Continuum Care For Continuum Care For Families Families Overview of the Overview of the ASAM Patient Placement ASAM Patient Placement Criteria Criteria Michael Ryan, LCSW, Michael Ryan, LCSW, CASAC CASAC February 2014 February 2014
Transcript
Continuum Care For Families Continuum Care For Families Overview of the ASAM Patient Overview of the ASAM Patient
Placement CriteriaPlacement Criteria
Michael Ryan, LCSW, Michael Ryan, LCSW, CASACCASAC
February 2014February 2014
• In the past AOD treatment models have been In the past AOD treatment models have been used as a “one size fits all” approach for almost used as a “one size fits all” approach for almost all patients who met the criteria for the treatment all patients who met the criteria for the treatment of alcohol or other drug addiction.of alcohol or other drug addiction.
• Today, in the AOD treatment field, there is a Today, in the AOD treatment field, there is a movement toward using a variety of treatment movement toward using a variety of treatment models to ensure access to quality treatment models to ensure access to quality treatment and conserve healthcare resources. Now and conserve healthcare resources. Now clinicians must focus on matching patients to clinicians must focus on matching patients to appropriate, specific treatment, rather than on appropriate, specific treatment, rather than on placing patients in established programs.placing patients in established programs.
• The success of clinically driven treatment The success of clinically driven treatment depends on the importance of an accurate depends on the importance of an accurate diagnosis.diagnosis.
• However, it is not only a diagnosis of an However, it is not only a diagnosis of an AOD disorder, but also of the severity of AOD disorder, but also of the severity of the disorder, that must determine the kind the disorder, that must determine the kind of treatment an individual patient should of treatment an individual patient should receive (Severity of Illness) (SI).receive (Severity of Illness) (SI).
• This determination can result in: This determination can result in: placement of patients in the correct level placement of patients in the correct level of care, movement to less intensive or of care, movement to less intensive or more intensive levels when appropriate, more intensive levels when appropriate, and matching patients individually to a and matching patients individually to a variety of treatment modalities at all levels variety of treatment modalities at all levels of care.of care.
• March 1991, the American Society of March 1991, the American Society of Addiction Medicine published “Patient Addiction Medicine published “Patient Placement Criteria for the Treatment of Placement Criteria for the Treatment of Psychoactive Substance Use Disorders”. Psychoactive Substance Use Disorders”. These criteria for admission, continued These criteria for admission, continued stay, and discharge were described in stay, and discharge were described in terms of four levels of care, for both adults terms of four levels of care, for both adults and adolescents. and adolescents.
• The American Society of Addiction The American Society of Addiction Medicine's (ASAM) Patient Placement Medicine's (ASAM) Patient Placement Criteria (ASAM PPC-2R) is the most Criteria (ASAM PPC-2R) is the most widely used and comprehensive national widely used and comprehensive national guidelines for placement, continued stay guidelines for placement, continued stay and discharge of patients with alcohol and and discharge of patients with alcohol and other drug problems. other drug problems.
Placement CriteriaPlacement Criteria
• The overall intent of patient placement guidelines is to The overall intent of patient placement guidelines is to place a person in the least intensive level of care that will place a person in the least intensive level of care that will achieve AOD treatment objectives without sacrificing achieve AOD treatment objectives without sacrificing safety or securitysafety or security
• They are also an attempt to establish patient placement They are also an attempt to establish patient placement criteria that are acceptable to all treatment providers and criteria that are acceptable to all treatment providers and payerspayers
• They support efforts to establish a common language for They support efforts to establish a common language for AOD abuse treatment, to agree on consistent placement AOD abuse treatment, to agree on consistent placement decisions and provide a focus for future researchdecisions and provide a focus for future research
The ASAM PPC-2RThe ASAM PPC-2R
• The ASAM PPC-2R provides two sets of guidelines, The ASAM PPC-2R provides two sets of guidelines, one for adults and one for adolescents, and four one for adults and one for adolescents, and four broad levels of care for each group. broad levels of care for each group.
• Level I Outpatient treatment Level I Outpatient treatment • Level II Intensive outpatient / partial hospitalizationLevel II Intensive outpatient / partial hospitalization• Level III Medically monitored intensive inpatient Level III Medically monitored intensive inpatient
treatmenttreatment• Level IV Medically managed intensive inpatient Level IV Medically managed intensive inpatient
treatment. treatment. •
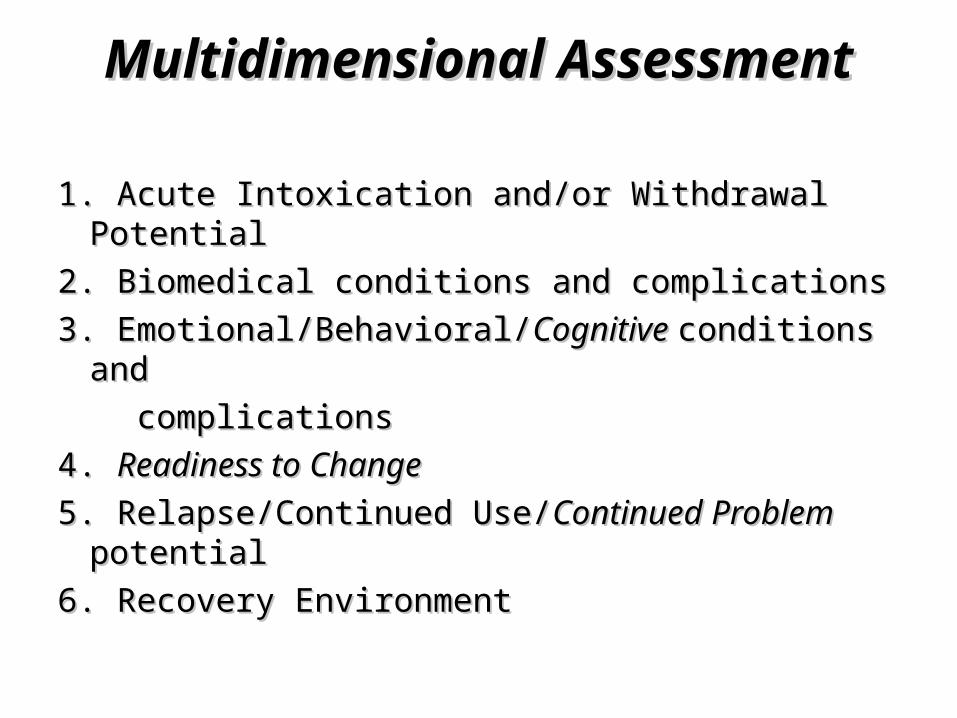
Six Assessment DimensionsSix Assessment Dimensions
• 2. Biomedical conditions and complications.2. Biomedical conditions and complications.• 3. Emotional, behavioral, or cognitive conditions 3. Emotional, behavioral, or cognitive conditions
and complications.and complications.• 4. Readiness to change, treatment acceptance / 4. Readiness to change, treatment acceptance /
resistance.resistance.
• 5. Relapse, continued use, or continued 5. Relapse, continued use, or continued problem potential.problem potential.
• 6. Recovery / living environment.6. Recovery / living environment.
• The ASAM criteria were designed to The ASAM criteria were designed to provide guidelines for placing patients with provide guidelines for placing patients with specific combinations of problems in specific combinations of problems in appropriate levels of safe and cost-appropriate levels of safe and cost-efficient care.efficient care.
• A strength of ASAM’s criteria is that they A strength of ASAM’s criteria is that they characterize levels of care and patients in characterize levels of care and patients in some detail.some detail.
• This common language of levels of care, This common language of levels of care, multidimensional assessment of severity, multidimensional assessment of severity, and specific placements of patients in a and specific placements of patients in a level of care give the treatment field level of care give the treatment field systematic ways to describe the treatment systematic ways to describe the treatment continuum and identify where patients continuum and identify where patients belong in the continuum.belong in the continuum.
Level I OutpatientLevel I Outpatient
• Outpatient Treatment – organized nonresidential Outpatient Treatment – organized nonresidential treatment service or an office practice with treatment service or an office practice with designated addiction professionals and designated addiction professionals and clinicians providing professionally directed AOD clinicians providing professionally directed AOD treatmenttreatment
• This treatment occurs in regularly scheduled This treatment occurs in regularly scheduled sessions usually totaling fewer than 9 contact sessions usually totaling fewer than 9 contact hours a week, includes both individual and hours a week, includes both individual and group therapygroup therapy
Level II Intensive Outpatient Level II Intensive Outpatient TreatmentTreatment
• Includes partial hospitalizationIncludes partial hospitalization
• Organized service in which addiction Organized service in which addiction professionals and clinicians provide professionals and clinicians provide several AOD service components to several AOD service components to clientsclients
• Minimum of 9 treatment hours per weekMinimum of 9 treatment hours per week
• Patients attend a full spectrum of Patients attend a full spectrum of treatment programmingtreatment programming
Level III Medically Monitored Level III Medically Monitored Intensive Inpatient TreatmentIntensive Inpatient Treatment
• Organized service conducted by addiction Organized service conducted by addiction professionals and clinicians who provide a professionals and clinicians who provide a planned regimen of around-the-clock planned regimen of around-the-clock professionally directed evaluation, care, and professionally directed evaluation, care, and treatment in an inpatient settingtreatment in an inpatient setting
• This level of care includes 24-hour observation, This level of care includes 24-hour observation, monitoring, and treatment. A multidisciplinary monitoring, and treatment. A multidisciplinary team functions under medical supervisionteam functions under medical supervision
Level IV Medically Managed Level IV Medically Managed Intensive Inpatient TreatmentIntensive Inpatient Treatment
• Organized service in which addiction Organized service in which addiction professionals and clinicians provide a planned professionals and clinicians provide a planned regimen of 24-hour medically directed regimen of 24-hour medically directed evaluation, care, and treatment in an acute care evaluation, care, and treatment in an acute care inpatient settinginpatient setting
• Patients generally have severe withdrawal or Patients generally have severe withdrawal or medical, emotional, or behavioral problems that medical, emotional, or behavioral problems that require primary medical and nursing servicesrequire primary medical and nursing services
Underlying Concepts of ASAM PPC Underlying Concepts of ASAM PPC Biopsychosocial Perspective of AddictionBiopsychosocial Perspective of Addiction
– Biopsychosocial in etiology, expression, Tx.Biopsychosocial in etiology, expression, Tx.– Comprehensive assessment and treatmentComprehensive assessment and treatment– Explains clinical diversity with commonalitiesExplains clinical diversity with commonalities– Promotes integration of knowledgePromotes integration of knowledge
2. Biomedical conditions and complications 2. Biomedical conditions and complications
3. Emotional/Behavioral/3. Emotional/Behavioral/Cognitive Cognitive conditions and conditions and
complications complications
4. 4. Readiness to ChangeReadiness to Change
5. Relapse/Continued Use/5. Relapse/Continued Use/Continued Problem Continued Problem potentialpotential
6. Recovery Environment6. Recovery Environment
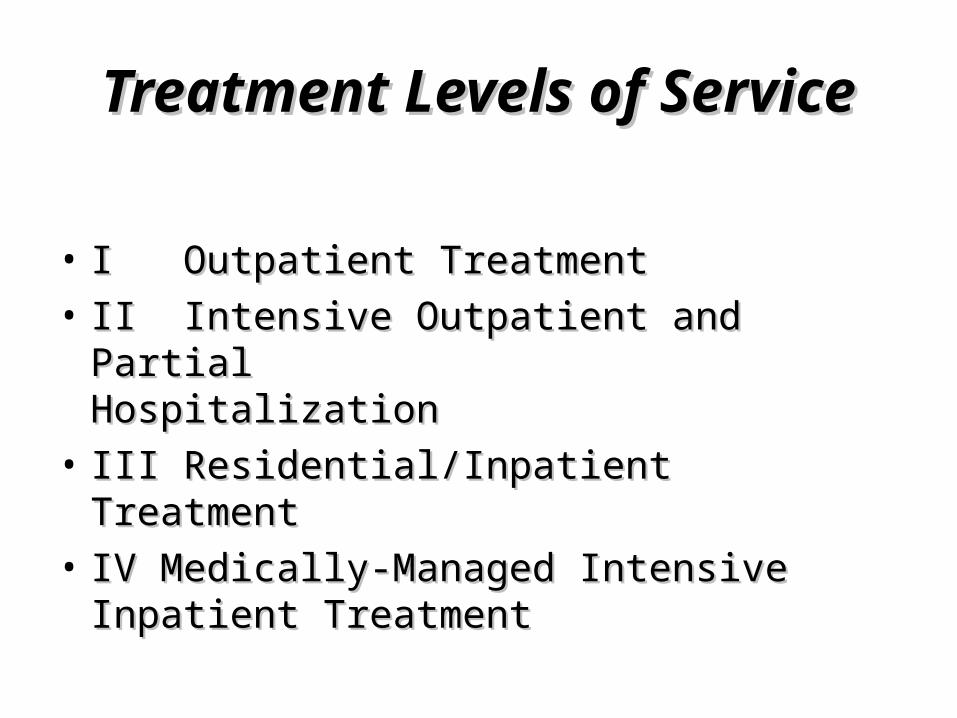
Treatment Levels of ServiceTreatment Levels of Service
• I Outpatient TreatmentI Outpatient Treatment
• II Intensive Outpatient and Partial II Intensive Outpatient and Partial Hospitalization Hospitalization
• III Residential/Inpatient TreatmentIII Residential/Inpatient Treatment
• IV Medically-Managed Intensive Inpatient IV Medically-Managed Intensive Inpatient TreatmentTreatment
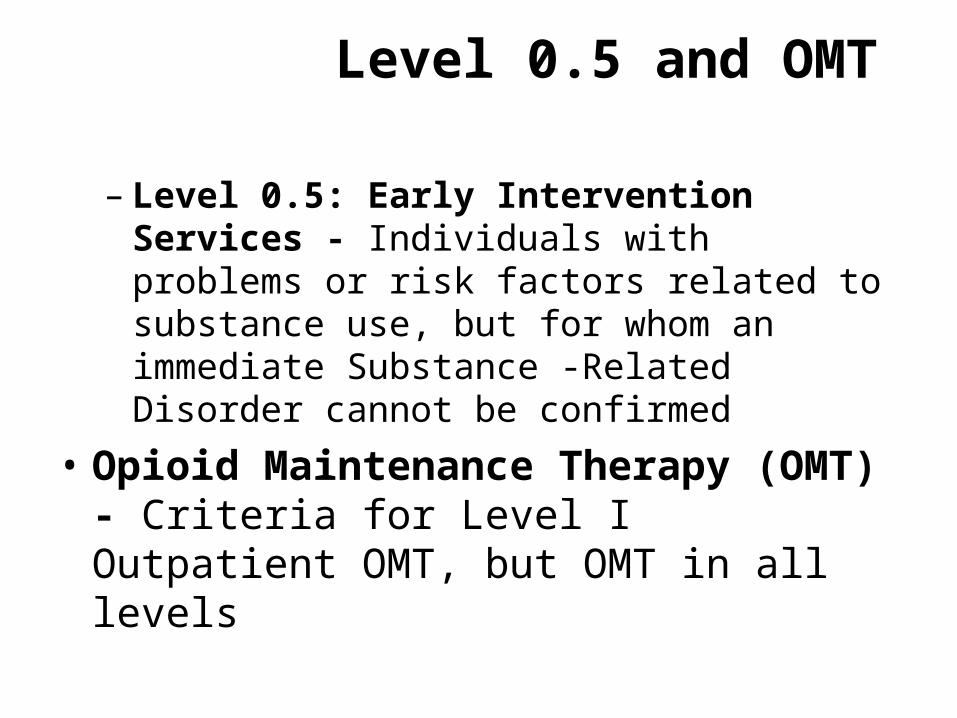
Level 0.5 and OMT
– Level 0.5: Early Intervention Services - Individuals with problems or risk factors related to substance use, but for whom an immediate Substance -Related Disorder cannot be confirmed
• Opioid Maintenance Therapy (OMT) - Criteria for Level I Outpatient OMT, but OMT in all levels
Detoxification Services for Dimension 1
• I-D - Ambulatory Detoxification without Extended On-site Monitoring
• II-D - Ambulatory Detoxification with Extended On-Site Monitoring
Detoxification Services Dimension IDetoxification Services Dimension I
• Level IV Medically-Managed Intensive Inpatient Treatment
Cost BenefitCost Benefit
• A strength of the ASAM criteria is the potential A strength of the ASAM criteria is the potential for cost savings. A major difference in cost is for cost savings. A major difference in cost is spanned in distinguishing between Level III and spanned in distinguishing between Level III and Level IV treatment (medically managed vs. Level IV treatment (medically managed vs. medically monitored; acute vs. subacute care).medically monitored; acute vs. subacute care).
• Previously, Level III (short term, medically Previously, Level III (short term, medically monitored, residential treatment) was frequently monitored, residential treatment) was frequently provided in hospital settings at acute-care rates.provided in hospital settings at acute-care rates.
• The codification of a continuum of care The codification of a continuum of care although limited to four levels of care although limited to four levels of care provides PPC that can help move the provides PPC that can help move the treatment field toward more treatment field toward more comprehensive and cost-effective comprehensive and cost-effective continuums of care.continuums of care.
• Uniform criteria can bring stability and Uniform criteria can bring stability and consistency to the field of AOD treatment, consistency to the field of AOD treatment, allowing diverse disciplines and organizations to allowing diverse disciplines and organizations to work together. Once implemented, they can work together. Once implemented, they can provide a common agenda, a common provide a common agenda, a common language, and shared expectations about language, and shared expectations about treatment across different groups of treatment across different groups of multidisciplinary service providers, payers, multidisciplinary service providers, payers, policymakers, and others.policymakers, and others.
• Most third-party insurance plans limit coverage Most third-party insurance plans limit coverage to services and supplies that are “medically to services and supplies that are “medically necessary.” While plans may define the term necessary.” While plans may define the term differently, the intent is to exclude from coverage differently, the intent is to exclude from coverage unnecessary treatment services, equipment, and unnecessary treatment services, equipment, and supplies.supplies.
• Most plans’ definition of medically necessary Most plans’ definition of medically necessary services include, at a minimum, the following services include, at a minimum, the following elements:elements:
• 1. The service must be ordered by a 1. The service must be ordered by a professional whose license qualifies him or professional whose license qualifies him or her to diagnose and deliver treatment.her to diagnose and deliver treatment.
• 2. It must be of the proper quantity, 2. It must be of the proper quantity, frequency, and duration for the condition frequency, and duration for the condition being treated.being treated.
• 3. It must not be experimental or 3. It must not be experimental or investigative.investigative.
• Failure to satisfy the second element is Failure to satisfy the second element is generally the issue in disputes between generally the issue in disputes between AOD treatment providers and third-party AOD treatment providers and third-party payers.payers.
StabilizationEarly Recovery
Middle RecoveryLate RecoveryMaintenance
PERIODS OF RECOVERY PERIODS OF RECOVERY TRANSITIONS TRANSITIONS
• Stabilization major task: recovering from withdrawal, Stabilization major task: recovering from withdrawal, overcoming preoccupation with chemicals, learning to overcoming preoccupation with chemicals, learning to cope without using AOD’s, and developing hope and cope without using AOD’s, and developing hope and motivation for long-term recovery.motivation for long-term recovery.
• Early Recovery major goal is to change attitudes and Early Recovery major goal is to change attitudes and beliefs about AOD use that put client at risk of relapse: beliefs about AOD use that put client at risk of relapse: changing ones understanding of AOD use and role it has changing ones understanding of AOD use and role it has played in ones life, exploring the purpose of AOD use, played in ones life, exploring the purpose of AOD use, learning to cope with life without AOD use by learning learning to cope with life without AOD use by learning new life skills. new life skills.
• Middle Recovery goal is usually the repair of damage to Middle Recovery goal is usually the repair of damage to life caused by AOD use: focusing on normal life issues life caused by AOD use: focusing on normal life issues rather than focusing on using AOD’s, making changes rather than focusing on using AOD’s, making changes that support life balance and ongoing personal growth.that support life balance and ongoing personal growth.
• Late Recovery goal is attaining lifestyle balance by Late Recovery goal is attaining lifestyle balance by overcoming problems that may have existed before overcoming problems that may have existed before AOD: recognizing problems form childhood that may be AOD: recognizing problems form childhood that may be affecting quality of life and recovery, making connections affecting quality of life and recovery, making connections between early problems and current problems, breaking between early problems and current problems, breaking the cycle of family dysfunction by restructuring habits of the cycle of family dysfunction by restructuring habits of thinking, feeling, and to support healthy living, moving thinking, feeling, and to support healthy living, moving past long-term obstacles to live lifestyle of choice. past long-term obstacles to live lifestyle of choice.
• Maintenance goal is to live productively and Maintenance goal is to live productively and enjoy life: maintaining some kind of program of enjoy life: maintaining some kind of program of recovery that helps a client recognize limitations recovery that helps a client recognize limitations imposed by AOD disorder, continuing to take imposed by AOD disorder, continuing to take personal inventory, improving conscious contact personal inventory, improving conscious contact with some sort of higher power, coping with with some sort of higher power, coping with normal life problems and complications, normal life problems and complications, continuing to grow and develop in all areas of continuing to grow and develop in all areas of life, coping with “stuck” points in recovery life, coping with “stuck” points in recovery process.process.
ChangeChange
• Any change means that something is different, Any change means that something is different, something (habit or way of daily life) must be left something (habit or way of daily life) must be left behind and a new way learned.behind and a new way learned.
• Changing social habits may mean that some of Changing social habits may mean that some of client’s friends will not understand and may not client’s friends will not understand and may not relate to client as they have in the past. Clients relate to client as they have in the past. Clients leave behind some lifestyle activities and friends leave behind some lifestyle activities and friends that they may have felt were important to them.that they may have felt were important to them.
• Feelings of loss are understandable, all new Feelings of loss are understandable, all new skills are important tasks in adjusting to life skills are important tasks in adjusting to life without what the client has lost. without what the client has lost.
Identifying FeelingsIdentifying Feelings
• The biggest problem most clients have in The biggest problem most clients have in identifying feelings is that they don’t have identifying feelings is that they don’t have words that describe their inner experience. words that describe their inner experience. There is something happening inside of There is something happening inside of them, but they don’t have words to tell them, but they don’t have words to tell someone else. Sometimes an exercise is someone else. Sometimes an exercise is created called a “feelings list” that client’s created called a “feelings list” that client’s can go over to help identify feelings and can go over to help identify feelings and put a name to them.put a name to them.
Life Management EvaluationLife Management Evaluation
• To determine what needs to change in a client’s life, it is To determine what needs to change in a client’s life, it is important to look at the whole life. A life-management important to look at the whole life. A life-management evaluation takes a look at four basic areas of life: evaluation takes a look at four basic areas of life: intimate / family life; work life (voc/ed); social life; and life intimate / family life; work life (voc/ed); social life; and life skills.skills.
• Intimate/family Life: applies to the people with whom a Intimate/family Life: applies to the people with whom a client lives with or is in close day-to-day contact with. client lives with or is in close day-to-day contact with. People with whom a client spends significant amounts of People with whom a client spends significant amounts of time with.time with.
• Work/Career Life: applies to people with whom the client Work/Career Life: applies to people with whom the client must interact with in meeting voc/ed goals.must interact with in meeting voc/ed goals.
• Social Life: people with whom the client is involved in Social Life: people with whom the client is involved in social activities but who are not part of their intimate or social activities but who are not part of their intimate or family life.family life.
• Life Skills: these are skills or activities a client has to Life Skills: these are skills or activities a client has to perform to keep life “functioning”, tasks a client needs to perform to keep life “functioning”, tasks a client needs to accomplish to keep problems from arising in ones life. accomplish to keep problems from arising in ones life. Life skills in problem solving, time management, financial Life skills in problem solving, time management, financial management etc.management etc.
• Sometimes a life management areas chart can be done Sometimes a life management areas chart can be done with the client to give direction as to what life areas need with the client to give direction as to what life areas need to be addressed. to be addressed.
• Many life-management skills have been lost or never Many life-management skills have been lost or never mastered during the periods of AOD use. Clients may mastered during the periods of AOD use. Clients may need to learn organizational skills to provide structure to need to learn organizational skills to provide structure to their lives. Clients may need help in developing life-their lives. Clients may need help in developing life-management skills.management skills.
• Impairments in thought and emotional processes are Impairments in thought and emotional processes are common in treatment. Retraining the impaired function common in treatment. Retraining the impaired function is possible. One method of structured practice of is possible. One method of structured practice of behavioral skills is called role playing. In role playing the behavioral skills is called role playing. In role playing the client is asked to recreate in a safe place (group or client is asked to recreate in a safe place (group or individual sessions) the actual situations that demand individual sessions) the actual situations that demand the use of a skill he/she is attempting to learn or relearn.the use of a skill he/she is attempting to learn or relearn.
• The client is then observed while trying to The client is then observed while trying to learn/relearn the skill and an appropriate learn/relearn the skill and an appropriate sequence of work-up steps is developed.sequence of work-up steps is developed.
• The most complex of life tasks can be broken The most complex of life tasks can be broken down into the simple component steps down into the simple component steps necessary to get there. Skills training simply necessary to get there. Skills training simply means breaking down skills into their simplest means breaking down skills into their simplest components and systematically learning each components and systematically learning each component and then assembling them into a component and then assembling them into a more complex skill.more complex skill.
Problem SolvingProblem Solving
• Problem identification – identifying what is causing the Problem identification – identifying what is causing the difficulty.difficulty.
• Problem clarification – being specific, is this the real Problem clarification – being specific, is this the real problem, or is there a more fundamental problem?problem, or is there a more fundamental problem?
• Identify alternatives – what are the options in dealing Identify alternatives – what are the options in dealing with the problem? Clients can make a list and see them with the problem? Clients can make a list and see them on paper, this can increase the clients chances of on paper, this can increase the clients chances of choosing the best solution.choosing the best solution.
• Projected consequences – what are the probable Projected consequences – what are the probable outcomes of each option. What is the best or worst case outcomes of each option. What is the best or worst case scenario from chosen option?scenario from chosen option?
• Decision - which option offers the best outcomes Decision - which option offers the best outcomes and seems to be the most reasonable choice for and seems to be the most reasonable choice for a solution based upon the alternatives.a solution based upon the alternatives.
• Action – Once a client decides on a solution to a Action – Once a client decides on a solution to a problem they need to plan how they will carry it problem they need to plan how they will carry it out. A plan is a map to achieve a goal.out. A plan is a map to achieve a goal.
• Follow-up – Carrying out of the plan is evaluated Follow-up – Carrying out of the plan is evaluated on how it is working. The plan can always be on how it is working. The plan can always be revised when a client realizes that another plan revised when a client realizes that another plan might work better. might work better.