40
Copyright © 2006 by Mosby, Inc. Slide 1 PART VII PART VII Environmental Lung Diseases Environmental Lung Diseases
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | teresa-thornton |
| View: | 213 times |
| Download: | 0 times |

Copyright © 2006 by Mosby, Inc.Slide 1
PART VIIPART VII
Environmental Lung DiseasesEnvironmental Lung Diseases

Copyright © 2006 by Mosby, Inc.Slide 2
Chapter 25Chapter 25Pneumoconiosis Pneumoconiosis
Figure 25-1. Pneumoconiosis, illustrated here in a case of asbestosis (close-up of one alveolar Figure 25-1. Pneumoconiosis, illustrated here in a case of asbestosis (close-up of one alveolar unit). unit). AF,AF, Asbestos fiber; Asbestos fiber; FIB,FIB, fibrosis; fibrosis; MM, macrophage. , macrophage. Inset,Inset, Cross-section showing fibrotic Cross-section showing fibrotic
thickening of the alveolus, a common secondary anatomic alteration of the lungs. thickening of the alveolus, a common secondary anatomic alteration of the lungs.
Copyright © 2006 by Mosby, Inc.Slide 3
Anatomic Alterations of the LungsAnatomic Alterations of the Lungs
Destruction of the alveoli and adjacent pulmonary Destruction of the alveoli and adjacent pulmonary capillariescapillaries
Fibrotic thickening of the respiratory bronchioles, Fibrotic thickening of the respiratory bronchioles, alveolar ducts, and alveolialveolar ducts, and alveoli
Cystlike structures (honeycomb appearance)Cystlike structures (honeycomb appearance) Fibrocalcific pleural plaques (e.g., asbestosis)Fibrocalcific pleural plaques (e.g., asbestosis) Airway obstruction caused by inflammation and Airway obstruction caused by inflammation and
excessive bronchial secretionsexcessive bronchial secretions BronchospasmBronchospasm Bronchogenic carcinomaBronchogenic carcinoma Mesothelioma (in asbestosis)Mesothelioma (in asbestosis)

Copyright © 2006 by Mosby, Inc.Slide 4
EtiologyEtiology
Etiologic DeterminantsEtiologic Determinants
Size of inhaled particleSize of inhaled particle 0.3 and 0.5 0.3 and 0.5 μμm reach the alveolim reach the alveoli
Chemical nature of the particleChemical nature of the particle
Concentration of the particleConcentration of the particle
Length of exposureLength of exposure
The individual’s susceptibilityThe individual’s susceptibility

Copyright © 2006 by Mosby, Inc.Slide 5
EtiologyEtiologyAsbestosisAsbestosis
Acoustic productsAcoustic products
Automobile Automobile undercoatingundercoating
Brake liningBrake lining
CementsCements
Clutch casingsClutch casings
Floor tilesFloor tiles
Fire-fighting suitsFire-fighting suits
Fireproof paintsFireproof paints
InsulationInsulation
Roofing materialsRoofing materials
Ropes Ropes
Steam pipe materialSteam pipe material

Copyright © 2006 by Mosby, Inc.Slide 6
EtiologyEtiologyCoal Worker’s PneumoconiosisCoal Worker’s Pneumoconiosis
The deposition and accumulation of large The deposition and accumulation of large amounts of coal dust cause what is know as amounts of coal dust cause what is know as coal worker’s pneumoconiosis (CWP)coal worker’s pneumoconiosis (CWP)
Also called:Also called: Coal miner’s lungCoal miner’s lung
Black lungBlack lung
Black phthisisBlack phthisis
Miner’s phthisisMiner’s phthisis

Copyright © 2006 by Mosby, Inc.Slide 7
EtiologyEtiologySilicosisSilicosis
Tunneling Tunneling
Hard-rock miningHard-rock mining
SandblastingSandblasting
Quarrying Quarrying
StonecuttingStonecutting
Foundry workFoundry work
Ceramics workCeramics work
Abrasive workAbrasive work
Brick makingBrick making
Paint makingPaint making
PolishingPolishing
Stone drillingStone drilling
Well drillingWell drilling

Copyright © 2006 by Mosby, Inc.Slide 8
EtiologyEtiologyBerylliosisBerylliosis
Beryllium is a steel-gray, lightweight Beryllium is a steel-gray, lightweight metal found in: metal found in: Certain plastics and ceramicsCertain plastics and ceramics
Rocket fuelsRocket fuels
X-rayX-ray

Copyright © 2006 by Mosby, Inc.Slide 9
EtiologyEtiologyOther Forms of PneumoconiosisOther Forms of Pneumoconiosis
AluminumAluminum Ammunition workersAmmunition workers
Baritosis (barium)Baritosis (barium) Barite millers and minersBarite millers and miners Ceramics workersCeramics workers
Kaolinosis (clay)Kaolinosis (clay) Brick makers and pottersBrick makers and potters Ceramics workersCeramics workers
Siderosis (iron)Siderosis (iron) Welders Welders
Talcosis (certain talcs)Talcosis (certain talcs) Ceramics workersCeramics workers Plastic and rubber workersPlastic and rubber workers

Copyright © 2006 by Mosby, Inc.Slide 10
Overview of the Cardiopulmonary Overview of the Cardiopulmonary Clinical Manifestations Associated Clinical Manifestations Associated
with PNEUMOCONIOSISwith PNEUMOCONIOSIS
The following clinical manifestations result from The following clinical manifestations result from the pathophysiologic mechanisms caused (or the pathophysiologic mechanisms caused (or activated) by activated) by Increased Alveolar-CapillaryIncreased Alveolar-Capillary membrane (see Figure 9-9), membrane (see Figure 9-9), BronchospasmBronchospasm (see Figure 9-10), and (see Figure 9-10), and Excessive Bronchial Excessive Bronchial SecretionsSecretions (see Figure 9-11)—the major (see Figure 9-11)—the major anatomic alterations of the lungs associated anatomic alterations of the lungs associated with chronic bronchitis (see Figure 25-1).with chronic bronchitis (see Figure 25-1).

Copyright © 2006 by Mosby, Inc.Slide 11
Figure 9-9. Increased alveolar-capillary membrane thickness clinical scenario.Figure 9-9. Increased alveolar-capillary membrane thickness clinical scenario.

Copyright © 2006 by Mosby, Inc.Slide 12
Figure 9-10. Bronchospasm clinical scenario (e.g., asthma). Figure 9-10. Bronchospasm clinical scenario (e.g., asthma).

Copyright © 2006 by Mosby, Inc.Slide 13
Figure 9-11. Excessive bronchial secretions clinical scenario. Figure 9-11. Excessive bronchial secretions clinical scenario.
Copyright © 2006 by Mosby, Inc.Slide 14
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Vital signsVital signs
Increased respiratory rateIncreased respiratory rate
Increased heart rate, cardiac output, Increased heart rate, cardiac output, blood pressureblood pressure

Copyright © 2006 by Mosby, Inc.Slide 15
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
CyanosisCyanosis
Digital clubbingDigital clubbing
Peripheral edema and venous distentionPeripheral edema and venous distention Distended neck veinsDistended neck veins
Pitting edemaPitting edema
Enlarged and tender liverEnlarged and tender liver
Cough and sputum productionCough and sputum production

Copyright © 2006 by Mosby, Inc.Slide 16
Digital Clubbing
Figure 2-46. Digital clubbing.Figure 2-46. Digital clubbing.

Copyright © 2006 by Mosby, Inc.Slide 17
DistendedDistendedNeck VeinsNeck Veins
Figure 2-48. Distended neck veins (Figure 2-48. Distended neck veins (arrowsarrows).).

Copyright © 2006 by Mosby, Inc.Slide 18
Figure 2-47. Pitting edema. From Bloom A, Ireland J: Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetesColor atlas of diabetes, ed 2,, ed 2,London, 1992, Mosby-Wolfe.London, 1992, Mosby-Wolfe.

Copyright © 2006 by Mosby, Inc.Slide 19
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Chest assessment findingsChest assessment findings Increased tactile and vocal fremitusIncreased tactile and vocal fremitus
Dull percussion noteDull percussion note
Bronchial breath soundsBronchial breath sounds
Crackles, rhonchi, and wheezingCrackles, rhonchi, and wheezing
Pleural friction rubPleural friction rub
Whispered pectoriloquyWhispered pectoriloquy

Copyright © 2006 by Mosby, Inc.Slide 20
Figure 2-11. Figure 2-11. A short, dull, or flat percussion note is typically produced over areas A short, dull, or flat percussion note is typically produced over areas of alveolar consolidation.of alveolar consolidation.

Copyright © 2006 by Mosby, Inc.Slide 21
Figure 2-16. Figure 2-16. Auscultation of bronchial breath sounds over a consolidated lung Auscultation of bronchial breath sounds over a consolidated lung unit.unit.
Copyright © 2006 by Mosby, Inc.Slide 22
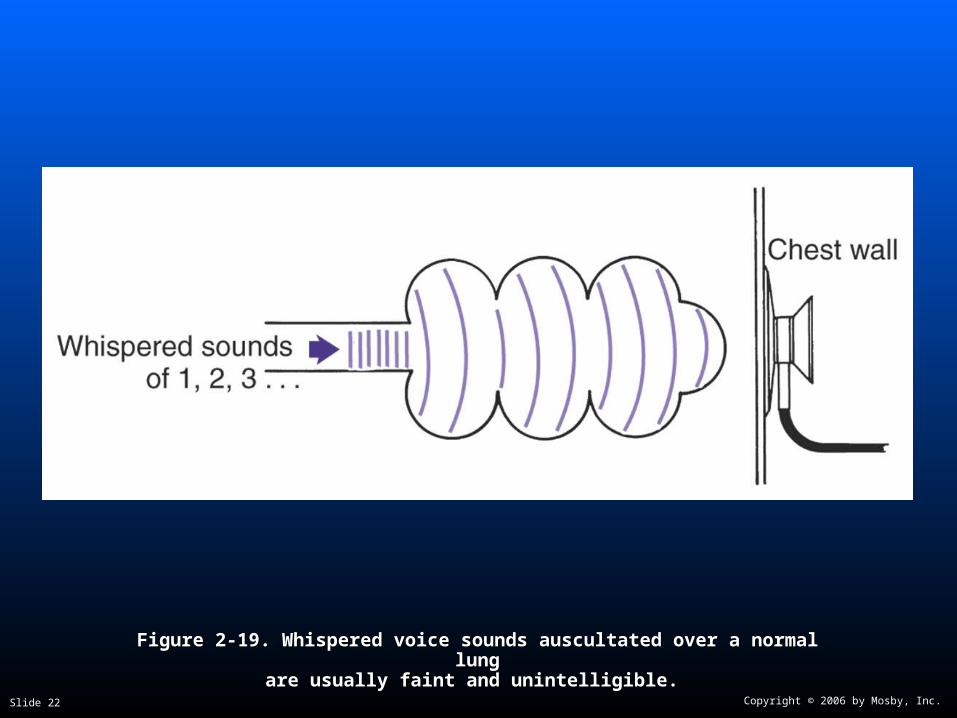
Figure 2-19. Figure 2-19. Whispered voice sounds auscultated over a normal lungWhispered voice sounds auscultated over a normal lungare usually faint and unintelligible.are usually faint and unintelligible.

Copyright © 2006 by Mosby, Inc.Slide 23
Clinical Data Obtained from Clinical Data Obtained from Laboratory Tests and Special Laboratory Tests and Special
ProceduresProcedures

Copyright © 2006 by Mosby, Inc.Slide 24
Pulmonary Function Study: Pulmonary Function Study: Expiratory Maneuver FindingsExpiratory Maneuver Findings
FVC FEVT FEF25%-75% FEF200-1200
PEFR MVV FEF50% FEV1%
N
FVC FEVT FEF25%-75% FEF200-1200
PEFR MVV FEF50% FEV1%
N

Copyright © 2006 by Mosby, Inc.Slide 25
Pulmonary Function Study: Pulmonary Function Study: Lung Volume and Capacity Findings Lung Volume and Capacity Findings
VT RV FRC TLC
VC IC ERV RV/TLC%
N or
VT RV FRC TLC
VC IC ERV RV/TLC%
N or

Copyright © 2006 by Mosby, Inc.Slide 26
Decreased Diffusion Capacity Decreased Diffusion Capacity (DL(DLCOCO))

Copyright © 2006 by Mosby, Inc.Slide 27
Arterial Blood GasesArterial Blood Gases
Mild to Moderate PneumoconiosisMild to Moderate Pneumoconiosis
Acute alveolar hyperventilation with Acute alveolar hyperventilation with hypoxemiahypoxemia
pH PaCO2 HCO3- PaO2
(Slightly)
pH PaCO2 HCO3- PaO2
(Slightly)

Copyright © 2006 by Mosby, Inc.Slide 28
Time and Progression of Disease Time and Progression of Disease
100100
5050
3030
8080
00
PaCO2
1010
2020
4040
Alveolar HyperventilationAlveolar Hyperventilation
6060
7070
9090 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
PaO2
Disease OnsetDisease OnsetP
aO2
or
PaC
O2
PaO
2 o
r P
aCO
2
Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation.

Copyright © 2006 by Mosby, Inc.Slide 29
Arterial Blood GasesArterial Blood Gases
Severe Pneumoconiosis with ExtensiveSevere Pneumoconiosis with ExtensiveFibrosisFibrosis
Chronic ventilatory failure with hypoxemiaChronic ventilatory failure with hypoxemia
pH PaCO2 HCO3- PaO2
Normal (Significantly)
pH PaCO2 HCO3- PaO2
Normal (Significantly)

Copyright © 2006 by Mosby, Inc.Slide 30
Time and Progression of DiseaseTime and Progression of Disease
100100
5050
3030
80
0
PaO2
1010
2020
4040
Alveolar HyperventilationAlveolar Hyperventilation
6060
7070
9090Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
Point at which PaO2 declines enough to stimulate peripheral oxygen receptors
PaCO 2
Chronic Ventilatory Failure Chronic Ventilatory FailureDisease OnsetDisease Onset
Point at which disease becomes severe and patient begins to become fatigued
Point at which disease becomes severe and patient begins to become fatigued
Pa0
2 o
r P
aC0 2
Pa0
2 o
r P
aC0 2
Figure 4-7. PaO2 and PaCO2 trends during acute or chronic ventilatory failure.

Copyright © 2006 by Mosby, Inc.Slide 31
Acute Ventilatory Changes Superimposed Acute Ventilatory Changes Superimposed on Chronic Ventilatory Failureon Chronic Ventilatory Failure
Acute alveolar hyperventilation on chronic Acute alveolar hyperventilation on chronic ventilatory failureventilatory failure
Acute ventilatory failure on chronic Acute ventilatory failure on chronic ventilatory failure ventilatory failure

Copyright © 2006 by Mosby, Inc.Slide 32
Oxygenation IndicesOxygenation Indices
QS/QT DO2 VO2 C(a-v)O2
Normal Normal
O2ER SvO2
QS/QT DO2 VO2 C(a-v)O2
Normal Normal
O2ER SvO2
Copyright © 2006 by Mosby, Inc.Slide 33
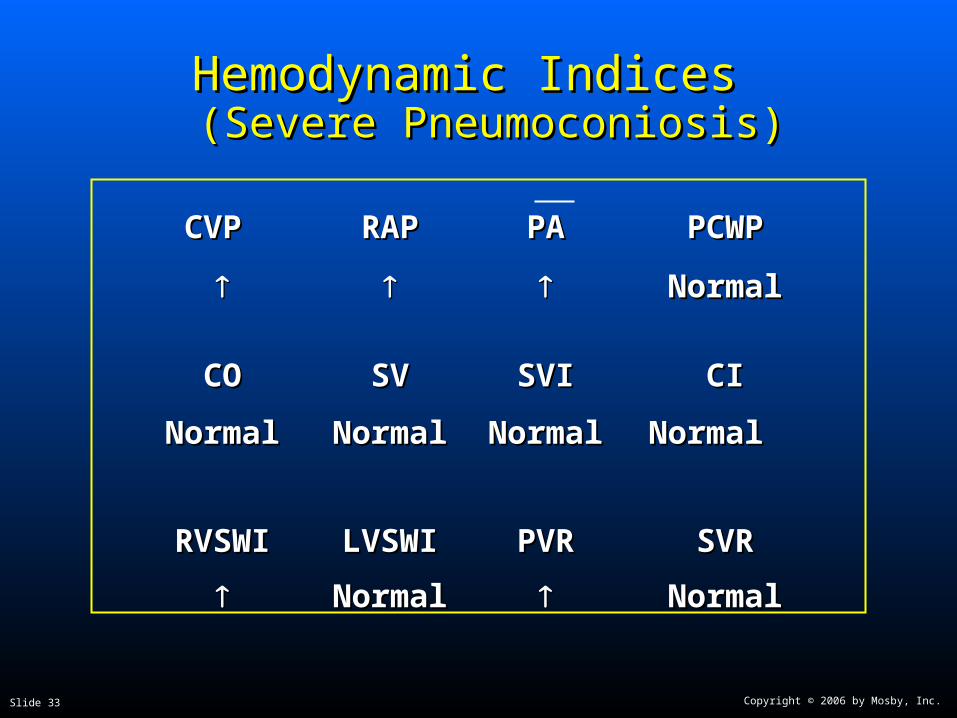
Hemodynamic Indices Hemodynamic Indices (Severe Pneumoconiosis) (Severe Pneumoconiosis)
CVP CVP RAPRAP PAPA PCWPPCWP
NormalNormal
COCO SVSV SVISVI CICI
NormalNormal NormalNormal NormalNormal Normal Normal
RVSWIRVSWI LVSWILVSWI PVRPVR SVRSVR
NormalNormal NormalNormal

Copyright © 2006 by Mosby, Inc.Slide 34
Laboratory FindingsLaboratory Findings
Complete blood count (CBC)Complete blood count (CBC) Elevated hemoglobin concentration and Elevated hemoglobin concentration and
hematocrit if the patient is chronically hypoxemichematocrit if the patient is chronically hypoxemic

Copyright © 2006 by Mosby, Inc.Slide 35
Radiologic FindingsRadiologic Findings
Chest radiographChest radiograph
Small rounded opacities scattered throughout Small rounded opacities scattered throughout the lungthe lung
Irregularly shaped opacitiesIrregularly shaped opacities
Irregular cardiac and diaphragmatic bordersIrregular cardiac and diaphragmatic borders
Pleural plaquesPleural plaques
Honeycomb appearanceHoneycomb appearance

Copyright © 2006 by Mosby, Inc.Slide 36
Figure 25-2. Figure 25-2. Chest X-ray of a patient with asbestosisChest X-ray of a patient with asbestosis..

Copyright © 2006 by Mosby, Inc.Slide 37
Figure 25-3, Figure 25-3, Calcified pleural plaques on the superior border of the Calcified pleural plaques on the superior border of the diaphragm (arrows) in a patient with asbestosis. Thickening of the diaphragm (arrows) in a patient with asbestosis. Thickening of the pleural margins also is seen along the lower lateral borders of the pleural margins also is seen along the lower lateral borders of the
chest. A, Anteroposterior view. B, Lateral viewchest. A, Anteroposterior view. B, Lateral view..
Copyright © 2006 by Mosby, Inc.Slide 38
General Management of General Management of PneumoconiosisPneumoconiosis
Control of occupational diseases is the Control of occupational diseases is the responsibility of the:responsibility of the: Worker Worker
Management Management
Community health departmentCommunity health department
State and federal governmentsState and federal governments
Prevention is the keyPrevention is the key
After the disease is established, it has no After the disease is established, it has no effective cureeffective cure

Copyright © 2006 by Mosby, Inc.Slide 39
General Management of General Management of PneumoconiosisPneumoconiosis
Respiratory care treatment protocolsRespiratory care treatment protocols Oxygen therapy protocolOxygen therapy protocol
Bronchopulmonary hygiene therapy protocolBronchopulmonary hygiene therapy protocol
Aerosolized medication protocolAerosolized medication protocol
Hyperinflation therapy protocolHyperinflation therapy protocol

Copyright © 2006 by Mosby, Inc.Slide 40
Classroom DiscussionClassroom DiscussionCase Study: PneumoconiosisCase Study: Pneumoconiosis

















