55
S Congenital Infections The elephant in the room Fetal Medicine – Old and New Dr JL van der Merwe SASOG 2014

S
Congenital Infections
The elephant in the room Fetal Medicine – Old and New
Dr JL van der Merwe
SASOG 2014


S Originally TORCH complex
S Toxoplasmosis
S Other [T. pallidum]
S Rubellavirus
S Cytomegalovirus (CMV)
S Herpes Simplex Virus (HSV)
S Now also perpetrators….
S Parvovirus B19
S Varicella-zoster virus
S Hep B
S Plasmodium
S HIV
S Mycobacterium tuberculosis
S Listeria Monocytogenes, Enterovisuses, Borrelia burgdorferi (Lyme Disease) …
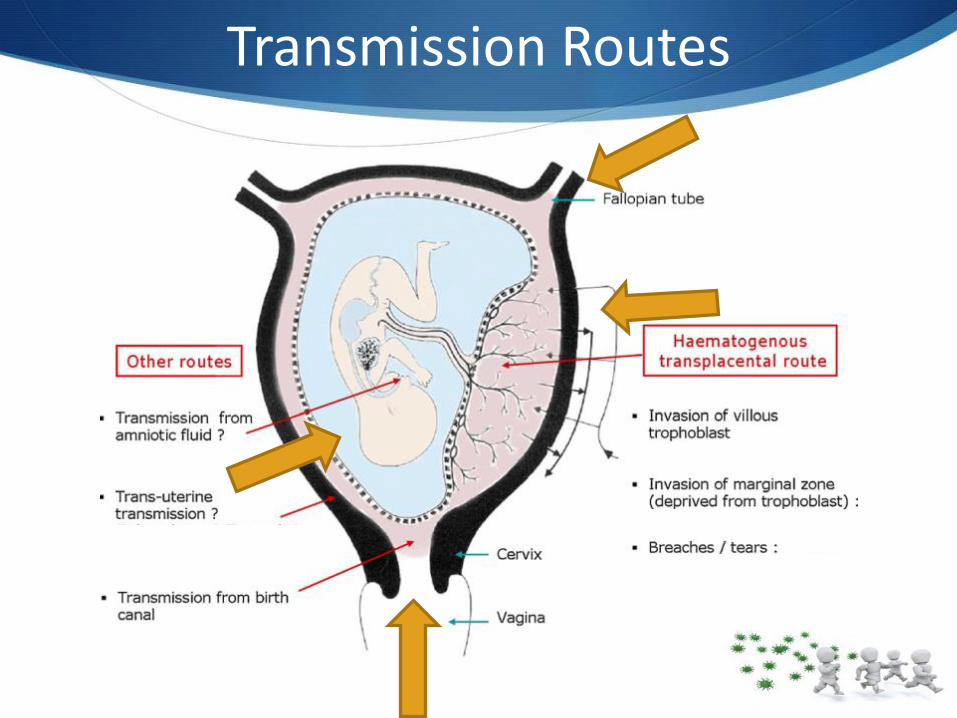
Transmission Routes

Transmission Timing

Manifestation influenced by…
Mode of acquisition
Maternal immunity
Timing (gestation)
Effect of pathogen on organogenesis
Fetal genetics
Teratogens:
• Varicella, Rubella
• CMV, HSV
• Influenza

S
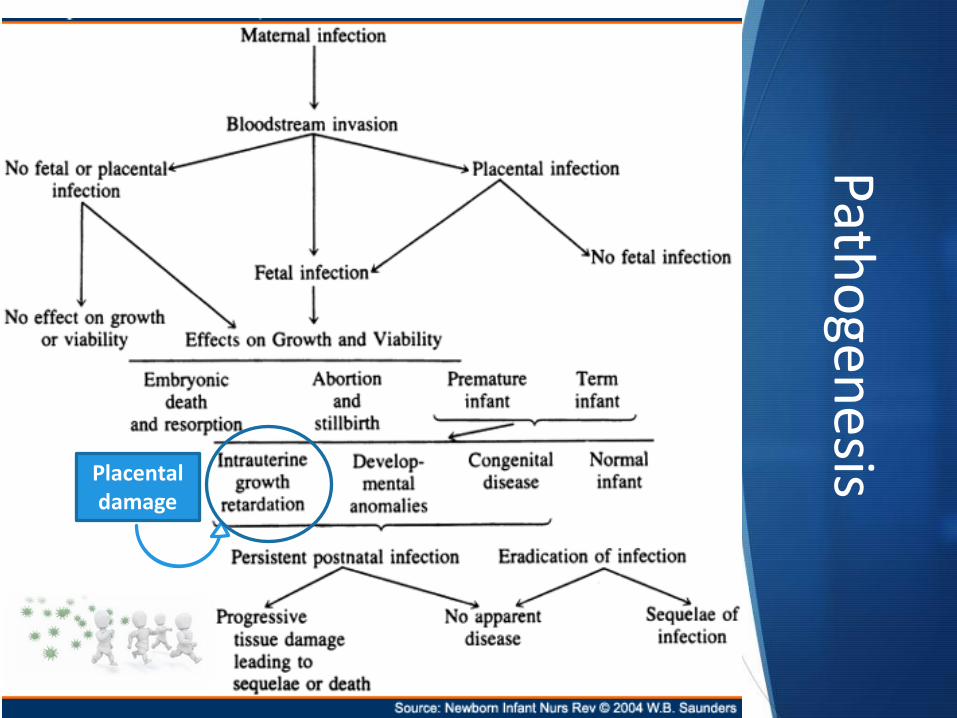
Patho
genesis
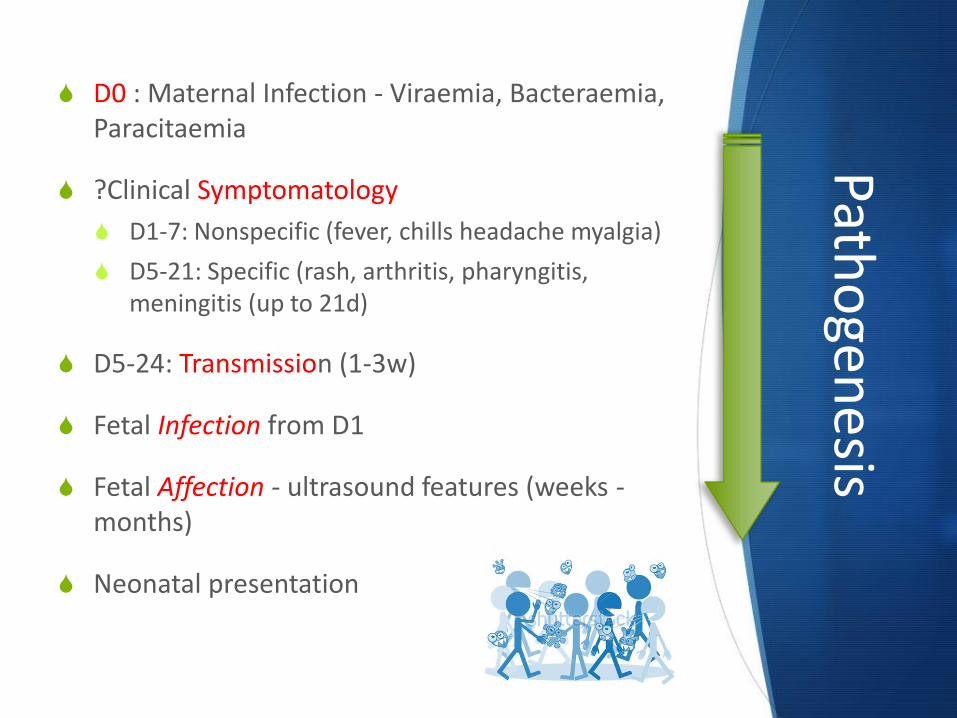
S D0 : Maternal Infection - Viraemia, Bacteraemia, Paracitaemia
S ?Clinical Symptomatology
S D1-7: Nonspecific (fever, chills headache myalgia)
S D5-21: Specific (rash, arthritis, pharyngitis, meningitis (up to 21d)
S D5-24: Transmission (1-3w)
S Fetal Infection from D1
S Fetal Affection - ultrasound features (weeks -months)
S Neonatal presentation

Patho
genesis
S D0 : Maternal Infection - Viraemia, Bacteraemia, Paracitaemia
S ?Clinical Symptomatology
S D1-7: Nonspecific (fever, chills headache myalgia)
S D5-21: Specific (rash, arthritis, pharyngitis, meningitis (up to 21d)
S D5-24: Transmission (1-3w)
S Fetal Infection from D1
S Fetal affection - Ultrasound features (weeks -months)
S Neonatal presentation
Patho
genesis
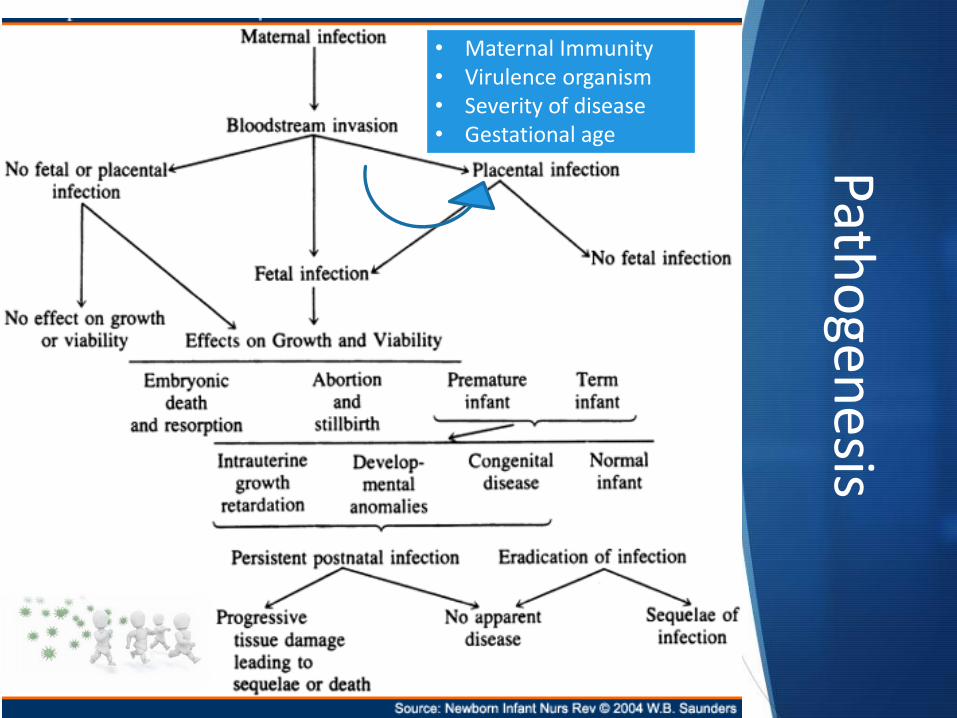
• Maternal Immunity • Virulence organism • Severity of disease • Gestational age
Patho
genesis
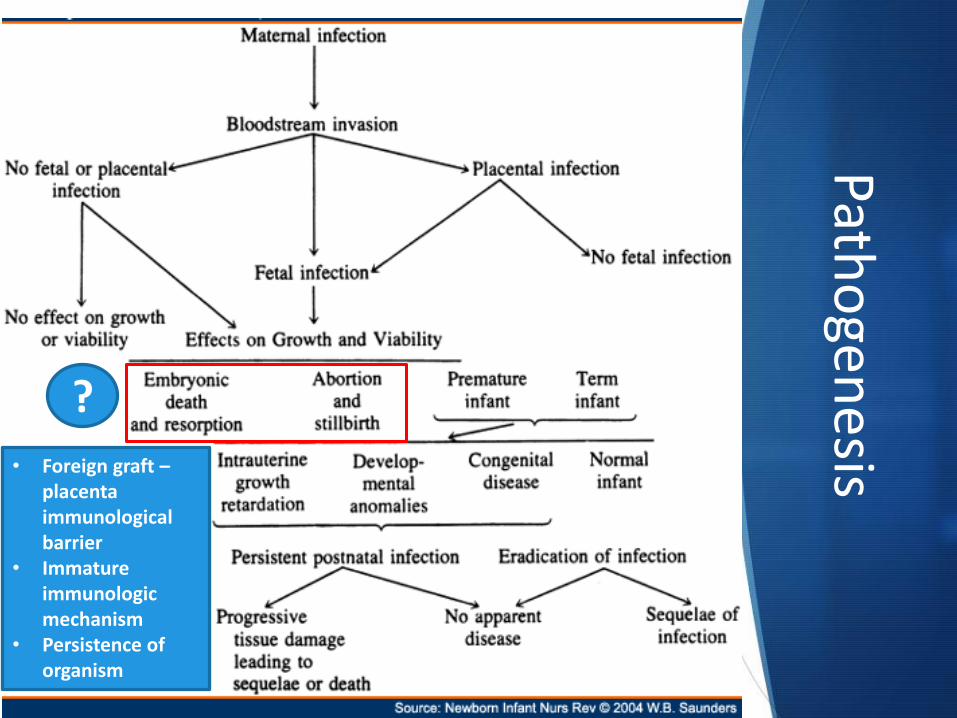
• Foreign graft – placenta immunological barrier
• Immature immunologic mechanism
• Persistence of organism
?
Patho
genesis
Placental damage

Patho
genesis
Progressive tissue
destruction • Toxoplasmosis • Syphilis • Rubella • CMV • HSV

Patho
genesis

Patho
genesis

Patho
genesis
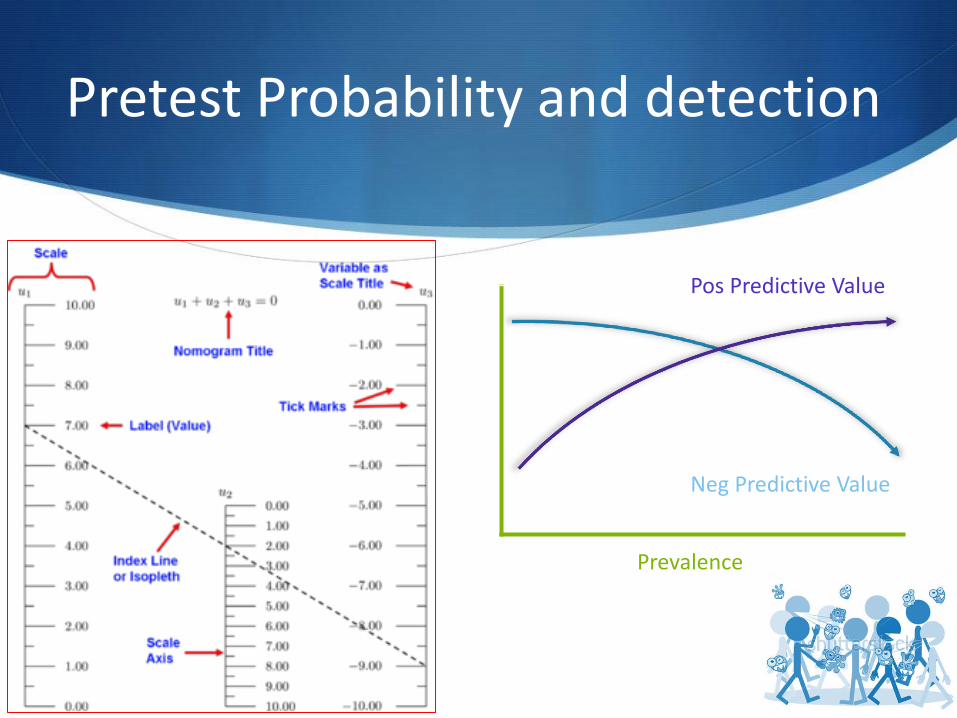
Pretest Probability and detection
Neg Predictive Value
Pos Predictive Value
Prevalence
S Primary Prevention

Current antenatal screening
Test Purpose Action
HIV antibody To enable measures to be taken to reduce vertical transmission.
If positive, ARVs and screening OI.
Syphilis To detect active infection. If reactive, treat with penicillin
Urine culture Treatment of asymptomatic UTI If asymptomatic bacteriuria, treat and repeat culture
Hep B surface antigen To determine chronic carriers. If positive, administer hepatitis B Ig and vaccine to infant at birth
Rubella IgG To determine susceptibility If negative, MMR before conception / post-partum.

CMV
S Primary Prevention – detect seronegative women (IgG -)
S Avoid high risk (children under 6y, sharing utensils)
S Good hygiene
S Primary screening – not recommended
S No vaccine is available
S In seropositive women, ? distinguish between primary –non-primary infection or determine the timing
S No evidence - antiviral drug treatment of primary infection
S Although fetal infection detected, no way to predict outcome

Toxoplasmosis
S Primary Prevention – detect seronegative women (IgG -)
S Avoid high risk (undercooked / cured meat, soil-contaminated fruit / vegetables)
S Primary screening – not recommended
S Screen IgM and/or IgG avidity
S IgM false positive rate (10-13m post after infection)
S Serial IgG titres - lab reproducibility problems
S IgM + and IgG –; both positive two weeks later can be useful
S Although treatment decrease significant CNS affect

What to do?
Assess risk profile
Inform of risks of exposure
Educate on preventative measures
• Vaccinations
• Hand hygiene
• Food (deli meats, soft cheese, unwashed veg)
• Cat litter boxes
• Avoid contact with sick people, wild pets, toddlers

S Secondary Prevention

Presentation
Maternal Features Contact with known infection
History of suggestive infection
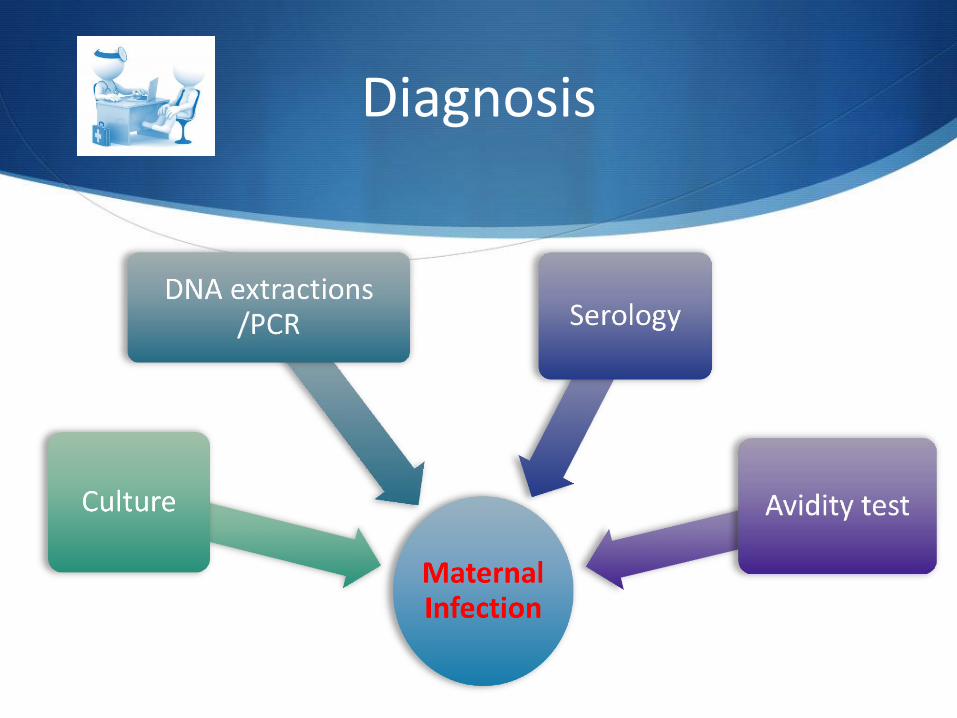
Diagnosis
Diagnosis
S Serology
S Prim infection = seroconversion
S Probable recent if IgM + WITH low IgG avidity
S Recurrent infection:
S Specific IgG + without IgM before pregnancy
S NOW significant increase IgG + titre

Diagnosis
S Avidity Test
S Abs avidity indicates -strength of multivalent Abs binding to multivalent antigen
S Low avidity <30% - suggests primary infection (<3 months)
S High avidity >70% - suggests infection of >4m ago

Prognosis
Number of cases
Severity of infection
Gestation
Transmission Toxo Transmission CMV Transmission Rubella
S Tertiary Prevention

Fetal Presentation
Maternal Features
Contact with known infection
History of suggestive infection
Ultrasound Abnormalities
Ventriculomegaly, Calcifications, echogenic bowels, Hepato- / Splenomegaly, Hydrops fetalis

Antenatal Ultrasound
Infection Main Features of Syndrome
Congenital toxoplasmosis Microcephaly, hydrocephalus, intracranial calcifications, ascites
Congenital syphilis Hepatosplenomegaly, ascites
Congenital rubella syndrome Cataracts, cardiac malformations (eg, patent ductus arteriosus, pulmonary artery hypoplasia), microcephaly, hepatosplenomegaly …
Congenital cytomegalovirus IUGR, microcephaly, hypotonia, intracranial calcifications
Congenital varicella syndrome Atrophy of extremities, microcephaly, cataracts, microphthalmia
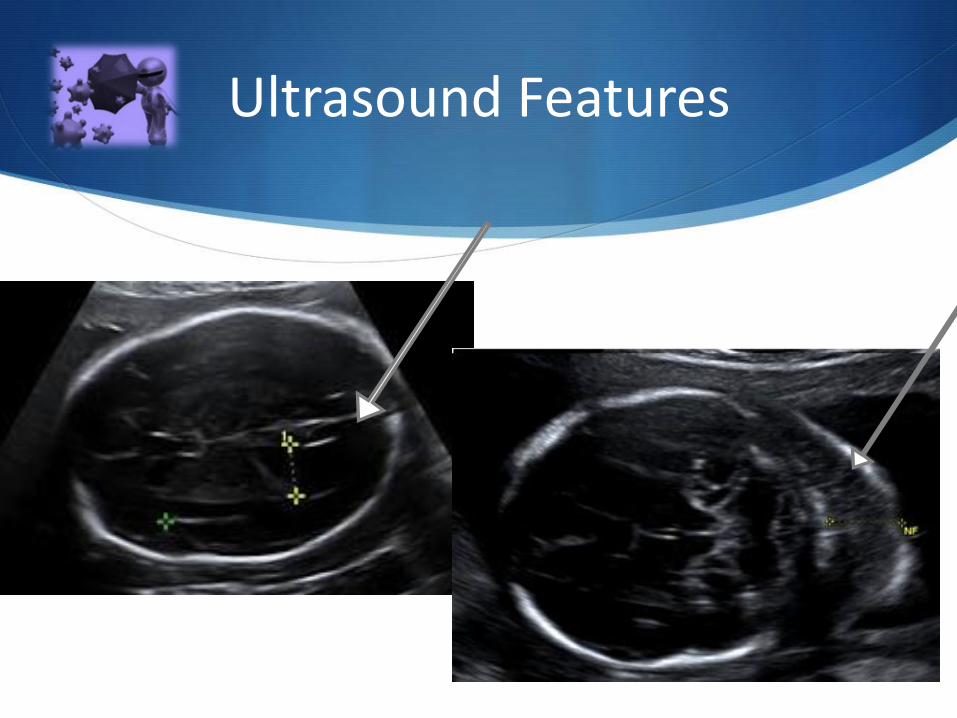
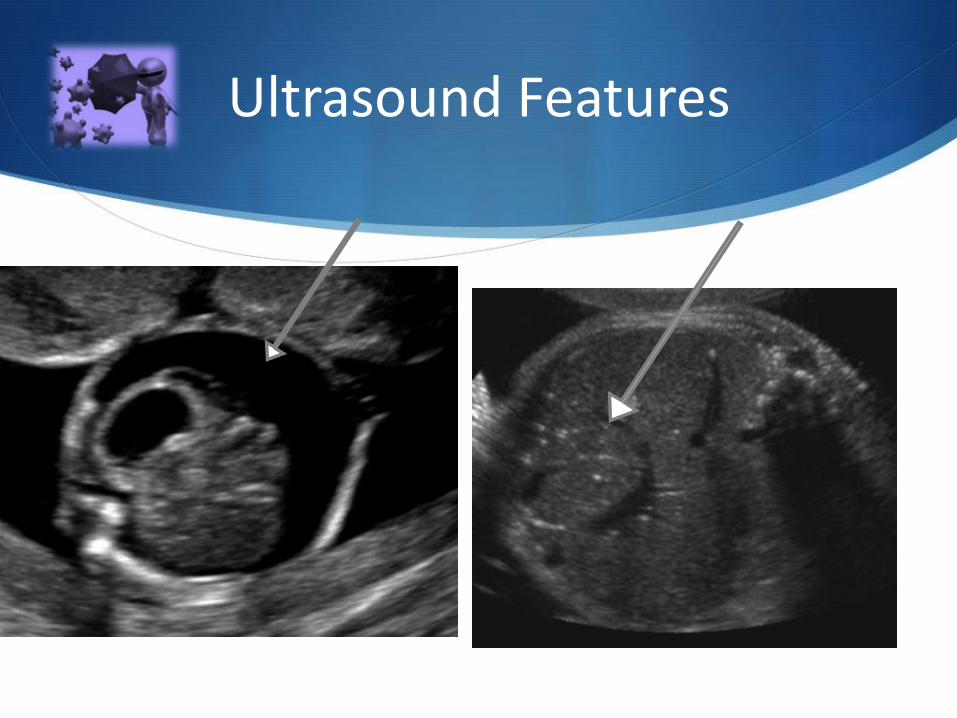
Ultrasound Features

Ultrasound Features
Example Ventricular dilatation (A), hyperechogenicity of the ventricular wall (B).
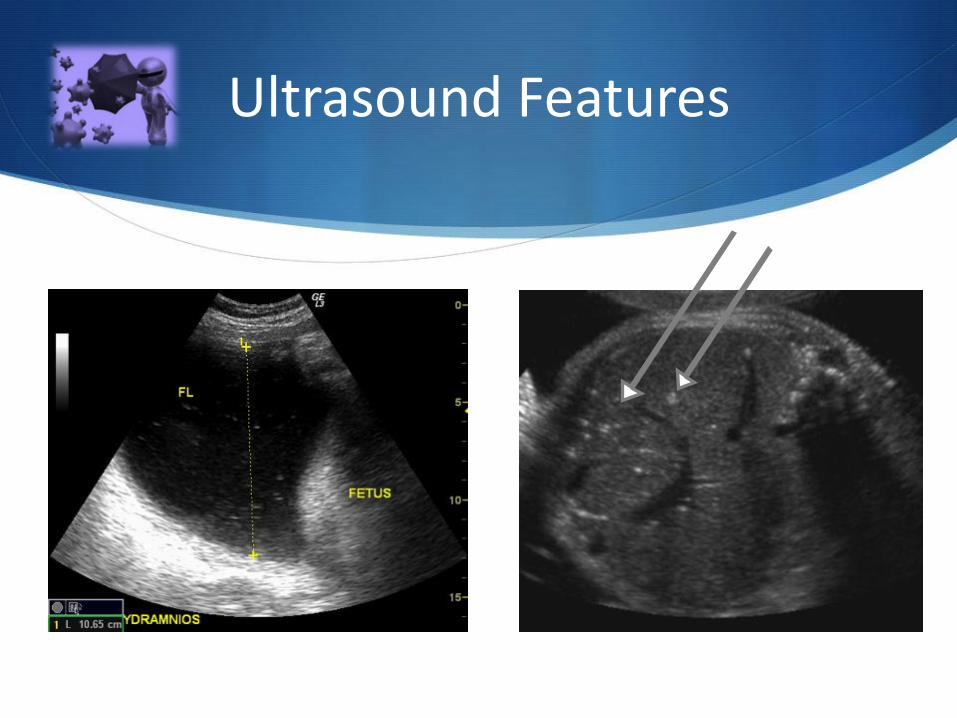
Ultrasound Features
Ultrasound Features

Ultrasound Features

Diagnosis - Fetal
S US Features - Syndromes
S Amniocentesis (after 20w)
S Viral culture 100% specific (…false-negative)
S Viral DNA isolation – PCR both sensitive and specific
S Cordocentesis – FBS
S Detection of viral PCR, IgM, or viral culture
S Together with hematologic, immunologic, and enzymatic measurements

Prognosis
Sonographic abnormalities:
• Associated abnl / extent
• No guarantee of normal fetus/infant if absent
Fetal blood parameters:
• specific IgM, viral load, biochemical, haematological
Viral load in amniotic fluid


S
Specific Infections

Rubella
S Mother:
S Isolate virus from throat / blood
S Paired serological samples
S IgG +, IgM + (Recent infection /reinfection) - Repeat 2w
S IgG -, IgM – (Susceptibility) Repeat if < 3w since contact, < 7d since onset)
S IgG -, IgM + Possible recent infection
S IgG +, IgM – Past infection /immunisation

Rubella
S Congenital rubella syndrome
S Transient abnormalities:
S Permanent abnormalities: cataract, glaucoma, CVS, deafness, microcephaly, MR
S Late abnormalities:
05
101520253035404550
1-4 wks 5-8 wks 9-12 wks > 12 wks
Risk of fetal infection
S Fetal Risk
S T1 - 80-90% transmission
80% abnl (multiple organ damage, miscarraige)
S T2 – 25% abnl (±100% hearing impairment/ ±50% eye abnl)
S >16w - Fetal affectation rare
CMV
S High risk groups for primary CMV
S Day care workers (11% incidence per year)
S Parents with child in day care (incidence of 20 – 30 %/y)
S Cannot be eradiated!
(Reactivation and reinfection common)
S Serologic testing recommended for:
S History suggestive
S Exposure to known CMV
S Immunocompromised
S Abnormalities on routine antenatal ultrasound

CMV
S Prim infect. - 30-40% transm.
S Reinfection - 1-2% transm.
S T1: severe sequelae
(deafness and mental
retardation)
S 10 - 20% infected infants:
sensorineural hearing loss,
ocular damage, impairment of
cognitive / motor function
0
10
20
30
40
50
60
70
1sttrimester
3rdtrimester
Primary Maternal Infection
CongenitalInfections
Symptomsat birth
Severehandicaps

CMV Diagnosis
S Ultrasound [detect typical features, sensitivity 30 – 50 %
S Amniocentesis [for PCR + culture] 4-6w after infection S 45 % sensitive If < 20 weeks
S 80 – 100 % sensitive if > 20 weeks gestation. Specificity up to 100 %.
S Viral loads of >103 copies/mL =symptomatic fetal infection (sens 70%)
S Fetal blood sampling S CMV- IgM > 20 weeks 50 – 80 % sensitive
S Severe congenital CMV
S Consider TOP
S experimental protocols with IV ganciclovir / Valganciclovir

Parvovirus B19
S Childhood viral exanthem erythema infectiosum
(Fifth disease or "Slapped cheek disease")
S Transmision:
S Transplacental up to 30%
S Fetal loss about 9% (T2)
S Overall fetal loss rate 1/60
[<20w up to 17%]
0
2
4
6
8
10
12
14
16
1-12 wks 13-20 wks > 20 wks
Risk of Fetal Infection

Parvovirus B19
S Fetal Affectation
S Aplastic anaemia
S Direct cadriomyopathy
S NIHF (nonimmune hydrops fetalis)
S IUFD – 1-12w after infection
S FBS:
S Fetal serology can be false negative
S PCR (best)
S Fetus – 1-2w review for 3m
S signs of hydrops
S MCA PSV

Toxoplasmosis
S Protozoan, Toxoplasma gondii [intracellular patasite]
S Fetal
S T1 Miscarraige
S Chorioretinits (blindness), encephalitis (micro- ,hydrocephaly and calcifications), jaundice
0%
10%
20%
30%
40%
50%
60%
70%
T1 T2 T3
Transplacental Toxoplasma and Congenital Infection
Transmission
Severe symptoms

Toxoplasmosis
S Investigations
S Ultrasound (>20w) - IUGR, ventriculomegaly, intracranial calcifications, or ascites
S Amniocentesis (4w after maternal) PCR and / or culture
S If US and AF negative - still consider treatment
S Infected mothers
S Spiramycin (1.5 grams every 12 hours) to prevent fetal infection
S 60% reduction
S Infected fetus
S Pyrimethamine and sulfadiazine with folinic acid (Leukovorin)
S TOP
Varicella-Zoster Virus
S Primary infection - chickenpox
S Highly infectious
S 10% respiratory complications
S Herpes zoster ("shingles")
S Not cause congenital /neonatal varicella
S Transplacental passage of antibodies [mother] T2 and T3
S Fetal infection rate 25%
S 2% - 10% fetuses develop VZV embryopathy
S 6 - 12 weeks - limb abn
S 16 to 20 weeks - eye and brain
S Later less frequent & severe

Varicella-Zoster Virus Management
S Infected mothers:
S VZIG does not protect the fetus
S Antiviral agent - acyclovir 5-10mg/kg IVI 8hly x 7d
S Women exposed - VZIG 125 U/10kg IMI (max 625 U)
S Women infected last few days of gestation - born within 2-4 days after the onset
S 20% risk for neonatal varicella - develop progressive varicella
S Administration of VZIG most valuable

Herpes Simplex
S HSV persist in latent state, resurfacing at any time
S Mostly acquired during delivery
S Primary infection - 33 to 50% transmission
S Recurrent disease - 1 to 3% transmission
S Primary HSV infection:
S Miscarriage
S Disseminated – hepatitis,
encephalitis,death
S PTL
S Perinatal infection
S Manifests during 1st month
Herpes Simplex Effects
S 3 major categories seen
S localized skin, eye and mouth infection
S encephalitis with or without skin, eye, and mouth disease
S disseminated infection [irritability, seizures, respiratory distress, jaundice, bleeding diathesis, and shock]
S CNS infections – chorioretinits, meningitis, encephalitis, MR

Herpes Simplex Management
S Caesarean section if primary, first episode, or recurrent HSV lesions present in labour
S Infants - cultures of nose, mouth, urine, and stool [24 – 48h]
S If any maternal cultures are positive or if disease is apparent
S Diagnosed new-borns - isolated to prevent nosocomial transmission
S Treatment include acyclovir IV (20 mg/kg/dose) q8 hours for 14 to 21 days



![Reducing Mortality and Infections After Congenital … Mortality and Infections After Congenital ... [CI] 0.62–0.81) ... Kathy J. Jenkins, MD, MPH,a Aldo R. Castañeda,Published](https://static.documents.pub/doc/80x56/5b00b0757f8b9af1148d012e/reducing-mortality-and-infections-after-congenital-mortality-and-infections.jpg)














