27
Congenital malformation of the reproductive organs Absence of vagina Uterine malformation Fallopian tube and ovary
Congenital malformation of the reproductive organs
Absence of vagina
Uterine malformation
Fallopian tube and ovary
Absence of vagina
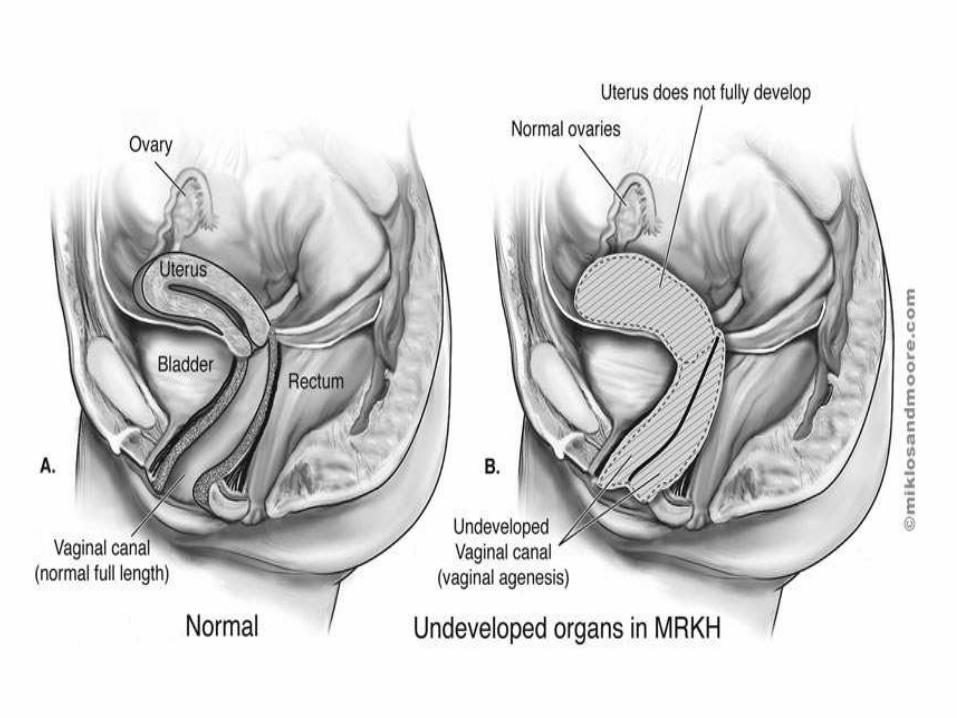
• Congenital absence of vagina is also known as"Rokitansky- Mayer – Hauser - Kuster Syndrome".Patients with this syndrome have a normal femalekaryotype. They typically present at the age ofmenarche or later because of primary amenorrheoa.Rarely is the abnormality discovered at birth. Onphysical examination findings include a normal vulvawith absent vagina or vagina represented by a dimple.There is usually absence of uterus and cervix. Theovaries are normal and there is normal cyclical ovarianfunction as reflected by circulating hormone levels andovulation and the fallopian tubes may or may not benormal but complete absence is rare.
Clinical features
• Absent vagina
• Absence of menstrual period
• Absent uterus and other reproductive organ
• Kidney abnormalities
• Skeletal abnormalities
• Hearing loss

Diagnosis Since outward genitalia appear normal, vaginalagenesis is not usually diagnosed until puberty.Typically, an adolescent girl 15 to 18 years oldconsults a pediatrician or gynecologist when herperiod does not start. The condition may also bediscovered in infancy or childhood whileinvestigating kidney, skeletal or other abnormalities,such as the absence of an anal opening.
Ultrasound – reveals if the uterus and ovaries arepresent and the presence and location of kidneys.
MRI – shows a more detailed picture of thereproductive tract and kidneys.

Treatment
Most young women are treated in their late teens orearly 20s. Others may wait until they are older andsexually active. Treatment is not urgent, but it is usuallynecessary before sexual intercourse.• Self dilation: some patients can create a vagina without
surgery using self dialation. In this treatment, thepatient presses a small rod (dialator) against the skin orthe small vagina for 15 to 20 minutes per day. This isoften done after bathing, when skin is more pliable.Progressively larger dilators are used to expand thevagina. Several month may be required to obtain thedesired result.
• Cont.….• Surgery (vaginoplasty): Surgery (vaginopalsty) is
used to create a functional vagina. Thesetreatments are usually delayed until the patientpossesses the maturity to handle follow updilation.
• Skin graft(McIndoe procedure)- The McIndoeprocedure) is the most commonly performedvaginal plasty. The procedure uses the skin graftfrom the buttock(which leaves only adisfigurement). The surgeon makes an incisionwhere the vagina would normally developed andinserts the graft to create a vagina. A mold isplaced in the newly formed vagina for seven days.
Cont…
• Counseling: it is often useful for a patient tospeak with a counselor about her condition. Aftertreatment patient can have a normal sex life.Although it is not common some patients havenormal uterus and can bear children. Typically,vaginal absence patients have undersized uterusand cannot become pregnant. However, if theirovaries are healthy, which is often the case,affected woman can have children by INF of theirown eggs with the pregnancy carried by asurrogate mother.
Uterine Malformation
• A uterine malformation is a type of femalegenital malformation resulting from anabnormal development of the Müllerianduct(s) during embryogenesis. Symptomsrange from amenorrhea, infertility, recurrentpregnancy loss, and pain, to normalfunctioning depending on the nature of thedefect.
Prevalence
• The prevalence of uterine malformation isestimated to be 6.7% in the generalpopulation, slightly higher (7.3%) in theinfertility population, and significantly higherin a population of women with a history ofrecurrent miscarriages (16%).
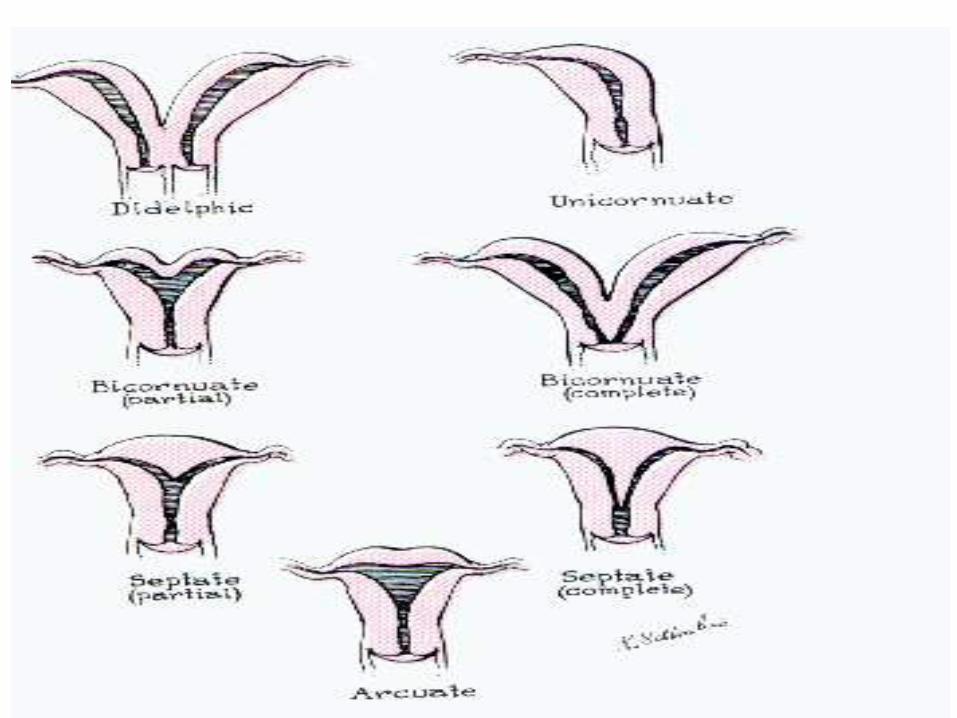

Types of uterine malformation
• Class I: hypoplasia/agenesis (absent uterus).Combined agenisis of the Uterus, cervix andupper portion of vagina. The condition is alsocalled Mayer-Rokitansky-Kuster-Hauser syndrome.The patient with MRKH syndrome will haveprimary amenorrhea. Patients have noreproductive potential aside from medicalintervention in the form of invirto fertilization ofharvested ova and implantation in a host uterus.
• Class II: Unicornuate uterus (a one-sided uterus).Only one side of the Müllerian duct forms. Theuterus has a typical "penis shape" on imagingsystems. Unicornuate Uterus
• If a woman has a Unicornuate uterus, she will have asingle uterine cavity with a cervix and one fallopiantube coming off of the uterus. In this malformation,the uterus only forms half-way. The other side of theuterus may have a rudimentary horn. An ultrasoundcan be used to find a Unicornuate uterinemalformation. Further diagnostic test used toconfirm this diagnosis are; hysteroscopy, ultrasound,and laparoscopy.
• Excision of rudimentari horn by Surgical procedure.
Cont.…
• Unfortunately, a woman with this malformation canhave much risk if she becomes pregnant. There is agreat risk of pregnancy loss and preterm labor. Also,there is a chance of the woman having an ectopicpregnancy. The common miscarriages due to thismalformation are caused by abnormalities in the bloodsupply of the uterus. The reason that there is a greatrisk for preterm labor is due to space restrictions in theUnicornuate uterus. Furthermore, for the woman withthe rudimentary horn, she will have greater risksassociated with pregnancy. This horn will cause a lot ofspace restriction which could result in ectopicpregnancy. This is the reason that most doctorsrecommend surgery to remove the rudimentary horn.
• Class III: Uterus Didelphys: A woman with adidelphic uterus has a duplication of the uterusand a duplication of the cervix. In thismalformation, there are two uterine cavities andtwo cervixes accompanying each cavity. It is notrecommended that a woman have surgery toconnect the two uteruses together. Women withthis malformation may be asymptomatic. Themalformation is normally found with a pelvicexamination. There are two common complaintsof women that have a didelphic uterus. There arecomplaints of dysmenorrheal (uterine pain duringmenstruation) and complaints of dyspareunia(painful sexual intercourse).
Cont…• Class IV: The bicornuate (heart-shaped) uterus has a
marked indentation and is separated into two differentcavities. This malformation is a result from the uterusforming improperly in the woman’s early prenataldevelopment. The way that a woman can confirm thatshe has a bicornuate uterus is by having an ultrasoundor by the use of laparoscopy. The primary risk withhaving a bicornuate uterus is preterm labor andcervical insufficiency. The cervical insufficiency couldcause the woman to have a miscarriage during thesecond trimester of pregnancy. The good news is thatthere is a chance that the baby can still survive.Furthermore, in some cases, a woman with this type ofuterine malformation can carry the baby to full termwith no complications. It just varies from person toperson.

• Class V: Septated uterus (uterine septum or partition).
• A woman with a septate uterine malformation willhave the problem from which the septum separatesthe uterine cavity into two separate cavities. Theseptum will arise at the top of the uterine cavity andthen extend down to the cervix and the vagina. It isnormally recommended that a woman with thismalformation have a simple out patient surgicalremoval of the septum.
• There is a risk of miscarriage associated with a septateuterine malformation. Furthermore, there is a chanceof preterm labor. Doctors can normally find a septateuterine malformation with the use of an ultrasound.However, to confirm the diagnosis, the woman willneed to have a hysteroscopy performed.
• Class VI(arcuate uterus):The arcuate uterushas a depression at the fundus. A woman withan arcuate uterus can carry a baby to full termpregnancy. However, this condition isassociated with a higher risk for miscarriageand premature births. The best way for awoman to find if she has this malformation isthrough transvaginal ultrasonography,hysterosalpingography, MRI, or hysteroscopy.In most cases, the woman will not have anyreproductive problems. For those that do havereproductive tribulations, there is the optionto have a hysteroscopic resection performed.
Cont.…• Class VI: DES uterus. Several women were treated
with diethylstilbestrol(DES), an estrogenanolouge prescribed to prevent miscarriage from1945-1971. The drug was withdrawn once itsteratogenic effects on the reproductive tracts ofmale and female foetus were understood. Theuterine anomaly is seen in the female as many as15% of women exposed to DES during pregnancy.Female fetuses who are affected have a variety ofabnormal findings that include uterinehypoplasia and a T- shaped uterine cavity.
• Patients with uterine abnormalities may haveassociated renal abnormalities includingunilateral renal agenesis.
Diagnosis
• Physical examination
• TAS and TVS
• Hysterosalpingography(HSG)
• MRI and CT scan
Clinical features
• Gynaecological impact
Infertility and dyaparaunia are offen seen in vaginal septum.
Dysmenorrhoea in bicornuate uterus or due to cryptomenorrhoea.
Menorrhagia also may occur in bicornuate uterus.
Obstetrical impact
Infertility
Early abortion
Ectopic pregnancy
Late abortion or premature abortion
IUGR
Management During pregnancy• When the diagnosis of uterine malformation is
made at the beginning of pregnancy, thetreatment can be only preventive(setting at rest,sonographic monitoring of the fetal growth andthe cervical competence). Cervical cerclageshould be proposed only in the case of provedcervical incompetence observed in 1/3 to ¼ ofuterine malformations.
• Abdominal mertoplasty could be done either byexcising the septum or by incising the septum.The success rate of abdominal metroplasy interms of live birth is 5-75%. Nowadayshysteroscopy metroplasty is done for thiscondition.
Abnormalities of the fallopian tube
• The fallopian tubes may be unduly elongated,may have accessory ostia or diverticula.Rarely, the tube may be absent on one side.These conditions may lower the fertility orfavour ectopic pregnancy.
Abnormalities of Ovaries
The congenital anomaly of the ovaries includescongenital absence of ovary and developmentaloverian cyst. Accessory ovary (division oforiginal ovary into two) also comes under thiscondition. Rarely, supernumerary ovaries maybe found in the broad ligaments.
Thank You

















