature-rise per second for a givenEM power applied across 30 GHz through 350 GHz relative to conventionaltemperature-rise per second at microwaves (2.54 GHz) in the endometriallining: (a) to realize 85 C (or 53 C elevation above the body-temperature) and(b) to realize 75 C (or 43 C elevation above the body-temperature).
inasmuch as EM power requirement at THz frequencies will beless than that for MEA, possibly a few watts may be requiredcorresponding to SAR-based scaled-down value of 30–70 Windicated for MEA. Elucidating exact power requirements forTEA via modeling and/or experiments with phantoms is anopen-question for future research.Adopting Gunn or Schottky diodes plus frequencymultipliers
in 100 GHz regime and use of evolving direct optical sourceslike quantum cascade lasers and other electro-optical methodslike gyrotrons and terahertz wave parametric oscillators, etc.[13] could be expected options in future for the TEA.Relevant to the data on temperature elevation of 43 C–53 C
above the body temperature needed during ablation of the en-dometrium, the computed results (obtained using equation (12)on temperature-rise per second versus frequency across 30–350GHz relative to conventional temperature-rise per second fea-sible with microwaves (at 2.45 GHz) is plotted in Fig. 3 as afunction of frequency. It can be inferred from Fig. 3, that fora given EM power applied at mm-wave/THz band frequencies,the increase in temperature could be an order faster than withtraditional microwaves. Thus, the proposed mm-wave/THz canfacilitate faster heating; that is, a faster growth rate of ablationzone temperature is feasible with the proposed method.3) Proliferation of Thermal Energy Across the Myometrium:
The zone of endometrium ablation includes the surface areaand a volume underneath in the myometrium as constrained bymedical requirements. As such, consistent with the rate of sur-face-temperature rise indicated above, the associated heat en-ergy at the surface should be conducted into the myometriumuniformly. Hence, based on the thermal conductivity (of about0.5 10 W m C), it can be surmised that a fair heat conduc-tion into the thin layer beneath the endometrium can be facili-tated. Again, relevant system design calculations on such heatconduction profile and exposure duration involved (to achievethe steady-state conditions) should be viewed in the light of EMpower supplied and the type of applicators adopted.
B. TEA: Requirements
1) Applicator: In MEA/TEA techniques, the EM-energy isapplied to the endometrial region via an intra-cervical/vaginalapplicator. It consists of a feed arrangement, an antenna and
a supporting shaft, which may accommodate some cooling fa-cility also. For example, the applicator used for MEA in [9]supports 2.5 GHz and has a coaxial-feed with non-bending tipdesigned for safe operation regardless of the size and shape ofuterine cavity. Its design conforms to the transmission of 70W microwave power. Another applicator for MEA describedin [8] supports 9.2 GHz microwaves consistent with the goal toachieve at least 5 mm necrosis required for a complete ablationof basal layer of the endometrium. Further, it is designed with adiameter less than 10 mm for easy access to uterine cavity viacervix and its feed-end shaft facilitated with cooling to avoidunwanted heating of endocervical tissues en route and avoidany possible post-operative infections. Further, the diameter ofthe applicator is minimized by loading the transmission-line(coaxial-line/waveguide) with a high permittivity dielectric ce-ramic up to the radiating tip. The dielectric-loading concurrentlyoffers heat-sinking and higher power-handling capabilities. Fur-ther, the radiator is designed for minimal VSWR characteris-tics to avoid reflected wastage of microwaves. Apart fromMEAcontexts, a variety of applicator designs have been indicated inthe literature for other organs. For example, triaxial antennasfor ablation in the kidney [12], rigid and longer shaft applicatorthat emits radiation topically over a required distance to createlinear lesion in endocardial and epicardial contexts [14], [15],distributed antennas for a designated zonal footprint [16] etc.are candidates indicated as radiating structures of applicators inmicrowave ablation methods.From the existing knowledge on antenna requirements for ab-
lation purposes, it may be possible to conceive compatible EMradiating structures for TEA applications. However, the foresee-able technical challenges can be identified as follows.• Designing miniaturized structures consistent with smallwavelengths: Scaled-down structures are better in somecontexts where the accessibility of the ablation zone is con-strained by the passage dimensions as in intravaginal ap-plicator designs.
• Effectively “matched-to-source” antenna: The distal endof the applicator namely, the radiating antenna shouldmaximize the energy transfer offering minimal reflectioncoefficient for low return-loss. This is required to avoidload on the generator as well as to reduce return pathtissue-heating. Designing mm-wave/THz band antennaswith matched VSWR is critical, though feasible.
• Desirable radiation pattern: This is dependent on appli-cation. Typically broadside mode directly launching EMenergy radially outward is designed for tumor ablationwherein the omnidirectional radiation pattern conformsto the near-spherical focal tumors. Likewise, end-fireantennas are required for localized heating as in car-diac ablation. This version of antenna is configured toend-fire at a catheter tip. In all, for low return-loss andfocused/zone-specific heating a variety of designs withhandle-shaft structure with slot, monopole, dipole, triaxialand choked radiating elements have been conceived [16].Further, looped and helical antennas have also been sug-gested.
• In the context of TEA under consideration, a broadsidestructure may be warranted to heat the endometrial surface,(unless a point ablation is required on a specific spot such
408 IEEE TRANSACTIONS ON TERAHERTZ SCIENCE AND TECHNOLOGY, VOL. 3, NO. 4, JULY 2013
as a polyp). In such cases, matched antenna designs can beconceived as sleeve versions as indicated, for example in[17], [18]. Thus, despite of technical challenges conceivingapplicators/antennas for TEA is feasible.
• Cooling the applicator: In MEA/TEA as well as in otherablation techniques, avoidance of incidental heating ofnearby tissues is required. For this purpose, typicallycooling-jackets (carrying water) are improvised consistentwith applicator dimensions, if the jacket does not prohibi-tively augment the size of the applicator. Other cryogeniccooling is also doable. In TEA, since the applicator isdown-sized, accommodating appropriate, smaller coolingsystem is conceivable and advantageous.
• Transmural considerations: In certain ablation efforts,heating of a certain zone will be implicated by a largefluid flow on the other side of the associated anatomicalwall, typically as in cardiac ablation. In such transmuralsituations, use of ablation would warrant special consider-ations regardless of using microwaves or THz. However,in TEA such transmural implication is not indicated.
C. TEA: Technical Challenges
Experimental/Clinical Studies: To the best of authors’knowledge, no known studies on TEA have been reported.This may be due to the fact that no known frequency band hasbeen formally specified as a standard for ablation applicationsin mm-wave/THz band. (though use of 120 and 380 THz andmid-infrared 12–120 THz are indicated in medical imaging toachieve high resolutions). As such, the effort addressed hereis a heuristic proposal yet to be investigated via experimentalstudies so as to elucidate the underlying technical challenges.At least, modeling uterus and endometrium with bio-phantommaterials and designing an appropriate applicator system atsome mm-wave/THz frequency can be the first step; and, it isbeing planned by the authors in the near future.Knowledge on athermal effects due to mm-wave/THz fre-
quencies (such as invasive interactions at DNA level causingpossible damages to genes expression) is currently sparse [19].Futuristic studies thereof are necessary and relevant considera-tions should duly be specified in TEA designs vis-à-vis the pro-cedure time (of exposure) and intensity of EM power sourcerequirements.
VII. CLOSURE
In short, the present study offers a proposal to evaluate thefeasibility of using mm-wave/THz band EM-energy for the pur-pose of ablation techniques. Specifically, the endometrial ab-lation is considered and preliminary details on the proposedstrategy are outlined.
REFERENCES
[1] S. L. Gaynor, G. D. Byrd, M. D. Diodato, Y. Ishii, A. M. Lee, S.M. Prasad, J. Gopal, R. B. Schuessler, and R. J. Damiano, Jr, “Mi-crowave ablation for atrial fibrillation: Dose-response curves in the car-dioplegia-arrested and beating heart,” Annu. Thorac. Surgery, vol. 81,no. 1, pp. 72–76, Jan. 2006.
[2] C. J. Simon, D. E. Dupuy, and W. W. Mayo-Smith, “Microwaveablation: Principles and applications,” Radio Graphics, vol. 25, pp.S69–S83, Oct. 2005.
[3] P. S. Neelakanta, Handbook of Electromagnetic Materials: Monolithicand Composite Versions and Their Applications. Boca Raton, FL:CRC, 1995, pp. 570–582.
[4] P. S. Neelakanta and K. P. Ramakrishnan, “Microwave-induced haz-ardous non-linear thermoelastic vibrations of the ocular lens in thehuman eye,” J. Biomechanics, vol. 12, no. 3, pp. 205–210, 1979.
[5] P. S. Neelakanta, “Microwave-induced injurious effects on the human-embryo in utero,” Biomed. Techn., vol. 23, no. 11, pp. 263–269, 1978.
[6] P. S. Neelakanta, “Electromagnetic heating in a model of frozen redblood-cells, Rep. III IPGA assignment,” Naval Aerospace Med. Lab.,Pensacola, FL, 1988.
[7] P. S. Neelakanta, “Rewarming of hypothermic human-limbs in vivo byRF induction heating: Theoretical considerations, Rep. II IPGA assign-ment,” Naval Aerospace Med. Lab., Pensacola, FL, 1988.
[8] I. B. Feldberg and N. J. Cronin, “A 9.2 GHz microwave applicatorfor the treatment of menorrhajia,” in 1988 IEEE MTT-S Int. Symp.,Baltimore, MD, 1998, pp. 755–758.
[9] S. Yeasmin, K. Nakayama, M. Ishibashi, A. Katagiri, K. Iida, N.Nakayama, S. Aoki, Y. Kanaoka, and K. Miyazaki, “Microwaveendometrial ablation as an alternative to hysterectomy for the emer-gent control of uterine bleeding in patients who are poor surgicalcandidates,” Arch. Gynecol. Obstet., vol. 280, no. 2, pp. 279–282,Aug. 2009.
[10] L. Mettler, “Long-term results in the treatment of menorrhajia and hy-permenorrhea with a thermal balloon endometrial ablation technique,”J. Soc. Laproendosc. Surgeons, vol. 6, pp. 305–309, 2002.
[11] E. Buckingham, “Model experiments and the form of empirical equa-tions,” Trans. ASME, vol. 37, pp. 263–296, 1915.
[12] P. F. Laeseke, F. T. Lee, Jr., L. A. Sampson, D. W. van der Weide,and C. L Brace, “Microwave ablation versus radiofrequency ablationin the Kidney: High power triaxial antennas create larger ablation zonesthan the similarly sized internally cooled electrodes,” J. Vasc. Interv.Radiol., vol. 20, no. 9, pp. 1224–1229, Sep. 2009.
[13] J. Yao, X. Degang, S. Bo, and L. Huan, “Tera-HZ radiation source bydeference frequency generation (DFG) and TPO with all solid statelasers,” Terahertz Sci. and Technol., vol. 1, no. 3, pp. 161–168, Sep.2008.
[14] A. E. Saltman, “Completely endoscopic microwave ablation of atrialfibrillation on the beating heart using bilateral thoracoscopy. clinicaltechniques,” Jul. 2005 [Online]. Available: http://www.ctsnet.org/sec-tions/clinicalresources/adultcardiac/expert_tech-11.html
[15] A. E. Saltman, “Microwave ablation: A new use for an old technology,”Bus. Briefing: US Cardiol., vol. 1, no. 1, pp. 1–7, 2004.
[16] C. L. Brace, “Microwave tissue ablation: Biophysics, technology andapplications,” Crit. Rev. Biomed. Eng., vol. 38, no. 1, pp. 65–78, 2010.
[17] T. S. Bird and G. L. James, “Input mismatch of mode coaxialwaveguide feeds,” IEEE Trans. Antennas Propag., vol. AP-34, no. 8,pp. 1030–1033, Aug. 1986.
[18] T. S. Bird, “ mode excitation of flanged circular axial coaxialwaveguide with an extended center conductor,” IEEE Trans. AntennasPropag., vol. AP-35, no. 32, pp. 1358–1366, Dec. 1987.
[19] B. S. Alexandrov, V. Gelev, A. R. Bishop, A. Usheva, and K. O. Ras-mussen, “DNA breathing dynamics in the presence of a terahertz field,”Phys. Lett. A, vol. 374, no. 10, pp. 1214–1217, Feb. 2010.
Perambur S. Neelakanta received the Ph.D. degree in electrical engineeringfrom Indian Institute of Technology (IIT), Madras, India, in 1975.Since 1988, he has been with the Department of Electrical and Computer
Engineering and Computer Science, Florida Atlantic University (FAU), BocaRaton, FL, USA, where he is currently a Professor He has 37 years of aca-demic and 5 years of corporate experience. He has published over 150 journalpapers and 6 books, 3 of which are in the area of telecommunications and one inEMmaterials. His research interests include bioengineering, bioinformatics andcomplex systems, wireline and wireless telecommunications, electromagneticsand EM-materials, stochastical communication theory, and information-theo-retics in neural networks.Dr. Neelakanta is a Fellow of IET (U.K.) and a Chartered Engineer.
Bharti Sharma (S’12) received the B.E. degree in electronics and telecommu-nications from University of Pune, Pune, India, and is currently working towardthe Ph.D. degree at Department of Electrical and Computer Engineering andComputer Science, Florida Atlantic University (FAU), Boca Raton, FL, USA.Following her Bachelor’s degree, she worked as a Lecturer at the Delhi Col-
lege of Engineering, New Delhi, India. Subsequently, she joined Florida Power& Light Company as a Systems Analyst.