24
Congenital Heart Disease By: Dr Ismah, Pediatric Department 1
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | snich |
| View: | 219 times |
| Download: | 4 times |
Congenital Heart Disease
By: Dr Ismah, Pediatric Department
1

OUTLINE• Epidemiology
• Anatomy
• Types
• Clinical approach
- History, physical exams
- Investigation
- General management
2

EPIDEMIOLOGY
• CHDs affect nearly 1% of or about 40,000 births per year in the United States
• The most common type of heart defect is a ventricular septal defect (VSD)
• About 95% of babies born with a non-critical CHD are expected to survive to 18 years of age [2012]
• About 69% of babies born with critical CHDs are expected to survive to 18 years of age [2012]
http://www.cdc.gov
• A study on under five deaths in Malaysia in the year 2006 showed that 10% of mortality was
directly related to CHD - http://mjpch.com
3

ANATOMY
http://www.stanfordchildrens.org
4

www.rch.org.au5

TYPES
Acyanotic Cyanotic
• Atrial septal defects (ASD)
• Ventricular septaldefects (VSD)
• Patent ductusarteriosus (PDA)
• Tetralogy of Fallot(TOF)
• Tricuspid atresia (TA)
• Transposition of the great vessels
6

7

Atrial Septal Defect
• Most commonly asymptomatic
• Features:
- Right ventricular heave
- S2 widely split and usually fixed
- Grade I-III/VI systolic murmur at the upper left sternal border
- Cardiac enlargement on CXR
8http://www.merckmanuals.com

Treatment
Small defects:
• No treatment
Large defects:
• Elective closure at 4-5 years age
9 Paeds Protocol 3rd Ed
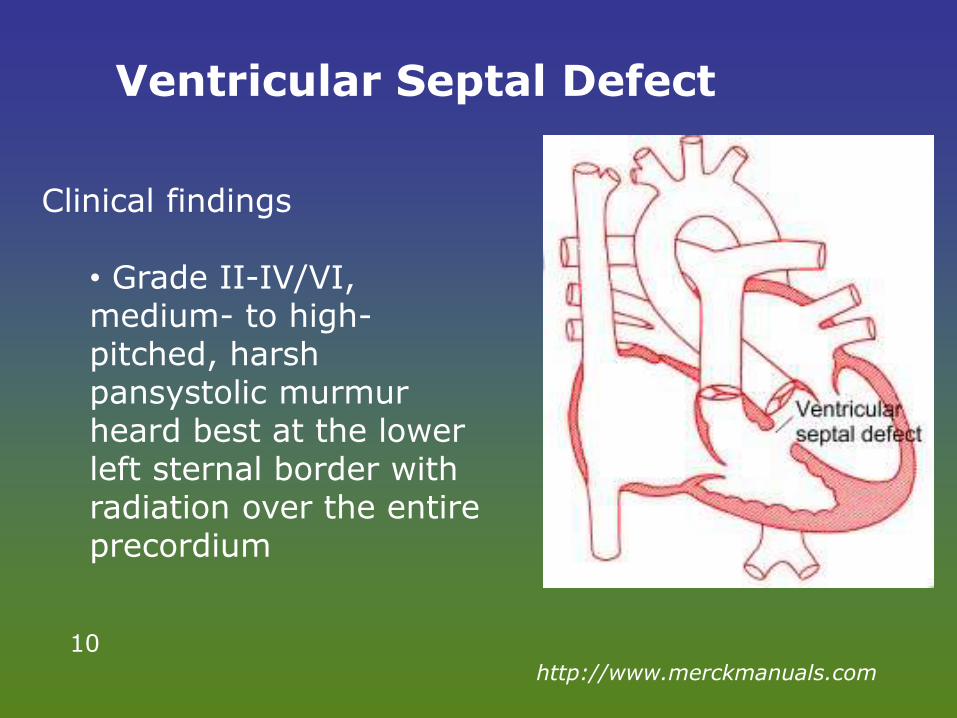
Ventricular Septal Defect
Clinical findings
• Grade II-IV/VI, medium- to high-pitched, harsh pansystolic murmur heard best at the lower left sternal border with radiation over the entire precordium
10http://www.merckmanuals.com

Treatment Small defects: Moderate defects: Large
defects:
No treatment; high rate of spontaneous closure. • SBE prophylaxis. • Yearly follow up for aortic valve prolapse, regurgitation. • Surgical closure indicated if prolapsed aortic valve.
- Anti-failure therapy if heart failure. - Surgical closure if:
• Heart failure not controlled by medical therapy. • Persistent cardiomegaly on chest X-ray. • Elevated pulmonary arterial pressure. • Aortic valve prolapse or regurgitation. • One episode of infective endocarditis.
Early primary surgical closure. • Pulmonary artery banding followed by VSD closure in multiple VSDs.
11 Paeds Protocol 3rd Ed

Patent Ductus Arteriosus
• Pulses are bounding and pulse pressure is widened
• Characteristically has continuous murmur is heard best in the upper left sternal border, machinery murmur
12
http://www.merckmanuals.com

Treatment
Small PDA:
• No treatment if there is no murmur
• If murmur present: elective closure as risk of endarteritis.
Moderate to large PDA:
• Anti-failure therapy if heart failure
• Timing, method of closure (surgical vstranscatheter) depends on symptom severity, size of PDA and body weight.
13 Paeds Protocol 3rd Ed

Tetralogy of Fallot
14http://my.clevelandclinic.org
Typical features
• Symptoms include cyanosis, dyspnea with feeding, poor growth, and
• Hypercyanotic "tet" spells (sudden, potentially lethal episodes of severe cyanosis)
• A harsh systolic murmur at the left upper sternal border with a single 2nd heart sound (S2) is common
15http://www.merckmanuals.com

Transposition of great arteries
16
http://mvpresource.com
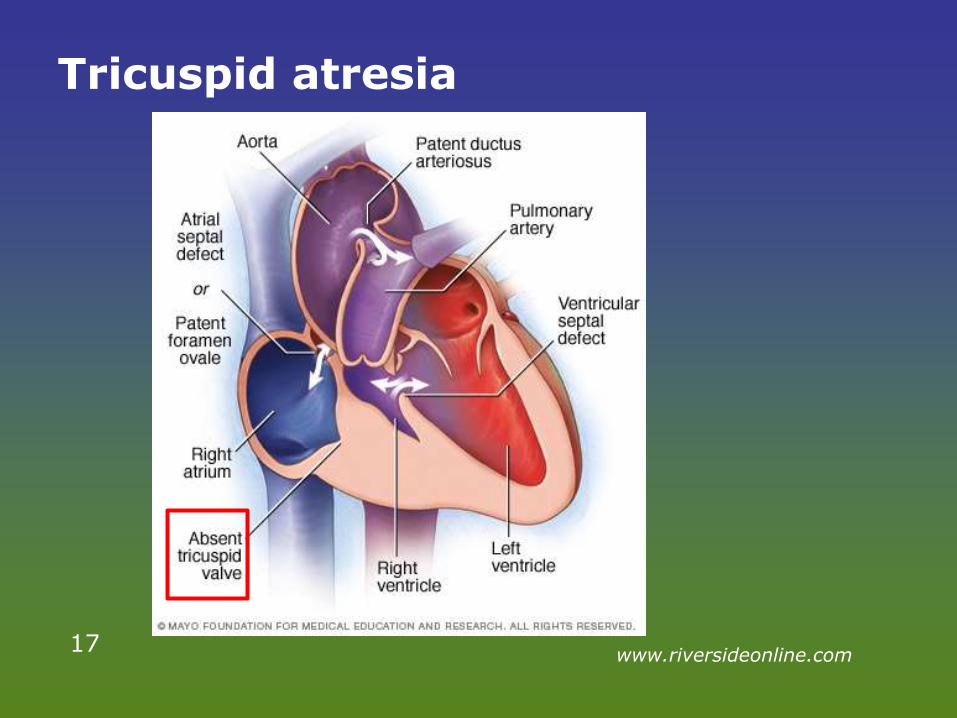
Tricuspid atresia
17www.riversideonline.com

HISTORY
• Antenatal scans (cardiac malformation, fetal arrhythmias, hydrops).
• Family history of congenital heart disease.
• Maternal illness: diabetes, rubella, teratogenicmedications.
• Perinatal problems: prematurity, meconiumaspiration, perinatal asphyxia.
18 Paeds Protocol 3rd Ed

PHYSICAL EXAMINATIONS
• Dysmorphism: Trisomy 21, 18, 13; Turner syndrome
• Central cyanosis.
• Tachypnoea.
• Weak or unequal pulses.
• Heart murmur.
• Hepatomegaly.
19 Paeds Protocol 3rd Ed

INVESTIGATIONS
- CXR
- Hyperoxia test:
• Administer 100% oxygen via headbox at 15 L/min for 15 mins.
• ABG taken from right radial artery.
• Cyanotic heart diseases: pO₂ < 100 mmHg; rise in pO₂ is < 20 mmHg.
- Echocardiography
20 Paeds Protocol 3rd Ed

GENERAL MANAGEMENT
• Correct metabolic acidosis, electrolyte
derangements, hypoglycaemia; prevent
hypothermia.
• Empirical treatment with IV antibiotics.
• Early cardiology consultation.
21 Paeds Protocol 3rd Ed
• IV Prostaglandin E infusion if duct-dependent lesions suspected:
- Starting dose: 10 – 40 ng/kg/min; maintenance: 2 – 10 ng/kg/min.
- Adverse effects: apnoea, fever, hypotension.
22

• If unresponsive to IV prostaglandin E, consider:
- Transposition of great arteries, obstructed total anomalous pulmonary.
- Blocked IV line.
- Non-cardiac diagnosis.
• Arrangement to transfer to regional cardiac center once stabilized.
23

THANK YOU
24












