34
Controversies in TB Meningitis Kelly Dooley, MD, PhD 7 th International Workshop on HIV Pediatrics Vancouver, Canada, 18 July 2015 D I V I S I O N O F C LI N I CA L PH AR M AC OL O G Y 1
Controversies in TB Meningitis
Kelly Dooley, MD, PhD7th International Workshop on HIV Pediatrics
Vancouver, Canada, 18 July 2015
D I V I S I O N O F
C LI N I CA L
P H AR M AC OL O G Y
1
Childhood TB: Towards Zero Deaths
• “Childhood TB needs to be lifted out of the shadows”• Historical neglect
• 530,000 cases in 2012 (underestimate)
• >75,000 deaths from TB yearly (in children without HIV)
2
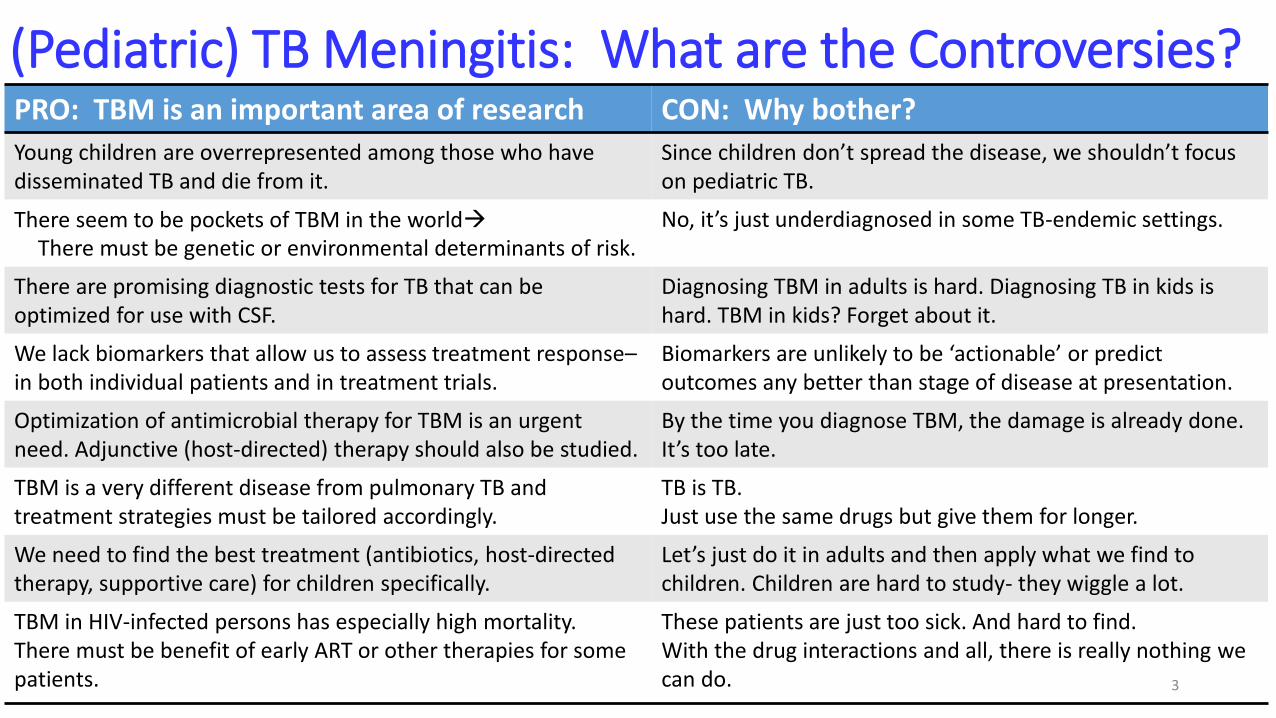
(Pediatric) TB Meningitis: What are the Controversies?PRO: TBM is an important area of research CON: Why bother?
Young children are overrepresented among those who have disseminated TB and die from it.
Since children don’t spread the disease, we shouldn’t focus on pediatric TB.
There seem to be pockets of TBM in the worldThere must be genetic or environmental determinants of risk.
No, it’s just underdiagnosed in some TB-endemic settings.
There are promising diagnostic tests for TB that can be optimized for use with CSF.
Diagnosing TBM in adults is hard. Diagnosing TB in kids is hard. TBM in kids? Forget about it.
We lack biomarkers that allow us to assess treatment response–in both individual patients and in treatment trials.
Biomarkers are unlikely to be ‘actionable’ or predict outcomes any better than stage of disease at presentation.
Optimization of antimicrobial therapy for TBM is an urgent need. Adjunctive (host-directed) therapy should also be studied.
By the time you diagnose TBM, the damage is already done. It’s too late.
TBM is a very different disease from pulmonary TB and treatment strategies must be tailored accordingly.
TB is TB. Just use the same drugs but give them for longer.
We need to find the best treatment (antibiotics, host-directed therapy, supportive care) for children specifically.
Let’s just do it in adults and then apply what we find to children. Children are hard to study- they wiggle a lot.
TBM in HIV-infected persons has especially high mortality. There must be benefit of early ART or other therapies for some patients.
These patients are just too sick. And hard to find.With the drug interactions and all, there is really nothing we can do. 3

Who gets TBM? Are there genetic determinants of risk and severity? Can these be used to direct interventions?
4
• Develops within one year of infection (household contact)
• Highest risk for severe disseminated disease like TBM: < 3 years of age, HIV co-infection, malnutrition
• Geographic variability in incidence-- “pockets of disease”• M. tuberculosis Strain? • Leukotriene A4 hydrolase (LTA4H) genotype distribution?
• Majority of children present at late stage:• Stage I (no focal neurologic signs, intact sensorium)• Stage II (disturbed consciousness or focal neurologic deficit)• Stage III (coma +/- focal neurologic deficits)
TBM: Epidemiology
5
6
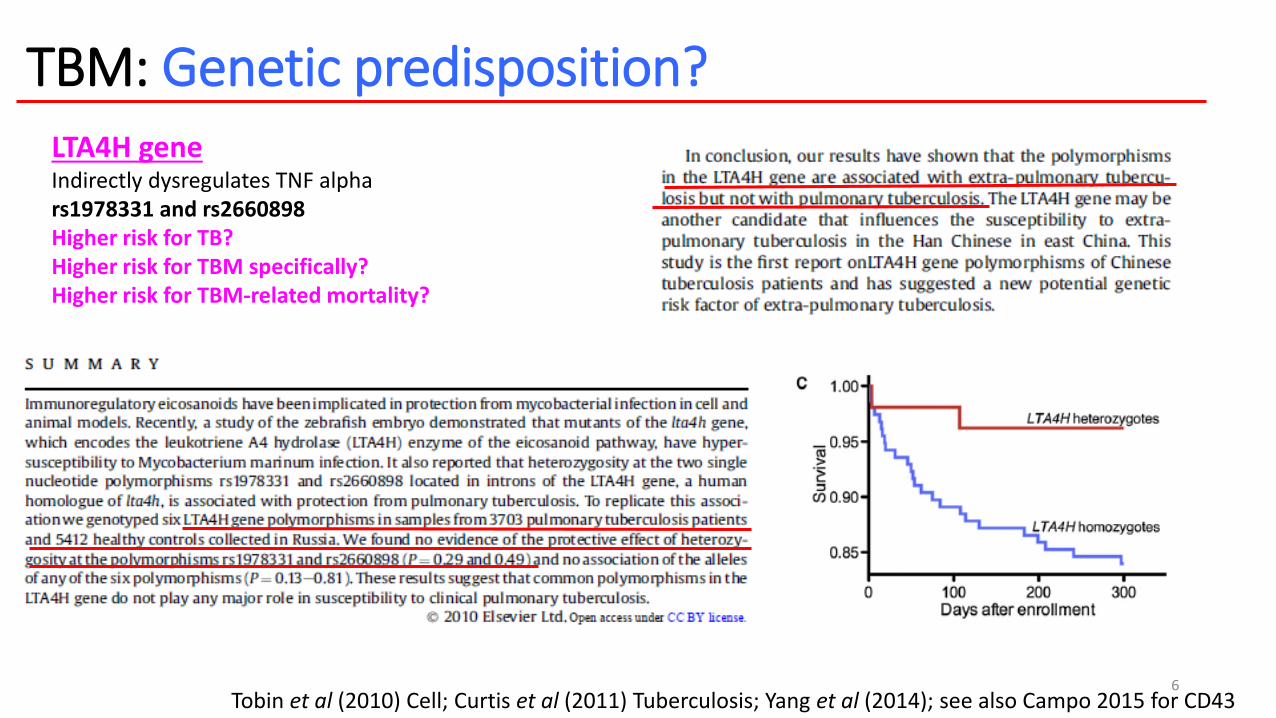
TBM: Genetic predisposition?LTA4H geneIndirectly dysregulates TNF alphars1978331 and rs2660898Higher risk for TB?Higher risk for TBM specifically?Higher risk for TBM-related mortality?
Tobin et al (2010) Cell; Curtis et al (2011) Tuberculosis; Yang et al (2014); see also Campo 2015 for CD43
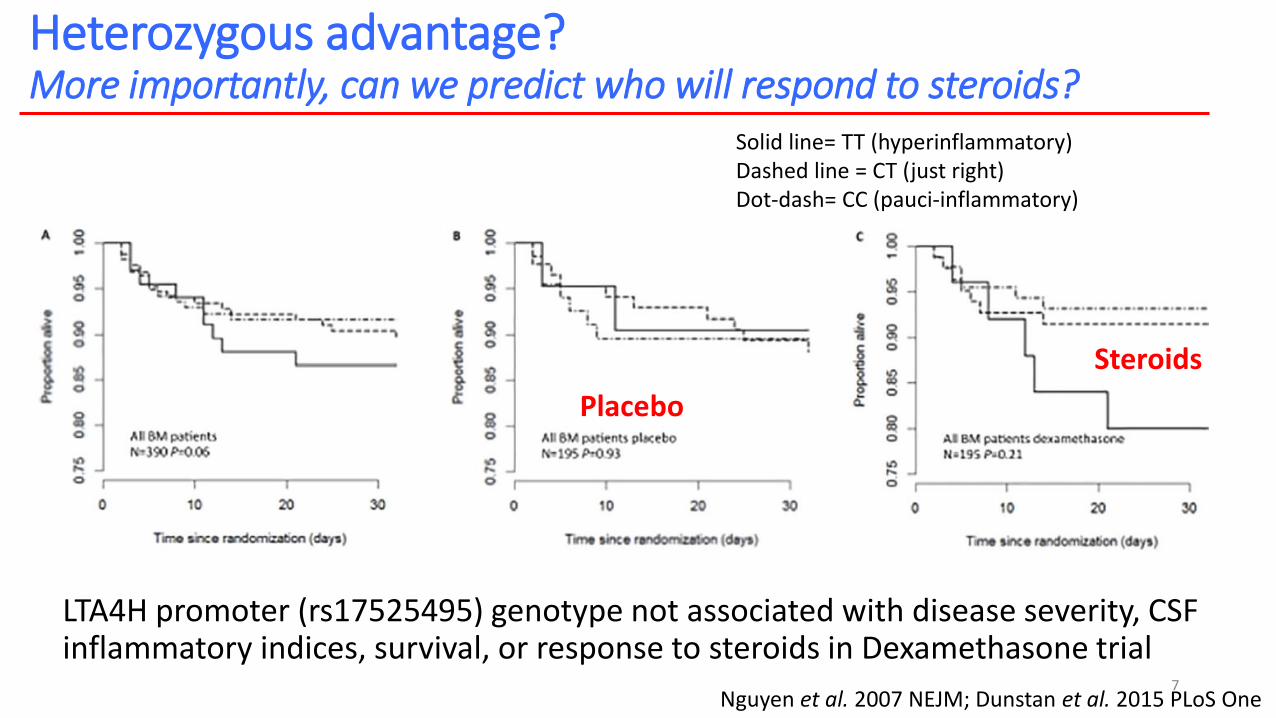
Heterozygous advantage? More importantly, can we predict who will respond to steroids?
LTA4H promoter (rs17525495) genotype not associated with disease severity, CSF inflammatory indices, survival, or response to steroids in Dexamethasone trial
7Nguyen et al. 2007 NEJM; Dunstan et al. 2015 PLoS One
Solid line= TT (hyperinflammatory)Dashed line = CT (just right)Dot-dash= CC (pauci-inflammatory)
Placebo
Steroids
What is the pathogenesis of TBM? Can better antimicrobial treatment be expected to improve outcomes?
8
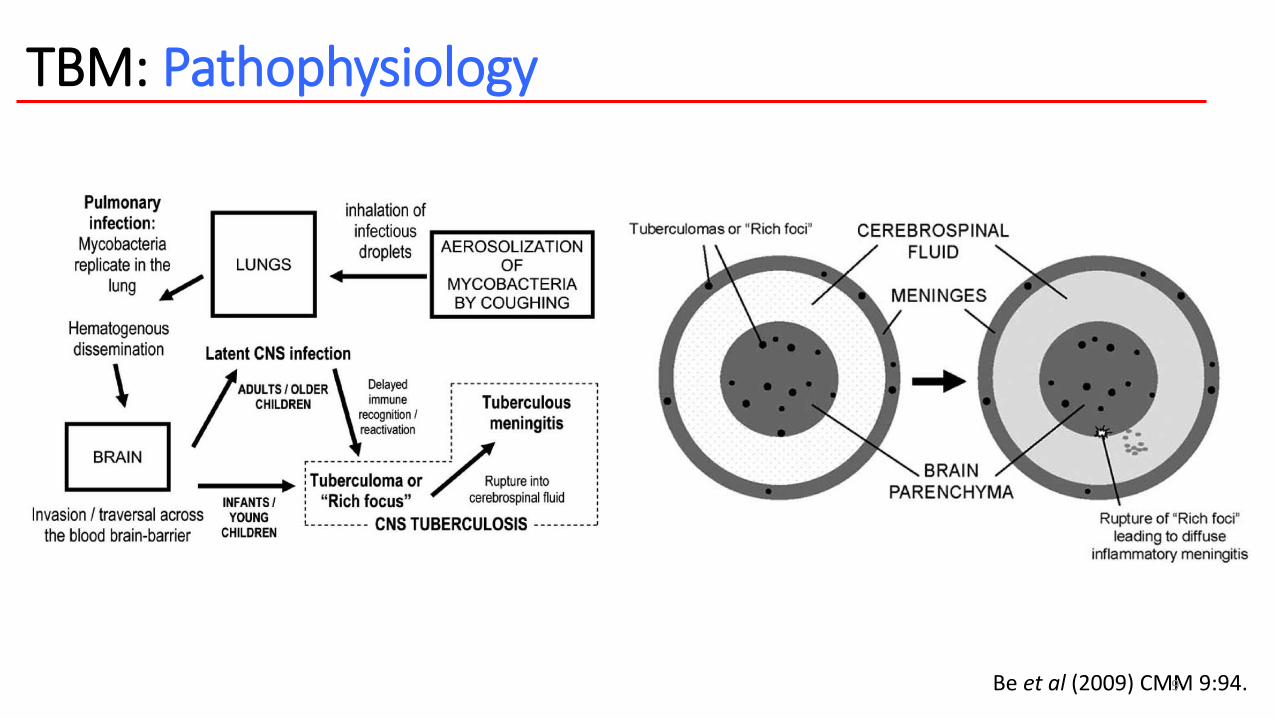
TBM: Pathophysiology
Be et al (2009) CMM 9:94.9
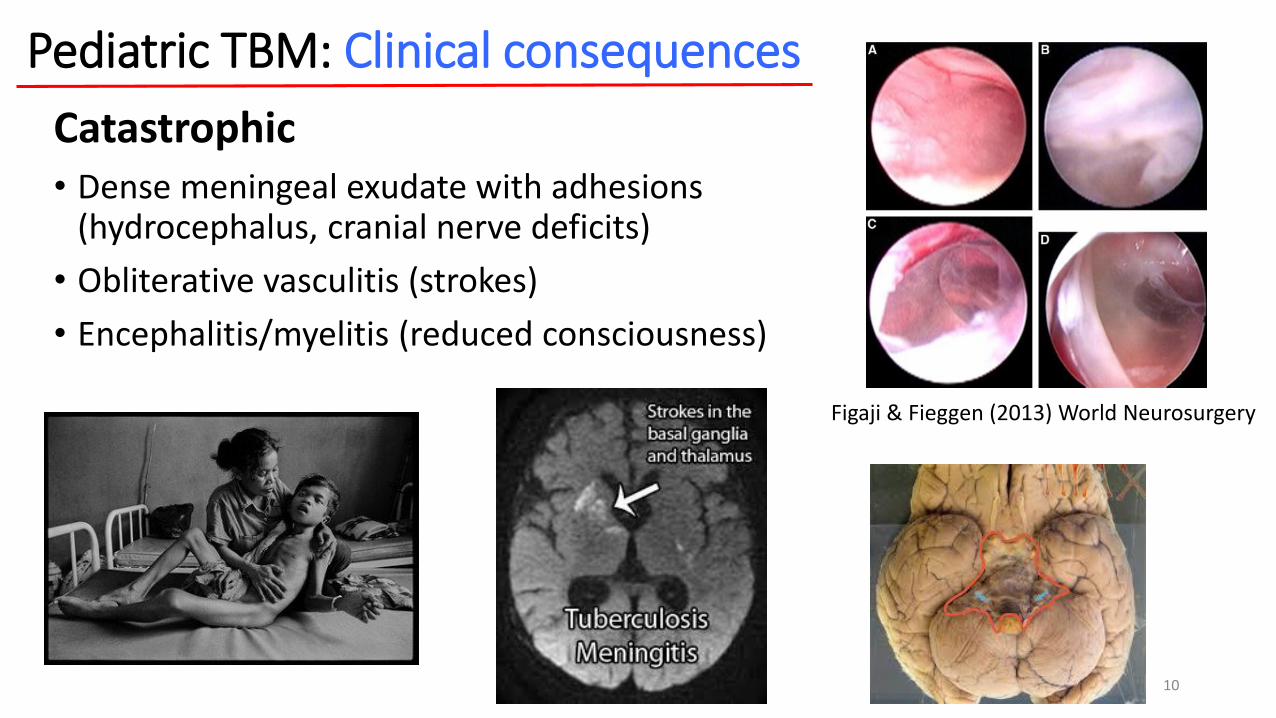
Pediatric TBM: Clinical consequences
Catastrophic• Dense meningeal exudate with adhesions
(hydrocephalus, cranial nerve deficits)
• Obliterative vasculitis (strokes)
• Encephalitis/myelitis (reduced consciousness)
10
Figaji & Fieggen (2013) World Neurosurgery

Do we need to study TBM in children specifically? Are disease manifestations and outcomes different in adults and children?
11
12
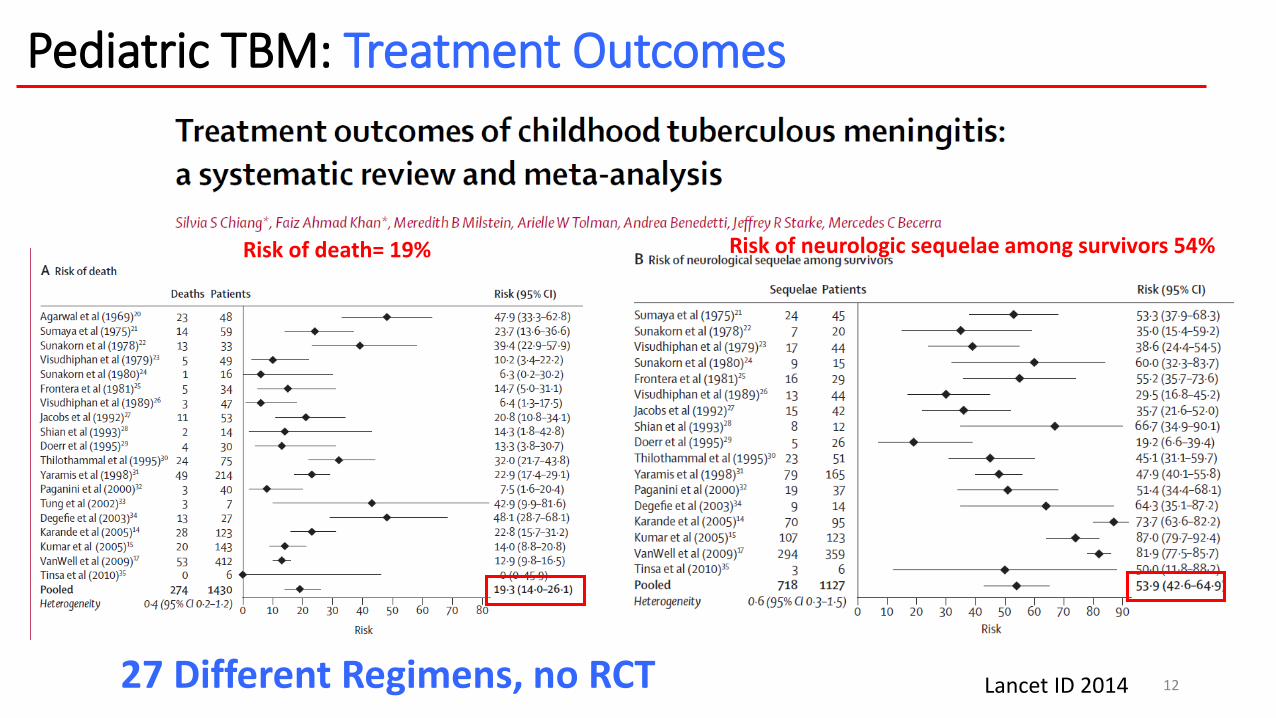
Pediatric TBM: Treatment Outcomes
Lancet ID 201427 Different Regimens, no RCT
Risk of death= 19% Risk of neurologic sequelae among survivors 54%
13
• Stage II and III TBM (N=554)• 6 months after treatment 58% with IQ deficit 50-80, 20% IQ deficit < 50Van Well (2009) Pediatrics
• Stage I-III TBM (N=123 children, ages 12-56 months)• 6-9 months after treatment, mild intellectual handicap 38% severe 25%
• Stage II and III TBM (N=74)• Behavioural disinhibitions as well as internalized emotional disorder Wait (2010) J Trop Ped
Long-term neurocognitive outcomes, impact on functioning in society, comparison to peers or children with other infectious diseases that impact the brain?
•Data are sparse: Cognitive and gross motor impairment, Behavioral difficulties, Emotional problems
Pediatric TB meningitis: What does TBM do to the developing brain?
Can we even diagnose TBM?14
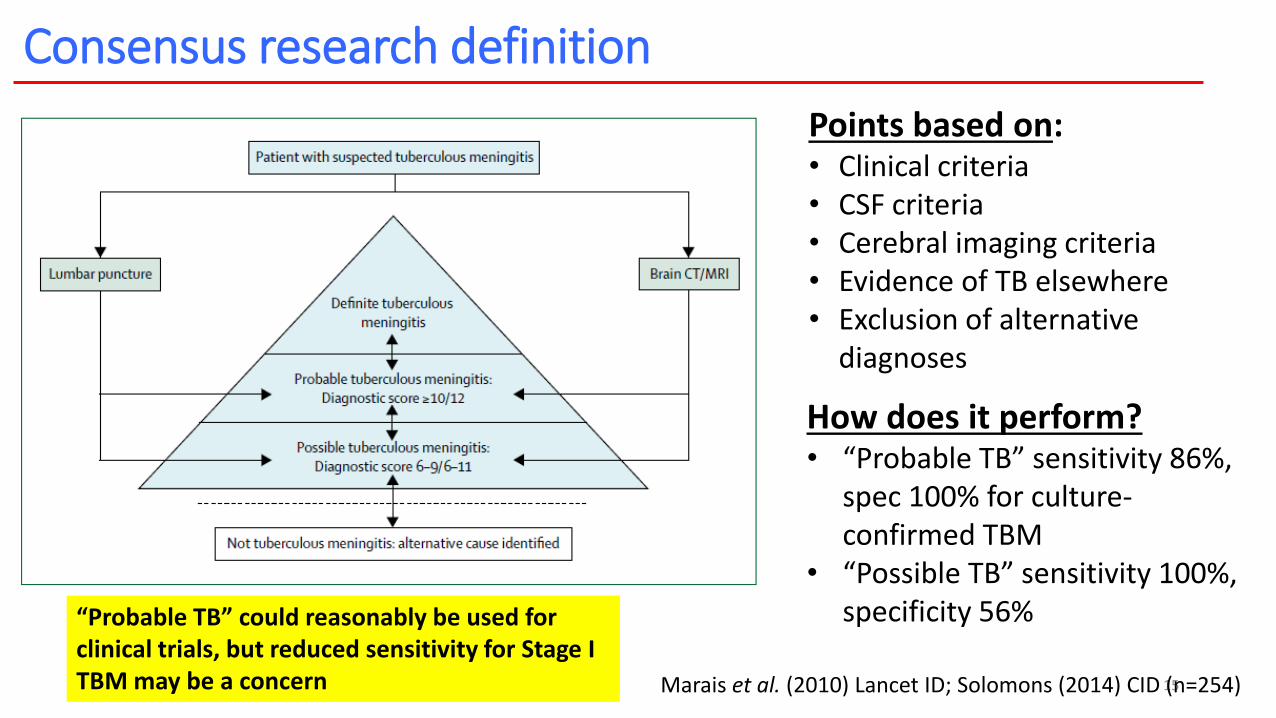
Consensus research definition
15
Points based on:• Clinical criteria• CSF criteria• Cerebral imaging criteria• Evidence of TB elsewhere• Exclusion of alternative
diagnoses
How does it perform?• “Probable TB” sensitivity 86%,
spec 100% for culture-confirmed TBM
• “Possible TB” sensitivity 100%, specificity 56%
Marais et al. (2010) Lancet ID; Solomons (2014) CID (n=254)
“Probable TB” could reasonably be used for clinical trials, but reduced sensitivity for Stage I TBM may be a concern

Gene Xpert on CSF- a promising new test?• Based on meta-analysis commissioned by WHO:
• pooled data from 13 studies including 709 CSF samples--• Xpert MTB/RIF in CSF has a sensitivity of 80% and specificity of 99%
16
World Health Organisation. 2013. Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children. Policy Update.
http://apps.who.int/iris/bitstream/10665/112472/1/9789241506335_eng.pdf
n.b. from recent JCM article: “Point-of-care tests have high accuracy to diagnose TBM in deceased HIV-infected adults.”
How do we treat TBM?How close are we to an ‘optimized regimen’?
17
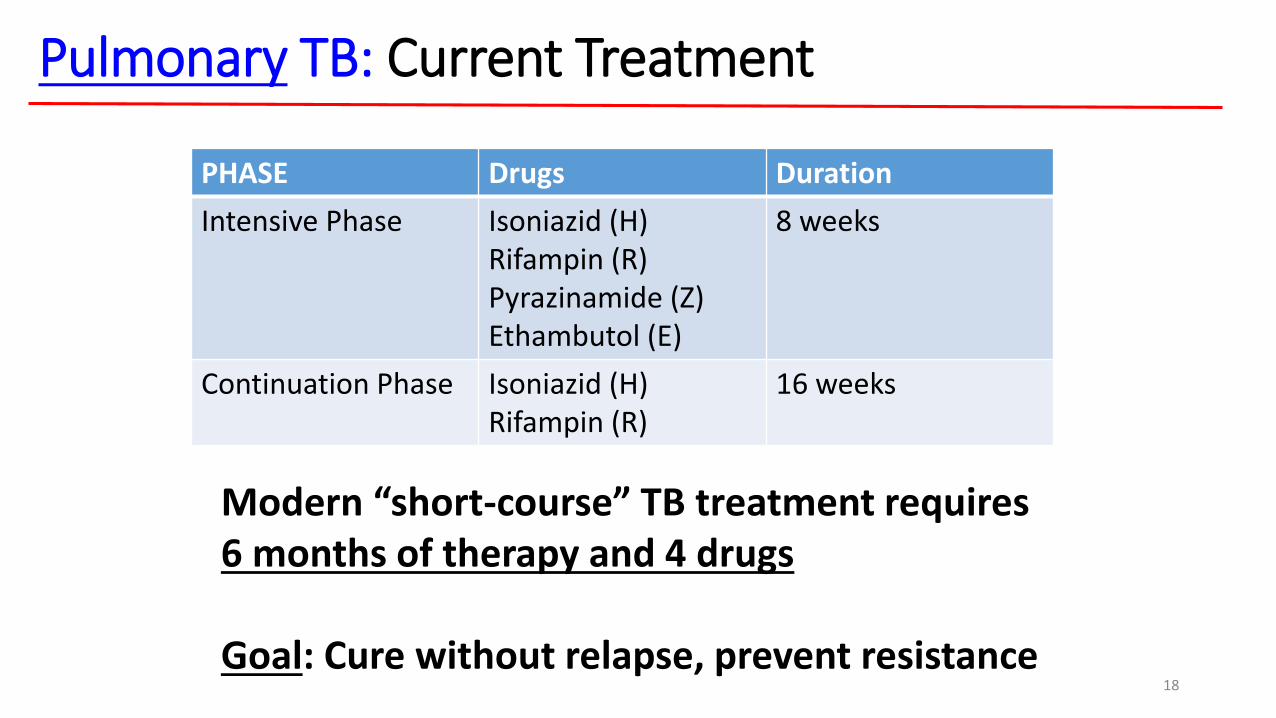
Pulmonary TB: Current Treatment
PHASE Drugs Duration
Intensive Phase Isoniazid (H)Rifampin (R)Pyrazinamide (Z)Ethambutol (E)
8 weeks
Continuation Phase Isoniazid (H)Rifampin (R)
16 weeks
Modern “short-course” TB treatment requires 6 months of therapy and 4 drugs
Goal: Cure without relapse, prevent resistance18
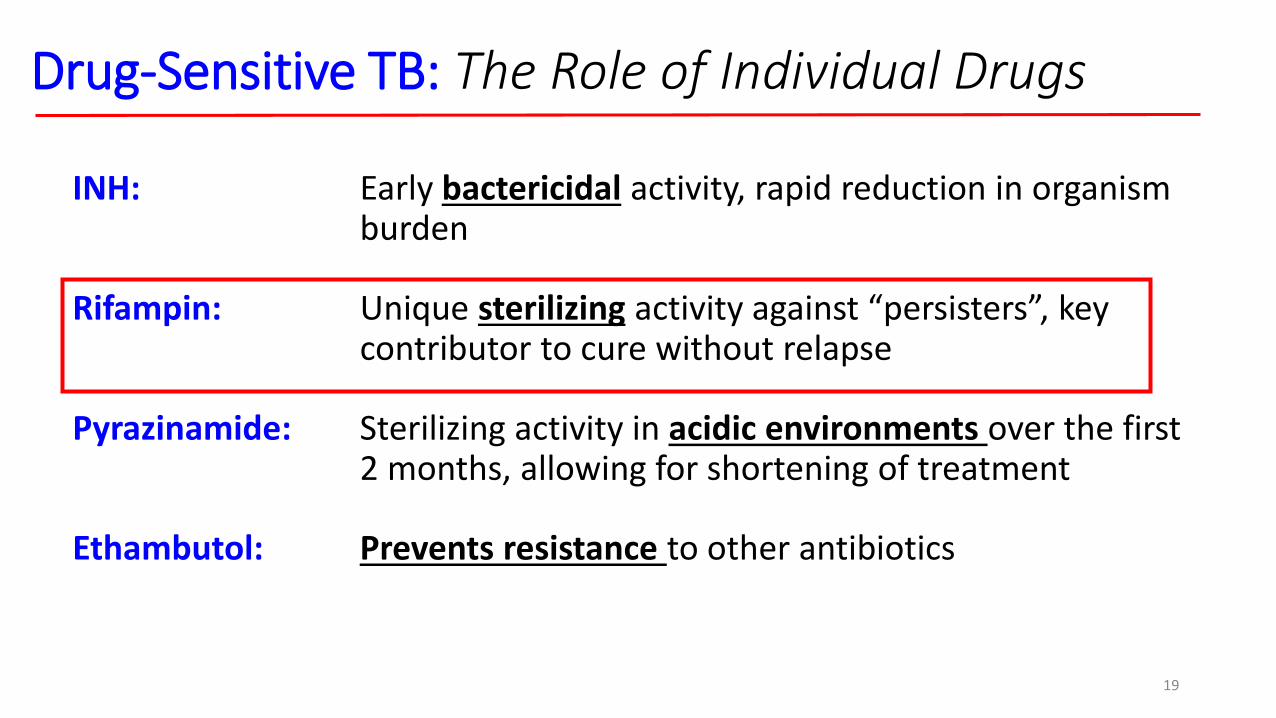
INH: Early bactericidal activity, rapid reduction in organism burden
Rifampin: Unique sterilizing activity against “persisters”, key contributor to cure without relapse
Pyrazinamide: Sterilizing activity in acidic environments over the first 2 months, allowing for shortening of treatment
Ethambutol: Prevents resistance to other antibiotics
Drug-Sensitive TB: The Role of Individual Drugs
19
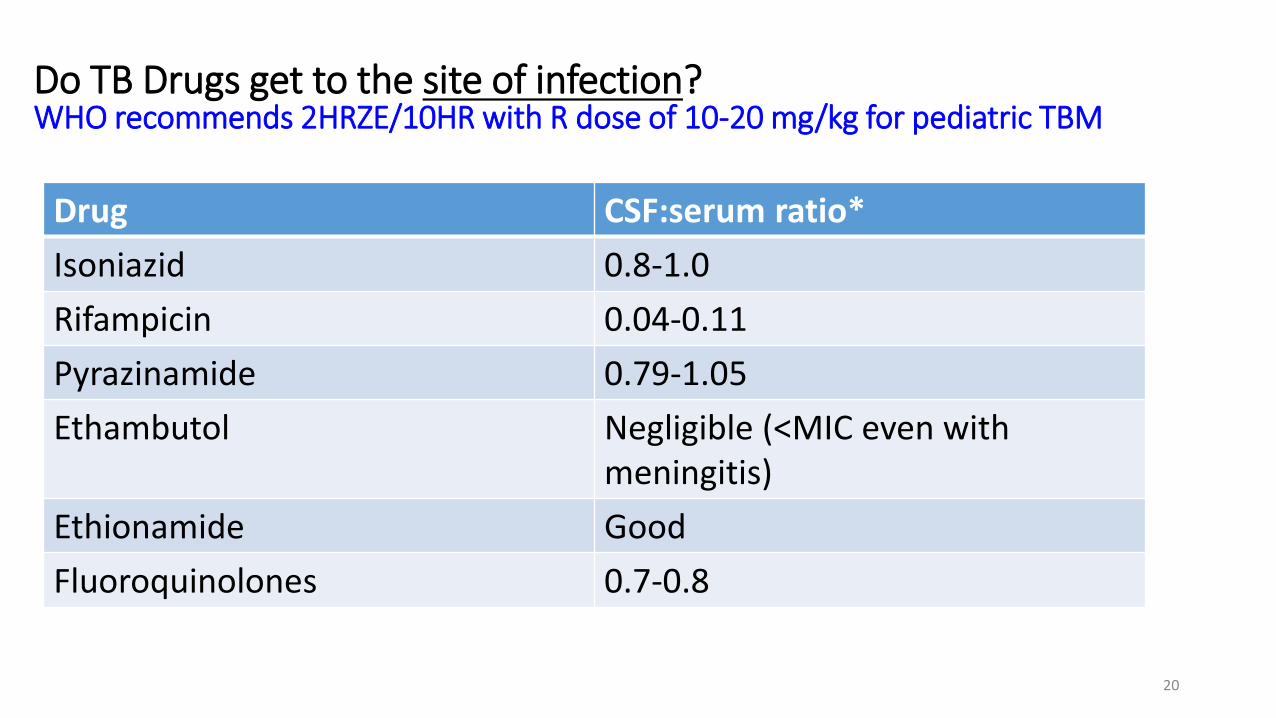
Drug CSF:serum ratio*
Isoniazid 0.8-1.0
Rifampicin 0.04-0.11
Pyrazinamide 0.79-1.05
Ethambutol Negligible (<MIC even with meningitis)
Ethionamide Good
Fluoroquinolones 0.7-0.8
20
Do TB Drugs get to the site of infection?WHO recommends 2HRZE/10HR with R dose of 10-20 mg/kg for pediatric TBM
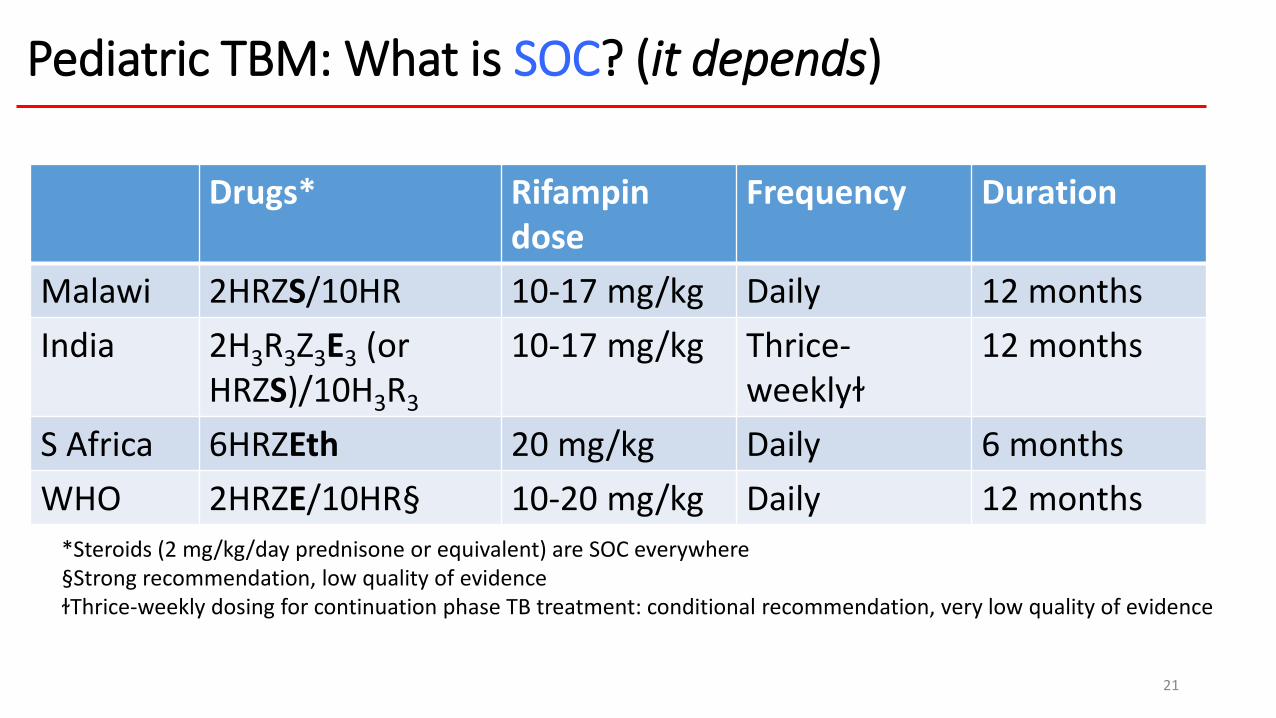
Drugs* Rifampin dose
Frequency Duration
Malawi 2HRZS/10HR 10-17 mg/kg Daily 12 months
India 2H3R3Z3E3 (orHRZS)/10H3R3
10-17 mg/kg Thrice-weeklyɫ
12 months
S Africa 6HRZEth 20 mg/kg Daily 6 months
WHO 2HRZE/10HR§ 10-20 mg/kg Daily 12 months
Pediatric TBM: What is SOC? (it depends)
*Steroids (2 mg/kg/day prednisone or equivalent) are SOC everywhere§Strong recommendation, low quality of evidenceɫThrice-weekly dosing for continuation phase TB treatment: conditional recommendation, very low quality of evidence
21
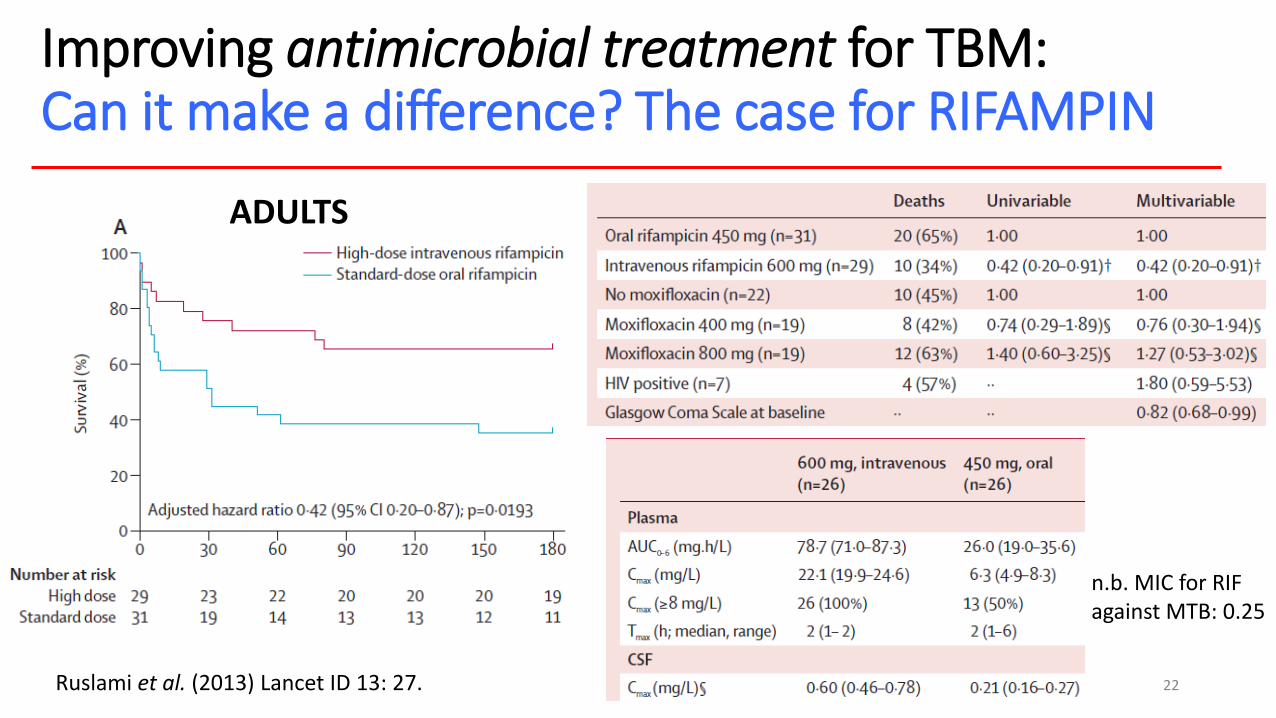
Improving antimicrobial treatment for TBM: Can it make a difference? The case for RIFAMPIN
Ruslami et al. (2013) Lancet ID 13: 27.
ADULTS
n.b. MIC for RIF against MTB: 0.25
22
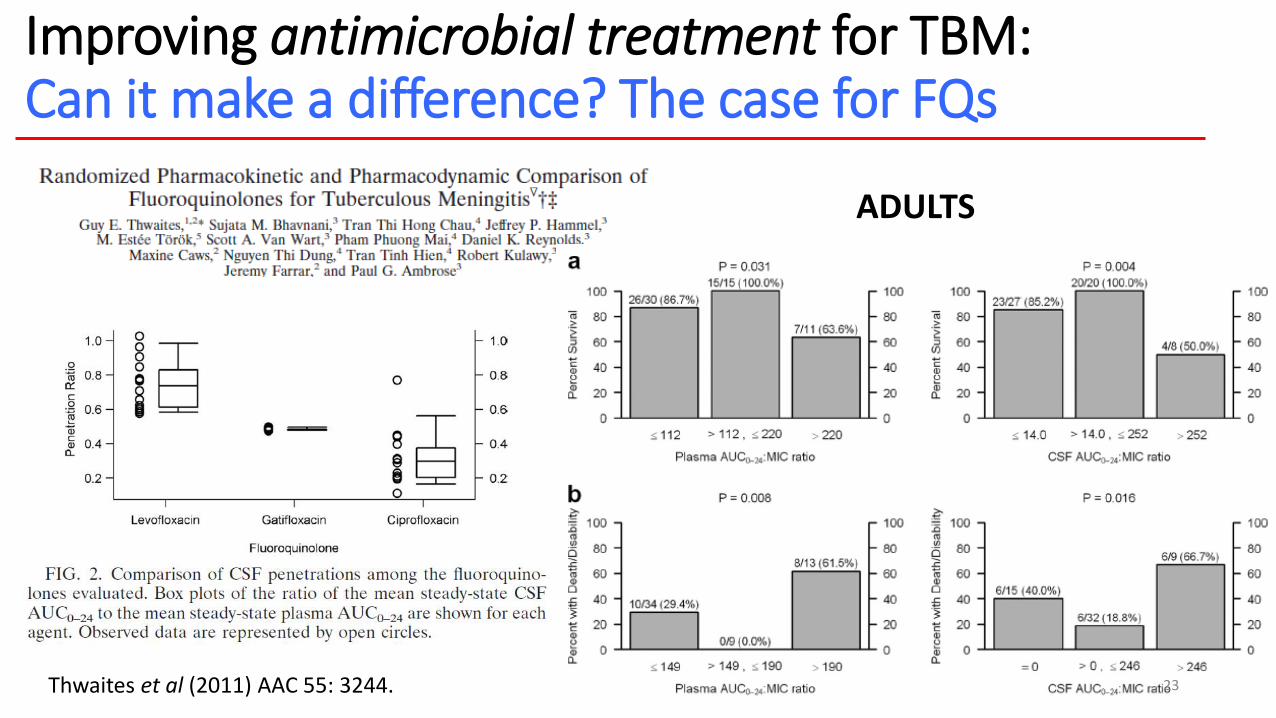
Improving antimicrobial treatment for TBM: Can it make a difference? The case for FQs
Thwaites et al (2011) AAC 55: 3244.
ADULTS
23
What about adjunctive treatment?Shouldn’t we be focusing on inflammation, vasculitis?
24
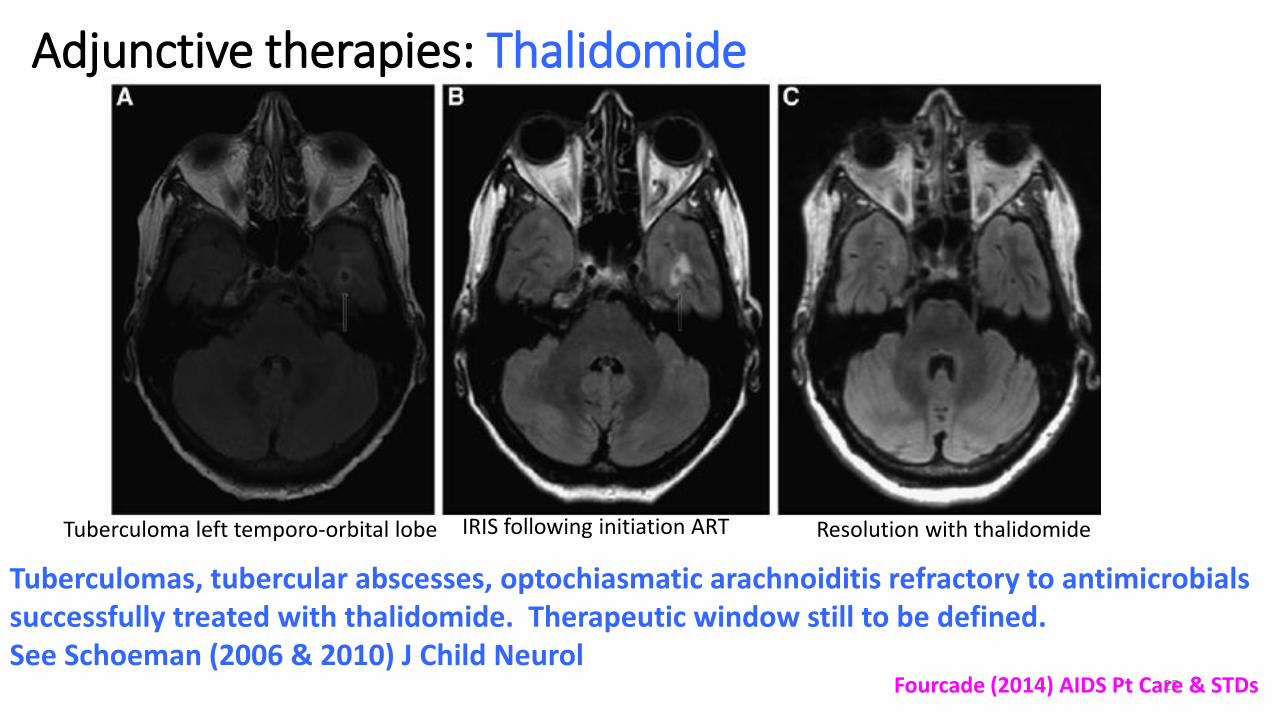
Adjunctive therapies: Thalidomide
25
Tuberculoma left temporo-orbital lobe IRIS following initiation ART Resolution with thalidomide
Fourcade (2014) AIDS Pt Care & STDs
Tuberculomas, tubercular abscesses, optochiasmatic arachnoiditis refractory to antimicrobials successfully treated with thalidomide. Therapeutic window still to be defined.See Schoeman (2006 & 2010) J Child Neurol
How can we run trials given the heterogeneity of disease?Are there any early biomarkers of treatment response to help us?
26
Biomarkers of treatment response
• Inflammatory markers: • cytokines in CSF-- TNF-alpha, IFN-gamma, IL6, neopterin
• Markers of neuronal injury--S100B, enolase
• Must consider blood-brain barrier integrity
• Do these markers (or others) correlate with acute neurologic outcomes, long-term neurologic and neurocognitive outcomes?
27
(This is a black box)
We do know some predictors of treatment outcome: Stage at presentation, HIV infection
28
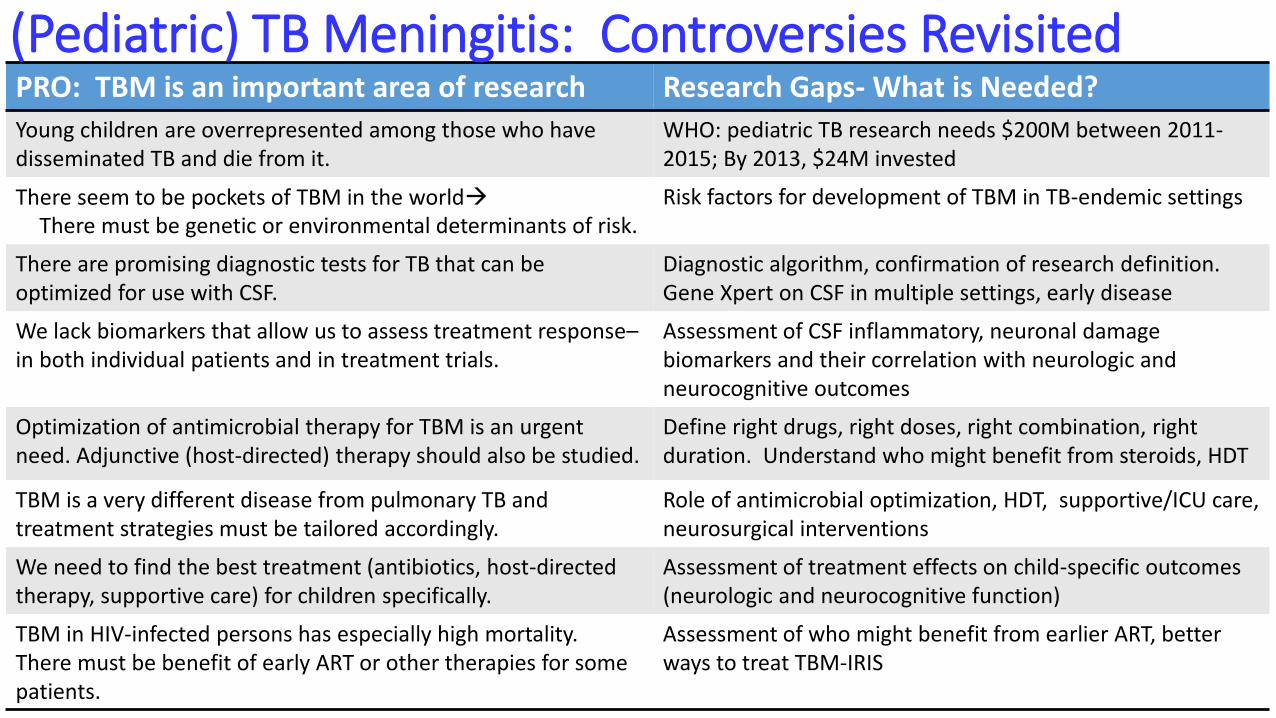
PRO: TBM is an important area of research Research Gaps- What is Needed?
Young children are overrepresented among those who have disseminated TB and die from it.
WHO: pediatric TB research needs $200M between 2011-2015; By 2013, $24M invested
There seem to be pockets of TBM in the worldThere must be genetic or environmental determinants of risk.
Risk factors for development of TBM in TB-endemic settings
There are promising diagnostic tests for TB that can be optimized for use with CSF.
Diagnostic algorithm, confirmation of research definition. Gene Xpert on CSF in multiple settings, early disease
We lack biomarkers that allow us to assess treatment response–in both individual patients and in treatment trials.
Assessment of CSF inflammatory, neuronal damage biomarkers and their correlation with neurologic and neurocognitive outcomes
Optimization of antimicrobial therapy for TBM is an urgent need. Adjunctive (host-directed) therapy should also be studied.
Define right drugs, right doses, right combination, right duration. Understand who might benefit from steroids, HDT
TBM is a very different disease from pulmonary TB and treatment strategies must be tailored accordingly.
Role of antimicrobial optimization, HDT, supportive/ICU care, neurosurgical interventions
We need to find the best treatment (antibiotics, host-directed therapy, supportive care) for children specifically.
Assessment of treatment effects on child-specific outcomes (neurologic and neurocognitive function)
TBM in HIV-infected persons has especially high mortality. There must be benefit of early ART or other therapies for some patients.
Assessment of who might benefit from earlier ART, better ways to treat TBM-IRIS
(Pediatric) TB Meningitis: Controversies Revisited
Optimizing Treatment to Improve TBM Outcomes in Children: The TBM-KIDS Trial
A Phase I/II Randomized, Open-label Trial to Evaluate the Pharmacokinetics, Safety, and Treatment Outcomes of High Dose Rifampicin with or without
Levofloxacin versus Standard Treatment for Pediatric Tuberculosis Meningitis
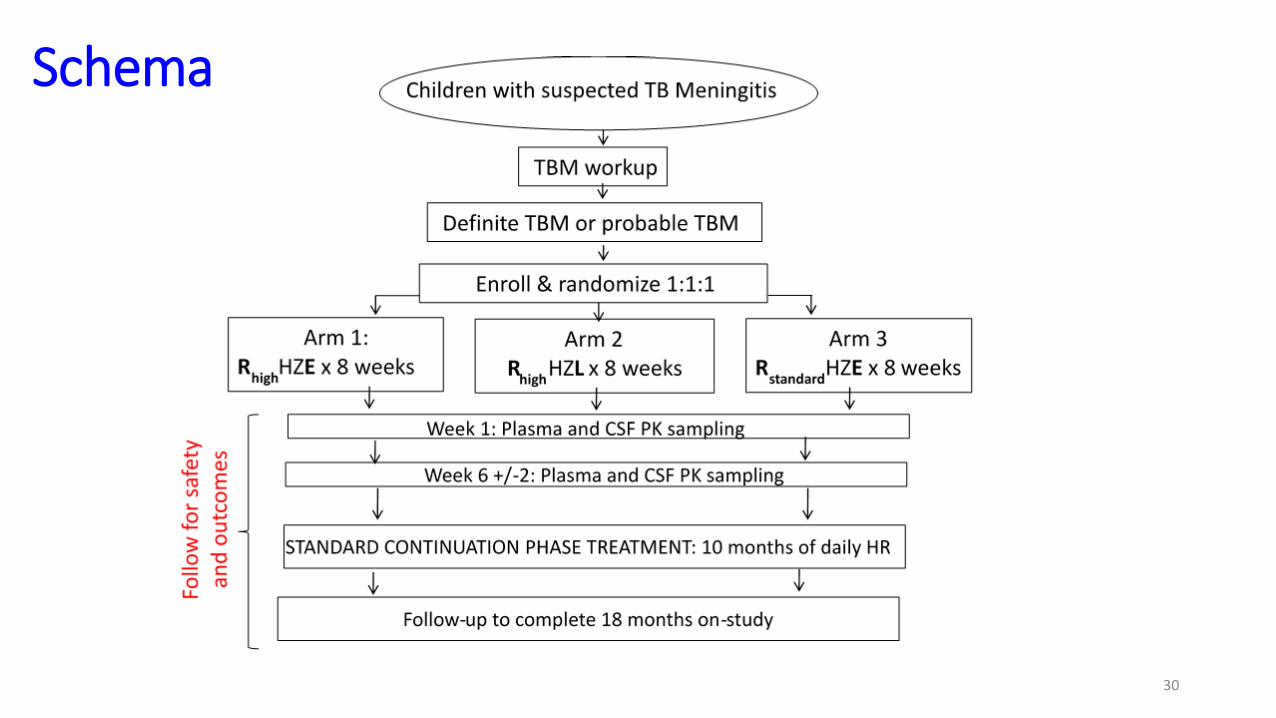
Schema
30

Measuring functional outcomes: Modified Rankin Scale for children
31

32
Measuring neurocognitive outcomes: Mullen Scales of Early Learning
Challenges:• “Cultural fairness”• Language• Validation• Very ill children• Training• Age range

NIRT/Chennai
Soumya Swaminathan-site PI, co-PI
Geetha Ramachandran-PK
Syed Hissar, Bella Devaleenal
S. Ezhilarasi --Institute for Child Health
BJMC/Pune
Aarti Kinikar-site PI
Nikhil Gupte-statistician
Vidya Mave, Nishi Suryavanshi, Smita Nimkar
Malawi
Blantyre: Geraint Davies, Carmen Gonzalez,
Macpherson Mallewa
Lilongwe: Mina Hosseinipour, Irwin Hoffman
IMPAACT Network
JHU
Kiran Thakur-neurologist
Ana Arenivas (KKI)-neuropsychologist
Lisa Wolf: Global study coordinator
Amita Gupta
UCSF
Rada Savic, pharmacometrician
UCT
Lubbe Wiesner
NICHD
Rohan Hazra
(Carol Worrell & Lynne Mofenson)
1R01HD0774944-01A1
33
Collaborative Team: TBM-KIDS
**Not a comprehensive list of important contributors
Thank you.
34WHO. Roadmap for Childhood Tuberculosis: Towards Zero Deaths

















