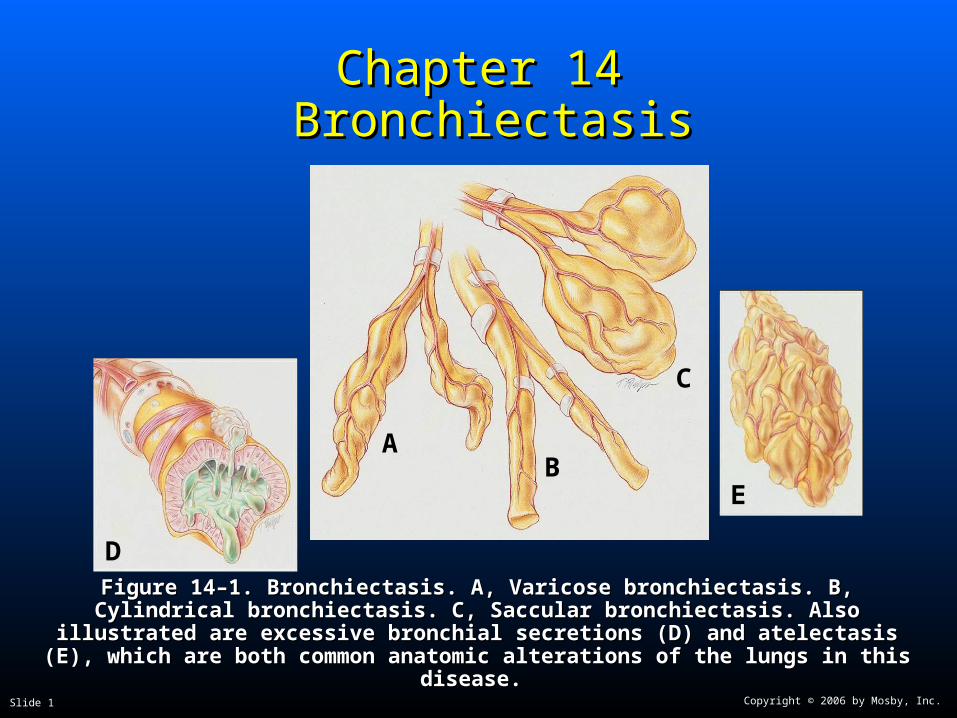
Figure 14–1. Bronchiectasis. A, Varicose bronchiectasis. B, Cylindrical bronchiectasis. C, Figure 14–1. Bronchiectasis. A, Varicose bronchiectasis. B, Cylindrical bronchiectasis. C, Saccular bronchiectasis. Also illustrated are excessive bronchial secretions (D) and Saccular bronchiectasis. Also illustrated are excessive bronchial secretions (D) and
atelectasis (E), which are both common anatomic alterations of the lungs in this disease.atelectasis (E), which are both common anatomic alterations of the lungs in this disease.
Overview of the Cardiopulmonary Overview of the Cardiopulmonary Clinical Manifestations Associated Clinical Manifestations Associated
with BRONCHIECTASISwith BRONCHIECTASIS
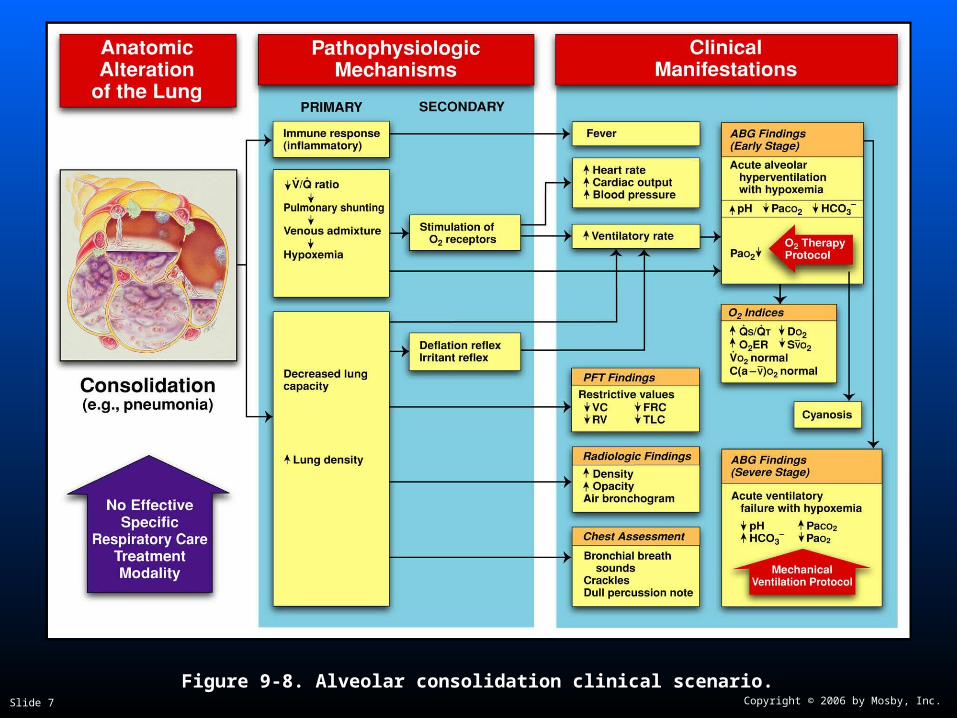
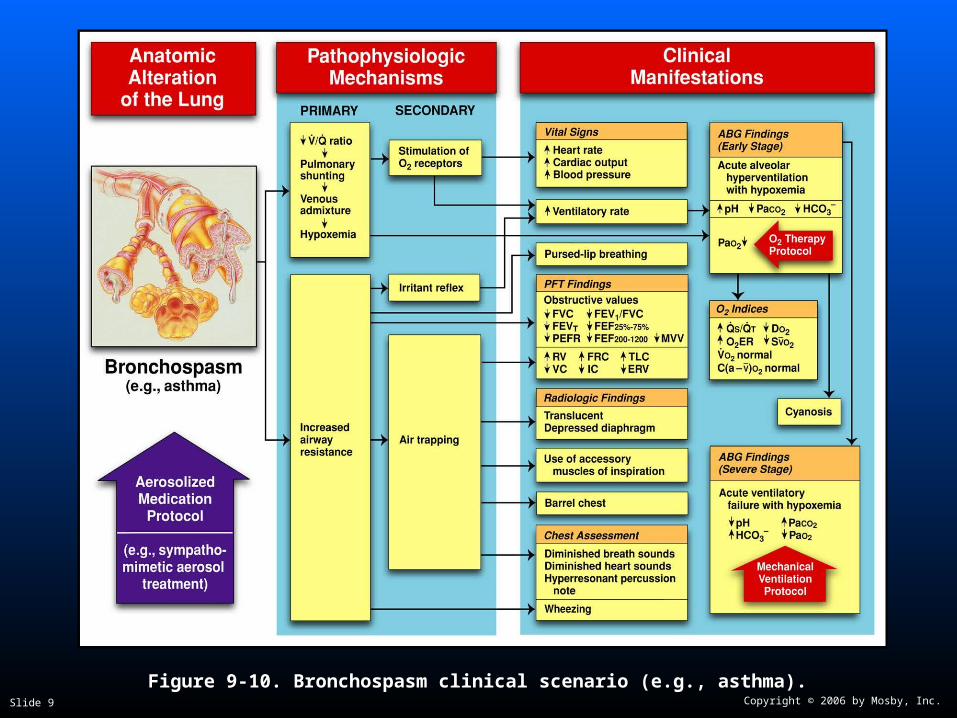
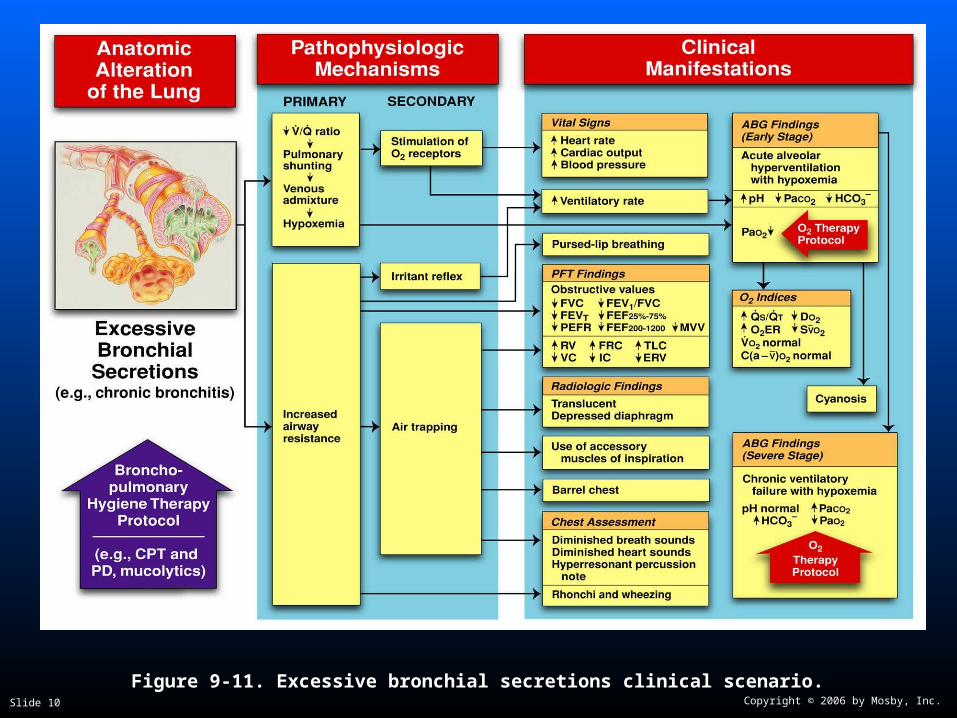
The following clinical manifestations result from the The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) pathophysiologic mechanisms caused (or activated) by by AtelectasisAtelectasis (see Figure 9-12), (see Figure 9-12), Consolidation Consolidation (see Figure 9-8), (see Figure 9-8), Bronchospasm Bronchospasm (see Figure 9-10), (see Figure 9-10), and and Excessive BronchialExcessive Bronchial Secretions Secretions (see Figure (see Figure 9-11)—the major anatomic alterations of the lungs 9-11)—the major anatomic alterations of the lungs associated with bronchiectasis (see Figure 14-1).associated with bronchiectasis (see Figure 14-1).
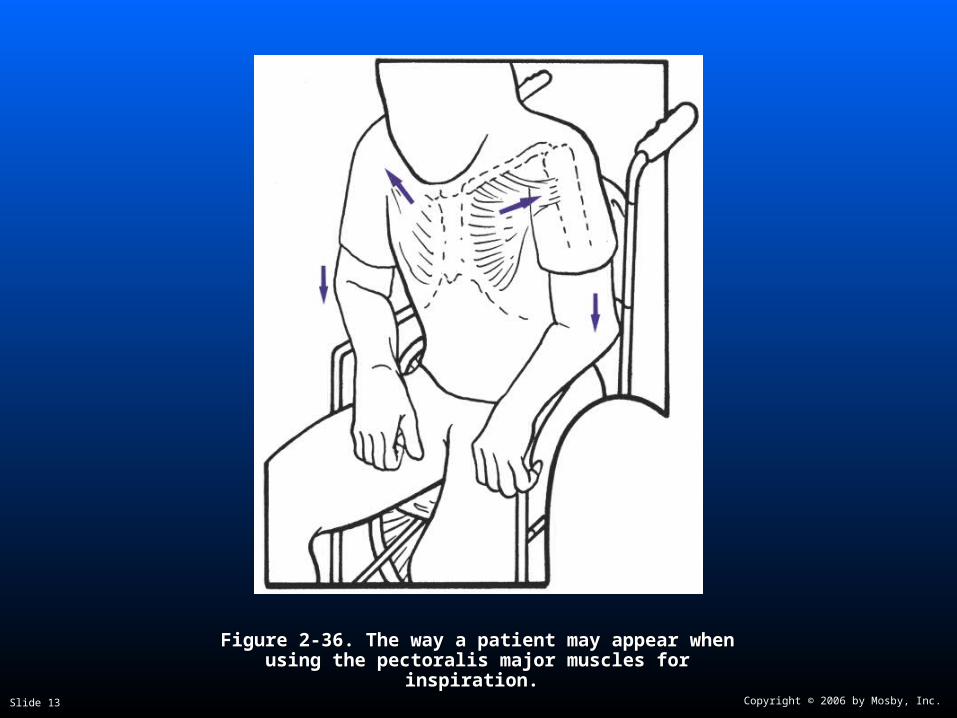
Figure 2-36. Figure 2-36. The way a patient may appear when using the The way a patient may appear when using the pectoralis major muscles for inspiration.pectoralis major muscles for inspiration.
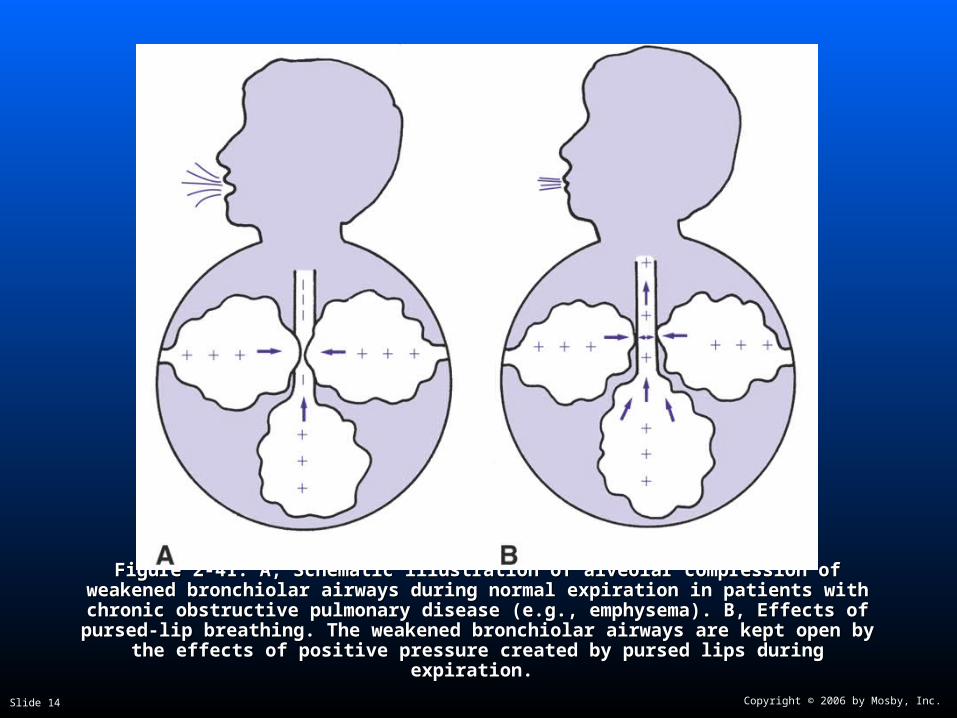
Figure 2-41. Figure 2-41. A, Schematic illustration of alveolar compression of weakened bronchiolar A, Schematic illustration of alveolar compression of weakened bronchiolar airways during normal expiration in patients with chronic obstructive pulmonary disease airways during normal expiration in patients with chronic obstructive pulmonary disease (e.g., emphysema). B, Effects of pursed-lip breathing. The weakened bronchiolar airways (e.g., emphysema). B, Effects of pursed-lip breathing. The weakened bronchiolar airways
are kept open by the effects of positive pressure created by pursed lips during expiration.are kept open by the effects of positive pressure created by pursed lips during expiration.
Figure 2-47. Pitting edema. From Bloom A, Ireland J: Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetesColor atlas of diabetes, ed 2,, ed 2,London, 1992, Mosby-Wolfe.London, 1992, Mosby-Wolfe.
Cough, sputum production, and hemoptysisCough, sputum production, and hemoptysis A chronic cough with production of large quantities A chronic cough with production of large quantities
of foul-smelling sputum is a hallmark of of foul-smelling sputum is a hallmark of bronchiectasisbronchiectasis
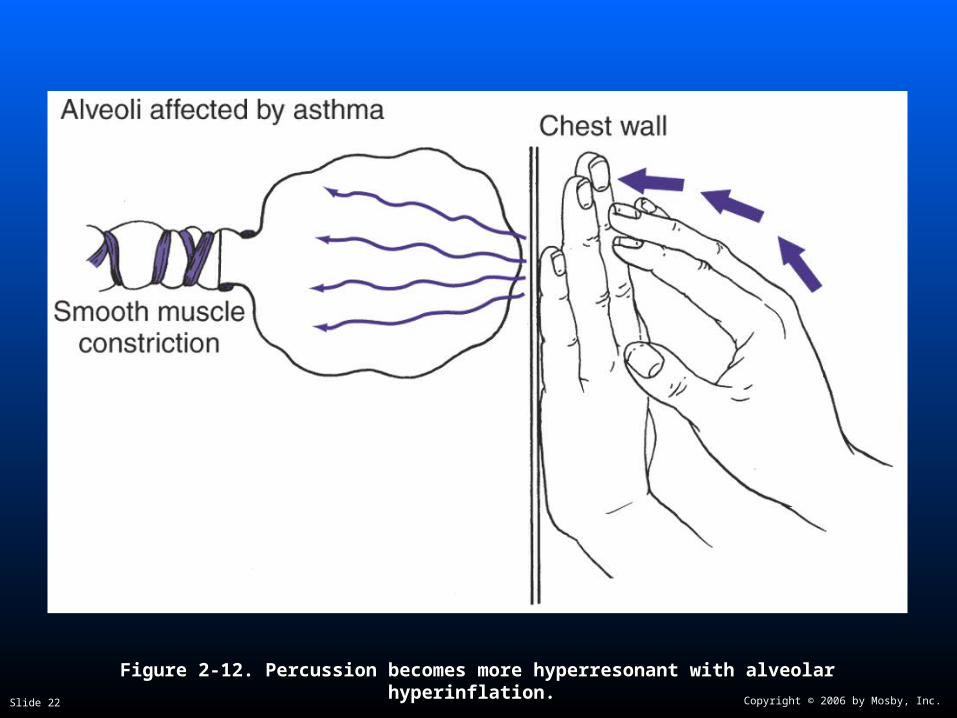
Figure 2-12. Figure 2-12. Percussion becomes more hyperresonant with alveolar hyperinflation.Percussion becomes more hyperresonant with alveolar hyperinflation.
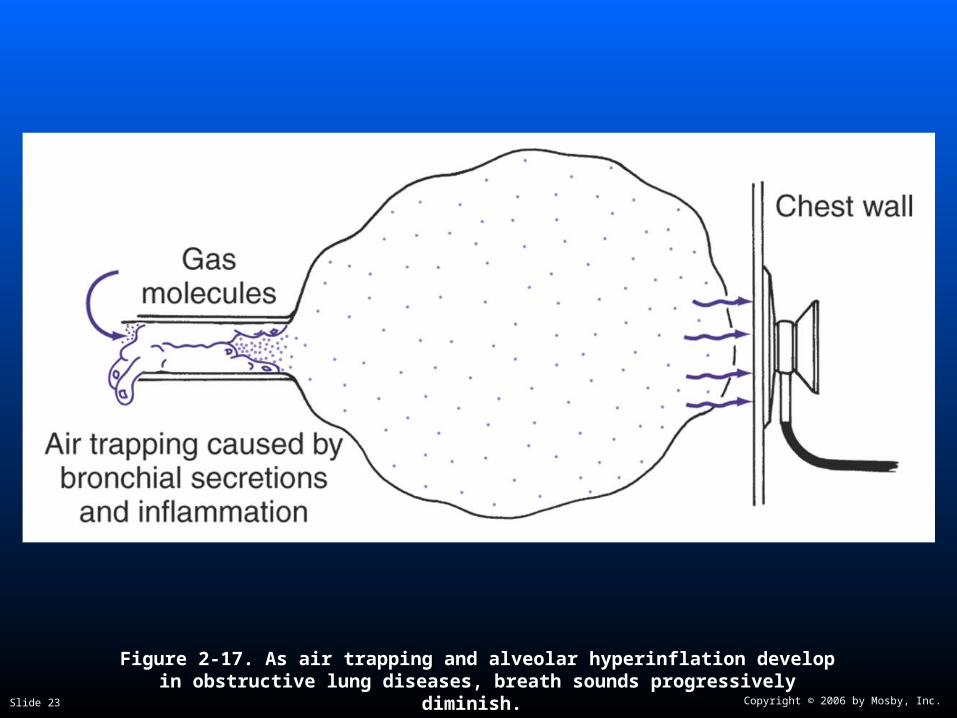
Figure 2-17. Figure 2-17. As air trapping and alveolar hyperinflation develop in obstructive As air trapping and alveolar hyperinflation develop in obstructive lung diseases, breath sounds progressively diminish.lung diseases, breath sounds progressively diminish.
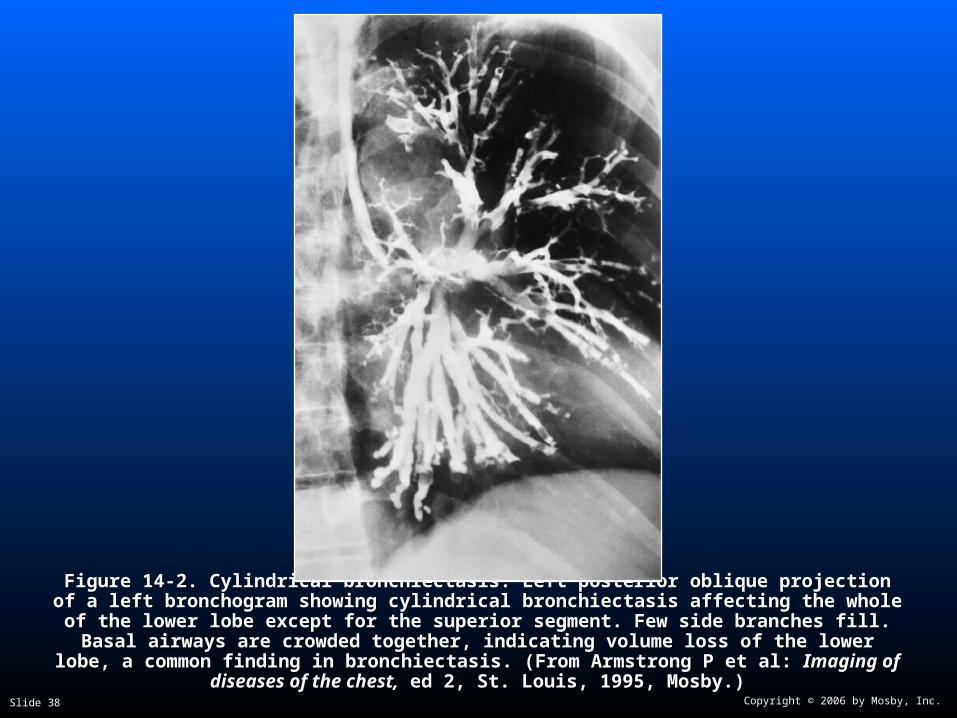
Figure 14-2. Figure 14-2. Cylindrical bronchiectasis. Left posterior oblique projection of a left bronchogram Cylindrical bronchiectasis. Left posterior oblique projection of a left bronchogram showing cylindrical bronchiectasis affecting the whole of the lower lobe except for the superior showing cylindrical bronchiectasis affecting the whole of the lower lobe except for the superior segment. Few side branches fill. Basal airways are crowded together, indicating volume loss of segment. Few side branches fill. Basal airways are crowded together, indicating volume loss of
the lower lobe, a common finding in bronchiectasis. (From Armstrong P et al: the lower lobe, a common finding in bronchiectasis. (From Armstrong P et al: Imaging of Imaging of diseases of the chest,diseases of the chest, ed 2, St. Louis, 1995, Mosby.) ed 2, St. Louis, 1995, Mosby.)
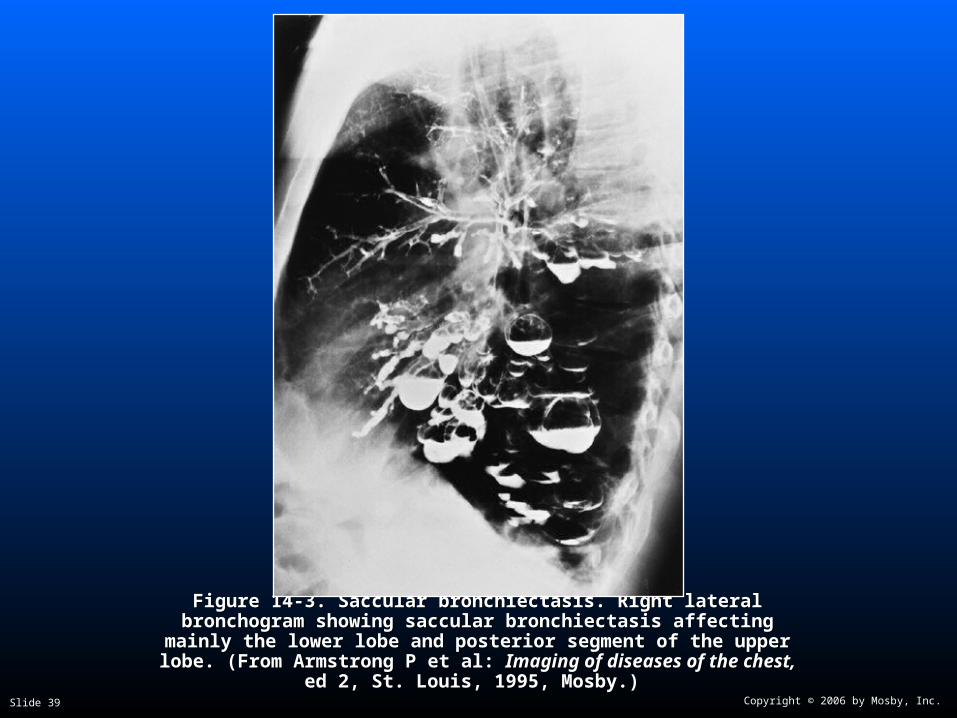
Figure 14-3. Figure 14-3. Saccular bronchiectasis. Right lateral bronchogram showing Saccular bronchiectasis. Right lateral bronchogram showing saccular bronchiectasis affecting mainly the lower lobe and posterior saccular bronchiectasis affecting mainly the lower lobe and posterior
segment of the upper lobe. (From Armstrong P et al: segment of the upper lobe. (From Armstrong P et al: Imaging of diseases Imaging of diseases of the chest,of the chest, ed 2, St. Louis, 1995, Mosby.) ed 2, St. Louis, 1995, Mosby.)
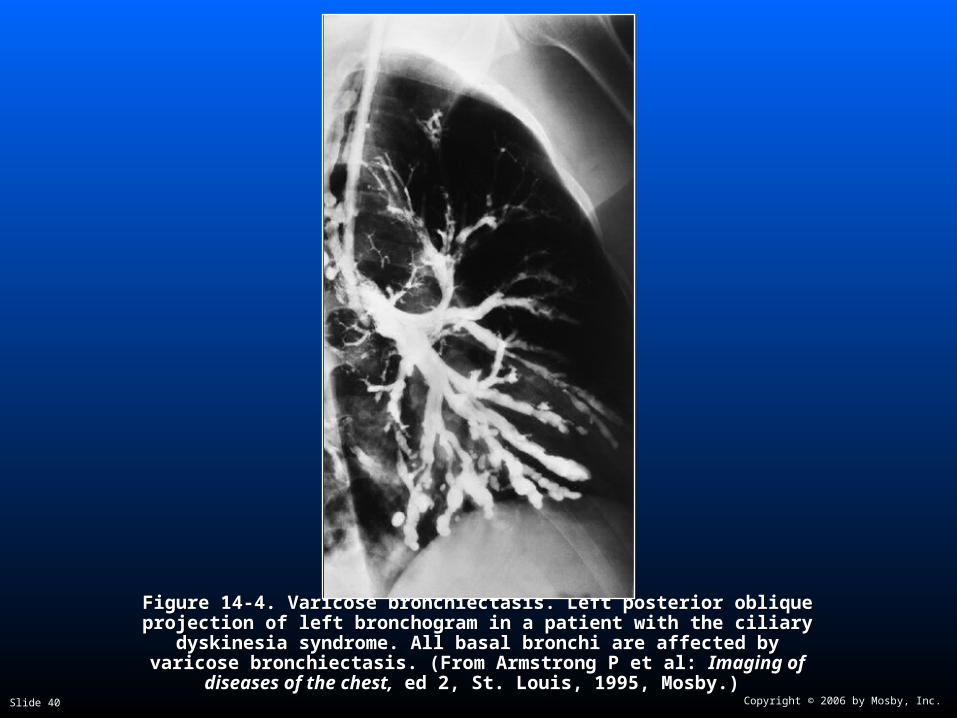
Figure 14-4. Figure 14-4. Varicose bronchiectasis. Left posterior oblique projection of left Varicose bronchiectasis. Left posterior oblique projection of left bronchogram in a patient with the ciliary dyskinesia syndrome. All basal bronchogram in a patient with the ciliary dyskinesia syndrome. All basal
bronchi are affected by varicose bronchiectasis. (From Armstrong P et al: bronchi are affected by varicose bronchiectasis. (From Armstrong P et al: Imaging of diseases of the chest,Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.) ed 2, St. Louis, 1995, Mosby.)
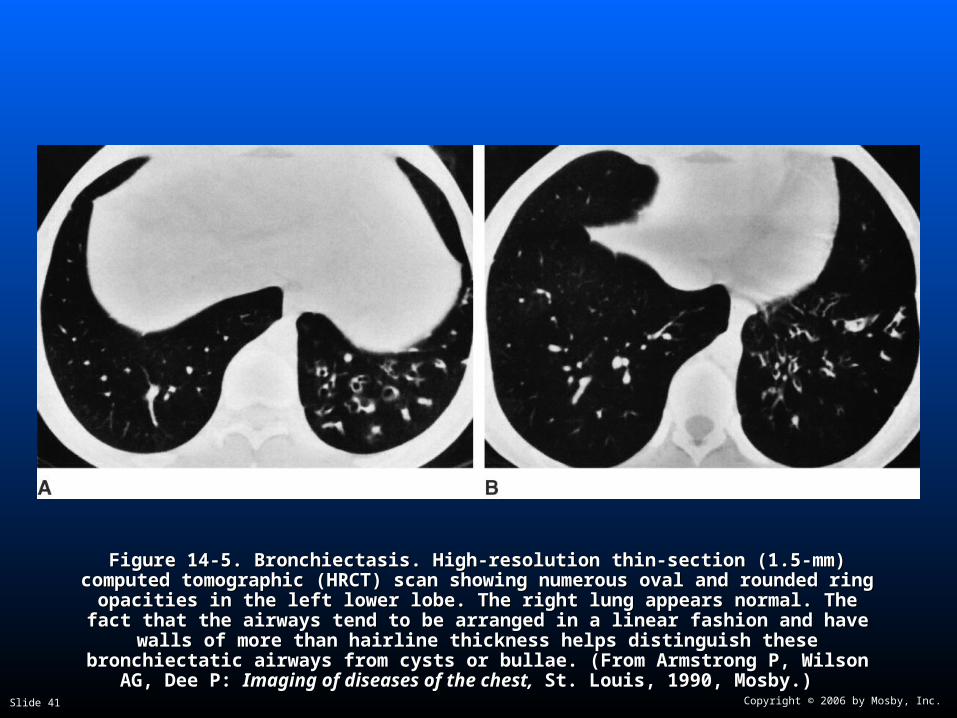
Figure 14-5. Figure 14-5. Bronchiectasis. High-resolution thin-section (1.5-mm) computed tomographic Bronchiectasis. High-resolution thin-section (1.5-mm) computed tomographic (HRCT) scan showing numerous oval and rounded ring opacities in the left lower lobe. (HRCT) scan showing numerous oval and rounded ring opacities in the left lower lobe. The right lung appears normal. The fact that the airways tend to be arranged in a linear The right lung appears normal. The fact that the airways tend to be arranged in a linear
fashion and have walls of more than hairline thickness helps distinguish these fashion and have walls of more than hairline thickness helps distinguish these bronchiectatic airways from cysts or bullae. (From Armstrong P, Wilson AG, Dee P: bronchiectatic airways from cysts or bullae. (From Armstrong P, Wilson AG, Dee P:
Imaging of diseases of the chest,Imaging of diseases of the chest, St. Louis, 1990, Mosby.) St. Louis, 1990, Mosby.)