Page 1
Your NHS partner for improving
health and integrating care
Get to know us or get in touch
Twitter: Mlcsu | Linkedin: Midlands and Lancashire Commissioning Support Unit
midlandsandlancashirecsu.nhs.uk
Consultation feedback on proposals to create a
Single Commissioning Organisation for Staffordshire
and Stoke-on-Trent
Report of findings
Monday, 2 September 2019
Page 2
2 | NHS Midlands & Lancashire Commissioning Support Unit
Table of Contents
1 Executive summary .................................................................................................................. 4 Introduction ............................................................................................................................... 4 Communications and engagement .......................................................................................... 4 Participants and respondents .................................................................................................. 5 Findings ..................................................................................................................................... 5 Comments on the options......................................................................................................... 6 Support for option 1 ......................................................................................................................................................... 6 Support for option 2 ......................................................................................................................................................... 6 Summary of organisational responses ............................................................................................................................ 7
Alternative options .................................................................................................................... 7
2 Introduction ............................................................................................................................... 8 Report authors ........................................................................................................................... 8 Report structure ........................................................................................................................ 8 Background ............................................................................................................................... 8 The proposals ............................................................................................................................ 9 Overview of the consultation .................................................................................................... 9
3 Communications and engagement methodology ................................................................ 10 Communications and collateral .............................................................................................. 10 Consultation document .................................................................................................................................................. 10 Press ............................................................................................................................................................................. 10 Social media .................................................................................................................................................................. 11 Web content .................................................................................................................................................................. 11 Distribution .................................................................................................................................................................... 11
Engagement channels ............................................................................................................. 12 Survey ........................................................................................................................................................................... 12 Public events ................................................................................................................................................................. 12 Consultation meetings ................................................................................................................................................... 14 Correspondence ............................................................................................................................................................ 15
4 Respondent profiling .............................................................................................................. 16 Demographic profile ................................................................................................................ 17 Map of consultation respondents ........................................................................................... 18
5 Findings ................................................................................................................................... 19 Reporting and analysis notes ................................................................................................. 19 Views on option 1 .................................................................................................................... 20 Feedback from the survey ............................................................................................................................................. 20 Feedback from correspondence .................................................................................................................................... 27
Views on option 2 .................................................................................................................... 29 Feedback from the survey ............................................................................................................................................. 29 Feedback from correspondence .................................................................................................................................... 35
Alternative options .................................................................................................................. 36 Feedback from the survey ............................................................................................................................................. 36 Feedback from correspondence .................................................................................................................................... 38
Considerations raised ............................................................................................................. 39 Feedback from correspondence .................................................................................................................................... 39
Other comments ...................................................................................................................... 40 Feedback from public events ......................................................................................................................................... 40 Feedback from other consultation meetings .................................................................................................................. 40
6 Conclusions ............................................................................................................................ 42 Comments on the options....................................................................................................... 42 Support for option 1 ....................................................................................................................................................... 42 Support for option 2 ....................................................................................................................................................... 43
Alternative options .................................................................................................................. 43
Appendix 1: Example social media posts .................................................................................. 44
Appendix 2: Organisations sending correspondence .............................................................. 45
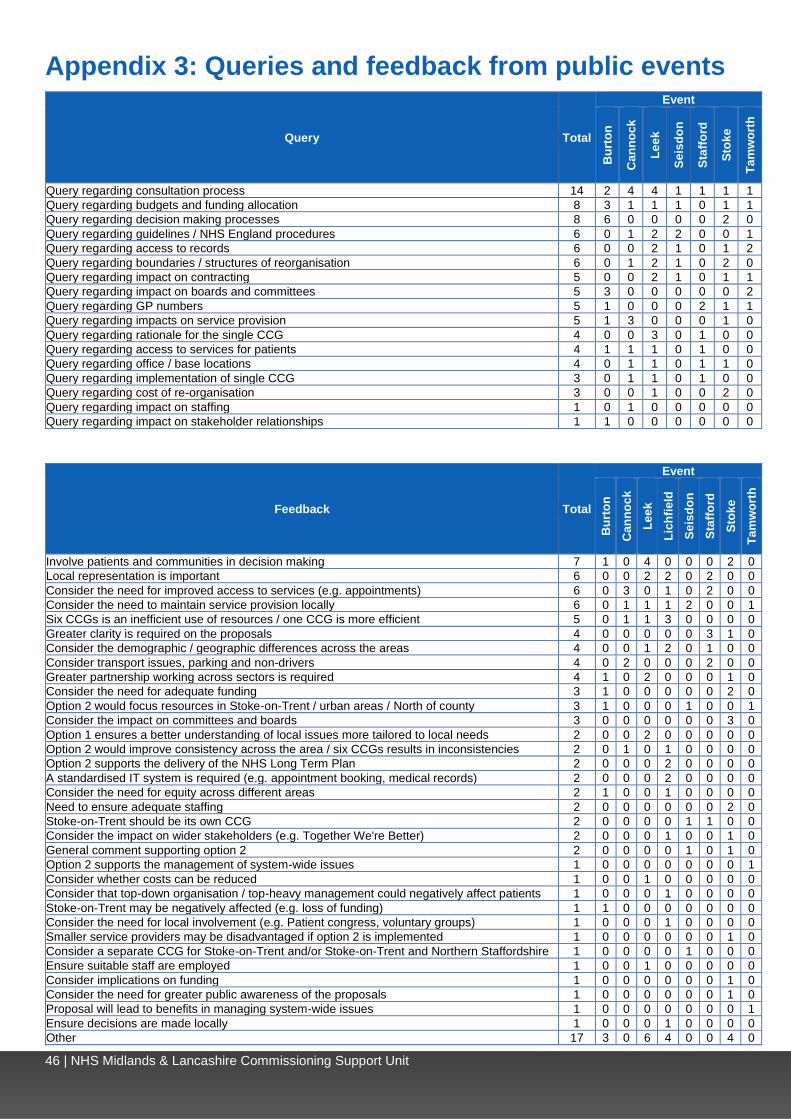
Appendix 3: Queries and feedback from public events ............................................................ 46
Appendix 4: Summary of event demographic profiling questionnaires .................................. 47
Page 3
3 | NHS Midlands & Lancashire Commissioning Support Unit
References
Figure 1. Map of the six Staffordshire and Stoke-on-Trent CCGs’ areas ....................................................... 8
Figure 2. Front cover and example pages of the consultation document ..................................................... 10
Figure 3. Map of public event locations ....................................................................................................... 13
Figure 4. Map of respondents’ location ........................................................................................................ 18
Table 1. Summary of support for the options ................................................................................................. 5
Table 2. Summary of organisational responses ............................................................................................. 7
Table 3. Press releases and press coverage ............................................................................................... 10
Table 4. Social media analytics ................................................................................................................... 11
Table 5. Emails sent .................................................................................................................................... 11
Table 6. Public events ................................................................................................................................. 12
Table 7. Consultation meetings ................................................................................................................... 14
Table 8. Correspondence received.............................................................................................................. 15
Table 9. Number of respondents and participants ....................................................................................... 16
Table 10. Survey respondent types ............................................................................................................. 16
Table 11. Respondents by CCG area .......................................................................................................... 16
Table 12. Profile of members of the public completing the survey ............................................................... 17
Table 13. Option 1: Keep the current arrangements of six separate CCGs under a single leadership team 20
Table 14. Option 1: What do you agree with? .............................................................................................. 21
Table 15. Option 1: Do you have any concerns or are there any groups or individuals you think may be
negatively impacted by this option? ............................................................................................................. 23
Table 16. Option 1: How could these negative impacts be overcome? ........................................................ 25
Table 17. Feedback from correspondence with positive themes around option 1 / negative themes around
option 2 ....................................................................................................................................................... 27
Table 18. Option 2: Develop a new, single CCG ......................................................................................... 29
Table 19. Option 2: What do you agree with? .............................................................................................. 30
Table 20. Option 2. Do you have any concerns or are there any groups or individuals you think may be
negatively impacted by this option? ............................................................................................................. 31
Table 21. How could these negative impacts be overcome? ....................................................................... 33
Table 22. Feedback from correspondence with positive themes around option 2 / negative themes around
option 1 ....................................................................................................................................................... 35
Table 23. Do you have any other suggested options that we should consider? ........................................... 36
Table 24. Feedback from correspondence with alternative options ............................................................. 38
Table 25. Themes for consideration and comments on consultation process raised in correspondence ..... 39
Table 26. Summary of support for the options ............................................................................................. 42
Page 4
4 | NHS Midlands & Lancashire Commissioning Support Unit
1 Executive summary This report of findings presents the feedback from the public consultation which took place across
Staffordshire between Thursday 9 May 2019 and Sunday 30 June 2019. The consultation was exploring
public, patient and wider stakeholder views on two proposals for the future of the six Staffordshire CCGs.
Introduction
Health services in Staffordshire and Stoke-on-Trent are currently split into six geographical areas and led by
six separate local Clinical Commissioning Groups (CCGs):
• Cannock Chase CCG
• East Staffordshire CCG
• North Staffordshire CCG
• Stafford and Surrounds CCG
• South East Staffordshire and Seisdon Peninsula CCG
• Stoke-on-Trent CCG.
The proposals are:
Option 1: Keep the current arrangements of six separate CCGs under a single leadership team
• The six CCGs will stay as separate organisations, each responsible for their own statutory functions
(legal obligations)
• The single leadership team will oversee the delivery of these, supported by meetings held jointly or
‘in common’
• The CCGs will align their priorities and objectives, but each CCG keeps its own constitution, and is
responsible for its own local area.
Option 2: Develop a new, single CCG
• To form a single Strategic Commissioning Organisation (SCO) for the county
• The single leadership team will oversee the delivery of the CCG’s statutory functions (legal
obligations), supported by governance (committee) meetings
• A single Governing Body will work to one set of statutory duties
• This model would free-up money and capacity to create efficiencies, for example across buildings,
processes and IT.
For further information, please view the consultation document.
Communications and engagement
A range of collateral was produced to provide information on the consultation and encourage feedback. This
included:
• A consultation document: ‘Your views on our journey...towards becoming a single Strategic
Commissioning Organisation’ to inform stakeholders of the consultation
• Two press releases: One at the start of the engagement period on 9 May 2019 and the second on
31 May to inform stakeholders of the extended closing date
• Social media posts: The consultation was promoted across the CCGs’ Facebook and Twitter
profiles
• Web content: The consultation was promoted on each of the CCGs’ websites.
Collateral was sent to all GP practices in the area, available at CCG offices, used at public events and
meetings and made available at Together We’re Better (the Staffordshire and Stoke-on-Trent Sustainability
Transformation Partnership) public listening events. Emails were also sent to inform stakeholders of the
Page 5
5 | NHS Midlands & Lancashire Commissioning Support Unit
consultation. These stakeholders included voluntary and patient representative groups, staff, GPs and
corporate stakeholders.
Feedback was gathered using the following engagement channels:
• Paper and online survey: This was structured into two main sections – views on the proposals and
demographic profiling questions
• Eight public events: These were held at locations across the consultation area
• Meetings: These were held with a range of stakeholders, including patient district groups, MPs and
scrutiny committees
• Correspondence: Stakeholders could provide feedback via email or letter.
Participants and respondents
Feedback on the consultation proposals came from:
• 76 responses to the consultation survey
• 80 participants at eight public events
• 27 pieces of correspondence
Survey respondents were asked questions to enable a demographic profile of respondents to be
understood. This is summarised below:
• Ethnicity: 42 (88%) respondents were White British and 4 (8%) White Irish
• Age category: 32 (67%) respondents were aged 60 or over
• Religion: 23 (55%) respondents were Christian and 15 (36%) had no religion
• Sex: 25 (51%) respondents were female and 20 (41%) were male
• Gender identity: 35 (81%) respondents had not undergone any gender reassignment
• Sexual orientation: 29 (64%) respondents were heterosexual and 3 (7%) bisexual
• Relationship status: 30 (63%) respondents were married
• Pregnancy: 1 (2%) respondent was currently pregnant
• Health problem or disability: 16 (36%) respondents had a health problem or disability which limited
their day-to-day activities
• Carer: 6 (13%) respondents were carers for a person aged 50 or over
• Armed services: 2 (4%) respondents had served in the armed services.
Findings
In the survey, a slightly greater proportion of respondents expressed support to keep the current
arrangements, with 29 (45%) of respondents supporting option 1, compared to 30 (42%) of respondents
who supported option 2, to create a single CCG.
A greater proportion of respondents were unsupportive of option 2, with 31 (44%) respondents indicating
they were not supportive, compared to 21 (32%) of respondents for option 1.
Table 1. Summary of support for the options
Supportive
(4 or 5) Neutral
(3) Not supportive
(1 or 2) Base
Option 1: Keep the current arrangements of six separate CCGs under a single leadership team
45% 23% 32% 65
Option 2: Develop a new, single CCG
42% 14% 44% 71
Page 6
6 | NHS Midlands & Lancashire Commissioning Support Unit
Comments on the options
Support for option 1
In support of option 1, it was commented that retaining six CCGs would ensure a better understanding of
local issues more tailored to local needs and local representation and involvement.
The need to consider the demographic and geographic differences in the area was a key theme throughout
(e.g. deprivation in Stoke-on-Trent, rural versus city).
There was concern that resources would be focused on Stoke-on-Trent / urban areas if option 2 was
implemented. However, there was also concern in the survey and in correspondence that Stoke-on-Trent
would be negatively affected if option 2 was implemented – for example, with a loss of funding.
Organisational comments: Organisations commenting in opposition to the proposal to create a single
CCG or expressing concerns included Stoke-on-Trent City Council, Cannock Chase Council, Hednesford
Town Council, Healthy Staffordshire Select Committee and Staffordshire Moorlands District Council.
• Stoke-on-Trent City Council expressed disagreement with option 2. The Deputy Leader of the
Council and Lead Member for Health and Social Care commented that Stoke-on-Trent is
demographically and geographically different from Staffordshire, and that a single CCG would lose
local focus and decision-making capability. They commented that funding would move from North to
South and there would be a shift in emphasis away from the population’s need to resolve financial
pressures.
• Stoke-on-Trent City Council Adults and Neighbourhoods Overview and Scrutiny Committee
expressed concern that a single CCG would result in a postcode lottery. They commented that there
would be variations in service provision and facilities in Stoke-on-Trent. They said that the result
would be a ‘one-size-fits-all’ commissioning model, with services not being commissioned according
to need.
• Healthy Staffordshire Select Committee expressed concern that the proposed move was
financially led and that commissioning policies had not been mentioned. They commented the North
and South of the county have differing population needs.
• Cannock Chase Council commented in opposition to the proposed creation of a single
commissioning organisation. They argued that it is a cost-cutting measure – not in the best interests
of patients and carers within Cannock Chase. They commented that a single commissioning
organisation would see resources diverted away from Cannock Chase. They expressed concern that
there would be a loss of influence over local clinical commissioning decisions and worsening of
existing poor engagement with the council.
• Hednesford Town Council commented that CCGs should remain local to ensure local
representation and understanding of local needs.
• Staffordshire Moorlands District Council commented that Staffordshire Moorlands has a large
rural population with different needs to the rest of the county. They expressed concern that localism
would be lost if the CCGs were to merge into one organisation.
• 3 local MPs also raised opposition to the single CCG. Concerns that they raised included a loss of
focus on local needs; effects on funding allocations and impacts on service provision.
Support for option 2
In support of option 2, it was commented that six CCGs are an inefficient use of resources and that one
CCG would be more efficient. Other comments were that option 2 would improve consistency across the
area, as having six CCGs results in inconsistencies whereas option 2 would result in economies of scale.
Organisational comments: Organisations expressing broad support for option 2 included NHS Trusts,
Healthwatch Staffordshire and Staffordshire County Council.
Page 7
7 | NHS Midlands & Lancashire Commissioning Support Unit
• North Staffordshire Combined Healthcare NHS Trust and University Hospitals of North
Midlands NHS Trust commented that the single CCG would support in the management of system-
wide issues.
• Midlands Partnership NHS Foundation Trust commented that a single CCG would support
collaborative working and ICP development; simplify governance arrangements; reduce duplication
and support equitable care across Staffordshire and Stoke-on-Trent.
• Healthwatch Staffordshire commented that the proposal would improve consistency and potentially
result in savings that could be reinvested into services.
• Staffordshire County Council also expressed support for option 2 in correspondence.
Summary of organisational responses
Table 2 provides a summary of the organisational views received via correspondence. These have been
split into broadly supportive of a single CCG and concerns raised or opposition to a single CCG. However,
those that have been categorised as broadly supportive may also have raised some considerations or
concerns and those categorised as concerns raised or opposition to a single CCG may also have made
positive comments.
Table 2. Summary of organisational responses
Broadly supportive of a single CCG Concerns raised or opposition to a single CCG
Healthwatch Staffordshire Adults and Neighbourhoods Overview and Scrutiny Committee, Stoke-on-Trent City Council
Midlands Partnership NHS Foundation Trust Cannock Chase Council
North Staffordshire Combined Healthcare NHS Trust Paul Farrelly MP
Staffordshire County Council Healthwatch Stoke-on-Trent
Tamworth Council Healthy Staffordshire Select Committee, Staffordshire County Council
University Hospitals of North Midlands NHS Trust Hednesford Town Council
Jeremy Lefroy MP*
Reach (part of Asist)
Ruth Smeeth MP
Gareth Snell MP
Staffordshire Moorlands District Council
Stoke-on-Trent City Council *Raised a query over funding
Alternative options
A key theme in both the survey and correspondence was that Stoke-on-Trent should be a standalone CCG.
The need to involve patients and communities in decision-making and to improve partnership working
across CCGs were key themes in the survey.
Organisational comments:
• Healthwatch Stoke-on-Trent queried why a Northern Staffordshire CCG is not an option.
• Stoke-on-Trent City Council (the Deputy Leader of the City Council and Lead Member for Health
and Social Care) commented that Stoke-on-Trent should remain its own CCG or there should be an
amalgamated CCG across Stoke-on-Trent and North Staffordshire on the same geographic
boundaries as the Northern Alliance.
• Similarly, Stoke-on-Trent City Council Adults and Neighbourhoods Overview and Scrutiny
Committee gave two alternative options: One CCG for Stoke-on-Trent and another CCG for the
remainder of Staffordshire, or three CCGs based on the three divisional committees for the North,
South East and South West as outlined within the proposed governance structure in the consultation.
Page 8
8 | NHS Midlands & Lancashire Commissioning Support Unit
2 Introduction
Report authors
The Staffordshire and Stoke-on-Trent Clinical Commissioning Groups commissioned NHS Midlands and
Lancashire Commissioning Support Unit (MLCSU) Communications and Engagement Service to coordinate
the independent analysis of the feedback from the consultation to produce this report.
Report structure
This report is structured into the following sections:
• Section 1: Executive summary
• Section 2: Introduction
• Section 3: Communications and engagement methodology
• Section 4: Respondent profiling
• Section 5: Findings
• Section 6: Conclusion.
Background
The background information in section 2.3 and 2.4 is taken from the consultation document.
Health services in Staffordshire and Stoke-on-Trent are
currently split into six geographical areas and led by six
separate local CCGs. These are:
• Cannock Chase CCG
• East Staffordshire CCG
• North Staffordshire CCG
• Stafford and Surrounds CCG
• South East Staffordshire and Seisdon Peninsula CCG
• Stoke-on-Trent CCG.
The CCGs need to keep ahead of the growing and changing
needs of the 1.1 million people living in Staffordshire and
Stoke-on-Trent. The NHS Long Term Plan, published in
January 2019, looks at working together effectively, with no
barriers.
In recent years, the six CCGs have developed closer working
relationships, and now have a single leadership team and
staffing structure. Governing Body meetings are also held ‘in
common’ so that any strategic decisions affecting the whole
population can be made. The CCGs are now proposing to
formalise these arrangements by creating a Single
Commissioning Organisation (SCO), with responsibility for
the entirety of Staffordshire and Stoke-on-Trent from April
2020.
In December 2018, the CCGs made an application to NHS England confirming their intention to develop and
operate as a single organisation. Consultation has already taken place with the Governing Bodies of the six
CCGs and with more than 150 GP surgeries in the region.
Figure 1. Map of the six Staffordshire and Stoke-on-Trent CCGs’ areas
Page 9
9 | NHS Midlands & Lancashire Commissioning Support Unit
The proposals
The proposals are:
Option 1: Keep the current arrangements of six separate CCGs under a single leadership team
• The six CCGs will stay as separate organisations, each responsible for their own statutory functions
(legal obligations)
• The single leadership team will oversee the delivery of these, supported by meetings held jointly or
‘in common’
• The CCGs will align their priorities and objectives, but each CCG keeps its own Constitution, and is
responsible for its own local area.
Option 2: Develop a new, single CCG
• To form a single Strategic Commissioning Organisation (SCO) for the county
• The single leadership team will oversee the delivery of the CCG’s statutory functions (legal
obligations), supported by governance (committee) meetings
• A single Governing Body will work to one set of statutory duties
• This model would free-up money and capacity to create efficiencies, for example across buildings,
processes and IT.
For further information, please view the consultation document.
Overview of the consultation
The consultation ran from Thursday 9 May 2019 until midnight on Sunday 30 June 2019. NHS Midlands and
Lancashire Commissioning Support Unit have collated all feedback gathered from the consultation and have
produced this report for the CCGs. A decision will be made by the CCGs’ Governing Bodies.
Page 10
10 | NHS Midlands & Lancashire Commissioning Support Unit
3 Communications and engagement methodology This section details the communication and engagement activities undertaken during the consultation
across the six CCG areas.
Communications and collateral
This section details the range of collateral used to promote the consultation.
Consultation document
A consultation document – ‘Your views on our journey...towards becoming a single Strategic Commissioning
Organisation’ – was produced, informing members of the public and other stakeholders of the proposals and
rationale for becoming a single CCG.
Press
Table 3 details the press releases produced regarding the consultation and the coverage generated.
Table 3. Press releases and press coverage
Date Headline Coverage / publication
Press releases
9 May 2019 Public, patients and partners to participate in
Staffordshire and Stoke-on-Trent NHS Commissioning Consultation
A little bit of Stone
Stoke Sentinel
31 May 2019 Consultation on health organisation extended to
allow more residents to participate No coverage
Press coverage
10 May 2019 Public consultation opens to create new single NHS
Clinical Commissioning Group A little bit of Stone
22 May 2019 CCG merger plan in bid to end ‘postcode lottery’ Stoke Sentinel
22 May 2019 Will this major healthcare shake-up be good to
patients? Stoke Sentinel
One reactive press enquiry was received from the Express and Star on 10 May 2019.
Figure 2. Front cover and example pages of the consultation document
Page 11
11 | NHS Midlands & Lancashire Commissioning Support Unit
Social media
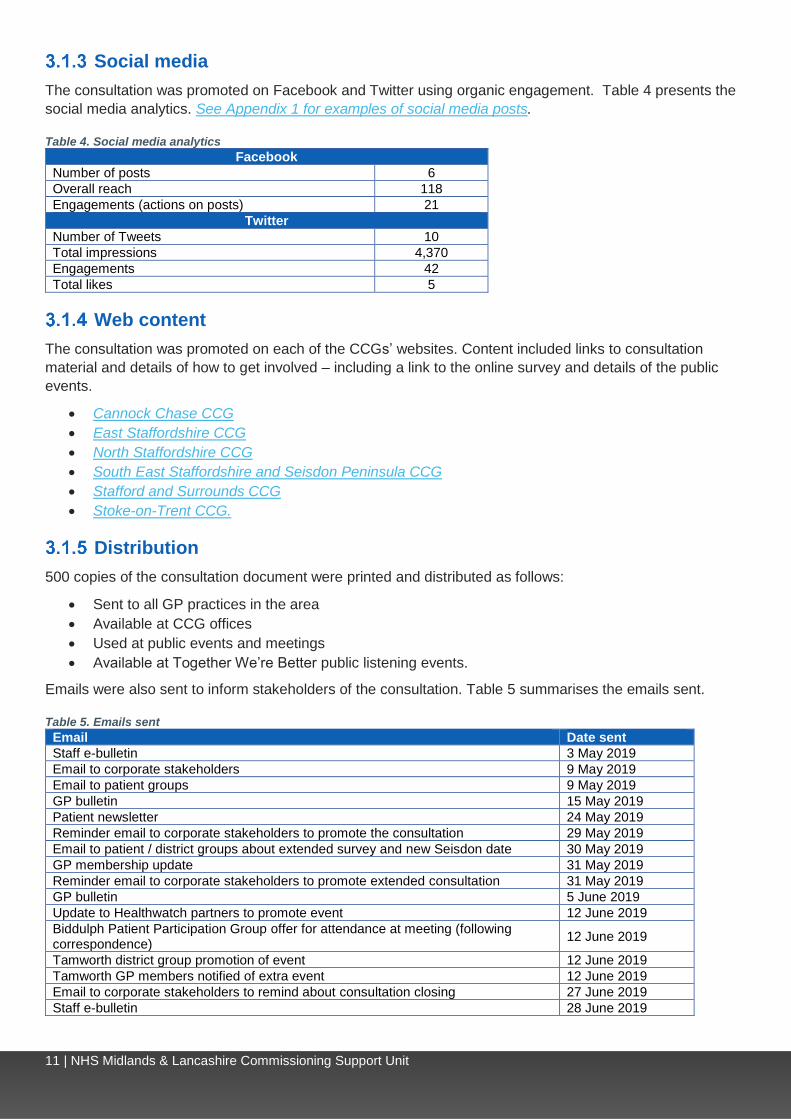
The consultation was promoted on Facebook and Twitter using organic engagement. Table 4 presents the
social media analytics. See Appendix 1 for examples of social media posts.
Table 4. Social media analytics
Facebook
Number of posts 6
Overall reach 118
Engagements (actions on posts) 21
Twitter
Number of Tweets 10
Total impressions 4,370
Engagements 42
Total likes 5
Web content
The consultation was promoted on each of the CCGs’ websites. Content included links to consultation
material and details of how to get involved – including a link to the online survey and details of the public
events.
• Cannock Chase CCG
• East Staffordshire CCG
• North Staffordshire CCG
• South East Staffordshire and Seisdon Peninsula CCG
• Stafford and Surrounds CCG
• Stoke-on-Trent CCG.
Distribution
500 copies of the consultation document were printed and distributed as follows:
• Sent to all GP practices in the area
• Available at CCG offices
• Used at public events and meetings
• Available at Together We’re Better public listening events.
Emails were also sent to inform stakeholders of the consultation. Table 5 summarises the emails sent.
Table 5. Emails sent
Email Date sent
Staff e-bulletin 3 May 2019
Email to corporate stakeholders 9 May 2019
Email to patient groups 9 May 2019
GP bulletin 15 May 2019
Patient newsletter 24 May 2019
Reminder email to corporate stakeholders to promote the consultation 29 May 2019
Email to patient / district groups about extended survey and new Seisdon date 30 May 2019
GP membership update 31 May 2019
Reminder email to corporate stakeholders to promote extended consultation 31 May 2019
GP bulletin 5 June 2019
Update to Healthwatch partners to promote event 12 June 2019
Biddulph Patient Participation Group offer for attendance at meeting (following correspondence)
12 June 2019
Tamworth district group promotion of event 12 June 2019
Tamworth GP members notified of extra event 12 June 2019
Email to corporate stakeholders to remind about consultation closing 27 June 2019
Staff e-bulletin 28 June 2019
Page 12
12 | NHS Midlands & Lancashire Commissioning Support Unit
Engagement channels
This section gives an overview of the engagement channels.
Survey
Both paper and online versions of the survey were used to gather feedback. The survey was split into two
sections:
• Your views on our proposals: This was split into views on option 1 and views on option 2
• About you: This section contained demographic profiling questions.
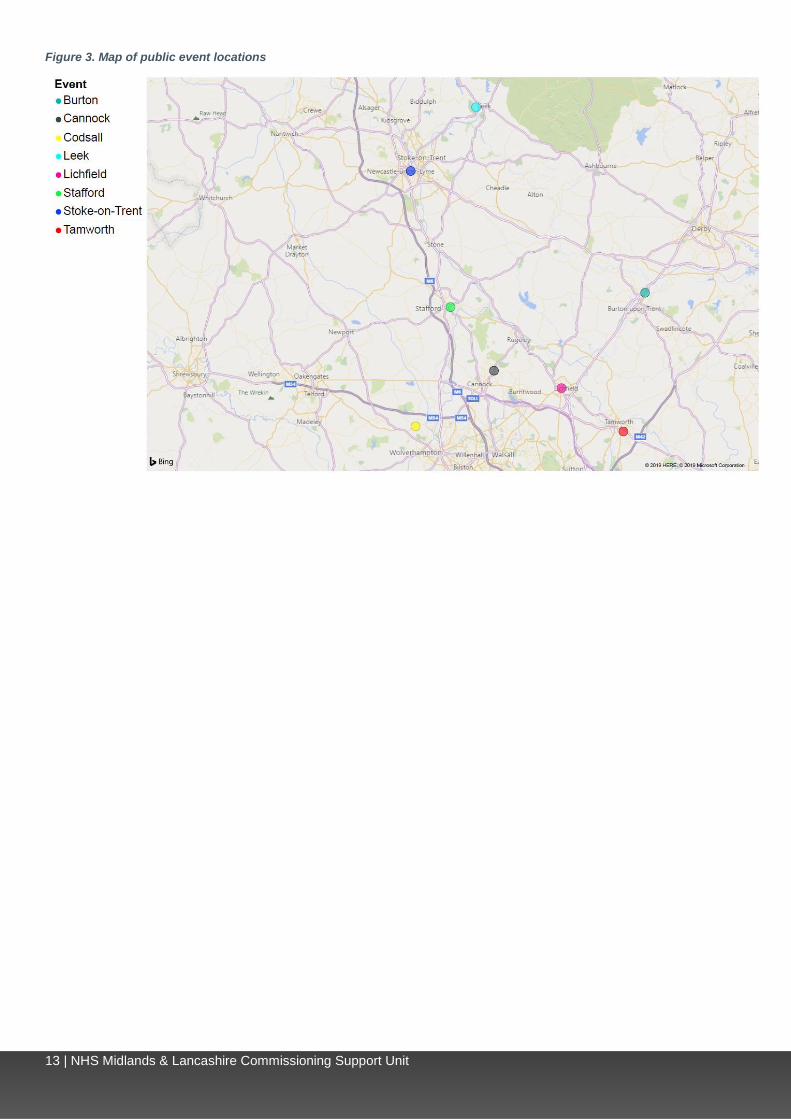
Public events
Eight public events were held to inform stakeholders of the proposals and gather feedback. This ensured
that there was an event held in each CCG area, with additional events held in South East Staffordshire and
Seisdon Peninsula CCG, as the CCG is split across two areas and to ensure there were events in both
Lichfield and Tamworth. Table 6 lists the events and figure 3 shows a map of the public events.
Table 6. Public events
Date CCG area Location Venue Number of
attendees
22 May Stoke-on-Trent CCG Stoke-on-Trent Medical Institute, Hartshill, Stoke-on-Trent ST4 7NY
16
23 May South East Staffordshire and Seisdon Peninsula CCG
Lichfield The George Hotel, Lichfield WS13 6PR 3
28 May North Staffordshire CCG Leek St. Edwards Academy, Leek ST13 8DN 9
29 May Stafford and Surrounds CCG Stafford Entrust, Stafford ST16 3TH 5
4 June Cannock Chase CCG Cannock Aquarius Ballroom, Hednesford, Cannock WS12 1BT
20
5 June East Staffordshire CCG Burton Pirelli Stadium, Burton DE13 0BH 5
7 June South East Staffordshire and Seisdon Peninsula CCG
Codsall Bill Brownhill Room, South Staffordshire District Council, Codsall WV8 1PX
5
20 June South East Staffordshire and Seisdon Peninsula CCG
Tamworth Tamworth Community Fire Station, Marlborough Way, Tamworth B77 2JN
17
Total 80
Page 13
13 | NHS Midlands & Lancashire Commissioning Support Unit
Figure 3. Map of public event locations
Page 14
14 | NHS Midlands & Lancashire Commissioning Support Unit
Consultation meetings
In addition to the public events, a range of meetings were attended to inform key stakeholders of the
proposals and gather feedback. These included overview and scrutiny committees (OSCs), MP meetings
and district meetings. Feedback received from meetings has been included in the report. Table 7 lists the
meetings.
Table 7. Consultation meetings
Date Type of event Feedback received
23 April 2019 Stafford County OSC No minutes received
29 April 2019 Stafford Borough OSC Brief meeting, not minuted
2 May 2019 Executive meeting No minutes received
8 May 2019 Patient Council Minutes received, included in section 5.5.2
14 May 2019 Patient Board No minutes received
16 May 2019 East Staffordshire OSC Informal meeting, not minuted
16 May 2019 South Staffordshire OSC No minutes received
16 May 2019 Cannock Chase District Group Minutes received, included in section 5.5.2
17 May 2019 Community Health Voice No minutes received
20 May 2019 Tamworth Scrutiny Committee No minutes received
20 May 2019 Lichfield OSC No minutes received
20 May 2019 South East Staffordshire District Patient Group No minutes received
21 May 2019 Seisdon District Patient Group Minutes received, included in section 5.5.2
22 May 2019 Stafford and Surrounds District Group No minutes received
23 May 2019 Cannock Chase OSC Brief meeting, not minuted
24 May 2019 MP meeting in North No minutes received
28 May 2019 MP meeting with Gareth Snell No minutes received
6 June 2019 Leek Moorlands Overview and Scrutiny
Committee No minutes received
6 June 2019 Staffordshire Health and Wellbeing Board Consultation materials shared for
information
13 June 2019 Stoke OSC No minutes received
18 June 2019 Patient Congress No minutes received
19 June 2019 Staff away day No minutes received
19 June 2019 Newcastle Health, Wellbeing and Partnerships
Scrutiny Committee
Draft minutes published online, included in
section 5.5.2
20 June 2019 Adult and Neighbourhoods OSC Response received as correspondence
25 June 2019 Staffordshire Moorlands District Council: Health
Overview and Scrutiny Panel Meeting
Response / summary of meeting received
as correspondence and minutes received
15 July 2019 Healthy Staffordshire Select Committee Response / summary of meeting received
as correspondence
31 July 2019 Tamworth OSC Brief meeting, not minuted
5 September 2019 Staffordshire Health and Wellbeing Board Briefing was shared virtually with members
during the consultation
Page 15
15 | NHS Midlands & Lancashire Commissioning Support Unit
Correspondence
In addition to the survey and public events, members of the public and other stakeholders independently
shared their thoughts and views using a range of correspondence methods. These included emails sent to
the consultation mailbox and written correspondence sent to the CCGs.
All correspondence has been analysed as part of the reporting process. Table 8 details the correspondence
received. See Appendix 2 for details of organisations sending correspondence.
Table 8. Correspondence received
Respondent type Email Letter Total
Member of the public 7 1 8
NHS Trust 0 3 3
Local authority / council 7 2 9
Patient representative group 0 2 2
Charity / voluntary organisation 0 1 1
MP / councillor 3 1 4
Total 17 10 27
Page 16
16 | NHS Midlands & Lancashire Commissioning Support Unit
4 Respondent profiling In this section, the respondents to the consultation are profiled. This section includes a breakdown of the
responses by type of engagement, a breakdown of survey responses by CCG area and response type, as
well as demographic information for those who indicated they were responding as a member of the public in
the survey.
Table 9 shows the numbers of respondents and participants.
Table 9. Number of respondents and participants
Engagement channel Number of respondents and participants
Consultation survey 76 respondents in total
(including paper and online)
Written correspondence 27 pieces of written correspondence received,
including letters and emails
Public events 8 public events held with 80 attendees in total*
*Only two of the 80 participants returned their demographic profiling questionnaire. A demographic profile summary of these
participants can be found in Appendix 3.
Table 10 shows the respondent types completing the survey.
Table 10. Survey respondent types
Survey respondent types Number of respondents %
As a member of the public 54 71%
On behalf of an NHS organisation 5 7%
On behalf of another public sector organisation 1 1%
On behalf of another organisation 2 3%
On behalf of a patient representative organisation 14 18%
On behalf of a voluntary organisation 7 9% Base 76
NB: Some respondents selected more than one option.
Table 11 presents the survey respondents by CCG area. Respondents were asked to provide their postcode, which was used to determine which CCG area they were from.
Table 11. Respondents by CCG area
CCG area Number of respondents %
Cannock Chase CCG 8 11%
East Staffordshire CCG 8 11%
North Staffordshire CCG 16 21%
South East Staffordshire and Seisdon Peninsula CCG 23 30%
Stafford and Surrounds CCG 9 12%
Stoke-on-Trent CCG 8 11%
Unknown 4 5% Base 76
Page 17
17 | NHS Midlands & Lancashire Commissioning Support Unit
Demographic profile
Table 12 shows a demographic profile of members of the public completing the survey.
Table 12. Profile of members of the public completing the survey
Ethnicity Sexual orientation
White: British 42 88% Heterosexual 29 64%
White: Irish 4 8% Bisexual 3 7%
Mixed: White and Asian 1 2% Prefer not to say 13 29%
Asian/Asian British: Other 1 2% Base 45
Base 48 Relationship status
Age category Married 30 63%
30 - 34 3 6% Single 4 8%
35 - 39 4 8% Divorced 2 4%
40 - 44 2 4% Lives with partner 2 4%
45 - 49 2 4% Widowed 4 8%
50 - 54 2 4% Prefer not to say 6 13%
55 - 59 2 4% Base 48
60 - 64 8 17% Pregnant currently
65 - 69 9 17% Yes 1 2%
70 - 74 9 19% No 38 84%
75 - 79 6 13% Prefer not to say 6 13%
Prefer not to say 2 4% Base 45
Base 48 Recently given birth
Religion Yes - -
No religion 15 36% No 40 89%
Christian 23 55% Prefer not to say 5 11%
Jewish 1 2% Base 45
Muslim 1 2% Health problem or disability
Any other religion 2 5% Yes, limited a lot 4 9%
Base 42 Yes, limited a little 12 27%
Sex No 29 64%
Male 20 41% Base 45
Female 25 51% Disability
Prefer not to say 4 8% Physical disability 5 26%
Base 49 Sensory disability 2 11%
Gender identity Mental health need 2 11%
Yes* 1 2% Learning disability or difficulty 1 5%
No 35 81% Other 1 5%
Prefer not to say 7 16% Prefer not to say 6 32%
Base 43 Base 19
Armed services Carer
Yes 2 4% Yes - young person(s) aged under 24 2 4%
No 39 87% Yes - adult(s) aged 25 to 49 1 2%
Prefer not to say 4 9% Yes - person(s) aged over 50 years 6 13%
Base 45 No 35 76%
Prefer not to say 3 7%
Base 45
*Have you gone through any part of a process or do you intend to (including thoughts and actions) to bring your physical sex
appearance and/or your gender role more in line with your gender identity? (This could include changing your name, your
appearance and the way you dress, taking hormones or having gender confirming surgery)
Page 18
18 | NHS Midlands & Lancashire Commissioning Support Unit
Map of consultation respondents
Figure 4 shows the locations of respondents completing the survey. Respondents were asked to provide
their postcode, which has been used to plot respondents’ locations on the map. Postcodes were provided by
72 respondents.
Figure 4. Map of respondents’ location
Page 19
19 | NHS Midlands & Lancashire Commissioning Support Unit
5 Findings This section presents the feedback on the proposals from the consultation survey, events, correspondence
and other channels. This section is structured as follows:
• Reporting and analysis notes
• Views on option 1
• Views on option 2
• Other suggested options.
Reporting and analysis notes
The consultation survey used a combination of ‘open text’ questions, for respondents to make written
comments and ‘closed’ questions where respondents ‘ticked’ their response to a number of pre-set
responses.
For the open questions, a random sample of responses from each question were read and the key themes
(codes) mentioned by respondents were identified. This was undertaken for every open question. Some
codes were replicable across more than one question, while others were specific to one or two questions.
This means that every comment was coded, because the list of themes was not predetermined, but instead
emerged from the responses received.
The section in the survey around views on the options was split into ‘views on option 1’ and ‘views on option
2’. The structure of the findings section mirrors this. However, some respondents chose to give their
feedback on option 2 in the option 1 section of the survey. Therefore, to gain a full picture of respondents’
views on each option, both sections should be read.
For survey responses, results are shown by CCG area. Respondents were asked to provide their postcode,
which was used to identify CCG area. Results are also shown by respondent type. Some respondents to the
survey selected multiple respondent types – those that selected both member of the public and on behalf of
an organisation have been treated as organisational responses.
Page 20
20 | NHS Midlands & Lancashire Commissioning Support Unit
Views on option 1
This section presents views on option 1: keep the current arrangements of six separate CCGs under a
single leadership team.
Feedback from the survey
Respondents were asked on a scale of 1 to 5 the extent to which they supported option 1, with 5 being very
supportive and 1 not at all supportive. Table 13 shows the feedback.
Overall, 29 (45%) of respondents expressed support for option 1.
Table 13. Option 1: Keep the current arrangements of six separate CCGs under a single leadership team
Level of support
Total
CCG Respondent type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r /
oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive
org
an
isation
Supportive (4 or 5)
45% 57% 63% 33% 50% 13% 63% 33% 40% 43% 56%
Neutral (3)
23% 14% 38% 33% 13% 25% 25% - 24% 14% 25%
Not supportive (1 or 2)
32% 29% - 33% 38% 63% 13% 67% 36% 43% 19%
Base 65 7 8 15 16 8 8 3 42 7 16
When comparing feedback by CCG area, support was highest among respondents from East Staffordshire
(5 / 63%) and Stoke-on-Trent (5 / 63%) and lowest in Stafford and Surrounds (1 / 13%).
When comparing feedback by respondent type, support was highest among voluntary / patient
representative organisations (9 / 56%) and lowest among members of the public (17 / 40%).
Page 21
21 | NHS Midlands & Lancashire Commissioning Support Unit
Table 14 shows the feedback when respondents were asked what they agreed with around option 1.
The key themes raised were:
• Option 1 ensures a better understanding of local issues more tailored to local needs (21)
• Option 1 ensures local representation and involvement (12)
• Local representation is important (9).
Table 14. Option 1: What do you agree with?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke
-on-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Option 1 ensures a better understanding of local issues more tailored to local needs
21 2 3 5 6 1 4 - 13 1 7
Option 1 ensures local representation and involvement
12 3 3 1 2 - 3 - 6 1 5
Local representation is important 9 - 2 3 2 2 - - 5 1 3
Six CCGs is an inefficient use of resources / one CCG is more efficient
8 1 - 2 1 3 - 1 4 2 2
A single leadership team is needed 8 1 1 - 5 1 - - 6 - 2
General comment in agreement with option 1 7 1 - 1 1 - 3 1 4 1 2
The current system works effectively 6 1 2 - 1 1 1 - 3 2 1
Option 2 would improve consistency across the area / six CCGs results in inconsistencies
4 - - 1 - 3 - - 2 1 1
General comment in agreement with option 2 3 1 - 1 1 - - - 2 - 1
General comment in disagreement with option 1 2 - - - 2 - - - 2 - -
General comment in disagreement with option 2 2 1 - - - 1 - - 1 - 1
Re-organisation is costly / unnecessary 1 - - - - 1 - - 1 - -
A separate CCG for Stoke-on-Trent and/or Stoke-on-Trent and Northern Staffordshire
1 1 - - - - - - - - 1
Other 1 - - - - - - 1 - 1 - Base 66 8 8 12 18 9 8 3 42 7 17
Key themes by CCG area:
• Cannock Chase: Option 1 ensures local representation and involvement (3)
• East Staffordshire: Option 1 ensures a better understanding of local issues more tailored to local
needs (3), Option 1 ensures local representation and involvement (3)
• North Staffordshire: Option 1 ensures a better understanding of local issues more tailored to local
needs (5)
• South East Staffordshire and Seisdon Peninsula: Option 1 ensures a better understanding of
local issues more tailored to local needs (6)
• Stafford and Surrounds: Six CCGs is an inefficient use of resources / one CCG is more efficient
(3), Option 2 would improve consistency across the area / six CCGs results in inconsistencies (3)
• Stoke-on-Trent: Option 1 ensures a better understanding of local issues more tailored to local
needs (4).
Page 22
22 | NHS Midlands & Lancashire Commissioning Support Unit
Key themes by respondent type:
• Member of the public: Option 1 ensures a better understanding of local issues more tailored to
local needs (13)
• NHS / public sector / other organisation: Six CCGs is an inefficient use of resources / one CCG is
more efficient (2), The current system works effectively (2)
• Voluntary / patient representative organisation: Option 1 ensures a better understanding of local
issues more tailored to local needs (7).
Table 15 shows the feedback when respondents were asked if they had any concerns or felt that there were
any groups or individuals they thought may be negatively impacted by this option.
The key themes raised were:
• Consider the demographic / geographic differences across the areas (14)
• Consider the need for equity across different areas (7).
Page 23
23 | NHS Midlands & Lancashire Commissioning Support Unit
Table 15. Option 1: Do you have any concerns or are there any groups or individuals you think may be negatively impacted by this option?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Consider the demographic / geographic differences across the areas
14 1 2 3 4 1 2 1 9 2 3
Consider the need for equity across different areas 7 1 1 1 2 1 1 - 4 1 2
Option 2 would focus resources in Stoke-on-Trent / urban areas
4 2 - 1 1 - - - 1 - 3
Option 2 may result in a loss of understanding of local issues / option 1 has a more local focus
4 - 1 1 1 - 1 - 1 1 2
Consider the need to maintain service provision locally
4 - - - 2 1 1 - 4 - -
Consider the need for adequate funding 3 - - - 2 - - 1 2 1 -
Re-organising structures negatively impacts on patients
3 1 - 1 - 1 - - 2 - 1
Consider potential job cuts if option 2 is implemented 3 - - 1 - 2 - - 3 - -
Consider transport issues, parking and non-drivers 3 - - 2 1 - - - 2 - 1
Six CCGs is an inefficient use of resources / one CCG is more efficient
3 - 1 - 1 1 - - 1 - 2
Consider the need for local identity 2 - - - 1 - 1 - - - 2
Consider the need for local involvement (e.g. Patient congress, voluntary groups)
2 - - 2 - - - - - 1 1
Option 2 may reduce involvement of vulnerable and seldom heard groups
2 - 1 - - - 1 - 1 - 1
Consider the need for improved access to services (e.g. appointments)
2 - - - 2 - - - 2 - -
Smaller service providers may be disadvantaged if option 2 is implemented
2 - - 1 - - 1 - 1 - 1
Need to ensure adequate staffing 2 - 1 - - 1 - - 1 1 -
Consider the needs of the elderly 2 - 1 1 - - - - 2 - -
Greater clarity is required on the proposals 1 - - - - - 1 - 1 - -
Consider whether costs can be reduced 1 - - - - - 1 - 1 - -
General comment in agreement with option 1 1 - - - - - 1 - - 1 -
Consider that top-down organisation / top-heavy management could negatively affect patients
1 - - - 1 - - - 1 - -
Stoke-on-Trent may be negatively affected (e.g. loss of funding)
1 - - - - - 1 - - - 1
Consider that option 2 could result in silo working 1 - - - 1 - - - 1 - -
Consider the boundaries of partner organisations 1 - - - - 1 - - - 1 -
No / no concerns / nothing 10 2 1 2 4 1 - - 8 - 2
Other 2 - - - 1 1 - - 2 - - Base 58 5 8 10 17 9 7 2 37 7 14
Key themes by CCG area:
• Cannock Chase: Option 2 would focus resources in Stoke-on-Trent / urban areas (2)
• East Staffordshire: Consider the demographic / geographic differences across the areas (2)
• North Staffordshire: Consider the demographic / geographic differences across the areas (3)
Page 24
24 | NHS Midlands & Lancashire Commissioning Support Unit
• South East Staffordshire and Seisdon Peninsula: Consider the demographic / geographic
differences across the areas (4)
• Stafford and Surrounds: Consider potential job cuts if option 2 is implemented (2)
• Stoke-on-Trent: Consider the demographic / geographic differences across the areas (2).
Key themes by respondent type:
• Member of the public: Consider the demographic / geographic differences across the areas (9)
• NHS / public sector / other organisation: Consider the demographic / geographic differences
across the areas (2)
• Voluntary / patient representative organisation: Consider the demographic / geographic
differences across the areas (3), Option 2 would focus resources in Stoke-on-Trent / urban areas (3).
Page 25
25 | NHS Midlands & Lancashire Commissioning Support Unit
Table 16 shows the feedback when respondents were asked how these negative impacts could be
overcome.
The key themes raised were:
• Keep option 1 / stay as it is (7)
• Option 2 should be implemented (5).
Table 16. Option 1: How could these negative impacts be overcome?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke
-on-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Keep option 1 / stay as it is 7 2 2 - 1 1 1 - 4 - 3
Option 2 should be implemented 5 - - 1 2 2 - - 2 1 2
Consider the demographic / geographic differences across the areas
4 - - 1 1 - 1 1 1 1 2
Involve patients and communities in decision making 4 - 1 3 - - - - 1 2 1
Ensure adequate local service provision and quality of care
4 - - 2 2 - - - 3 - 1
More funding is required 4 1 1 - 1 1 - - 3 - 1
Ensure suitable staff are employed 3 - 1 - - 2 - - 2 1 -
CCGs should work together without becoming one CCG
2 - - - 2 - - - 2 - -
Ensure that smaller areas retain a voice 2 - - 1 1 - - - - 1 1
Ensure standards are equitable across the CCGs 2 - - - - - 2 - - 1 1
Consider the need for improved access to services (e.g. appointments)
2 - - - 2 - - - 2 - -
Ensure governance is effective 2 - - - - - 2 - - 1 1
A separate CCG for Stoke-on-Trent and/or Stoke-on-Trent and Northern Staffordshire
2 1 - - - - - 1 1 - 1
CCG membership should be voluntary 1 - - - - - 1 - 1 - -
Greater partnership working across sectors is required
1 - - - - 1 - - - 1 -
Consider reducing CCGs without combining as one 1 - 1 - - - - - 1 - -
Improve Primary Care Networks 1 - - - - 1 - - 1 - -
Ensure fair / equal distribution of funding if option 2 is implemented
1 - - 1 - - - - - 1 -
Ensure decisions are made locally 1 - - - 1 - - - 1 - - Base 48 5 6 8 11 9 7 2 29 7 12
Key themes by CCG area:
• Cannock Chase: Keep option 1 / stay as it is (2)
• East Staffordshire: Keep option 1 / stay as it is (2)
• North Staffordshire: Involve patients and communities in decision making (3)
• South East Staffordshire and Seisdon Peninsula: Option 2 should be implemented (2), ensure
adequate local service provision and quality of care (2), CCGs should work together without
becoming one CCG (2), consider the need for improved access to services (e.g. appointments) (2)
• Stafford and Surrounds: Option 2 should be implemented (2), ensure suitable staff are employed
(2)
Page 26
26 | NHS Midlands & Lancashire Commissioning Support Unit
• Stoke-on-Trent: Ensure standards are equitable across the CCGs (2), ensure governance is
effective (2).
Key themes by respondent type:
• Member of the public: Keep option 1 / stay as it is (4)
• NHS / public sector / other organisation: Involve patients and communities in decision making (2)
• Voluntary / patient representative organisation: Keep option 1 / stay as it is (3).
Page 27
27 | NHS Midlands & Lancashire Commissioning Support Unit
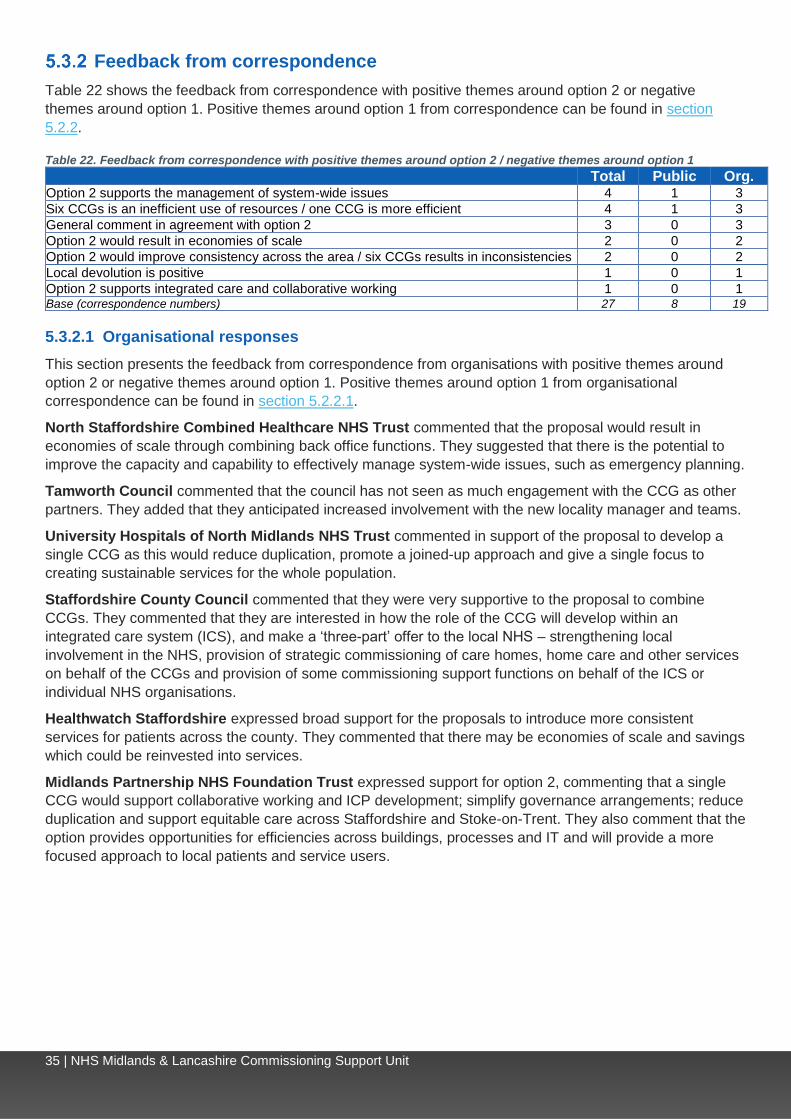
Feedback from correspondence
Table 17 shows the feedback from correspondence with positive themes around option 1 or negative
themes around option 2. Positive themes around option 2 from correspondence can be found in section
5.3.2.
Table 17. Feedback from correspondence with positive themes around option 1 / negative themes around option 2
Total Public Org.
Option 2 may result in a loss of understanding of local issues / option 1 has a more local focus
11 1 10
Stoke-on-Trent may be negatively affected by option 2 (e.g. loss of funding) 6 1 5
General comment in disagreement with option 2 4 1 3
Option 1 ensures local representation and involvement / option 2 will reduce involvement
3 0 3
Proposed savings will not be realised 2 1 1
Re-organisation is costly / unnecessary 2 1 1
Keep option 1 / stay as it is 3 1 2
Re-organising structures negatively impacts on patients 3 0 3
General comment in agreement with option 1 2 0 2
Proposal will adversely affect system management 1 1 0
Staffordshire is a large area for one CCG 1 0 1
Cannock may be negatively affected 1 0 1
Option 2 may reduce involvement of vulnerable and seldom heard groups 1 0 1
Smaller service providers may be disadvantaged if option 2 is implemented 1 0 1 Base (correspondence numbers) 27 8 19
5.2.2.1 Organisational responses
This section presents the feedback from correspondence submitted by organisations or MPs with positive
themes around option 1 or negative themes around option 2. Positive themes around option 2 from
organisational correspondence can be found in section 5.3.2.1.
Stoke-on-Trent City Council (the Deputy Leader of the Council and Lead Member for Health and Social
Care) commented in disagreement with option 2. They reasoned that as Stoke-on-Trent is the 14th most
deprived local authority in the country with significant health inequalities, it is therefore different
demographically and geographically from Staffordshire. They expressed concern that Stoke-on-Trent would
lose local focus and decision-making capability, funding would move from North to South and that there
would be a shift in emphasis away from the population’s need to resolve financial pressures.
Stoke-on-Trent City Council Adults and Neighbourhoods Overview and Scrutiny Committee
responded in support of option 1 (retaining six CCGs) and against option 2 (creating a single CCG). They
expressed concern that a single CCG would result in a postcode lottery with variations in service provision.
They commented that the proposal could reduce facilities in Stoke-on-Trent and lead to residents having to
travel further. They argued that the proposal would result in a ‘one-size-fits-all’ commissioning model with
services not being commissioned according to need.
Paul Farrelly MP commented in opposition to option 2. They suggested that health services are more
responsive to local needs when they are organised locally. Concerned that the CCG will be rooted in
Stafford, they argued that the county is a very diverse area with no natural connection between localities.
Gareth Snell MP also commented in opposition to option 2. They highlighted concerns over the
management and accountability of a single CCG; inadequate CCG ratings and impacts on budgets and cuts
to services. They also commented that smaller service providers may be disadvantaged with worsening
relationships with the community and voluntary sector, which could disadvantage those with specific needs.
Ruth Smeeth MP also raised opposition to option 2. They commented that due to the current ratings of five
of the six CCGs, they felt that the CCGs were not stable enough to become a single CCG without adversely
affecting service provision. They commented that North Staffordshire and Stoke-on-Trent CCGs currently
have a higher funding allocation, which would not be protected in a single CCG. They also highlighted
concerns over governance and that local needs would not be represented as well in a single CCG.
Page 28
28 | NHS Midlands & Lancashire Commissioning Support Unit
Feedback was received from Reach (part of Asist), following a meeting held with members of the public with
learning difficulties. They highlighted concerns that one CCG would be too big to support the health needs
of the whole of Staffordshire, as the area is too big and would need to ensure that finance and information
was adequate for each locality.
Staffordshire Moorlands District Council commented that Staffordshire Moorlands has a large rural
population with different needs. They expressed concern that localism would be lost if the CCGs were to
merge into one organisation.
Cannock Chase Council commented in opposition to the proposed creation of a single commissioning
organisation. They commented that it is a cost-cutting measure, not in the best interests of patients and
carers within Cannock Chase. They expressed concern that the merger would see resources diverted away
from Cannock Chase, a loss of influence over local clinical commissioning decisions and worsening of
existing poor engagement with the council.
Hednesford Town Council commented that that governance structures of CCGs should remain
autonomous and local to their represented communities. The CCG needs to remain at local level in order to
be in touch with local needs.
A Newcastle-under-Lyme Borough Councillor commented in supported of retaining the current six CCGs.
Page 29
29 | NHS Midlands & Lancashire Commissioning Support Unit
Views on option 2
This section presents the views on option 2: develop a new, single CCG.
Feedback from the survey
Respondents were asked on a scale of 1 to 5 the extent to which they supported option 2, with 5 being very
supportive and 1 not at all supportive. Table 18 shows the feedback.
Overall, 30 (42%) of respondents expressed support for option 2.
Table 18. Option 2: Develop a new, single CCG
Level of support
Total
CCG Respondent type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r /
oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive
org
an
isation
Supportive (4 or 5)
42% 38% 13% 38% 50% 78% 38% - 43% 43% 40%
Neutral (3)
14% - 25% 23% 18% 11% - - 18% 14% -
Not supportive (1 or 2)
44% 63% 63% 38% 32% 11% 63% 100% 39% 43% 60%
Base 71 8 8 13 22 9 8 3 49 7 15
When comparing feedback by CCG area, support was highest among respondents from Stafford and
Surrounds (7 / 78%) and lowest in East Staffordshire (1 / 13%).
When comparing feedback by respondent type, support was at similar levels across all respondent types.
Page 30
30 | NHS Midlands & Lancashire Commissioning Support Unit
Table 19 shows the feedback when respondents were asked what they agreed with around option 2.
The key themes raised were:
• Six CCGs is an inefficient use of resources / one CCG is more efficient (27)
• General comment in disagreement with option 2 (13).
Table 19. Option 2: What do you agree with?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East S
taff
ord
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Six CCGs is an inefficient use of resources / one CCG is more efficient
27 3 3 3 9 5 4 - 21 3 3
General comment in disagreement with option 2 13 2 2 2 3 - 3 1 7 2 4
Option 2 would improve consistency across the area / six CCGs results in inconsistencies
7 - 1 2 2 2 - - 6 - 1
Option 2 would result in economies of scale 6 - 1 2 1 2 - - 4 - 2
Local representation is important 6 - 3 1 1 1 - - 4 - 2
General comment in agreement with option 2 6 - - 2 2 - 2 - 3 1 2
Option 2 supports the management of system-wide issues
5 - - 1 3 - 1 - 3 1 1
Option 1 ensures a better understanding of local issues more tailored to local needs
3 1 - 2 - - - - 1 - 2
A single leadership team is needed 3 - - 1 2 - - - 2 1 -
Option 2 supports the delivery of the NHS Long Term Plan
2 - 1 - - - 1 - - 1 1
General comment in agreement with option 1 1 - - - - - 1 - - - 1
Other 7 1 - 2 2 1 - 1 1 1 5 Base 65 6 8 14 19 8 8 2 43 7 15
Key themes by CCG area:
• Cannock Chase: Six CCGs is an inefficient use of resources / one CCG is more efficient (3)
• East Staffordshire: Six CCGs is an inefficient use of resources / one CCG is more efficient (3),
Local representation is important (3)
• North Staffordshire: Six CCGs is an inefficient use of resources / one CCG is more efficient (3)
• South East Staffordshire and Seisdon Peninsula: Six CCGs is an inefficient use of resources /
one CCG is more efficient (9)
• Stafford and Surrounds: Six CCGs is an inefficient use of resources / one CCG is more efficient (5)
• Stoke-on-Trent: Six CCGs is an inefficient use of resources / one CCG is more efficient (4).
Key themes by respondent type:
• Member of the public: Six CCGs is an inefficient use of resources / one CCG is more efficient (21)
• NHS / public sector / other organisation: Six CCGs is an inefficient use of resources / one CCG is
more efficient (3)
• Voluntary / patient representative organisation: General comment in disagreement with option 2
(4).
Page 31
31 | NHS Midlands & Lancashire Commissioning Support Unit
Table 20 shows the feedback when respondents were asked if they had any concerns or felt that there were
any groups or individuals they thought may be negatively impacted by this option.
The key themes raised were:
• Consider the demographic / geographic differences across the areas (12)
• Option 2 would focus resources in Stoke-on-Trent / urban areas (10)
• Consider the need for local involvement (e.g. Patient congress, voluntary groups) (9).
Table 20. Option 2. Do you have any concerns or are there any groups or individuals you think may be negatively impacted by this option?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East S
taff
ord
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Consider the demographic / geographic differences across the areas
12 1 2 3 3 1 2 - 6 1 5
Option 2 would focus resources in Stoke-on-Trent / urban areas
10 2 1 2 5 - - - 6 1 3
Consider the need for local involvement (e.g. Patient congress, voluntary groups)
9 1 1 2 3 - 2 - 7 1 1
Option 2 may result in a loss of understanding of local issues / option 1 has a more local focus
8 1 - 2 2 2 1 - 7 - 1
Consider the need for equity across different areas 4 1 - 1 2 - - - 3 - 1
Stoke-on-Trent may be negatively affected (e.g. loss of funding)
4 - - 1 - 1 1 1 2 1 1
Option 2 may reduce involvement of vulnerable and seldom heard groups
4 - - - 1 - 3 - 2 - 2
Consider the need to maintain service provision locally
4 - 1 - 2 1 - - 2 1 1
No / no concerns / nothing 4 - 1 - 2 1 - - 4 - -
Consider the need for adequate funding 3 - 2 - - - - 1 1 1 1
Consider the need for improved access to services (e.g. appointments)
3 - - 1 2 - - - 3 - -
Consider potential job cuts if option 2 is implemented 3 - - 1 1 1 - - 3 - -
Re-organising structures negatively impacts on patients
2 - 2 - - - - - 1 1 -
Consider the boundaries of partner organisations 2 - - - - 1 1 - - - 2
Smaller service providers may be disadvantaged if option 2 is implemented
2 - - - - - 2 - - - 2
Need to ensure adequate staffing 2 - - - 2 - - - 2 - -
Consider reducing CCGs without combining as one 2 1 - - - 1 - - 1 - 1
Consider whether costs can be reduced 1 - - 1 - - - - - 1 -
A standardised IT system is required (e.g. appointment booking, medical records)
1 - - - 1 - - - 1 - -
Consider transport issues, parking and non-drivers 1 - - - 1 - - - 1 - -
Consider the needs of the elderly 1 - - - 1 - - - 1 - -
Other 9 - - 4 1 1 1 2 5 1 3 Base 67 5 7 15 20 8 8 4 44 7 16
Page 32
32 | NHS Midlands & Lancashire Commissioning Support Unit
Key themes by CCG area:
• Cannock Chase: Option 2 would focus resources in Stoke-on-Trent / urban areas (2)
• East Staffordshire: Consider the demographic / geographic differences across the areas (2),
Consider the need for adequate funding (2), re-organising structures negatively impacts on patients
(2)
• North Staffordshire: Consider the demographic / geographic differences across the areas (3)
• South East Staffordshire and Seisdon Peninsula: Option 2 would focus resources in Stoke-on-
Trent / urban areas (5)
• Stafford and Surrounds: Option 2 may result in a loss of understanding of local issues / option 1
has a more local focus (2)
• Stoke-on-Trent: Option 2 may reduce involvement of vulnerable and seldom heard groups (3).
Key themes by respondent type:
• Member of the public: Consider the need for local involvement (e.g. Patient congress, voluntary
groups) (7), option 2 may result in a loss of understanding of local issues / option 1 has a more local
focus (7)
• NHS / public sector / other organisation: Limited comments raised
• Voluntary / patient representative organisation: Consider the demographic / geographic
differences across the areas (5).
Page 33
33 | NHS Midlands & Lancashire Commissioning Support Unit
Table 21 shows the feedback when respondents were asked how these negative impacts could be
overcome.
The key themes raised were:
• Involve patients and communities in decision making (20)
• Keep option 1 / stay as it is (10)
• Consider the demographic / geographic differences across the areas (8).
Table 21. How could these negative impacts be overcome?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East S
taff
ord
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke
-on-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Involve patients and communities in decision making 20 - 4 4 8 2 2 - 12 3 5
Keep option 1 / stay as it is 10 2 - 2 2 - 3 1 6 - 4
Consider the demographic / geographic differences across the areas
8 - - 1 3 - 4 - 4 1 3
Ensure governance is effective 5 2 1 - - 1 1 - 2 2 1
Ensure suitable staff are employed 4 - - 1 2 1 - - 4 - -
Ensure adequate local service provision and quality of care
4 - - 1 2 1 - - 2 1 1
Ensure decisions are made locally 4 - - 1 1 1 1 - 1 2 1
A separate CCG for Stoke-on-Trent and/or Stoke-on-Trent and Northern Staffordshire
2 1 - 1 - - - - 1 - 1
Greater partnership working across sectors is required
2 - 1 - - 1 - - - 1 1
Ensure standards are equitable across the CCGs 2 - - - - 1 1 - 1 1 -
Consider the need for improved access to services (e.g. appointments)
2 - - 2 - - - - 1 - 1
More funding is required 2 1 - - - 1 - - 1 - 1
Ensure fair / equal distribution of funding if option 2 is implemented
2 - 1 - 1 - - - 2 - -
Improve Primary Care Networks 1 - - 1 - - - - - - 1
Involve GPs in decision making 1 - - 1 - - - - 1 - -
Other 16 1 2 3 5 3 - 2 12 2 2 Base 63 5 7 13 19 8 8 3 42 7 14
Key themes by CCG area:
• Cannock Chase: Keep option 1 / stay as it is (2), ensure governance is effective (2)
• East Staffordshire: Involve patients and communities in decision making (4)
• North Staffordshire: Involve patients and communities in decision making (4)
• South East Staffordshire and Seisdon Peninsula: Involve patients and communities in decision
making (8)
• Stafford and Surrounds: Involve patients and communities in decision making (2)
• Stoke-on-Trent: Consider the demographic / geographic differences across the areas (4).
Page 34
34 | NHS Midlands & Lancashire Commissioning Support Unit
Key themes by respondent type:
• Member of the public: Involve patients and communities in decision making (12)
• NHS / public sector / other organisation: Involve patients and communities in decision making (3)
• Voluntary / patient representative organisation: Involve patients and communities in decision
making (5).
5.3.1.1 Organisational responses
A survey respondent indicating they were responding on behalf of Midlands and Lancashire
Commissioning Support Unit commented that they supported option 2, as it would benefit the health
system in Staffordshire in delivering the NHS Long Term Plan and would provide an opportunity to deliver
quality at-scale commissioning solutions. They also commented that the model supports better integration
across commissioners, providers and primary care, and would reduce duplication with a much more
streamlined, less bureaucratic delegations and decision-making processes.
Page 35
35 | NHS Midlands & Lancashire Commissioning Support Unit
Feedback from correspondence
Table 22 shows the feedback from correspondence with positive themes around option 2 or negative
themes around option 1. Positive themes around option 1 from correspondence can be found in section
5.2.2.
Table 22. Feedback from correspondence with positive themes around option 2 / negative themes around option 1
Total Public Org. Option 2 supports the management of system-wide issues 4 1 3
Six CCGs is an inefficient use of resources / one CCG is more efficient 4 1 3
General comment in agreement with option 2 3 0 3
Option 2 would result in economies of scale 2 0 2
Option 2 would improve consistency across the area / six CCGs results in inconsistencies 2 0 2
Local devolution is positive 1 0 1
Option 2 supports integrated care and collaborative working 1 0 1 Base (correspondence numbers) 27 8 19
5.3.2.1 Organisational responses
This section presents the feedback from correspondence from organisations with positive themes around
option 2 or negative themes around option 1. Positive themes around option 1 from organisational
correspondence can be found in section 5.2.2.1.
North Staffordshire Combined Healthcare NHS Trust commented that the proposal would result in
economies of scale through combining back office functions. They suggested that there is the potential to
improve the capacity and capability to effectively manage system-wide issues, such as emergency planning.
Tamworth Council commented that the council has not seen as much engagement with the CCG as other
partners. They added that they anticipated increased involvement with the new locality manager and teams.
University Hospitals of North Midlands NHS Trust commented in support of the proposal to develop a
single CCG as this would reduce duplication, promote a joined-up approach and give a single focus to
creating sustainable services for the whole population.
Staffordshire County Council commented that they were very supportive to the proposal to combine
CCGs. They commented that they are interested in how the role of the CCG will develop within an
integrated care system (ICS), and make a ‘three-part’ offer to the local NHS – strengthening local
involvement in the NHS, provision of strategic commissioning of care homes, home care and other services
on behalf of the CCGs and provision of some commissioning support functions on behalf of the ICS or
individual NHS organisations.
Healthwatch Staffordshire expressed broad support for the proposals to introduce more consistent
services for patients across the county. They commented that there may be economies of scale and savings
which could be reinvested into services.
Midlands Partnership NHS Foundation Trust expressed support for option 2, commenting that a single
CCG would support collaborative working and ICP development; simplify governance arrangements; reduce
duplication and support equitable care across Staffordshire and Stoke-on-Trent. They also comment that the
option provides opportunities for efficiencies across buildings, processes and IT and will provide a more
focused approach to local patients and service users.
Page 36
36 | NHS Midlands & Lancashire Commissioning Support Unit
Alternative options
This section presents feedback on alternative options.
Feedback from the survey
Table 23 shows the feedback when respondents were asked if they had any other suggested options that
should be considered.
The key themes raised were:
• Stoke-on-Trent should be its own CCG (6)
• Involve patients and communities in decision making (6)
• Improve partnership working across CCGs (5).
Table 23. Do you have any other suggested options that we should consider?
Total
CCG Respondent
type
Cann
ock C
hase
East
Sta
fford
shire
Nort
h S
taff
ord
shire
South
East
Sta
fford
shire
an
d
Seis
don P
enin
su
la
Sta
fford
and S
urr
ou
nds
Sto
ke-o
n-T
rent
Unknow
n
Mem
ber
of
the p
ublic
NH
S / p
ub
lic s
ecto
r / oth
er
org
an
isation
Volu
nta
ry / p
atie
nt
repre
senta
tive o
rgan
isation
Stoke-on-Trent should be its own CCG 6 2 - 1 - - 2 1 3 - 3
Involve patients and communities in decision making 6 1 - 1 2 1 1 - 4 - 2
Improve partnership working across CCGs 5 1 1 - 2 1 - - 1 2 2
Form a Northern Staffordshire CCG and a Southern Staffordshire CCG
4 - - 3 - 1 - - 2 1 1
Change is not necessary 3 1 - - 1 1 - - 2 - 1
Form three CCGs in the area 2 - - 1 - - 1 - 1 1 -
GPs and practice staff should be directly employed by the NHS
1 - - - - - 1 - 1 - -
South East Staffordshire and Seisdon Peninsula CCG should be part of Wolverhampton or Dudley CCG
1 - - - 1 - - - 1 - -
Improve partnership working with other CCGs (e.g. Derbyshire CCGs)
1 - 1 - - - - - - - 1
Reduce office locations 1 - - - 1 - - - 1 - -
Consider greater patient education 1 - - - 1 - - - 1 - -
No / nothing 12 - 2 2 3 3 1 1 8 2 2
Other 13 - 1 - 8 2 1 1 11 - 2 Base 53 4 5 8 17 9 7 3 34 6 13
Key themes by CCG area:
• Cannock Chase: Stoke-on-Trent should be its own CCG (2)
• East Staffordshire: Limited comments raised
• North Staffordshire: Form a Northern Staffordshire CCG and a Southern Staffordshire CCG (3)
• South East Staffordshire and Seisdon Peninsula: Involve patients and communities in decision
making (2), improve partnership working across CCGs (2)
• Stafford and Surrounds: Limited comments raised
• Stoke-on-Trent: Stoke-on-Trent should be its own CCG (2).
Page 37
37 | NHS Midlands & Lancashire Commissioning Support Unit
Key themes by respondent type:
• Member of the public: Involve patients and communities in decision making (4)
• NHS / public sector / other organisation: Improve partnership working across CCGs (2)
• Voluntary / patient representative organisation: Stoke-on-Trent should be its own CCG (3).
Page 38
38 | NHS Midlands & Lancashire Commissioning Support Unit
Feedback from correspondence
Table 24 shows the alternative options outlined in the correspondence received
Table 24. Feedback from correspondence with alternative options Total Public Org.
Stoke-on-Trent should be its own CCG 3 0 3
Consider a Northern Staffordshire CCG (e.g. combining Stoke-on-Trent and North Staffordshire CCGs)
2 0 2
Form three CCGs in the area 1 0 1
CCGs should work together without becoming one CCG 1 0 1 Base (correspondence numbers) 27 8 19
5.4.2.1 Organisational responses
Healthwatch Stoke-on-Trent requested detail on why a Northern Staffordshire CCG is not an option.
Stoke-on-Trent City Council (the Deputy Leader of the City Council and Lead Member for Health and
Social Care) made two alternative suggestions:
• Stoke-on-Trent should remain its own CCG
• There should be an amalgamated CCG across Stoke-on-Trent and North Staffordshire on the same
geographic boundaries as the Northern Alliance.
Stoke-on-Trent City Council Adults and Neighbourhoods Overview and Scrutiny Committee also
made two alternative suggestions:
• One CCG for Stoke-on-Trent and another CCG for the remainder of Staffordshire
• Three CCGs based on the three divisional committees for the North, South East and South West as
outlined within the proposed governance structure in the consultation document.
Page 39
39 | NHS Midlands & Lancashire Commissioning Support Unit
Considerations raised
Feedback from correspondence
Table 25 presents the themes for consideration raised in correspondence, as well as comments on the
consultation process.
Table 25. Themes for consideration and comments on consultation process raised in correspondence
Total Public Org.
For consideration
Consider the demographic / geographic differences across the areas 8 1 7
Consider deprivation in Stoke-on-Trent 7 1 6
Consider the need to maintain service provision locally 5 0 5
Consider the impact on wider stakeholders (e.g. Together We're Better) 5 2 3
Patient care is more important than NHS structures 4 2 2
Involve patients and communities in decision making 4 1 3
Consider the need for equity across different areas 3 1 2
Consider implications on funding 2 0 2
Consider the need for improved access to services (e.g. appointments) 2 0 2
Consider potential job cuts if option 2 is implemented 2 0 2
Consider the financial position of CCGs 2 1 1
Consider local service provision 2 1 1
Consider the need for adequate funding 1 1 0
Ensure fair / equal distribution of funding if option 2 is implemented 1 0 1
Consider how the impact of changes will be measured 1 0 1
Involve GPs in decision making 1 0 1
Ensure decisions are made locally 1 0 1
Consider the role of a single CCG in an integrated care system 1 0 1
Consider impacts on access to services 1 0 1
Consider quality of care by commissioned providers 1 1 0
Consider the need for cultural change 1 0 1
Comments on
consultation process
Consider the need for engagement across the consultation area 4 3 1
Consider the need for greater public awareness of the proposals 3 0 3
Greater clarity is required on the proposals 3 1 2
Consultation should not be necessary for these proposals (e.g. waste of money / no public interest)
1 1 0
Base (correspondence numbers) 27 8 19
5.5.1.1 Organisational responses Healthy Staffordshire Select Committee expressed concern that the proposed move was financially led,
and that commissioning policies had not been mentioned. They commented that the North and South of the
county have differing population needs. They expressed concern that commissioning policies would be
changed to the detriment of the public. They felt that cultural change was needed more than changing the
structures.
Jeremy Lefroy MP queried how funding would be managed, given that CCGs currently receive different
levels of funding.
Page 40
40 | NHS Midlands & Lancashire Commissioning Support Unit
Other comments
Feedback from public events
This section summarises the feedback from the public events. See Appendix 3 for coded queries and
feedback from public events.
Cannock Chase CCG
At the Cannock public event, considerations were raised over the need for improved access to services (e.g.
appointments) and transport issues, parking and non-drivers. Queries were also raised regarding the
consultation process and the impacts on service provision.
East Staffordshire CCG
At the Burton public event, queries were raised around decision making processes – impacts on boards and
committees, as well as budgets and funding allocation.
North Staffordshire CCG
At the Leek public event, comments included the need to involve patients and communities in decision
making – greater partnership working across sectors is required, local representation is important and option
1 ensures a better understanding of local issues as it is more tailored to local needs. Queries were raised
regarding the consultation process rationale for the single CCG.
South East Staffordshire and Seisdon Peninsula CCG
At the Lichfield public event, comments in support of option 2 were raised, including: six CCGs is an
inefficient use of resources / one CCG is more efficient, and option 2 supports the delivery of the NHS Long
Term Plan. Considerations were also raised, including: the importance of local representation, requirements
for a standardised IT system (e.g. appointment booking, medical records) and the need to consider the
demographic / geographic differences across the areas.
At the Tamworth public event, comments included that option 2 would support the management of system-
wide issues. Queries were also raised, including: the impact on boards and committees, and access to
records.
At the Codsall public event, comments included the need to maintain service provision locally. Queries were
also raised around guidelines / NHS England procedures.
Stafford and Surrounds CCG
At the Stafford public event, comments included greater clarity being required on the proposals – local
representation being important and the need for improved access to services. Queries were raised around
GP numbers and the impacts of option 2.
Stoke-on-Trent CCG
At the Stoke-on-Trent public event, considerations were raised over the impact on committees and boards
and the need for adequate funding. Other comments included the need for adequate staffing and to involve
patients and communities in decision making. Queries were raised around re-organisation, including the
cost of reorganisation, boundaries / structures of reorganisation and decision-making processes.
Feedback from other consultation meetings
This section presents feedback from other consultation meetings that were minuted.
Cannock Patient District Group
It was queried what would happen if three CCGs agreed to move towards one single strategic organisation
and three did not.
Seisdon Patient District Group
Page 41
41 | NHS Midlands & Lancashire Commissioning Support Unit
Members commented that the title of the new CCG should not include Stoke-on-Trent and wanted
assurance that local considerations would be considered. It was queried whether GPs were in favour of the
merger.
Patient Council Meeting
It was acknowledged that Stoke-on-Trent is a deprived area, but there are also deprived areas in
Staffordshire Moorlands and Cannock Chase that need funding. It was queried whether the single CCG
would change the health postcode lottery; for example, in hearing aid provision. It was also queried whether
some of this alignment work could take place now as there is a single leadership team in place and whether
there would be the same funding per patient across the CCG area. It was commented that members need to
be involved and give feedback and that some services would be better commissioned across a single
footprint, such as child and adolescent mental health commissioned beds.
Staffordshire Moorlands District Council: Health Overview and Scrutiny Panel Meeting
It was commented that the CCGs should recognise the difference in needs of patients and the providers of
care for the North and South of the county, and that Staffordshire Moorlands has different needs to other
areas due to its rural population. Members highlighted concern that as the CCGs had different policies, and
that services provided to patients would be levelled down to the lowest common denominator. Members
were not convinced that a single strategic commissioning organisation would improve the level of service
and patient care provided.
According to this group, the main services the public wish to see improvements to are GP appointments, out
of hours service and an increased number of nursing staff.
It was commented that structural changes had been seen since the 1980s and it seemed that there was a
constant churn of change for little practical result. Members felt that the main driver for change was to
reduce costs and that there was no clear evidence to support changes to social policies. Some members
thought that GPs should be able to influence decision making without a merger of the CCGs. It was also
commented that localism would be lost if the CCGs were to merge into one organisation.
Some members agreed with reduced management within the proposed new structure but had concerns on
how this would fit in with other organisational structures and the voluntary sector.
It was commented that feedback should be gathered more regularly and from a wider group of people. It
was also suggested that there should be a method to measure the impact of the proposed changes.
Newcastle-under-Lyme Health, Wellbeing and Partnerships Scrutiny Committee
Members of the committee engaged in discussions with CCG representatives in attendance. Members felt
uncertain that the requirement for services in respect to elderly people was adequately met. Specific
questions from members included the safeguarding of services and managed care pathways and the
consolidation of maternity services. Concern were raised around the loss of jobs on combining sites and
availability of appointments to patients locally.
Members asked for assurance on the co-existence of urban and rural models and whether the savings
made would be used to purchase extra integrated care packages. Members also asked about the
organisational / geographical barriers to change and the alternative views.
Page 42
42 | NHS Midlands & Lancashire Commissioning Support Unit
6 Conclusions In the survey, a slightly greater proportion of respondents expressed support to keep the current
arrangements, with 29 (45%) of respondents supporting option 1, compared to 30 (42%) of respondents
who supported option 2, to create a single CCG.
A greater proportion of respondents were unsupportive of option 2, with 31 (44%) respondents indicating
they were not supportive, compared to 21 (32%) of respondents for option 1.
Table 26. Summary of support for the options
Supportive
(4 or 5) Neutral
(3) Not supportive
(1 or 2) Base
Option 1: Keep the current arrangements of six separate CCGs under a single leadership team
45% 23% 32% 65
Option 2: Develop a new, single CCG
42% 14% 44% 71
Comments on the options
Support for option 1
In support of option 1, it was commented that retaining six CCGs would ensure a better understanding of
local issues more tailored to local needs and local representation and involvement.
The need to consider the demographic and geographic differences in the area was a key theme throughout
the survey and correspondence (e.g. deprivation in Stoke-on-Trent, rural versus urban).
There was concern that resources would be focused on Stoke-on-Trent / urban areas if option 2 was
implemented. However, there was also concern in the survey and in correspondence that Stoke-on-Trent
would be negatively affected if option 2 was implemented – for example, with a loss of funding.
Organisations commenting in opposition to the proposal to create a single CCG or expressing concerns
included Stoke-on-Trent City Council, Cannock Chase Council, Healthy Staffordshire Select Committee and
Staffordshire Moorlands District Council.
Stoke-on-Trent City Council expressed disagreement with option 2. The Deputy Leader of the Council and
Lead Member for Health and Social Care commented that Stoke-on-Trent is demographically and
geographically different from Staffordshire, and that a single CCG would lose local focus and decision-
making capability. They expressed concern that funding would move from North to South and there would
be a shift in emphasis away from the population’s need to resolve financial pressures. Stoke-on-Trent City
Council Adults and Neighbourhoods Overview and Scrutiny Committee expressed concern that a single
CCG would result in a postcode lottery. They commented that there would be variations in service provision
and facilities in Stoke-on-Trent. They said that the result would be a ‘one-size-fits-all’ commissioning model,
with services not being commissioned according to need.
Healthy Staffordshire Select Committee expressed concern that the proposed move was financially led and
that commissioning policies had not been mentioned. They commented the North and South of the county
have differing population needs.
Cannock Chase Council commented in opposition to the proposed creation of a single commissioning
organisation. They argued that it is a cost-cutting measure – not in the best interests of patients and carers
within Cannock Chase. They commented that a single commissioning organisation would see resources
diverted away from Cannock Chase. They expressed concern that there would be a loss of influence over
local clinical commissioning decisions and worsening of existing poor engagement with the council.
Hednesford Town Council also commented that CCGs should remain local to ensure local representation
and understanding of local needs.
Page 43
43 | NHS Midlands & Lancashire Commissioning Support Unit
Support for option 2
In support of option 2, it was commented that six CCGs are an inefficient use of resources and that one
CCG would be more efficient. Other comments were that option 2 would improve consistency across the
area, as having six CCGs results in inconsistencies whereas option 2 would result in economies of scale.
Organisations expressing broad support for option 2 included NHS Trusts, Staffordshire County Council and
Healthwatch Staffordshire. Both North Staffordshire Combined Healthcare NHS Trust and University
Hospitals of North Midlands NHS Trust commented that the single CCG would support in the management
of system-wide issues. Midlands Partnership NHS Foundation Trust commented that a single CCG would
support collaborative working and ICP development; simplify governance arrangements; reduce duplication
and support equitable care across Staffordshire and Stoke-on-Trent. Healthwatch Staffordshire commented
that the proposal would result in savings that could be reinvested into services.
Alternative options
A key theme in both the survey and correspondence was that Stoke-on-Trent should be a standalone CCG.
This was also highlighted by Stoke-on-Trent City Council (the Deputy Leader of the City Council and Lead
Member for Health and Social Care), who also suggested an amalgamated CCG across Stoke-on-Trent and
North Staffordshire on the same geographic boundaries as the Northern Alliance. Similarly, Stoke-on-Trent
City Council Adults and Neighbourhoods Overview and Scrutiny Committee made two alternative
suggestions: A CCG for Stoke-on-Trent and another CCG for the remainder of Staffordshire or three CCGs
based on the three divisional committees for the North, South East and South West as outlined within the
proposed governance structure in the consultation document.
The need to involve patients and communities in decision-making was another key theme in the survey.
Healthwatch Stoke-on-Trent requested detail on why a Northern Staffordshire CCG is not an option.
Page 44
44 | NHS Midlands & Lancashire Commissioning Support Unit
Appendix 1: Example social media posts
Page 45
45 | NHS Midlands & Lancashire Commissioning Support Unit
Appendix 2: Organisations sending correspondence
Respondent type Organisations and MPs with representatives sending correspondence
Charity / voluntary organisations Reach (part of Asist)
Local authorities
Adults and Neighbourhoods Overview and Scrutiny Committee, Stoke-on-
Trent City Council
Cannock Chase Council
Healthy Staffordshire Select Committee, Staffordshire County Council
Hednesford Town Council
Newcastle-under-Lyme Borough Council
Staffordshire County Council
Staffordshire Moorlands District Council
Stoke-on-Trent City Council
Tamworth Council
MPs
Paul Farrelly MP
Jeremy Lefroy MP
Ruth Smeeth MP
Gareth Snell MP
NHS Trusts
Midlands Partnership NHS Foundation Trust
North Staffordshire Combined Healthcare NHS Trust
University Hospitals North Midlands NHS Trust
Patient representative groups Healthwatch Staffordshire
Healthwatch Stoke-on-Trent
Page 46
46 | NHS Midlands & Lancashire Commissioning Support Unit
Appendix 3: Queries and feedback from public events
Query Total
Event
Bu
rto
n
Ca
nn
oc
k
Le
ek
Se
isd
on
Sta
ffo
rd
Sto
ke
Ta
mw
ort
h
Query regarding consultation process 14 2 4 4 1 1 1 1
Query regarding budgets and funding allocation 8 3 1 1 1 0 1 1
Query regarding decision making processes 8 6 0 0 0 0 2 0
Query regarding guidelines / NHS England procedures 6 0 1 2 2 0 0 1
Query regarding access to records 6 0 0 2 1 0 1 2
Query regarding boundaries / structures of reorganisation 6 0 1 2 1 0 2 0
Query regarding impact on contracting 5 0 0 2 1 0 1 1
Query regarding impact on boards and committees 5 3 0 0 0 0 0 2
Query regarding GP numbers 5 1 0 0 0 2 1 1
Query regarding impacts on service provision 5 1 3 0 0 0 1 0
Query regarding rationale for the single CCG 4 0 0 3 0 1 0 0
Query regarding access to services for patients 4 1 1 1 0 1 0 0
Query regarding office / base locations 4 0 1 1 0 1 1 0
Query regarding implementation of single CCG 3 0 1 1 0 1 0 0
Query regarding cost of re-organisation 3 0 0 1 0 0 2 0
Query regarding impact on staffing 1 0 1 0 0 0 0 0
Query regarding impact on stakeholder relationships 1 1 0 0 0 0 0 0
Feedback Total
Event
Bu
rto
n
Can
no
ck
Le
ek
Lic
hfi
eld
Se
isd
on
Sta
ffo
rd
Sto
ke
Ta
mw
ort
h
Involve patients and communities in decision making 7 1 0 4 0 0 0 2 0
Local representation is important 6 0 0 2 2 0 2 0 0
Consider the need for improved access to services (e.g. appointments) 6 0 3 0 1 0 2 0 0
Consider the need to maintain service provision locally 6 0 1 1 1 2 0 0 1
Six CCGs is an inefficient use of resources / one CCG is more efficient 5 0 1 1 3 0 0 0 0
Greater clarity is required on the proposals 4 0 0 0 0 0 3 1 0
Consider the demographic / geographic differences across the areas 4 0 0 1 2 0 1 0 0
Consider transport issues, parking and non-drivers 4 0 2 0 0 0 2 0 0
Greater partnership working across sectors is required 4 1 0 2 0 0 0 1 0
Consider the need for adequate funding 3 1 0 0 0 0 0 2 0
Option 2 would focus resources in Stoke-on-Trent / urban areas / North of county 3 1 0 0 0 1 0 0 1
Consider the impact on committees and boards 3 0 0 0 0 0 0 3 0
Option 1 ensures a better understanding of local issues more tailored to local needs 2 0 0 2 0 0 0 0 0
Option 2 would improve consistency across the area / six CCGs results in inconsistencies 2 0 1 0 1 0 0 0 0
Option 2 supports the delivery of the NHS Long Term Plan 2 0 0 0 2 0 0 0 0
A standardised IT system is required (e.g. appointment booking, medical records) 2 0 0 0 2 0 0 0 0
Consider the need for equity across different areas 2 1 0 0 1 0 0 0 0
Need to ensure adequate staffing 2 0 0 0 0 0 0 2 0
Stoke-on-Trent should be its own CCG 2 0 0 0 0 1 1 0 0
Consider the impact on wider stakeholders (e.g. Together We're Better) 2 0 0 0 1 0 0 1 0
General comment supporting option 2 2 0 0 0 0 1 0 1 0
Option 2 supports the management of system-wide issues 1 0 0 0 0 0 0 0 1
Consider whether costs can be reduced 1 0 0 1 0 0 0 0 0
Consider that top-down organisation / top-heavy management could negatively affect patients 1 0 0 0 1 0 0 0 0
Stoke-on-Trent may be negatively affected (e.g. loss of funding) 1 1 0 0 0 0 0 0 0
Consider the need for local involvement (e.g. Patient congress, voluntary groups) 1 0 0 0 1 0 0 0 0
Smaller service providers may be disadvantaged if option 2 is implemented 1 0 0 0 0 0 0 1 0
Consider a separate CCG for Stoke-on-Trent and/or Stoke-on-Trent and Northern Staffordshire 1 0 0 0 0 1 0 0 0
Ensure suitable staff are employed 1 0 0 1 0 0 0 0 0
Consider implications on funding 1 0 0 0 0 0 0 1 0
Consider the need for greater public awareness of the proposals 1 0 0 0 0 0 0 1 0
Proposal will lead to benefits in managing system-wide issues 1 0 0 0 0 0 0 0 1
Ensure decisions are made locally 1 0 0 0 1 0 0 0 0
Other 17 3 0 6 4 0 0 4 0
Page 47
47 | NHS Midlands & Lancashire Commissioning Support Unit
Appendix 4: Summary of event demographic profiling
questionnaires The profile of the two event participants submitting their demographic profiling questionnaire is:
• Religion: Both respondents had no religion
• Sex: Both respondents were male
• Gender identity: Both respondents had not undergone any gender reassignment
• Sexual orientation: Both respondents were heterosexual
• Relationship status: One respondent was married; one was single.
No further questions were answered.