Page 1
Copyright © 2013, Canadian Cardiovascular Society23-04-21 1
Anderson TJ, Gregoire J et al., Can J Cardiol 2013 Feb;29(2): 151-167
Disclaimer
The Canadian Cardiovascular Society (CCS) welcomes reuse of our educational slide deck for medical institution internal education or training (i.e. grand rounds, medical college/classroom education, etc.). However, if the material is being used in an industry sponsored CME program, permission must be sought through our publisher Elsevier (www.onlinecjc.com). If your reuse request qualifies as medical institution internal education, you may reuse the material under the following conditions:
• You must cite the Canadian Journal of Cardiology and the Canadian Cardiovascular Society as references.
• You may not use any Canadian Cardiovascular Society logos or trademarks on any slides or anywhere in your presentation or publications.• Do not modify the slide content.• If repeating recommendations from the published guideline, do not modify the recommendation wording.
Page 2
23-04-21 2Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
CANADIAN CARDIOVASCULAR SOCIETY GUIDELINES ON THE USE OF CARDIAC
RESYNCHRONIZATION THERAPY: EVIDENCE AND PATIENT SELECTION
R Parkash, F Philippon, D Exner, and D Birnieon behalf of the CRT Guidelines Panels.
Page 3
23-04-21 3Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Disclosures
www.ccs.ca
Guidelines are available on line
www.ccsguidelineprograms.ca
Can J Cardiol 2013; 29(2):182-195
Page 4
23-04-21 4Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
CCS CRT Guidelines 2012Secondary Panel•Lyall Higginson•Jonathan Howlett•Aaron Low•Robert McKelvie•John Sapp•Miriam Shanks •Mario Talajic•Michel White•Raymond Yee
Primary Panel•David Birnie•Derek Exner (co-chair)•Jeff Healey•Eric LaRose•Gordon Moe•Ratika Parkash (co-chair)•François Philippon•Anthony Tang•Bernard Thibault
Page 5
23-04-21 5Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Session Overview
• Focus on evidence-based prescription of CRT, based on scientific data
• Review of GRADE process
• Case-based presentation of guidelines
– Eight recommendations
– Practical Tips
Page 6
23-04-21 6Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Objectives
At the end of this session:1. Review the appropriate selection of patients for CRT2. Discuss the role of CRT-pacing3. Describe the risks and benefits related to patients with
AF, RBBB and chronic RV pacing4. Understand technical issues related to CRT including
lead placement5. Discuss the role of imaging in assessment of CRT
Page 7
23-04-21 7Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
GRADE Approach• Development of guidelines through:
– Critical evaluation of literature– Expert consensus– Use of Grading of Recommendations Assessment,
Development, and Evaluation 1. Quality of Evidence:
High, Moderate, Low or Very Low2. Strength of Recommendations
Strong or WeakGuyatt et al. 2011 J Clin Epi 64: 383-94
Page 8
23-04-21 8Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Case 1
• 78 year old woman– sinus rhythm, – dilated cardiomyopathy (NYHA III), &– LVEF 25%– Co-morbidities – DM, PVD, & eGFR 33 ml/min
• Medications:– Carvedilol (6.125 mg BID) & ramipril (1.25 mg OD)
initiated 5 weeks ago (not on spironolactone).
Page 9
23-04-21 9Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Case 1 - ECG
Page 10
23-04-21 10Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation One Strength Quality
Adequate medical therapy be
implemented prior to the
initiation of CRT, that each
patient’s suitability for CRT be
thoroughly assessed, and the
details of that assessment be
recorded in their medical record.
Strong Low
Can J Cardiol 2013; 29(2):182-195
Page 11
23-04-21 11Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
• Continued up-titration of medical therapy– Carvedilol (25 mg BID), ramipril (5 mg OD) &
spironolactone (25mg OD)
• Remains class III, LVEF now 30%
Case 1 - continued
Page 12
23-04-21 12Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation One - Practical Tips
• The reasons for non-use of recommended heart failure medications or the prescription of lower than the recommended doses of these agents should be recorded.
• Each patient’s functional capacity should be assessed, the QRS duration measured from a standard 12 lead ECG, and the LVEF quantified using a validated assessment method.
Page 13
23-04-21 13Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Two Strength Quality
CRT is recommended for patients
in sinus rhythm with NYHA class
II / III / ambulatory IV heart failure
symptoms, a LVEF ≤ 35%, and
QRS duration ≥ 130 ms due to
left bundle branch block.
Strong High
Can J Cardiol 2013; 29(2):182-195
Page 14
23-04-21 14Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Clinical Trial Evidence
Can J Cardiol 2013; 29(2):182-195
Page 15
23-04-21 15Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Clinical Trial Evidence
Page 16
23-04-21 16Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Summary of Evidence
• Very few NYHA I or non-ambulatory IV patients• Mean QRS: 153-173 ms• Most had LBBB• Patients with severe comorbidities excluded:
– Severe pulmonary disease– Severe liver disease– Severe renal disease– Limited life expectancy
Page 17
23-04-21 17Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Two - Practical Tips
• There is insufficient evidence to recommend CRT for patients with NYHA class I or patients non-ambulatory class IV NYHA symptoms.
• There is also insufficient data to recommend CRT in patients with QRS duration < 130 ms.
• Patients with LBBB and QRS duration ≥ 150 ms appear more likely to benefit from CRT than patients with non-LBBB conduction and/or less QRS prolongation.
Page 18
23-04-21 18Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Review of Case 1
• 78 year old woman– sinus rhythm, – dilated cardiomyopathy (NYHA III), &– LVEF 30%– Co-morbidities - DM, PVD, & eGFR 33 ml/min– Carvedilol (25 mg BID), ramipril (5 mg OD) &
sprionolactone (25 mg OD).
Page 19
23-04-21 19Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Three Strength Quality
A CRT pacemaker is
recommended for patients
who are suitable for
resynchronization therapy,
but not for an ICD.
Strong Moderate
Can J Cardiol 2013; 29(2):182-195
Page 20
23-04-21 20Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Clinical Trial Evidence
Can J Cardiol 2013; 29(2):182-195
Page 21
23-04-21 21Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Summary: CRT-P & CRT-D
COMPANIONDeath or hospitalisation
• CRT-P: HR 0.81 p<0.01• CRT-D: HR 0.80 p<0.01
Death• CRT-P: HR 0.76 p=0.059• CRT-D: HR 0.64 p=0.003
CARE HFDeath or hospitalisation
• CRT-P: 0.73 p<0.001
Death• CRT-P: 0.74 p<0.0002
Page 22
23-04-21 22Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Risk Factors•NYHA > II•Age > 70 years•BUN > 26 mg/dl•QRSd > 120 ms•AF
• MADIT II cohort• 1191 pts• F-UP 8 years
Page 23
23-04-21 23Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
JACC 2012; 59:2075-9
Page 24
23-04-21 24Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Page 25
23-04-21 25Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Three - Practical Tips
• CRT-P has been shown to reduce morbidity and mortality in patients with NYHA class III and ambulatory class IV heart failure symptoms.
• Therapy should be individualized in accordance with the overall goals of care.
Page 26
23-04-21 26Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
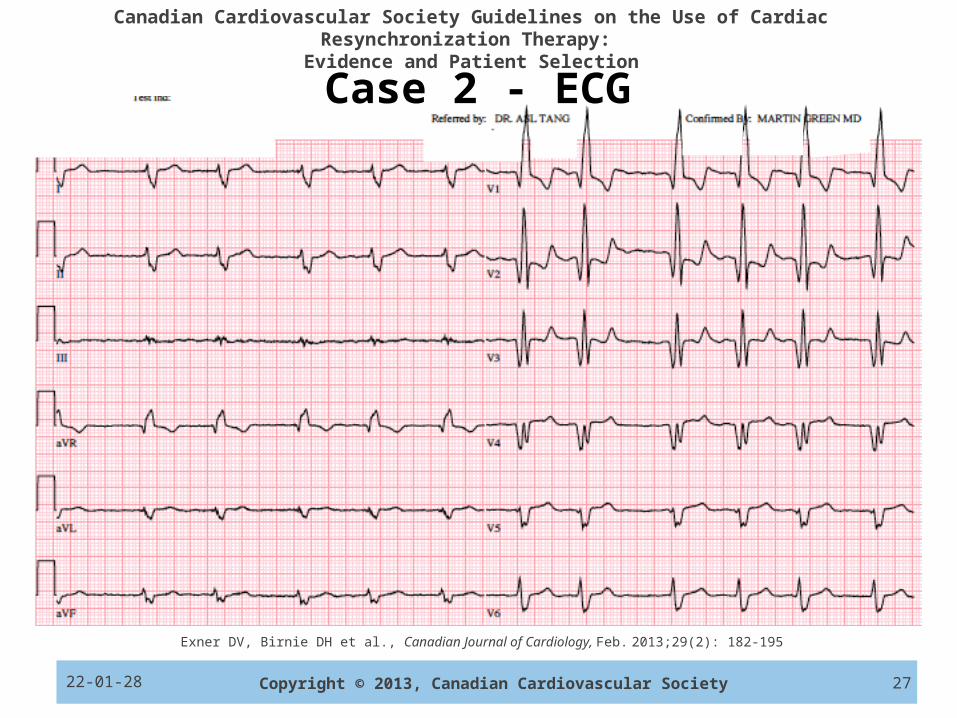
Case 2
• 57 year old man– Paroxysmal atrial fibrillation, – Ischemic cardiomyopathy (NYHA II), & LVEF 28%– Co-morbidities - HTN
• Medications:– EC ASA 81 mg OD, bisoprolol (10 mg OD),
perindopril (8 mg OD), spironolactone (25 mg OD) & rosuvastatin 20 mg OD.
Page 27
23-04-21 27Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Case 2 - ECG
Page 28
23-04-21 28Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Five Strength Quality
CRT may be considered for
patients in permanent AF
who are otherwise suitable
for this therapy.
Weak Low
Can J Cardiol 2013; 29(2):182-195
Page 29
23-04-21 29Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Utility of CRT in Patients with AF
Systematic review and meta-analysis
Death, CRT non-response, LV remodeling, quality of life, & six-min walk distance.
23 observational studies, 7,495 CRT recipients
25.5% with AF,
Mean follow-up of 33 months. Wilton et al. Heart Rhythm 2011;8:1088-94
Page 30
23-04-21 30Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Greater non-response (34.5% AF vs. 26.7% NSR)
Wilton et al. Heart Rhythm 2011;8:1088-94
Page 31
23-04-21 31Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Higher annual mortality (10.8% AF vs. 7.1% NSR)
Wilton et al. Heart Rhythm 2011;8:1088-94
Page 32
23-04-21 32Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
RAFT – AF Subset
Healey et al. Circulation Heart Failure 2012;5:566-70.
~ 34% of CRT-treated patients had ≥95% & ~ 47% had ≥90% biventricular pacing.
Page 33
23-04-21 33Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
RAFT – AF Subset
Healey et al. Circulation Heart Failure 2012;5:566-70.
Page 34
23-04-21 34Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Five - Practical Tips• The amount of biventricular pacing needs to be
evaluated.
• Arrhythmia device counters alone may not accurately reflect the true percent biventricular pacing.
• It is important to ensure a very high percentage of biventricular pacing.
• AV junctional ablation may be necessary to achieve sufficient biventricular pacing.
Page 35
23-04-21 35Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Case 2 – continued (amiodarone added)
Page 36
23-04-21 36Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Six Strength Quality
CRT may be considered for
patients in sinus rhythm with
NYHA class II / III / ambulatory
IV heart failure, LVEF ≤ 35%,
& QRS duration ≥ 150 msec
not due to LBBB conduction.
Weak Low
Can J Cardiol 2013; 29(2):182-195
Page 37
23-04-21 37Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
CRT in Patients with RBBBFive studies, with 259 patients randomized to CRT and 226 randomized to non-CRT.
RBBB; N (%)MIRACLE 28 (6.2)CONTAK CD 33 (5.7)CARE-HF 35 (4.3)MADIT-CRT 228 (12.5)RAFT 161 (9.0)
Nery et al. Heart Rhythm 2011;8:1083-87
Page 38
23-04-21 38Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
CRT-D
ICD
RBBB
HR (95% CI): 1.24 (0.65, 2.36)Log rank p = 0.48
NIVCD
HR (95% CI): 1.0 (0.60, 1.66)Log rank p = 0.84
RAFTBirnie et al CCS Conference , Vancouver2011
Page 39
23-04-21 39Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Page 40
23-04-21 40Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Severely prolonged QRS
Moderately prolonged QRS
Systematic review and meta-analysis
Page 41
23-04-21 41Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Six - Practical Tip
• There is no clear evidence of benefit with CRT among patients with QRS durations < 150 ms due to non-LBBB conduction.
Page 42
23-04-21 42Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Echo Dyssynchrony Assessment
Page 43
23-04-21 43Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Eight Strength Quality
Routine assessment of
dyssynchrony with present
echocardiographic techniques
is not recommended to guide
the prescription of CRT.
Strong Low
Can J Cardiol 2013; 29(2):182-195
Page 44
23-04-21 44Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Mechanical Dyssynchrony
Mostly echo; some nuclear & MRISingle center studies: echo mechanical dyssynchrony accurately predicts response to CRT Large multi-centre study (PROSPECT): failed to confirm this.
PROSPECT STUDY (Circulation. 2008;117: 2608-2616.)
Conclusion “no echo measure of mechanical dyssynchrony can be used to improve selection of patients for CRT”
Page 45
23-04-21 45Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
LV scar and response to CRT
• The extent of LV scaring seems important in determining response to CRT
• Some studies have found that it is the global extent of LV scar that is important
• Others found the size of the lateral to be key.
Page 46
23-04-21 46Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Eight - Practical Tips
• Issues of reproducibility and inter- and intra-rater assessment limit the routine role of echo to guide the prescription of CRT.
• The utility of imaging methods is under investigation.
Page 47
23-04-21 47Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
72 year old female
•Dual chamber pacemaker (AVB in 2006)
• Before PM - underlying atrial rhythm with 1° AV block, QRS 80 ms, & LVEF 45%
• Now - 100% RV paced (underlying CHB)
• LVEF now 32%, BNP is 1200
• Progressive DOE (now NYHA III)
•Carvedilol 25 mg BID, Ramipril 10 mg BID, & Spironolactone 25 mg OD
Case 3
Page 48
23-04-21 48Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Case 3 - ECG
Page 49
23-04-21 49Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Seven Strength Quality
CRT may be considered for
patients who are chronically
RV-paced or are likely to be
chronically paced, have
signs and/or symptoms of
heart failure, and a LVEF ≤
35%.
Weak Low
Can J Cardiol 2013; 29(2):182-195
Page 50
23-04-21 50Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Biventricular vs. LV Pacing in Patients with LV Dysfunction and AV Block (BLOCK HF)
N = 691; LV dysfunction & heart block CRT versus RV pacing (pacemaker or ICD).Mean LVEF 40%, 84% NYHA class II or III, Average follow-up 37 monthsResults for CRT vs. RV pacing
- 25% reduction in risk of death, need for IV HF therapy, or > 15% LV ESV index (1° outcome)
- 30% reduction in HF hospitalization (2° outcome) - No significant Δ in mortality (2° outcome)
Page 51
23-04-21 51Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Seven - Practical Tips• RV pacing may be harmful and strategies to minimize RV
pacing should be implemented prior to CRT upgrade.• The utility of CRT in patients who do not have a pre-
existing LBBB and are chronically RV paced is uncertain. • Patients undergoing AV junctional ablation with
moderate LV dysfunction may benefit from CRT.• It is often difficult to reliably predict which patients will
be chronically RV paced at the time initiating pacing.• The risks of CRT upgrade need to be considered and
balanced with the potential benefits of CRT upgrade.
Page 52
23-04-21 52Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Angiogram
1
2
3
Page 53
23-04-21 53Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Recommendation Four Strength Quality
In patients treated with CRT,
pacing from a non-apical LV
epicardial region may be
considered.
Weak Low
Can J Cardiol 2013; 29(2):182-195
Page 54
23-04-21 54Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Avoid “apical”Circulation 2011;123:1166
Page 55
23-04-21 55Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Anterior vs. lateral vs. posteriorCirculation 2011;123:1166
Page 56
23-04-21 56Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
LV Lead Placement
Page 57
23-04-21 57Copyright © 2013, Canadian Cardiovascular Society
Exner DV, Birnie DH et al., Canadian Journal of Cardiology, Feb. 2013;29(2): 182-195
Canadian Cardiovascular Society Guidelines on the Use of Cardiac Resynchronization Therapy: Evidence and Patient Selection
Questions & Review of Objectives
1. Review the appropriate selection of patients for CRT
2. Discuss the role of CRT-pacing
3. Describe the risks and benefits related to patients with AF, RBBB and chronic RV pacing
4. Understand technical issues related to CRT including lead placement
5. Discuss the role of imaging in assessment of CRT