BREAST DISEASE: DIAGNOSIS AND CONTEMPORARY MANAGEMENT 0889–8545/02 $15.00 .00 CONTEMPORARY MANAGEMENT OF BREAST CANCER Maureen A. Chung, MD, PhD, FACS, David Wazer, MD, and Blake Cady, MD, FACS There has been a dramatic change in the clinical presentation of breast cancer. In the 1970s and early 1980s, breast cancer usually was detected by clinical examination. With the advent of widespread screening mammography, many women are now diagnosed in the preclinical stage, with lesions detected solely by mammography. As a result, there has been a stage shift in presentation, with an increase in preinvasive ductal carcinoma in situ (DCIS) and small invasive breast cancers (cancers 1.0 cm and less in maximum dimension). 14 Because of the dramatic increase in stage 0 and 1 breast cancer, the radical treatment of these cancers has been reevaluated. 8 These very early forms of breast cancer may be treated with less aggressive therapy and treatment modi- fied based on presentation and accepted prognostic factors. This article discusses some of the current nonconventional methods of treating breast cancer, which take advantage of this earlier presentation. The authors’ approach emphasizes the identification of women who may benefit from less invasive surgery and adjuvant radiotherapy with no sacrifice in survival and little impact on local recurrence. The treatment guidelines currently used at the authors’ center are presented, as well as the data supporting the treatment protocol. MANAGEMENT OF IN SITU BREAST CANCER In situ lesions include lobular carcinoma in situ (LCIS) and DCIS. DCIS is a true precursor lesion for invasive breast cancer. The term LCIS was first coined by Foote and Stewart 30 to describe a nonproliferative lobular lesion of the From The Breast Health Center, Women and Infants Hospital (MAC, BC); Department of Surgery, Brown University School of Medicine (MA, DW, BC); Department of Radia- tion Oncology, Rhode Island Hospital and New England Medical Center (DW), Provi- dence, Rhode Island; and Tufts University School of Medicine, Boston, Massachu- setts (DW) OBSTETRICS AND GYNECOLOGY CLINICS OF NORTH AMERICA VOLUME 29 • NUMBER 1 • MARCH 2002 173
Transcript
BREAST DISEASE: DIAGNOSIS ANDCONTEMPORARY MANAGEMENT 0889–8545/02 $15.00 � .00
CONTEMPORARY MANAGEMENTOF BREAST CANCER
Maureen A. Chung, MD, PhD, FACS, David Wazer, MD,and Blake Cady, MD, FACS
There has been a dramatic change in the clinical presentation of breastcancer. In the 1970s and early 1980s, breast cancer usually was detected byclinical examination. With the advent of widespread screening mammography,many women are now diagnosed in the preclinical stage, with lesions detectedsolely by mammography. As a result, there has been a stage shift in presentation,with an increase in preinvasive ductal carcinoma in situ (DCIS) and smallinvasive breast cancers (cancers 1.0 cm and less in maximum dimension).14
Because of the dramatic increase in stage 0 and 1 breast cancer, the radicaltreatment of these cancers has been reevaluated.8 These very early forms ofbreast cancer may be treated with less aggressive therapy and treatment modi-fied based on presentation and accepted prognostic factors. This article discussessome of the current nonconventional methods of treating breast cancer, whichtake advantage of this earlier presentation. The authors’ approach emphasizesthe identification of women who may benefit from less invasive surgery andadjuvant radiotherapy with no sacrifice in survival and little impact on localrecurrence. The treatment guidelines currently used at the authors’ center arepresented, as well as the data supporting the treatment protocol.
MANAGEMENT OF IN SITU BREAST CANCER
In situ lesions include lobular carcinoma in situ (LCIS) and DCIS. DCIS is atrue precursor lesion for invasive breast cancer. The term LCIS was first coinedby Foote and Stewart30 to describe a nonproliferative lobular lesion of the
From The Breast Health Center, Women and Infants Hospital (MAC, BC); Department ofSurgery, Brown University School of Medicine (MA, DW, BC); Department of Radia-tion Oncology, Rhode Island Hospital and New England Medical Center (DW), Provi-dence, Rhode Island; and Tufts University School of Medicine, Boston, Massachu-setts (DW)
OBSTETRICS AND GYNECOLOGY CLINICS OF NORTH AMERICA
VOLUME 29 • NUMBER 1 • MARCH 2002 173
174 CHUNG et al
breast. LCIS tends to occur in premenopausal women and is not detectedmammographically. This pathologic entity is associated with an increased riskfor the subsequent development of breast cancer, predominantly of ductal histol-ogy.35 The increased risk for breast cancer includes both breasts.22 The currenttreatment for women with LCIS is observation50 or chemoprevention with tamox-ifen,51 or, occasionally, bilateral mastectomy if there are other strong risk factors.
Unlike LCIS, DCIS is a preinvasive breast cancer that, left untreated, mayprogress to an invasive breast cancer. The surgical management of DCIS remainscontroversial. Surgical options for DCIS have included lumpectomy, with orwithout radiation, or total mastectomy. At the recent consensus conference onDCIS, no unanimity could be reached concerning management after completelocal surgical excision, that is, the choice of observation alone, adjuvant wholebreast irradiation, tamoxifen, or a combination of radiotherapy and tamoxifen.58
Currently, the standard of care for the treatment of DCIS is mastectomy orlumpectomy to a tumor-free margin, with adjuvant whole breast irradiation orlumpectomy alone in selected cases. These recommendations have been sup-ported by the results of two prospective randomized trials, comparing lumpec-tomy with or without whole breast irradiation, and the results of one largeprospectively collected patient database. The first trial, the National SurgicalAdjuvant Breast Project (NSABP) B-17 trial, randomized 817 patients with DCISto lumpectomy with or without whole breast irradiation.23 At 8 years’ follow-up, the local recurrence rate for patients treated with surgical excision alone wastwice that observed for patients treated with surgical excision and radiation(27% and 12%, respectively). The second randomized study, the European Orga-nization for Research and Treatment of Cancer (EORTC) trial 10853,41 random-ized 1002 women to lumpectomy with or without radiotherapy and showedthat lumpectomy alone for DCIS also resulted in about twice the local recurrencerate as that seen for surgical excision with radiation (17% versus 11%, respec-tively). In addition to a reduction in local recurrence, radiotherapy reduced therisk of a subsequent invasive cancer. Two thirds of the local recurrences in theNSABP B-17 trial were DCIS; the remainder of the recurrences were invasivecancer. In the EORTC trial 10853, the recurrent cancers were evenly distributedbetween DCIS and invasive cancer. Based on these results, the current recom-mendation to minimize the risk of local recurrence for DCIS is lumpectomy plusadjuvant radiation for patients in whom a negative tumor margin has beenachieved. Silverstein and colleagues60 have published the largest prospectivelycollected database from a single institution for patients with DCIS. Their datasuggest that DCIS is a heterogenous disease. Several categories of patientsmay be treated by lumpectomy alone without radiotherapy because their localrecurrence rate is low, whereas other patients are best treated with a mastectomy.
With increased mammographic screening, a greater proportion of DCIS willbe detected at smaller sizes.27 These lesions may have less potential for progres-sion to invasion and local recurrence. It is clear from a review of autopsy studiesthat not all forms of DCIS are capable of progressing to invasion, because theprevalence of undetected DCIS in patients dying of other causes has beenreported to be as much as 9%, with the prevalence of unsuspected invasivebreast cancer 1.3%.69 These data suggest that a substantial proportion of DCISmay remain clinically innocuous, and overtreatment should be avoided. Becausemammographic screening is recommended beginning at age 40 years, morewomen are diagnosed with DCIS at an early age.20 These women may have alife expectancy of 40 additional years and are at significant risk for the develop-ment of a second cancer, DCIS or invasive. Prior treatment with whole breastirradiation may preclude breast conservation in these women.
CONTEMPORARY MANAGEMENT OF BREAST CANCER 175
The randomized trials have been criticized because all forms of DCIS wereclassified as one cancer, and the definition of a negative margin was too minimal.Some lesions are very small with a low biologic potential for progression toinvasion or recurrence, whereas others have a significant potential for progres-sion to invasive cancer.34 The difficulty rests with the inability to distinguish theforms of DCIS with differing biologic potentials, which would permit tailoringthe treatment to the biologic potential in local recurrence, progression, andinvasion.
Because DCIS is a preinvasive cancer or precursor lesion, the likelihood ofdying from this disease is extremely low. Data from the Surveillance, Epidemiol-ogy, and End Results program (SEER) indicate that, of women diagnosed withDCIS from 1984 to 1989, 0.7% died of breast cancer within 5 years and 1.9%within 10 years.21 The main outcome is not mortality but local recurrence. A lowrate of local recurrence for DCIS is important because one half of local recur-rences occur as invasive disease with metastatic potential if not detected early.Many studies, most of them retrospective, have attempted to identify prognosticfeatures that might predict local recurrence. Lagios and colleagues42 observedthat DCIS with a high nuclear grade and comedonecrosis had an eightfoldincrease in local recurrence compared with the rate for patients without thesehistologic characteristics. A similar observation has been reported by others.5
Other factors associated with an increase in local recurrence include young age,6
palpable lesions (versus those detected solely by mammography),2 larger size,42
multifocal or multicentric lesions,20 and width of the surgical margin. The relativeincrease in local recurrence related to these prognostic factors is summarized inTable 1. The importance of margin width has been emphasized in several studies.Weng and co-workers70 evaluated patients treated with lumpectomy, with orwithout radiotherapy, and reported a twofold increase in the local recurrencerate in patients who had close or positive tumor margins. The local recurrencerate for DCIS with a close or positive surgical margin was increased sevenfold
Table 1. PROGNOSTIC FACTORS FOR LOCAL RECURRENCE OF DUCTALCARCINOMA IN SITU (DCIS) AFTER BREAST CONSERVATION, WITH OR WITHOUTADJUVANT RADIOTHERAPY
RelativePrognostic Factor Risks* Series
Age �50 years 2–4� MSKCC, NSABP-24,28 William Beaumont68
Palpable tumor 1.6–3.0� NSBAP-24, William BeaumontTumor size �1.0 cm 1.6–3.0� Meta-analysis
MSKCC, NSBP-17, NSABP-24, William Beaumont,Comedonecrosis 1.4–4.4� meta-analysis7†
MSKCC, NSBP-17, South Manchester,11 WilliamHigh nuclear grade 1.3–2.8� Beaumont, meta-analysisPositive or close MSKCC, NSBP-17, South Manchester, NSABP-24,
surgical margins 1.3–7.5� William BeaumontMultifocal tumor 1.5� NSA-17
*Relative risk is expressed as relative increase for prognostic factor as compared within a groupwith prognostic factor absent.
MSKCC � Memorial Sloan Kettering Cancer Center, New York; NSABP-17 � National SurgicalAdjuvant Breast Project 17—randomized trial of lumpectomy with or without radiotherapy for DCIS;NSABP-24 � National Surgical Adjuvant Breast Project 24—randomized trial of lumpectomy andradiotherapy with or without adjuvant tamoxifen for DCIS.
†Meta-analysis evaluating factors associated with local recurrence.
176 CHUNG et al
when compared with a greater surgical margin in another study from England.11a
The increase in local recurrence occurred despite adjuvant therapy with radiationand tamoxifen. Many studies included patients treated with and without radio-therapy after surgical excision. In the most recent NSA BP study B-24,28 allpatients were treated with radiotherapy, and one half received adjuvant tamoxi-fen, further reducing the risk of local recurrence.
Following a multifactorial analysis of the surgical, pathologic, and patientfeatures and their biologic potential, Silverstein and colleagues60 developed theVan Nuys Pathologic Classification System to define the likelihood of localrecurrence of DCIS after breast conservation. This analysis included three sig-nificant prognostic features: tumor size, tumor grade (with or without necrosis),and width of the surgical margin. The age of the patient has been added in arecent modification of the Van Nuys Pathologic Classification. In the initialclassification, the tumor grade and comedonecrosis were used to reflect thebiology of the tumor, whereas the size and surgical margin reflected the extentof disease and the surgeon’s ability to excise the tumor adequately. Each majorfeature was rated on a 3-point scale. Using these three parameters, every DCIScould be scored with the Van Nuys Prognostic Index (VNPI) and classified intolow (score 3 or 4), intermediate (score 5, 6, or 7), or high (score 8 or 9) likelihoodof local recurrence (Table 2). Silverstein and colleagues then determined theeffect of adjuvant radiotherapy on the recurrence rate. Patients with a lowlikelihood of recurrence (VNPI of 3 or 4) had a rate of 2% to 3% at 8 years—arate that could not be improved with adjuvant whole breast irradiation. Patientswith a high likelihood of local recurrence (VNPI of 8 or 9) had a local recurrencerate of 60% after breast conservation, even if adjuvant breast radiotherapy wasused. For these patients, a mastectomy is clearly indicated. For patients at anintermediate risk for local recurrence (VNPI of 5, 6, or 7), the addition ofadjuvant whole breast irradiation slightly decreased the local recurrence rate.Because the VNPI score included width of the surgical margin, VNPI scorescould be reduced by a reexcision of the biopsy cavity to achieve a greatersurgical margin.
Silverstein and co-workers updated their initial data in 199961 and againin 2000.62 With 547 patients prospectively enrolled in this database on breastconservation after the excision of DCIS, the measured margin emerged as themost important prognostic feature predicting local recurrence. A margin width10 mm or greater resulted in a low recurrence rate (3% or 4%), equivalent to theVNPI low-risk group, and was not further reduced by the addition of wholebreast radiotherapy. The overall local recurrence risk ratio (RR) for DCIS excisedwith a 10-mm, tumor-free margin was 1.14 [95% confidence interval (CI), 0.10–12.64], which is not statistically different from the RR for surgical excision withadjuvant whole breast irradiation. Stratification according to necrosis, nucleargrade, and size resulted in RRs of 1.22 (95% CI, 0.11–13.93), 1.08 (95% CI,0.09–12.70), and 1.69 (95% CI, 0.15–12.70), respectively. These relative RRs werenot statistically significantly different for excision alone or excision plus adjuvantradiotherapy.
Patients with a VNPI of 8 or 9 represent a unique category of patients athigh risk. These patients are equivalent to the premammographic era of palpablecomedo-type DCIS and similar to the high-risk subgroup of patients describedby Tabar and colleagues.63 These patients usually have histologically high-gradelesions and extensive casting-type microcalcifications on mammography occu-pying more than one quadrant of the breast. These extensive DCIS lesionsfrequently have multiple microinvasive or T1a invasive foci.72 Because it isdifficult to diagnose microinvasion preoperatively on core biopsies, it has been
CONTEMPORARY MANAGEMENT OF BREAST CANCER 177
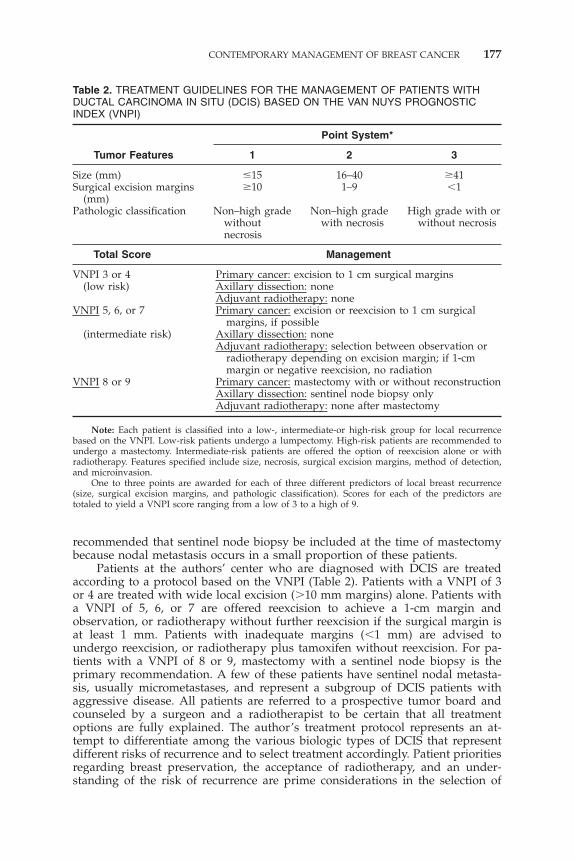
Table 2. TREATMENT GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITHDUCTAL CARCINOMA IN SITU (DCIS) BASED ON THE VAN NUYS PROGNOSTICINDEX (VNPI)
(mm)Pathologic classification Non–high grade Non–high grade High grade with or
without with necrosis without necrosisnecrosis
Total Score Management
VNPI 3 or 4 Primary cancer: excision to 1 cm surgical margins(low risk) Axillary dissection: none
Adjuvant radiotherapy: noneVNPI 5, 6, or 7 Primary cancer: excision or reexcision to 1 cm surgical
margins, if possible(intermediate risk) Axillary dissection: none
Adjuvant radiotherapy: selection between observation orradiotherapy depending on excision margin; if 1-cmmargin or negative reexcision, no radiation
VNPI 8 or 9 Primary cancer: mastectomy with or without reconstructionAxillary dissection: sentinel node biopsy onlyAdjuvant radiotherapy: none after mastectomy
Note: Each patient is classified into a low-, intermediate-or high-risk group for local recurrencebased on the VNPI. Low-risk patients undergo a lumpectomy. High-risk patients are recommended toundergo a mastectomy. Intermediate-risk patients are offered the option of reexcision alone or withradiotherapy. Features specified include size, necrosis, surgical excision margins, method of detection,and microinvasion.
One to three points are awarded for each of three different predictors of local breast recurrence(size, surgical excision margins, and pathologic classification). Scores for each of the predictors aretotaled to yield a VNPI score ranging from a low of 3 to a high of 9.
recommended that sentinel node biopsy be included at the time of mastectomybecause nodal metastasis occurs in a small proportion of these patients.
Patients at the authors’ center who are diagnosed with DCIS are treatedaccording to a protocol based on the VNPI (Table 2). Patients with a VNPI of 3or 4 are treated with wide local excision (�10 mm margins) alone. Patients witha VNPI of 5, 6, or 7 are offered reexcision to achieve a 1-cm margin andobservation, or radiotherapy without further reexcision if the surgical margin isat least 1 mm. Patients with inadequate margins (�1 mm) are advised toundergo reexcision, or radiotherapy plus tamoxifen without reexcision. For pa-tients with a VNPI of 8 or 9, mastectomy with a sentinel node biopsy is theprimary recommendation. A few of these patients have sentinel nodal metasta-sis, usually micrometastases, and represent a subgroup of DCIS patients withaggressive disease. All patients are referred to a prospective tumor board andcounseled by a surgeon and a radiotherapist to be certain that all treatmentoptions are fully explained. The author’s treatment protocol represents an at-tempt to differentiate among the various biologic types of DCIS that representdifferent risks of recurrence and to select treatment accordingly. Patient prioritiesregarding breast preservation, the acceptance of radiotherapy, and an under-standing of the risk of recurrence are prime considerations in the selection of
178 CHUNG et al
therapy. As stated previously, the treatment of DCIS remains controversial. Thearticle by Schwartz and Terribile elsewhere in this issue diseases this problemin more detail.
INVASIVE BREAST CANCER
As a result of mammographic screening, the mean and median tumor sizeof invasive breast cancer have greatly decreased. Based on data from the RhodeIsland Department of Health, approximately two thirds of women who wereappropriate candidates had screening mammography in 1995 and 1996.14 Themedian maximum tumor diameter of all invasive breast cancers during thesetwo decades decreased from 2.0 to 1.5 cm. With this decrease in median tumorsize, there has been a corresponding shift in stage presentation, with approxi-mately 11% and 44% of women diagnosed with stage 0 and 1 breast cancer,respectively.
A corresponding dramatic increase has occurred in the proportion of womenwith invasive breast cancers 1.0 cm or smaller in maximum diameter (T1a andT1b). If no nodal metastases are present, long-term survival of greater than 95%(T1a) or 90% (T1b) can be expected with local and regional treatment only.Because these women present with the earliest form of invasive disease, someauthorities question whether they should be treated with the standard radicaltherapy, that is, modified radical mastectomy, or breast conservation therapy(lumpectomy, whole breast irradiation, and axillary node dissection). Less ag-gressive locoregional therapy for these small breast cancers can be separatedinto two treatment categories. One category considers the risk of local recur-rences and the other the risk of lymph node metastasis. The first treatmentcategory includes wide local excision with an adequate surgical margin (�1 cm).In the second category, patients at low risk of nodal metastasis could be sparedan axillary dissection by performing sentinel node biopsy, or even evaluation bya sentinel node biopsy if the likelihood of node metastasis is less than 5%.
Local Treatment of Invasive Breast Cancer
Most women with a localized breast cancer can be treated with breastconservation surgery. Even women with locally advanced breast cancers may becandidates for breast conservation after successful neoadjuvant chemotherapy.Several randomized trials have shown that, although there is an increased localrecurrence rate for women treated with breast conservation with or withoutadjuvant radiotherapy, there is no difference in overall survival when mastec-tomy is compared with breast-conserving surgery.10, 25 A recent meta-analysis ofadjuvant whole breast radiotherapy after breast conservation concluded thatthe addition of radiotherapy after breast conservation surgery decreased localrecurrence by two-thirds, with no difference in overall survival.19 Because thereis no difference in overall survival, the question remains whether there is adifference in the mastectomy rate for women initially treated with breast conser-vation who have a later recurrence. In a recent study,36 no long-term differencewas noted in the mastectomy rate in women treated initially with or withoutradiotherapy who later had a recurrence. Approximately two thirds of womeninitially treated with lumpectomy alone who have a recurrence could be treatedwith reexcision and adjuvant radiotherapy. Only one third who had a recurrence
CONTEMPORARY MANAGEMENT OF BREAST CANCER 179
after lumpectomy and radiotherapy could be treated with local excision alone;two thirds required a mastectomy.
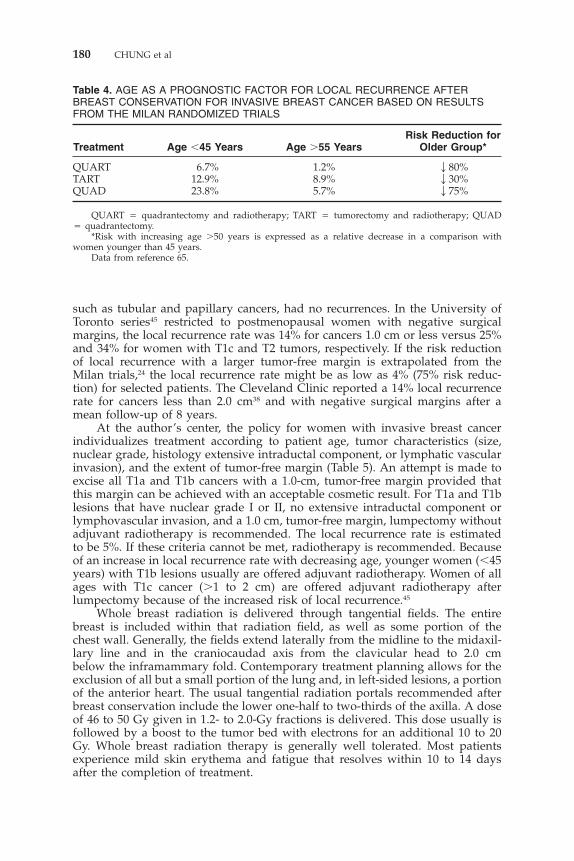
The local recurrence rates in women with breast cancer treated with lumpec-tomy alone in the randomized trials are summarized in Table 3. These trialsincluded predominantly postmenopausal women with a tumor size of 2.0 cm orless. Close examination of these trial results has demonstrated several prognosticfactors associated with decreased local recurrence. Women older than 50 years,or postmenopausal women, had one-half the local recurrence rate when com-pared with younger or premenopausal women.16, 43 The extent of the surgicalmargin is another major factor predicting local recurrence after breast conserva-tion. This observation is best illustrated in the Milan trials, which comparedquadrantectomy with tumorectomy, both with axillary dissection and radiother-apy.24 With a median follow-up of 79 months, women with cancers less than 2.5cm in diameter had a local recurrence rate of 12.8% after tumorectomy andradiotherapy versus 3.3% after quadrantectomy (gross tumor margin �2.0 cm)and radiotherapy.65 The decreased risk of local recurrence with increasing agewas additive to that achieved with radiotherapy (Table 4). Women with a well-differentiated cancer or tumor with nuclear grade I also had a decreased localrecurrence rate. Adverse prognostic factors for local recurrence included thepresence of lymphovascular invasion16 or an extensive intraductal component ofthe primary cancer.66
Using these prognostic factors, a subgroup of women with a low risk forlocal recurrence after lumpectomy without radiation may be identified. Schnittand co-workers57 reported that their local recurrence rate after lumpectomy onlyfor clinical T1 lesions with a 1.0-cm surgical margin was 16%, a rate significantlylower than that reported for lumpectomy alone in the randomized trials but stillconsidered high. Three recurrences were outside the quadrant of the primarytumor and detected more than 30 months after the initial diagnosis, suggestingthat these were new primary cancers. If these three cases were excluded, thelocal recurrence rate was 13%. In addition, grade I cancers and special types,
Table 3. COMPARISON OF LOCAL RECURRENCE IN PATIENTS TREATED WITHBREAST CONSERVATION RANDOMIZED TO ADJUVANT RADIOTHERAPY OROBSERVATION
Tumor Size Local Recurrence Follow-UpSeries (cm) Treatment Rate (%) (Months)
Milan III67 �2.5 QUART 0.3 39QUAD 8.8
Uppsala-Orebro43 �2.0 LAND � RT 2.3 103LAND 18.4
Toronto (PMH)16 �4.0 LAND � RT 11.0 43LAND 35.0
NSABP B-0629 �4.0 LAND � RT 12.0LAND 43.0
Scottish Cancer Trials �4.0 LAND � RT 5.8 68Breast Group LAND 24.5
Finnish Trial36 �2.0 LAND � RT 8.0LAND 29.0
Note: In general, a 75% decrease in local recurrence was observed in patients treated with adjuvantwhole breast irradiation after breast conservation surgery.
QUART � quadrantectomy and radiotherapy; QUAD � quadrantectomy; LAND � RT � lumpec-tomy, axillary node dissection, and radiotherapy; LAND � lumpectomy and axillary node dissection.
180 CHUNG et al
Table 4. AGE AS A PROGNOSTIC FACTOR FOR LOCAL RECURRENCE AFTERBREAST CONSERVATION FOR INVASIVE BREAST CANCER BASED ON RESULTSFROM THE MILAN RANDOMIZED TRIALS
Risk Reduction forTreatment Age �45 Years Age �55 Years Older Group*
QUART � quadrantectomy and radiotherapy; TART � tumorectomy and radiotherapy; QUAD� quadrantectomy.
*Risk with increasing age �50 years is expressed as a relative decrease in a comparison withwomen younger than 45 years.
Data from reference 65.
such as tubular and papillary cancers, had no recurrences. In the University ofToronto series45 restricted to postmenopausal women with negative surgicalmargins, the local recurrence rate was 14% for cancers 1.0 cm or less versus 25%and 34% for women with T1c and T2 tumors, respectively. If the risk reductionof local recurrence with a larger tumor-free margin is extrapolated from theMilan trials,24 the local recurrence rate might be as low as 4% (75% risk reduc-tion) for selected patients. The Cleveland Clinic reported a 14% local recurrencerate for cancers less than 2.0 cm38 and with negative surgical margins after amean follow-up of 8 years.
At the author’s center, the policy for women with invasive breast cancerindividualizes treatment according to patient age, tumor characteristics (size,nuclear grade, histology extensive intraductal component, or lymphatic vascularinvasion), and the extent of tumor-free margin (Table 5). An attempt is made toexcise all T1a and T1b cancers with a 1.0-cm, tumor-free margin provided thatthis margin can be achieved with an acceptable cosmetic result. For T1a and T1blesions that have nuclear grade I or II, no extensive intraductal component orlymphovascular invasion, and a 1.0 cm, tumor-free margin, lumpectomy withoutadjuvant radiotherapy is recommended. The local recurrence rate is estimatedto be 5%. If these criteria cannot be met, radiotherapy is recommended. Becauseof an increase in local recurrence rate with decreasing age, younger women (�45years) with T1b lesions usually are offered adjuvant radiotherapy. Women of allages with T1c cancer (�1 to 2 cm) are offered adjuvant radiotherapy afterlumpectomy because of the increased risk of local recurrence.45
Whole breast radiation is delivered through tangential fields. The entirebreast is included within that radiation field, as well as some portion of thechest wall. Generally, the fields extend laterally from the midline to the midaxil-lary line and in the craniocaudad axis from the clavicular head to 2.0 cmbelow the inframammary fold. Contemporary treatment planning allows for theexclusion of all but a small portion of the lung and, in left-sided lesions, a portionof the anterior heart. The usual tangential radiation portals recommended afterbreast conservation include the lower one-half to two-thirds of the axilla. A doseof 46 to 50 Gy given in 1.2- to 2.0-Gy fractions is delivered. This dose usually isfollowed by a boost to the tumor bed with electrons for an additional 10 to 20Gy. Whole breast radiation therapy is generally well tolerated. Most patientsexperience mild skin erythema and fatigue that resolves within 10 to 14 daysafter the completion of treatment.
CONTEMPORARY MANAGEMENT OF BREAST CANCER 181
Table 5. TREATMENT GUIDELINES FOR WOMEN WITH INVASIVE DUCTALCARCINOMA (IDC) TREATED AT THE BREAST HEALTH CENTER, PROVIDENCE,RHODE ISLAND
Typeof
Lesion Management
T1a Primary cancer: excision to 1 cm marginAxillary lymph node analysis: avoid SNBx unless LVI�, poor nuclear gradeAdjuvant radiotherapy: avoid if possible, but selective application if �1 cm
T1b Primary cancer: excision to 1 cm marginAxillary lymph node analysis: SNBx, axillary dissection if SN�
macrometastasisAdjuvant radiotherapy: yes, all patients �45 years generally; no, patients �45
years generally, but consider grade, size, and marginAdjuvant chemotherapy of hormone therapy: selective based on SN and
primary tumor prognostic featuresNB For any patient with poor nuclear grade LVI or other poor prognostic features:
systemic therapy suggested; axillary dissection if SN� usually, but notalways (i.e., micrometastasis)
T1c Primary cancer: excision or reexcision to negative (if EIC�) or only focallypositive margin (EIC�), or mastectomy with axillary dissection with orwithout reconstruction
Axillary lymph node: SNBx, axillary dissection if SN�Adjuvant radiotherapy: yes, if breast conservationAdjuvant chemotherapy: yes, generally
T2 Primary cancer: excision to negative or focally positive margin, or mastectomyAxillary lymph node: if mastectomy, axillary dissection; if breast conservation,
SNBx; if SN�, axillary dissectionAdjuvant radiotherapy: yes, if breast conservation; consider postmastectomy for
poor prognosisAdjuvant chemotherapy or hormones: yes, generally; emphasize induction
chemotherapy for all cancers �3 cm; if complete or partial chemotherapyresponse, excision and radiotherapy, if possible; if minor or no response,consider mastectomy and axillary dissection, may elect breast conservationwith radiation
EIC � extensive intraductal component; ER � estrogen receptor; PR � progesterone receptor; LVI� lymphovascular invasion; SNBx � sentinel node biopsy; DNA & S phase � cancer cell chromosomeanalysis; Her 2 Neu � oncogene analysis.
Note: Features specified include age, method of detection, size, grade, surgical margin, histologictype, sentinel node or axilllary lymph node status, EIC status, and other prognostic indices (ER, PR,LVI, DNA & S phase, Her 2 Neu). The strategy is based on age, method of detection, size, grade, EIC,lymph node metastasis, and prognostic features of the primary cancer.
Axillary Evaluation in Invasive Breast Cancer
The presence of regional nodal metastasis remains one of the most importantprognostic indicator of overall survival in women with early breast cancer;however, it is difficult clinically to predict axillary nodal status accurately. Owingto the limitations of clinical axillary evaluation, an axillary nodal dissection hasremained as an integral component of the surgical treatment of women withbreast cancer. Several large randomized trials10, 25 have demonstrated that axillarydissection has no impact on survival in women with breast cancer and a clini-
182 CHUNG et al
cally negative axilla, implying that the presence of lymph node metastasis inbreast cancer is an indicator but not a governor of survival.9 Although thesubstantial morbidity of axillary dissection can largely be eliminated with senti-nel node biopsy, this procedure is not without some morbidity.47 The questionremains whether it is possible to identify women with such an extremely lowincidence of nodal metastasis that axillary evaluation either by an axillary nodedissection or sentinel node biopsy could be obviated.
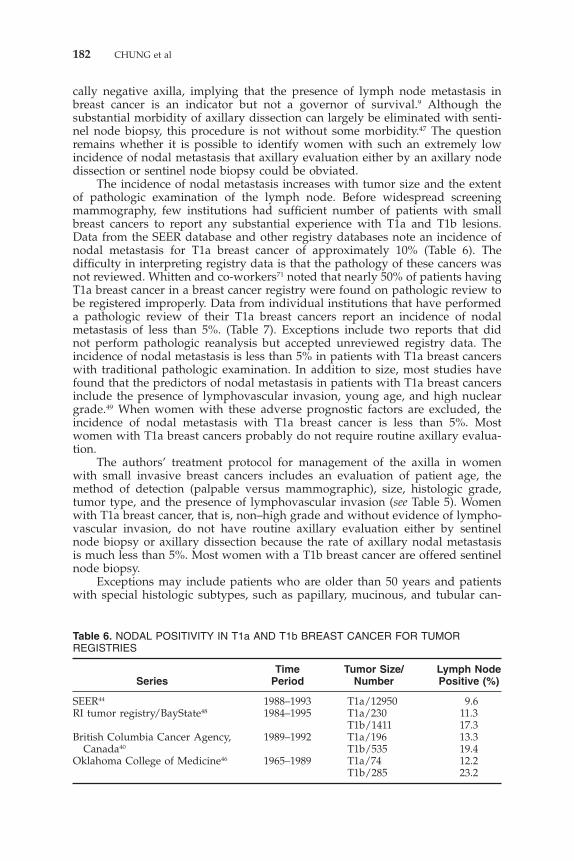
The incidence of nodal metastasis increases with tumor size and the extentof pathologic examination of the lymph node. Before widespread screeningmammography, few institutions had sufficient number of patients with smallbreast cancers to report any substantial experience with T1a and T1b lesions.Data from the SEER database and other registry databases note an incidence ofnodal metastasis for T1a breast cancer of approximately 10% (Table 6). Thedifficulty in interpreting registry data is that the pathology of these cancers wasnot reviewed. Whitten and co-workers71 noted that nearly 50% of patients havingT1a breast cancer in a breast cancer registry were found on pathologic review tobe registered improperly. Data from individual institutions that have performeda pathologic review of their T1a breast cancers report an incidence of nodalmetastasis of less than 5%. (Table 7). Exceptions include two reports that didnot perform pathologic reanalysis but accepted unreviewed registry data. Theincidence of nodal metastasis is less than 5% in patients with T1a breast cancerswith traditional pathologic examination. In addition to size, most studies havefound that the predictors of nodal metastasis in patients with T1a breast cancersinclude the presence of lymphovascular invasion, young age, and high nucleargrade.49 When women with these adverse prognostic factors are excluded, theincidence of nodal metastasis with T1a breast cancer is less than 5%. Mostwomen with T1a breast cancers probably do not require routine axillary evalua-tion.
The authors’ treatment protocol for management of the axilla in womenwith small invasive breast cancers includes an evaluation of patient age, themethod of detection (palpable versus mammographic), size, histologic grade,tumor type, and the presence of lymphovascular invasion (see Table 5). Womenwith T1a breast cancer, that is, non–high grade and without evidence of lympho-vascular invasion, do not have routine axillary evaluation either by sentinelnode biopsy or axillary dissection because the rate of axillary nodal metastasisis much less than 5%. Most women with a T1b breast cancer are offered sentinelnode biopsy.
Exceptions may include patients who are older than 50 years and patientswith special histologic subtypes, such as papillary, mucinous, and tubular can-
Table 6. NODAL POSITIVITY IN T1a AND T1b BREAST CANCER FOR TUMORREGISTRIES
Time Tumor Size/ Lymph NodeSeries Period Number Positive (%)
St. Joseph Hospital, 1987–1994 T1a/74 4.5 High nuclear gradeColorado12
John Wayne Cancer 1988–1994 T1a/20 10.0Institute33 T1b/68 13.0
Mount Sinai Medical Center, 1993–1998 T1a/105 8.0 Age �40 years and LVINY32 T1b/275 15.0
Virginia Mason Hospital, 1977–1987 T1a/34 3.0WA52 T1b/144 10.0
Centro per lo Studio e la 1970–1992 T1a/31 0Prevenziona Oncologica of T1b/123 6.9Florence15
LVI � lymphovascular invasion.
cers. In patients with T1c and larger cancers with a clinically negative axilla, asentinel node biopsy is recommended. The incidence of nodal metastasis is 30%in this group of women. If the sentinel lymph node is negative for metastaticdisease, no further axillary surgery is necessary, and separate nodal radiationfields are not recommended beyond the tangential portals included for wholebreast radiotherapy.
Most patients with a positive sentinel lymph node undergo a level I/IIlymph node dissection or are randomized to the American College of SurgeonsZ0011 trial, which compares axillary node dissection with observation only.Patients with T1a and T1b cancers with a single axillary lymph node micrometas-tasis do not generally need axillary dissection nor separate nodal radiationbecause the presence of other axillary metastasis in this setting is exceedingly
184 CHUNG et al
low.13 In patients with T1c and T2 cancers and a positive sentinel node biopsy,including micrometastases, an axillary node dissection is recommended.
Sentinel node biopsy has been performed since 1998 at the authors’ center.There has been a progression in the injection site from intraparenchymal tointradermal for the radioactive colloid and from intraparenchymal to periareolainjection for the blue dye. Currently, an intradermal, unfiltered, technetiumsulfur colloid injection over the primary cancer site combined with subareolarblue dye injections are the preferred sites to identify the sentinel lymph node.Overall, a sentinel lymph node was identified in 95.5% of the 315 patients in theauthors’ series. This rate has increased to 99% in the last 150 patients using thecurrent technique. Patients with a negative sentinel lymph node do not undergoaxillary dissection or separate nodal radiation. Because axillary dissection hasnot been routinely performed in all patients with a negative sentinel lymphnode, the specificity of the sentinel node biopsy in the author’s series is notcompletely known—however, a careful follow-up of patients demonstrates afalse-negative rate of 1%. With a median follow-up of 24 months, an axillaryrecurrence has developed in 2 of 199 patients who had a negative sentinel nodebiopsy. One patient had four negative sentinel lymph nodes but a recurrence inthe axilla after 4 months. The second patient with a T1c lesion had four negativesentinel lymph nodes; she had a recurrence 11 months later with regional andsystemic metastasis. These two patients represent true false-negative sentinellymph node findings. There have been two other axillary recurrences. Onepatient had a cancer with a poor prognosis in which the sentinel lymph nodewas not identified, refused axillary dissection but accepted axillary radiation,and had a recurrence at 19 months. The second patient had a T1c lesion with apositive sentinel lymph node, refused an axillary dissection or radiation, andhad a recurrence at 6 months.
NEOADJUVANT THERAPY FOR BREAST CANCER
Although mammographic screening has resulted in an increased detectionof DCIS and small invasive breast cancers, some women still present with locallyadvanced breast cancers. This category includes women with a large primarytumor, a clinically positive axillary lymph node, or inflammatory breast cancer.Usually, these patients are young women who have not yet begun screening, orolder women who have not participated in screening or who have missedroutine yearly screening. Neoadjuvant or preoperative chemotherapy in thesepatients has a response rate of 70% to 90%; approximately 20% of these womenhave a complete clinical response.56 Although neoadjuvant chemotherapy hasnot been shown to improve survival, patients who respond to chemotherapyhave an improved disease-free survival exceeding 80% at 5 years26 for patientswith a complete pathologic response. There is also an increased rate of breastconservation in patients who undergo neoadjuvant chemotherapy. Before ther-apy, all patients have a core needle biopsy of the primary lesion for histologicdiagnosis, determination of the histologic grade, and measurement of hormonalreceptor status. An axillary ultrasound is performed in women with a clinicallynegative axilla, and suspicious lymph nodes are evaluated by fine-needle aspira-tion cytology to permit accurate staging.
At the authors’ center, locally advanced cancers are defined as tumors largerthan 3.0 cm, documented by clinical or radiographic measurements, or tumorsin patients with clinically or sonographically positive lymph nodes confirmedby fine-needle aspiration cytology.
CONTEMPORARY MANAGEMENT OF BREAST CANCER 185
These women receive neoadjuvant therapy, usually, anthracycline-based,followed by definitive surgery. Patients also receive postmastectomy radiation.Depending on the response to neoadjuvant therapy and the axillary nodal status,selected patients receive adjuvant taxane chemotherapy following surgery. Non-responders or patients with extensive residual disease after chemotherapy havea poor prognosis and are considered for clinical trials.
SUMMARY
Breast cancer is a heterogenous disease with significant variations in biologicpotential, ranging from small, low-grade, DCIS discovered mammographicallywith essentially no impact on patient survival to rapidly growing, palpable,locally advanced invasive breast cancer with clinically palpable nodal metastasis.The current challenge is to identify the clinical, pathologic, and molecular factorsthat determine the biologic potential of a particular breast cancer. Although size,nodal status, histologic grade, age, surgical margin, and hormone receptor statusof breast cancer are the most important prognostic factors, the focus of researchmust be beyond these factors to other nonspecific prognostic information. Bonemarrow micrometastasis may be an important factor to help predict outcome,7a
and the complement of sentinel node biopsy, bone marrow analysis, and primarytumor features may allow physicians to better select therapy. With increasedunderstanding of the individual molecular events that control the invasivepotential of a particular cancer, practitioners should be better able to predictmore accurately which patients have little risk of recurrent disease or metastasisand would be best served by surgery alone versus patients who have a high riskof recurrent and metastatic disease and who should receive multimodality care.
References
1. Abner AL, Collins L, Peiro G, et al: Correlation of tumor size and axillary lymphnode involvement with prognosis in patients with T1 breast carcinoma. Cancer 83:2502–2608, 1998
2. Amichette M, Caffo O, Richetti A, et al: Subclinical ductal carcinoma in situ of thebreast: Treatment with conservative surgery and radiotherapy. Tumori 85:488–493,1999
3. Anan K, Mitsuyama S, Tamae K, et al: Axillary lymph node metastasis in patientswith small carcinomas of the breast: Is accurate prediction possible? Eur J Surg 166:610–615, 2000
4. Barth A, Craig PH, Silverstein MJ: Predictors of axillary lymph node metastasis inpatients with T1 breast carcinoma. Cancer 79:1918–1922, 1997
5. Bellamy COC, McDonald C, Salter DM, et al: Non-invasive ductal carcinoma of thebreast: The relevance of histologic categorization. Hum Pathol 24:16–23, 1993
6. Bijker N, Peterse JL, Duchateau L, et al: Risk factors for recurrence and metastasisafter breast-conserving therapy for ductal carcinoma-in-situ: Analysis of EuropeanOrganization for Research and Treatment of Breast Cancer Trial 10853. J Clin Oncol19:2263–2271, 2001
7. Boyages J, Delaney G, Taylor R: Predictors of local recurrence after treatment ofductal carcinoma in situ: A meta-analysis. Cancer 85:616–628, 1999
7a. Braun S, Cevatli BS, Assemi C, et al: Comparative analysis of micrometastasis to thebone marrow and lymph nodes of node-negative breast cancer patients receiving noadjuvant therapy. J Clin Oncol 19:1468–1475, 2001
8. Cady B, Stone MD, Wayne J: New therapeutic possibilities in primary invasive breastcancer. Ann Surg 218:338–349, 1993
186 CHUNG et al
9. Cady B: Basic principles in surgical oncology. Arch Surg 132:338–346, 199710. Cancer Research Campaign Working Party: CRC (Kings/Cambridge) trial for early
breast cancer. Detailed uptake of the tenth year. Lancet 11:55–60, 198011. Chan KC, Knox WF, Sinha G, et al: Extent of excision margin width required in breast
conserving surgery for ductal carcinoma in situ. Cancer 91:9–16, 200111a. Chon KC, Knox WF, Sinha G, et al: Extent of excision width required in breast
conserving surgery for ductal carcinoma in situ. Cancer 91:9–16, 200112. Chontos AJ, Maher DP, Ratzer ER, et al: Axillary lymph node dissection: Is it required
in T1a breast cancer? J Am Coll Surg 184:493–498, 199713. Chu KU, Turner RR, Hansen NM, et al: Do all patients with sentinel node metastasis
from breast carcinoma need complete axillary dissection? Ann Surg 229:536–541, 199914. Chung M, Fulton J, Cady B: Trends in breast cancer incidence and presentation in a
population screened for breast cancer. Seminars in Breast Disease 2:55–63, 199915. Ciatto S, Del Turco R, Bonardi R, et al: Non-palpable lesions of the breast detected
by mammography—review of the 1182 consecutive histologically confirmed cases.Eur J Cancer 30A:40–44, 1994
16. Clark RM, McCulloch PB, Levine MN, et al: Randomized clinical trial to assess theeffectiveness of breast irradiation following lumpectomy and axillary dissection fornode negative cancer. J Natl Cancer Inst 84:683–689, 1992
17. Coombs JH, Hubbard E, Hudson K, et al: Ductal carcinoma in situ of the breast:Correlation of pathologic and mammographic features with extent of disease. AmSurg 63:1079–1083, 1997
18. Dowlastshahi K, Snider HC, Kim R: Axillary node status in nonpalpable breast cancer.Ann Surg Oncol 2:424–428, 1995
19. Early breast cancer trialists collaborative group: Favorable and unfavorable effects onlong term survival of radiotherapy for early breast cancer: An overview of therandomised trials. Lancet 355:1757–1770, 2000
20. Ernster VL, Barclay J, Kerlikowske K, et al: Incidence and treatment for ductalcarcinoma in situ of the breast. JAMA 275:913–918, 1996
21. Ernster VL, Barclay J, Kerlikowske K, et al: Mortality among women with ductalcarcinoma in situ of the breast in the population-based surveillance, epidemiologyand end results program. Arch Intern Med 160:953–958, 2000
22. Fisher ER, Constantino J, Fisher B, et al: Pathologic findings from the NationalSurgical Adjuvant Breast Project (NSABP) Protocol 17: Five-year observations con-cerning lobular carcinoma in situ. Cancer 78:1403–1416, 1996
23. Fisher B, Costantino J, Redmond C, et al: Lumpectomy compared with lumpectomyand radiation therapy for the treatment of intraductal breast cancer. N Engl J Med328:1581–1596, 1993
24. Fisher B, Anderson S, Fisher ER, et al: Significance of ipsilateral breast recurranceafter lumpectomy. Lancet 338:327–331, 1991
25. Fisher B, Redmond C, Fisher ER, et al: Ten-year results of a randomized clinical trialcomparing radical mastectomy and total mastectomy with or without radiation. NEngl J Med 312:674–681, 1985
26. Fisher B, Brown A, Mamounas E, et al: Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: Findings from NationalSurgical Adjuvant Breast and Bowel Project B-18. J Clin Oncol 15:2483–2493, 1997
27. Fisher ER, Dignam J, Tan-Chiu E, et al: Pathologic findings from the National SurgicalAdjuvant Breast Project (NSABP) eight-year update of protocol B-17: Intraductalcarcinoma. Cancer 86:429–438, 1999
28. Fisher B, Dignam J, Wolmark N, et al: Tamoxifen in treatment of intraductal breastcancer. National Surgical Adjuvant Breast and Bowel Project B-24 randomized con-trolled trial. Lancet 353:1993–2000, 1999
29. Fisher B, Anderson S, Fisher ER, et al: Significance of ipsilateral breast recurrenceafter lumpectomy. Lancet 338:327–331, 1991
30. Foote FW, Stewart FW: Lobular carcinoma in situ: A rare form of mammary cancer.Am J Pathol 17:491–495, 1941
31. Forrest AP, Stewart HJ, Everington D, et al: Randomised controlled trial of conserva-
CONTEMPORARY MANAGEMENT OF BREAST CANCER 187
tion therapy for breast cancer: 6 Year analysis of the Scottish trial. Lancet 348:708–713, 1996
32. Gajdos C, Tartter PI, Bleiweiss IJ: Lymphatic invasion, tumor size, and age areindependent predictors of axillary lymph node metastases in women with T1 breastcancers. Ann Surg 230:692–696, 1999
33. Giuliano AE, Barth AM, Spivack B, et al: Incidence and predictors of axillary metasta-sis in T1 carcinoma of the breast. J Am Coll Surg 183:185–189, 1996
34. Gupta SK, Douglas-Jones AG, Fenn N, et al: The clinical behavior of breast carcinomais probably determined at the preinvasive stage (ductal carcinoma in situ). Cancer80:1740–1745, 1997
35. Haagensen CD, Lane N, Lattes R, et al: Lobular neoplasia (so-called lobular carcinomain situ) of the breast. Cancer 42:737–769, 1978
36. Hakama M, Saaristo R, Isola J, et al: Lumpectomy with or without postoperativeradiotherapy for breast cancer with favourable prognostic features: Results of arandomized study. Br J Cancer 84:164–169, 2001
37. Halverson KJ, Perez CA, Myerson R, et al: Management of the axilla in patients withbreast cancers 1 centimeter or smaller. Am J Clin Oncol (CCT) 17:461–466, 1994
38. Hermann RE, Esselstyn CB, Grundfest-Broniatowski S, et al: Partial mastectomywithout radiation is adequate treatment for patients with stages 0 and 1 carcinomaof the breast Surg Gynecol Obstet 177:247–253, 1993
40. Jackson JSH, Olivotto IA, Wai E, et al: A decision analysis of the effect of avoidingaxillary lymph node dissection in low risk women with invasive breast carcinoma.Cancer 88:1852–1862, 2000
41. Julien JP, Bijker N, Fentiman IS, et al: Radiotherapy in breast-conserving treatmentfor ductal carcinoma in situ: First results of the EORTC randomized phase III trial10853. Lancet 355:528–533, 2000
42. Lagios MD, Margolin FR, Westdahl PR, et al: Mammographically detected ductcarcinoma in situ: Frequency of local recurrence following tylectomy and prognosticeffect of nuclear grade on local recurrence. Cancer 63:618–624, 1989
43. Liljegren G, Holmberg L, Bergh J, et al: 10-Year results after sector resection with orwithout postoperative radiotherapy for stage I breast cancer: A randomized trial. JClin Oncol 17:2326–2333, 1999
44. Maibenco DC, Weiss LK, Pawlish KS, et al: Axillary lymph node metastasis associatedwith small invasive breast carcinomas. Cancer 85:1530–1536, 1999
45. McCready DR, Chapman JA, Hanna WM, et al: Factors associated with local breastcancer recurrence after lumpectomy alone: Postmenopausal patients. Ann Surg Oncol7:562–567, 2000
46. McGee JM, Youmans R, Clingan F, et al: The value of axillary dissection in T1a breastcancer. Am J Surg 172:501–505, 1996
47. Mullan MH, Deacock SJ, Quiney NF, et al: Anaphylaxis to patent blue dye duringsentinel lymph node biopsy for breast cancer. Eur J Surg Oncol 27:218–219, 2001
48. Mustafa IA, Bland KI: Indications for axillary dissection in T1 breast cancer. AnnSurg Oncol 5:4–8, 1998
49. Mustafa IA, Cole B, Wanebo HJ, et al: The impact of histopathology on nodalmetastasis in minimal breast cancer. Arch Surg 132:384–391, 1997
50. Osborne MP, Hoda SA: Current management of lobular carcinoma in situ of thebreast. Oncology 8:45–54, 1994
51. Osborne MP, Borgen PI: Atypical ductal and lobular hyperplasia and breast cancerrisk. Surg Clin North Am 2:1–11, 1993
52. Reger V, Beito G, Jolly PC: Factors affecting the incidence of lymph node metastasesin small cancers of the breast. Am J Surg 157:501–502, 1989
53. Rivadeneira DE, Simmons RM, Christos PJ, et al: Predictive factors associated withaxillary lymph node metastases in T1a and T1b breast carcinomas: Analysis in morethan 900 patients. J Am Coll Surg 191:1–6, 2000
54. Rush Port E, Tan LK, Borgen PI, et al: Incidence of axillary lymph node metastasis inT1a and T1b breast carcinoma. Ann Surg Oncol 5:23–27, 1998
55. Saiz E, Toonkel R, Poppiti RJ, et al: Infiltrating breast carcinoma smaller than 0.5centimeters: Is lymph node dissection necessary? Cancer 85:2206–2211, 1999
188 CHUNG et al
56. Sapunar F, Smith IE: Neoadjuvant chemotherapy for breast cancer. Ann Med 32:43–50, 2000
57. Schnitt SJ, Hayman J, Gelman R, et al: A prospective study of conservative surgeryalone in the treatment of selected patients with stage I breast cancer. Cancer 77:1094–1100, 1996
58. Schwartz GF, Solin LJ, Olivotto IO, et al, and the Consensus Conference Committee:The Consensus Conference on the Treatment of In Situ Ductal Carcinoma of theBreast, April 22–25, 1999. Seminars in Breast Disease 3:209–217, 2000
59. Shoup M, Malinzak L, Weisenberger J, et al: Predictors of axillary lymph nodemetastasis in T1 breast carcinoma. Am Surg 65:748–752, 1999
60. Silverstein MJ, Lagios MD, Craig PH, et al: A prognostic index for ductal carcinomain situ of the breast. Cancer 77:2267–2274, 1996
61. Silverstein MJ, Lagios M, Groshen S, et al: The influence of margin width on localcontrol in patients with ductal carcinoma in situ (DCIS) of the breast. N Engl J Med340:1455–1461, 1999
62. Silverstein MJ: Current status of the Van Nuys Prognostic Index for patients withductal carcinoma in situ of the breast. Seminars in Breast Disease 3:220–228, 2000
63. Tabar L, Chen H-H, Duffy SW, et al: A novel method for prediction of long-termoutcome of women with T1a, T1b, and 10–14 mm invasive breast cancers: A prospec-tive study. Lancet 355:429–433, 2000
64. Van Zee KJ, Liberman L, Samli B, et al: Long term follow-up of women with ductalcarcinoma in situ treated with breast conservation surgery: The effect of age. Cancer86:1757–1767, 1999
65. Veronesi U, Salvadori A, Luini M, et al: Breast conservation is a safe method inpatients with small cancer of the breast: Long-term results of three randomised trialson 1973 patients. Eur J Cancer 31A:1574–1579, 1995
66. Veronesi U, Volterrani F, Luini A, et al: Quadrantectomy versus lumpectomy for smallsize breast cancer. Eur J Cancer 26:671–673, 1990
67. Veronesi U, Luini A, del Vecchio M, et al: Radiotherapy after breast-preservingsurgery in women with localized cancer of the breast. N Engl J Med 328:1587–1591,1993
68. Vicin FA, Kestin LL, Goldstein NS, et al: Impact of young age on outcome in patientswith ductal carcinoma in situ treated with breast conserving surgery. J Clin Oncol 18:296–306, 2000
69. Welch GH, Black WC: Using autopsy series to estimate the disease ‘reservoir’ forductal carcinoma in situ of the breast: How much more breast cancer can we find?Ann Intern Med 127:1023–1028, 1997
70. Weng EJ, Juillard GJ, Parker RG, et al: Outcomes and factors impacting local recur-rence of ductal carcinoma in situ. Cancer 88:1643–1649, 2000
71. Whitten TM, Fraser HR, Christensen WN, et al: Axillary lymph node metastasis instage T1a breast cancer: A pathologic review of 82 patients. Am Surg 63:1–6, 1997
72. Zavotsky J, Hansen N, Brennan MB, et al: Lymph node metastasis from ductalcarcinoma in situ with microinvasion. Cancer 85:2439–2443, 1999
Address reprint requests to
Maureen A. Chung, MD, PhD, FACSThe Breast Health Center, Women and Infants Hospital