25
| Date post: | 15-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | drmanish-kumar |
| View: | 55 times |
| Download: | 3 times |


Congenital Inguinal HerniaCongenital Inguinal Hernia Indirect Inguinal Hernia Indirect Inguinal Hernia
Continued patency of the Processus Continued patency of the Processus Vaginalis Vaginalis
Patent PV sac is potential Patent PV sac is potential hernia/hydrocoelehernia/hydrocoele
In hernia the sac is wider & contains an In hernia the sac is wider & contains an intraabdominal structureintraabdominal structure
In hydrocoele the sac is narrow & In hydrocoele the sac is narrow & contains only peritoneal fluidcontains only peritoneal fluid

Processus VaginalisProcessus Vaginalis . . . . . . PV develops during12th wk of gestation PV develops during12th wk of gestation
Out pouching of the peritoneal cavity through Out pouching of the peritoneal cavity through the internal ringthe internal ring
PV plays an integral role in the descent of testesPV plays an integral role in the descent of testes
PV obliterates spontaneously from the deep ring PV obliterates spontaneously from the deep ring to the testisto the testis
possible role of CGRP in fusion of PVpossible role of CGRP in fusion of PV
Distal portion persists as tunica vaginalisDistal portion persists as tunica vaginalis

At birth PV is patent in up to 80% At birth PV is patent in up to 80% infants.infants.


IncidenceIncidence 0.8 – 4 %0.8 – 4 %
Highest in 1st year of lifeHighest in 1st year of life
Incidence in premature infants 16 – Incidence in premature infants 16 – 25%25%
M:F is 6:1M:F is 6:1
Right 60%, Left 30%, Bilateral 10%Right 60%, Left 30%, Bilateral 10%

Factors contributing to Factors contributing to development of herniadevelopment of hernia
Undescended testisUndescended testis Increased peritoneal fluid :Increased peritoneal fluid : Ascites, VP shuntAscites, VP shunt
Increased abdominal pressure :Increased abdominal pressure : Severe ascites, Meconium peritonitis,Severe ascites, Meconium peritonitis,
post repair of Exomphalos / CDHpost repair of Exomphalos / CDH
Chronic respiratory disease :Chronic respiratory disease : Cystic fibrosisCystic fibrosis
Connective tissue disorders:Connective tissue disorders: Ehlers –Danlos, Marfans, MucopolysaccharidosisEhlers –Danlos, Marfans, Mucopolysaccharidosis

Clinical FeaturesClinical Features Bulge in inguinal area extending towards / Bulge in inguinal area extending towards /
into scrotum with crying / straining into scrotum with crying / straining
may be present at birth or appear latermay be present at birth or appear later
reduces in size when the child is relaxed / reduces in size when the child is relaxed / asleepasleep
smooth soft-firm mass that emerges from the smooth soft-firm mass that emerges from the external ring lateral and above pubic tubercle, external ring lateral and above pubic tubercle, enlarges with increased abdominal pressureenlarges with increased abdominal pressure

Can be reduced with gentle pressure, Can be reduced with gentle pressure, may reduce with gurgling noisemay reduce with gurgling noise
Examine position of testis – Examine position of testis – undescended / retractileundescended / retractile
Reappears on crying / valsalva Reappears on crying / valsalva (blowing a balloon / coughing ) (blowing a balloon / coughing ) preferably while standingpreferably while standing
Thickening & silkiness on palpating the Thickening & silkiness on palpating the cord as it crosses pubic tubercle – cord as it crosses pubic tubercle – Silk Silk Glove signGlove sign
If in doubt re-evaluate at second visitIf in doubt re-evaluate at second visit

ManagementManagement Inguinal hernia does not resolve Inguinal hernia does not resolve
spontaneouslyspontaneously
Must be operated because of high Must be operated because of high risk of incarcerationrisk of incarceration
Operation : Operation : HerniotomyHerniotomy - High suture ligation - High suture ligation
of the sac at the internal ringof the sac at the internal ring
Open technique / LaparoscopyOpen technique / Laparoscopy

Technique Technique Anaesthesia:Anaesthesia:
In infants – ETGAIn infants – ETGA
Older children – facial or laryngeal Older children – facial or laryngeal maskmask
Transverse groin skin crease Transverse groin skin crease incision incision
Open layersOpen layers Incision in external oblique Incision in external oblique
aponeurosis lateral to external ring aponeurosis lateral to external ring
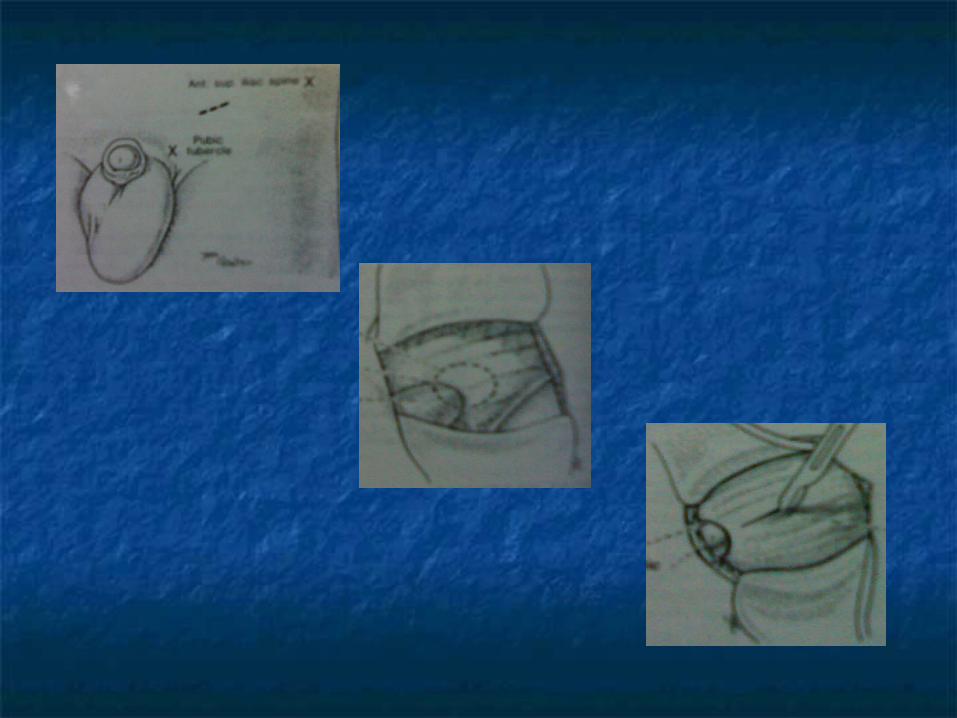

Fibres of cremasteric fascia are Fibres of cremasteric fascia are separatedseparated
Shiny glistening white hernial sac Shiny glistening white hernial sac identified & lifted with blunt forcepsidentified & lifted with blunt forceps
In males the sac lies anterior & medial In males the sac lies anterior & medial to vas & vesselsto vas & vessels
Vas & vessels are never held with Vas & vessels are never held with
forceps, dissected off the sac with forceps, dissected off the sac with overlying areolar tissueoverlying areolar tissue


In females there are no significant structures In females there are no significant structures other than round ligament of uterusother than round ligament of uterus
Ensure there are no contents in the sac, divide Ensure there are no contents in the sac, divide between clampsbetween clamps
Dissect proximally upto neck of the sacDissect proximally upto neck of the sac
Twist the proximal sac & transfix the neck at Twist the proximal sac & transfix the neck at the level of deep ringthe level of deep ring
Traction on the testis to return it to the scrotumTraction on the testis to return it to the scrotum
Closure in layers Closure in layers

Contralateral explorationContralateral exploration Selected contralateral exploration:Selected contralateral exploration: Age:Age: 40% contralateral hernias occur after unilateral 40% contralateral hernias occur after unilateral
surgery in children under 1 yrsurgery in children under 1 yr
Side of hernia:Side of hernia: Left Left
Sex:Sex: Female Female
Patency of PV sac on opposite side:Patency of PV sac on opposite side: Herniography, Herniography, intraoperative pnuemoperitoneum, Choledochoscope / intraoperative pnuemoperitoneum, Choledochoscope / laparoscopelaparoscope
Conditions predisposing to hernia on the opposite side:Conditions predisposing to hernia on the opposite side: VP Shunt, connective tissue disordersVP Shunt, connective tissue disorders
Poor risk for GAPoor risk for GA
Irreducible HerniaIrreducible Hernia
Incarcerated hernia: contents cannot be Incarcerated hernia: contents cannot be easily reduced into peritoneal cavityeasily reduced into peritoneal cavity
Irritability, pain in the groin / abdomen, Irritability, pain in the groin / abdomen, vomitingvomiting
Tense, tender, non fluctuant mass in Tense, tender, non fluctuant mass in the groin, may extend into scrotum, the groin, may extend into scrotum, not transilluminantnot transilluminant
Bilious vomiting, abdominal distension Bilious vomiting, abdominal distension indicates obstruction of bowelindicates obstruction of bowel

Strangulated hernia: Tightly Strangulated hernia: Tightly constricted at the neck resulting in constricted at the neck resulting in ischemia of contents.ischemia of contents.
Pain intensifies, vomiting becomes Pain intensifies, vomiting becomes bilious. Blood in stoolsbilious. Blood in stools
Mass is tender, edema & reddening of Mass is tender, edema & reddening of overlying skin, feveroverlying skin, fever

Management:Management:
Non operative:Non operative: only when there is only when there is no e/o ischemiano e/o ischemia
Under sedation & analgesia reduce Under sedation & analgesia reduce the hernia by gentle compressionthe hernia by gentle compression
Elective herniotomy after 48 hrs by Elective herniotomy after 48 hrs by which time there is less edemawhich time there is less edema

Operative:Operative: When hernia cannot be When hernia cannot be reduced or hernia is strangulatedreduced or hernia is strangulated
Hernial sac opened. Look for viability Hernial sac opened. Look for viability of bowelof bowel
Deep ring can be enlarged by Deep ring can be enlarged by incising the arching fibres of conjoint incising the arching fibres of conjoint tendon superiorlytendon superiorly
Tell tale e/o ischemia – bloody or foul Tell tale e/o ischemia – bloody or foul smelling fluid in the sac. Explore the smelling fluid in the sac. Explore the abdomen abdomen

Complications of Complications of herniotomyherniotomy
Ascending / trapped testisAscending / trapped testis
Recurrence – 0.8%Recurrence – 0.8%
Injury to vasInjury to vas
Testicular atrophyTesticular atrophy

Congenital HydrocoeleCongenital Hydrocoele
Usually noted in early infancy, can occur Usually noted in early infancy, can occur at anytimeat anytime
Often bilateralOften bilateral
Soft, bluish, fluctuant swelling Soft, bluish, fluctuant swelling surrounding the testissurrounding the testis
Fluctuate in size: smaller at night when Fluctuate in size: smaller at night when the child is relaxedthe child is relaxed

Neck of the hydrocoele narrows at the Neck of the hydrocoele narrows at the external ring & usually does not extend external ring & usually does not extend into the inguinal canalinto the inguinal canal
Hallmark: Brilliant transilluminationHallmark: Brilliant transillumination
In most children with congenital In most children with congenital hydrocoele the PV sac closes and hydrocoele the PV sac closes and hydrocoele resolves between 12 – 24 hydrocoele resolves between 12 – 24 monthsmonths
There is no e/o hydrocoele will evolve into There is no e/o hydrocoele will evolve into herniahernia


ManagementManagement
Observation for first 2 years unless Observation for first 2 years unless large, painfullarge, painful
Herniotomy if it persists > 2 yrsHerniotomy if it persists > 2 yrs

















