Cosmetic Special Topic Abdominoplasty and Abdominal Wall Rehabilitation: A Comprehensive Approach Oscar M. Ramirez, M.D. Baltimore, Md. Standard abdominoplasty techniques involve a low hor- izontal or W skin excision, muscle plication, and umbilical transposition. Newer techniques include suction-assisted lipectomy, the use of high lateral tension with fascial sus- pension, and external oblique muscle advancement. The author has modified these traditional procedures and added new techniques to improve the aesthetic and func- tional results of the abdominoplasty procedure. This mod- ification provides a comprehensive approach to abdom- inal wall aesthetic improvement and rehabilitation. The comprehensive approach described includes four com- ponents: the “U-M dermolipectomy,” “V umbilicoplasty,” the rectus abdominis “myofascial release,” and suction- assisted lipectomy. The patient is marked while standing for areas of suction lipectomy and undermining. The lower incision is designed as an open U with the lateral limbs placed inside the bikini line. The upper incision is a lazy M with the higher peaks located at the level of the flanks. Subcutaneous hydration is achieved to perform suction along the flanks, waistline, and iliac areas. Gentle suction of the flaps is also performed. The umbilicus is cored out in a heart shape. The flaps within the U-M marks are excised, and the undermining is performed to the xiphoid and costal margins. The rectus diastasis is marked, and the anterior rectus fascia is incised at the junction of the medial third with the central third of the width of the rectus sheath. Horizontal figure-eight plication sutures by using the lateral fascial edge enable easier infolding of the central tissue. The new recipient of the umbilicus is made by an incision in a V shape on the abdominal flap. The umbilicus is telescoped, and the triangular flap of the abdomen is sutured to the triangular defect of the um- bilicus. Skin flap fixation to the umbilicus relieves tension in the lower portion of the flap. The upper skin flap, which is cut in an M manner, provides lateral tension and matches the length of the lower flap. A standard fascial suspension is used and closure is performed in layers. The techniques described here are intertwined procedures. Each facilitates the accomplishment of the other proce- dure, and they complement each other. They all attain the 12 objectives of the abdominoplasty described. These combined techniques have been used in 104 patients in a period of 11 years. Complications were minimal and easily manageable, except for one patient who required excision of a pseudobursa and retightening of the lower quadrants of the abdominal wall musculature to correct extreme lordosis. A comprehensive approach for the treatment of complex abdominal wall aesthetic and functional defects is presented. These require thoughtful integration of the four components mentioned. This approach has allowed predictable, reproducible, and aesthetically pleasing re- sults. (Plast. Reconstr. Surg. 105: 425, 2000.) Traditional abdominoplasty techniques for severe deformities include the following proce- dures: (1) “dermolipectomy” for removal of excess fat and skin, (2) “plication” of the ante- rior rectus sheath for muscle diastasis, and (3) transposition of the umbilicus to a new loca- tion in the abdominal wall skin. Newer tech- niques developed in the past few years include (1) suction-assisted lipectomy, (2) high lateral tension closure with fascial suspension, and (3) external oblique fascial advancement to create a smaller waistline. Some of these techniques may have draw- backs, and the newer maneuvers, particularly the external oblique muscle advancement, can be technically challenging. Therefore, the author has modified these traditional procedures and added new techniques to improve the aesthetics and functional results of the abdominoplasty pro- cedure. I postulate that the combination of these techniques provides a comprehensive approach to abdominal wall rehabilitation with superior aesthetic results. OBJECTIVES OF ABDOMINOPLASTY Every abdominoplasty should have the fol- lowing objectives, and every described tech- nique should be measured against these objec- tives: (1) place the incisions within the bikini line; (2) reduce or eliminate striae; (3) flatten and tighten the abdomen; (4) decrease the size From the Johns Hopkins University and the University of Maryland School of Medicine. Received for publication April 27, 1999; revised June 28, 1999. 425
Transcript
Cosmetic Special Topic
Abdominoplasty and Abdominal WallRehabilitation: A Comprehensive ApproachOscar M. Ramirez, M.D.Baltimore, Md.
Standard abdominoplasty techniques involve a low hor-izontal or W skin excision, muscle plication, and umbilicaltransposition. Newer techniques include suction-assistedlipectomy, the use of high lateral tension with fascial sus-pension, and external oblique muscle advancement. Theauthor has modified these traditional procedures andadded new techniques to improve the aesthetic and func-tional results of the abdominoplasty procedure. This mod-ification provides a comprehensive approach to abdom-inal wall aesthetic improvement and rehabilitation. Thecomprehensive approach described includes four com-ponents: the “U-M dermolipectomy,” “V umbilicoplasty,”the rectus abdominis “myofascial release,” and suction-assisted lipectomy. The patient is marked while standingfor areas of suction lipectomy and undermining. Thelower incision is designed as an open U with the laterallimbs placed inside the bikini line. The upper incision isa lazy M with the higher peaks located at the level of theflanks. Subcutaneous hydration is achieved to performsuction along the flanks, waistline, and iliac areas. Gentlesuction of the flaps is also performed. The umbilicus iscored out in a heart shape. The flaps within the U-M marksare excised, and the undermining is performed to thexiphoid and costal margins. The rectus diastasis is marked,and the anterior rectus fascia is incised at the junction ofthe medial third with the central third of the width of therectus sheath. Horizontal figure-eight plication sutures byusing the lateral fascial edge enable easier infolding of thecentral tissue. The new recipient of the umbilicus is madeby an incision in a V shape on the abdominal flap. Theumbilicus is telescoped, and the triangular flap of theabdomen is sutured to the triangular defect of the um-bilicus. Skin flap fixation to the umbilicus relieves tensionin the lower portion of the flap. The upper skin flap, whichis cut in an M manner, provides lateral tension andmatches the length of the lower flap. A standard fascialsuspension is used and closure is performed in layers. Thetechniques described here are intertwined procedures.Each facilitates the accomplishment of the other proce-dure, and they complement each other. They all attain the12 objectives of the abdominoplasty described. Thesecombined techniques have been used in 104 patients in aperiod of 11 years. Complications were minimal and easilymanageable, except for one patient who required excisionof a pseudobursa and retightening of the lower quadrantsof the abdominal wall musculature to correct extreme
lordosis. A comprehensive approach for the treatment ofcomplex abdominal wall aesthetic and functional defectsis presented. These require thoughtful integration of thefour components mentioned. This approach has allowedpredictable, reproducible, and aesthetically pleasing re-sults. (Plast. Reconstr. Surg. 105: 425, 2000.)
Traditional abdominoplasty techniques forsevere deformities include the following proce-dures: (1) “dermolipectomy” for removal ofexcess fat and skin, (2) “plication” of the ante-rior rectus sheath for muscle diastasis, and (3)transposition of the umbilicus to a new loca-tion in the abdominal wall skin. Newer tech-niques developed in the past few years include(1) suction-assisted lipectomy, (2) high lateraltension closure with fascial suspension, and (3)external oblique fascial advancement to createa smaller waistline.
Some of these techniques may have draw-backs, and the newer maneuvers, particularlythe external oblique muscle advancement, canbe technically challenging. Therefore, the authorhas modified these traditional procedures andadded new techniques to improve the aestheticsand functional results of the abdominoplasty pro-cedure. I postulate that the combination of thesetechniques provides a comprehensive approachto abdominal wall rehabilitation with superioraesthetic results.
OBJECTIVES OF ABDOMINOPLASTY
Every abdominoplasty should have the fol-lowing objectives, and every described tech-nique should be measured against these objec-tives: (1) place the incisions within the bikiniline; (2) reduce or eliminate striae; (3) flattenand tighten the abdomen; (4) decrease the size
From the Johns Hopkins University and the University of Maryland School of Medicine. Received for publication April 27, 1999; revised June28, 1999.
425
of the waistline; (5) decrease the thickness ofthe subcutaneous fat throughout the abdo-men, flanks, and iliac areas; (6) rejuvenate thepubis from a triangular senescent to an ovalyouthful form; (7) lift the lax anterolateralthigh skin near the groin crease and iliac areas;(8) create a well-defined xiphoumbilical de-pression; (9) give an illusion of an athleticabdomen, (10) change body posture; (11) cor-rect any hernia; (12) relieve back pain if this isrelated to muscle laxity of the abdomen.
The technique described herein attainsthese objectives. In many patients with severeaesthetic and functional problems, it is a trulyrehabilitative operation. In all, there are foursurgical components.
First Component: The “U-M” Dermolipectomy
The U-M abdominoplasty was designed toplace the incisions inside the aesthetic units ofthe abdomen.1 Conceptionally, this incision isvery similar to the “bicycle handlebar” de-scribed by Baroudi and Ferreira.2 The U-Mincision includes an open U and a lazy M (Figs.1 and 2). This particular geometrical designaccomplishes several goals: (1) The length ofthe lower incision matches the length of theupper incision. This technique makes lesslikely an interminable chase of the “dog-ears”at the end of the incisions. (2) The final clo-sure finishes within the abdominal wall aes-thetic units and follows a parallel line to a“french-cut” bikini. (3) The concept of highlateral tension is incorporated in the design,which lifts the lax anterolateral thigh.3 (4) Be-cause the pubic incision is very low, it dimin-ishes the size of the pubis and also lifts the
pubic area, changing the shape from a senes-cent, triangular form to an oval, youthful one.
Second Component: “V” Umbilicoplasty
One method of coring out the umbilicus fortransposition during an abdominoplasty isthrough a circular incision. The recipient inci-sion is also a circular defect. This may producea constricting scar contracture that narrows theumbilical opening. To avoid this problem, wehave designed the umbilical incision by excis-ing a triangular flap on the upper or lowermeridian of the umbilicus (Fig. 3, left). Thelocation of this will depend on patient’s desireto have a “frowning” or “smiling” navel. The Vincision gives a “smiling” appearance, whereas
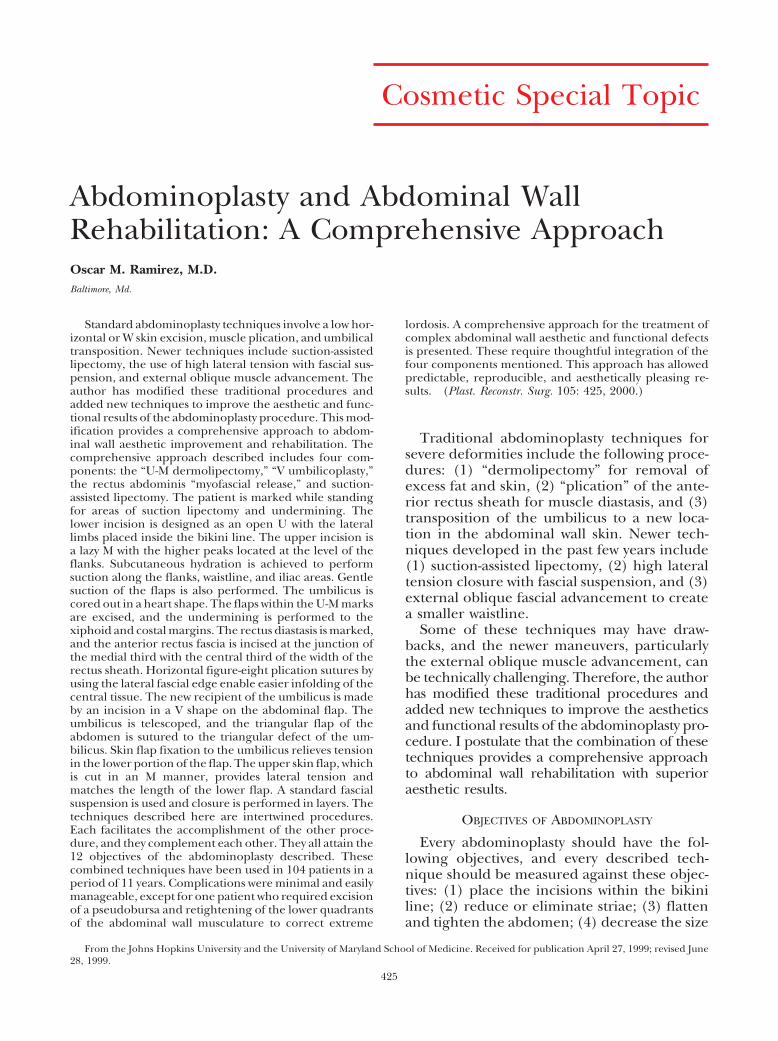
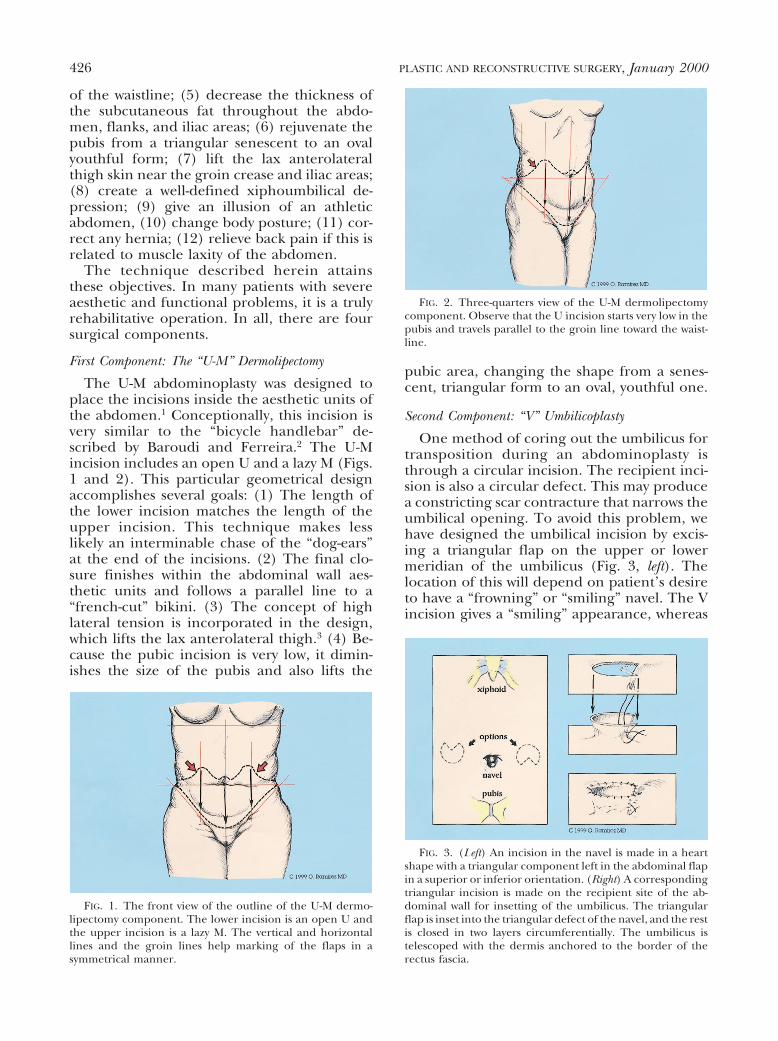
FIG. 1. The front view of the outline of the U-M dermo-lipectomy component. The lower incision is an open U andthe upper incision is a lazy M. The vertical and horizontallines and the groin lines help marking of the flaps in asymmetrical manner.
FIG. 2. Three-quarters view of the U-M dermolipectomycomponent. Observe that the U incision starts very low in thepubis and travels parallel to the groin line toward the waist-line.
FIG. 3. (Left) An incision in the navel is made in a heartshape with a triangular component left in the abdominal flapin a superior or inferior orientation. (Right) A correspondingtriangular incision is made on the recipient site of the ab-dominal wall for insetting of the umbilicus. The triangularflap is inset into the triangular defect of the navel, and the restis closed in two layers circumferentially. The umbilicus istelescoped with the dermis anchored to the border of therectus fascia.
426 PLASTIC AND RECONSTRUCTIVE SURGERY, January 2000
the inverted V gives a “frowning” navel. The Vincision seems to be preferred by patients. Ialso favor this incision because it helps to an-chor the upper abdominal flap to the naveland reduces tension on the lower flap at thepubic line closure (the portion of the flap withmore risk of vascular compromise). The recip-ient defect of the navel is created by a recipro-cal, triangular incision of the abdominal flap.The tension in the abdominal flap will createthe heart-shaped defect, and the triangularflap is inset in the triangular defect of the navel(Fig. 3, right). The most important feature ofthe V umbilicoplasty is that it avoids a concen-tric scar contracture. This technique is a mod-ification of a previous work presented by Juri etal.4
Third Component: The Rectus Abdominis “Myofas-cial Release” and Repair
The traditional method of correcting diasta-sis recti is by plicating one intact anterior rec-tus sheath against the opposite member (Fig. 4,left). This method usually creates significanttension as the anterior rectus fascia is advancedover the encased rectus muscles toward themidline. This technique may produce signifi-cant postoperative pain. Furthermore, it will beineffective in defining the waistline. To avoidthese problems, we have applied to our ab-dominoplasties a technique I have called “rec-tus abdominis myofascial release” (Fig. 4,right). This technique is an offspring of theexperience gained using the “component sep-aration” method for closure of abdominal walldefects.5 The anatomic and physical principleis that a gradual release and undermining of
the components of the abdominal wall dimin-ishes the index of tension during abdominalwall closure.6 Therefore, the first step is toincise the anterior rectus sheath at the junctionof the inner one-third with the middle third ofthe rectus muscle width. In cases of significantabdominal laxity, this incision is made at abouthalf of the rectus width. These incisions meetat the level of the xiphoid process superiorlyand the pubis inferiorly (Fig. 5). The rectusmyofascial release allows the centrifugal forcesof the rectus muscles to push the muscles to-ward the midline, facilitating closure with de-creased tension. It also allows better pull of theexternal oblique muscle, which in turn will bemore effective in redefining and decreasingthe waistline measurements (Fig. 6). The aver-age width of advancement at the level of thenavel is 10.5 cm. It varies from 6 to 18 cm.
Fourth Component: Suction-Assisted Lipectomy
Most patients with skin excess also have athick panniculus on the abdomen and neigh-boring areas. This requires contouring bymeans of suction lipectomy at the time of theabdominoplasty. Although, ideally, total con-touring with suction should be done as a pre-liminary stage to abdominoplasty, in reality,this is almost impossible. This staged approachis reserved only for the high-risk (class III)patient.7 Patients of class I and II can have thecombined procedure, but the suction lipec-tomy should be attempted with caution andthe patient should be informed about the po-tential increased risk if liposuction beyond mi-nor contouring is planned.
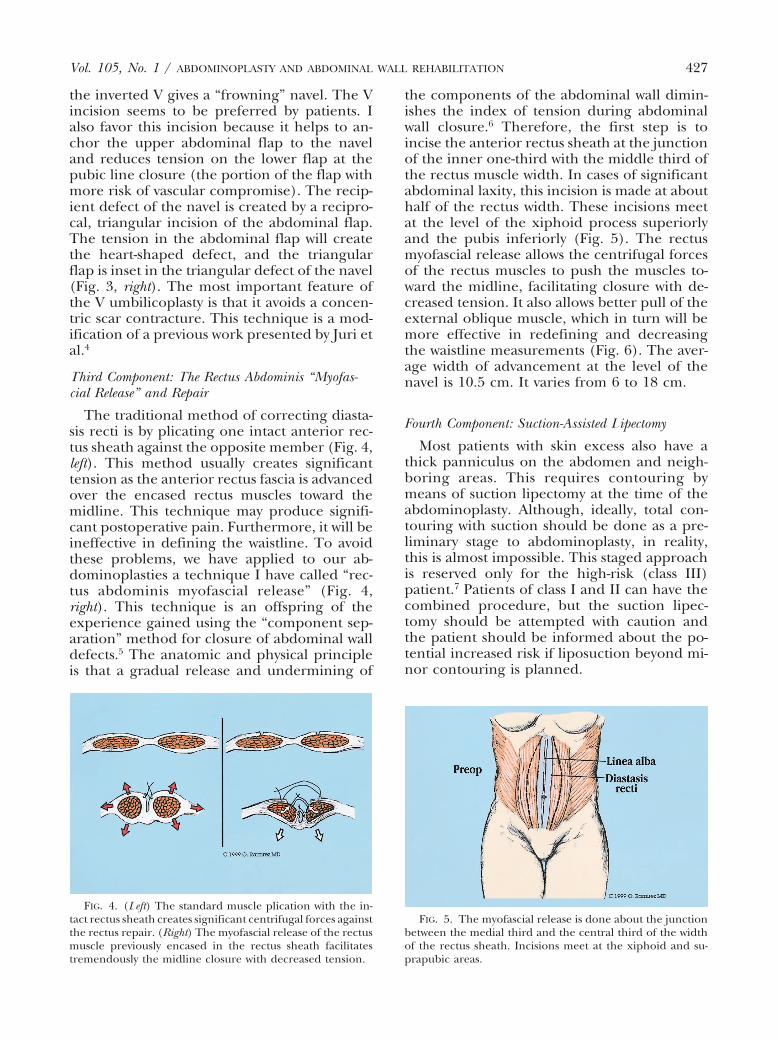
FIG. 4. (Left) The standard muscle plication with the in-tact rectus sheath creates significant centrifugal forces againstthe rectus repair. (Right) The myofascial release of the rectusmuscle previously encased in the rectus sheath facilitatestremendously the midline closure with decreased tension.
FIG. 5. The myofascial release is done about the junctionbetween the medial third and the central third of the widthof the rectus sheath. Incisions meet at the xiphoid and su-prapubic areas.
When suction-assisted lipectomy is per-formed at the time of the abdominoplasty, Iusually follow the recommendations describedby Matarasso7 with only one exception: the newxiphoumbilical depression is suctioned moreliberally. As advised by him, I also would notrecommend suction in the central portion ofthe flap below the new umbilical position. Suc-tion is done with small cannulas, i.e., 2 to 3mm, following the axial orientation of the ves-sels outside and inside the “vascular arc” ex-cept in the new xiphoumbilical midline, whereby its nature, the suction should be done in avertical direction.
SURGICAL TECHNIQUE
Preoperative Management
Plication techniques, myofascial advance-ments, or both, will compress the contents ofthe abdominal cavity. This will produce a sig-nificant counterforce toward the redefined ab-dominal wall, producing pain, potential dehis-cence, and ileus paralyticus. The latter willincrease further the internal pressure, creatingan increasingly deteriorating vicious cycle. Ifthe patient vomits, it will increase even morethe tension against the myofascial suture lineclosure. The increase in abdominal pressurewill also compress the posterior abdominalstructures from which the inferior vena cava isthe most compressible. This will produce astagnation of the venous return with the sub-sequent potential development of massivedeep venous thrombosis. To avoid this chain ofevents, it is essential to prevent bowel disten-tion by the following maneuvers: a good bowel
preparation that includes a clear liquid diet for2 to 3 days before surgery, laxatives, enemas,and antibiotics to decrease the growth of bac-teria flora responsible for intestinal gas andstool production. In addition, I include in myregimen Reglan (chlorpropamide) 10 mgorally every 6 hours to decrease production ofgastrointestinal juice and to stimulate peristal-sis of bowels in the early postoperative period.This regimen has made postoperative recoveryeasier and less painful. Most importantly, wehave seen only one case of minor deep venousthrombosis (at the calf) and no cases of post-operative ileus paralyticus or abdominal disten-tion.
Preoperative Markings
Markings are made in the standing position.Reference marks are outlined initially. Theseinclude groin lines with direct extension intothe upper iliac areas, central midline of theabdomen, parallel lines to the central midlinethat crosses the flanks, a vertical line on thesilhouette of the patient that crosses the waist-line and lateral hip areas. Another line perpen-dicular to the midline is made across the ab-domen usually at the level of the navel. Thesereference lines are useful for markings of theplanned flap excision as symmetrical as possi-ble (Figs. 1 and 2).
The open U is marked first. For this, thepubic skin is lifted and a horizontal line ismarked, leaving a reasonable pubic size. Thismark is approximately 5 to 7 cm from theanterior vulvar commissure. The line extendsjust medial to the groin areas. From here, thedirection of the line is quickly diverted towardthe waistline area. During this process, onesurgeon’s hand elevates the thigh skin in avertical direction. The procedure is repeatedon the contralateral side.
The lazy M is marked next. This design has asequence of hills and valleys with the centralportion just above the umbilicus and the high-est point at the level of the linea semicircularis.A gentle slope is constructed about the flankareas, and this line gradually tapers to meet theuppermost extension of the U component.The M configuration can change slightly toadapt to the areas of more skin laxity or ten-sion.
The Operation
Surgery is performed under general anesthe-sia. Intermittent compression devices are ap-
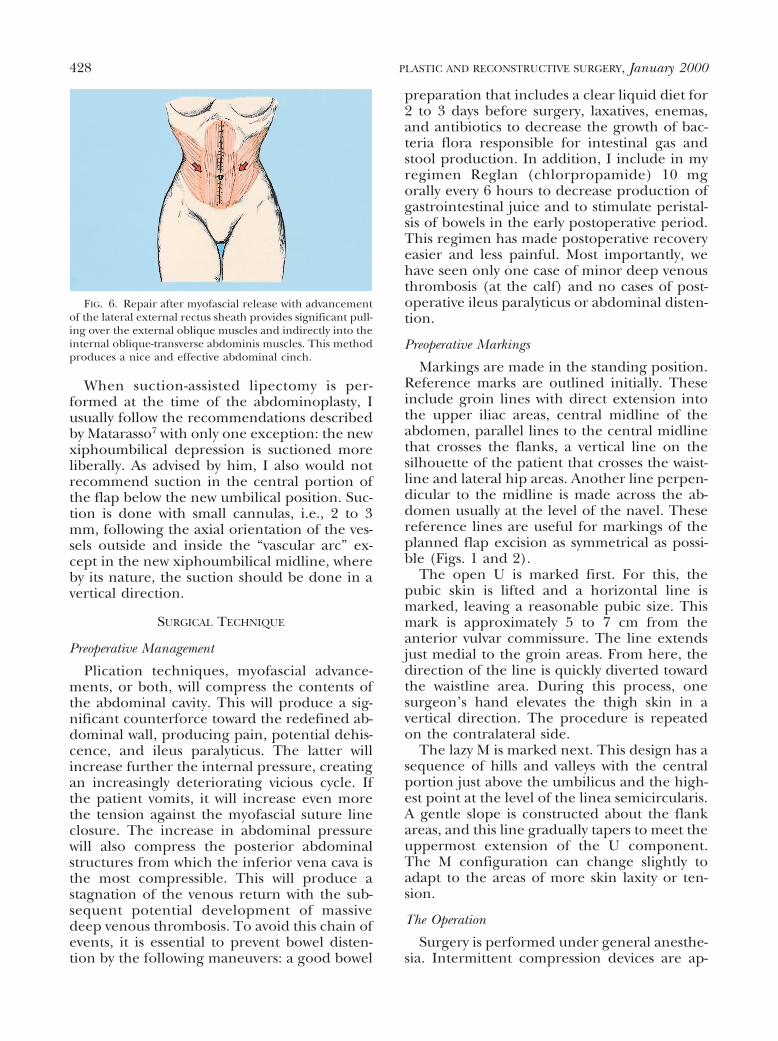
FIG. 6. Repair after myofascial release with advancementof the lateral external rectus sheath provides significant pull-ing over the external oblique muscles and indirectly into theinternal oblique-transverse abdominis muscles. This methodproduces a nice and effective abdominal cinch.
428 PLASTIC AND RECONSTRUCTIVE SURGERY, January 2000
plied to the lower extremities. Dissection isperformed under “subcutaneous hydration.”We prefer this concept rather than the “tumes-cent” concept because we do not want to pro-duce the “orange peel” appearance on the ab-dominal flaps. We believe that the “tumescent”technique hinders the blood supply of theflaps, particularly if the flaps have to be elevat-ed.8 Suction-assisted lipectomy of the iliac areasand waistline is routinely performed with 4- to5-mm cannulas. I avoid suctioning the pubis; itsshortening and lifting will usually decrease itsbulk. The central thickness of the subcutane-ous layer of the flap to be advanced inferiorly issuctioned with 2- to 3-mm cannulas. If suctionis performed, this procedure should follow theorientation of the vascular supply to the ab-dominal flaps, namely an oblique directionfrom inferior to superior and from medial tolateral. Extreme caution is advised to avoidcompromising the blood supply of the abdom-inal flap. The portion of flap above the posi-tion of the new umbilicus is suctioned up to thesubdermal layer to create the xiphoumbilicaldepression. This is done through the recipientdefect made for the navel and by using smallcannulas. Etching in the midline below theumbilicus is never performed, to avoid vascularcompromise of the infraumbilical flap. Fromthe aesthetic point of view, this etching is notneeded.
Dermolipectomy is done by incising, ini-tially, the U component. Flap elevation is donewith the electrocautery; however, the large per-forators are better handled by suture ligationor application of hemoclips. This method willensure complete hemostasis and avoid poten-tial bleeding postoperatively during coughing.The large vessels underneath the useful por-tion of the flap are also suture ligated ratherthan electrocoagulated to avoid spread of heatdamage on its corresponding vascular tree.When dissection approaches the navel, this iscored out after the incision in the navel isdone, as will be explained in the umbilicoplastysection. Dissection extends up to the costalmargins and the xiphoid areas. A trial of ad-vancement of the flap with the operative tablebent to 45 degrees is made. The previouslymarked upper incision (M component) ismatched against the lower incision. If any dis-crepancy exists, appropriate adjustments aremade before committing yourself to the finalflap trim.
If a smaller abdominoplasty is required and
the pubic-umbilicus distance is high, you couldperform an “umbilical float” procedure by us-ing the U-M abdominoplasty pattern. However,with this technique, the navel could be reposi-tioned 2 or 3 cm only. The use of this variationis limited to a very small group of patients.
The abdominal muscle repair is done afterthe abdominal skin flap is elevated. Althoughvariations in the fascial closure are made toaddress specific patients’ problems, in the ma-jority of patients, the technique used is as fol-lows: The rectus diastasis is marked and anelliptical shape from xiphoid to pubis on theanterior rectus sheath is marked with the wid-est portion around the navel. This ellipse variesfrom 6 to 18 cm with an average of 10.5 cm(5.25 cm to each side of the midline). About1-cm incisions every 3 to 4 cm in an interruptedmanner are made along the markings on theanterior rectus sheath by using the cold knife.The hemostat is introduced in each incision,the fascia elevated, and the initial incisions isconnected with electrocautery (Fig. 7, above).The area of the tendinous inscriptions is avoided.Occasionally, you may encounter a musculocuta-neous perforator, which is suture ligated. Themidline repair is done with 0 to no. 2 Tevdek(Deknatal DSP, Fall River, Mass.). Suture sizedepends on the strength of the tissues. The su-tures are applied in a horizontal figure-eight withinverted knots. Two key sutures are applied, onejust above and another one just below the navel(about 3 to 4 cm equal distance). The navel canbe seen to drop immediately a few cm below thelevel of the rectus repair line. To avoid potentialdifficulty in retrieving the navel, a 3-0 nylon su-ture tie is applied to it. The rest of the myofascialrepair is done from xiphoid to pubis (Fig. 7,below). If the abdominal laxity is significantand/or the waistline measurements must be de-creased significantly, then the medial border ofthe rectus muscle is repaired in the midline andindependently the lateral rectus fascia, which isdissected laterally to the linea semicircularis, isadvanced over and repaired in the midline. Thisapproach will provide a more effective tractionon the external oblique muscle and decrease thesize of the waistline. To aid in muscle relax-ation and avoid pain in the first 24 hours, theabdominal muscles are infiltrated with 0.25%bupivacaine mixed with 1:100,000 epineph-rine solution. About 80 to 100 cc of thissolution is injected just underneath the ex-ternal fascial layers of the rectus and externaloblique muscles by using long blunt needles
used for epidural anesthesia (Tuey needles).The trajectory of the needle must be visual-ized throughout the entire length by thetranslucency of the fascia. This way, you willavoid inadvertent injection deep in the abdo-men or in the muscle itself. The higher con-centration of epinephrine in relation to thebupivacaine is to make its absorption veryslow.
The umbilicoplasty has several steps (Fig. 3):first, the navel is cored out after a heart-shapedincision on its periphery is made. This proce-dure requires the excision of a triangular flapof navel skin in a superior or inferior meridian.The usually long umbilical stalk is telescopedwith sutures applied from subdermis to fascialayer of the rectus. During the trial of flapclosure, the umbilical demarcator is used tolocate the navel’s new position in the abdomi-nal wall skin. After this is done, a triangularincision is done on the abdominal skin. Upontraction of the flap, the defect becomes a heart-
shaped one. The skin recipient around the newnavel position is defatted to simulate a similarconcavity around the navel seen in the idealabdomen. The navel is inset in its new positionin the abdominal wall in two layers by usingnonabsorbable suture material.
Trimming of the upper abdominal flap isdone with incision of the skin at a 90-degreeangle in relation to the surface and the subcu-taneous/Scarpa’s fascia layer at a 45-degreeangle. This approach is because these laststructures are usually retracted superiorly withthe initial incision. When closure of this layer ismade, it will fit exactly at the suture line and itwill not be redundant. Abdominal flap closureis done in two to three layers. The initial layerof sutures is applied at the midline, to central-ize the midline. Another key suture is appliedmidway between the midline and the end ofthe suture line closure with the upper flappushed toward the midline. This way, the up-per flaps near the midline are closed with min-imal or no tension. The final closure is per-formed from lateral to medial, always with theupper flap being constantly shifted manuallytoward the midline, because the natural ten-dency of this flap is to rotate laterally. Twoclosed-system suction drains are left under theflaps with the ends toward the flanks and in acrisscrossed manner. Topifoam (LySonic, Inc.,Carpinteria, Calif.) dressing and a well-contoured abdominal binder are applied.
Postoperative Management
After surgery, intravenous fluids and intrave-nous antibiotics are given for 24 hours. Ambu-lation is started the next day. A clear liquid dietis given for 3 or more days. Supportive stock-ings and intermittent compression devices areused until full ambulation is obtained. Chlor-propamide 10 mg every 6 hours orally andstool softeners are given until regular bowelmovement is obtained. Drains are advanced atthe third or fourth postoperative day. They areremoved when fluid collection is ,20 cc per 24hours per drain or at 5 days postoperatively,whichever comes first. An abdominal binder isused for several weeks postoperatively. Drivingis allowed at 3 to 4 weeks postoperatively. Briskwalking is allowed at 6 to 8 weeks, jogging at 10to 12 weeks, and exercise without restrictionafter 14 to 16 weeks.
FIG. 7. (Above) Intraoperative view of the myofascial re-lease with incisions meeting around the xiphoid and supra-pubic areas. The widest area of the incision is around thenavel. U, umbilicus; P, pubis; X, xiphoid. (Below) Completionof the lateral rectus sheath repair with decrease of the widthof the abdominal girth. Arrows pointing to the umbilicus (U)and the forces around the waistline. X, xiphoid; P, pubis.
430 PLASTIC AND RECONSTRUCTIVE SURGERY, January 2000
CLINICAL EXPERIENCE
The comprehensive approach described inthis study has been used in our practice since1988. One hundred four patients have receivedthis combined procedure. Patients in whomalloplastic materials were used for abdominalwall repair are not included in this report.Patient satisfaction has been extremely high,and the complication rate is small. We havehad three patients with small areas of skin ne-crosis (5 3 4 cm, 3 3 4 cm, and 3 3 3 cm,respectively) in the lower central abdominalflap. Two patients required secondary revision,one 3 weeks postoperatively and another oneseveral months later. These revisions did notcompromise the final aesthetic or functionalresult. Five patients developed seroma that re-quired serial aspiration of fluid. One patientrequired excision of a pseudobursa for chronicfluid collection; this same patient required fur-ther tightening of lower quadrants on thelower abdominal wall musculature, mostly tocorrect her body posture (extreme lordosis).One patient developed a drain tract infectiontreated successfully with drainage and antibiot-ics. No secondary hernias were seen. Twenty-six patients having moderate or severe backpain were completely relieved of their pain. Allpatients gained improvements in their postureand how their clothing fit. Many patients be-gan wearing bikini bathing suits that they wereunwilling to wear preoperatively. In 20 consec-utive patients, we measured the waist circum-ference preoperatively and at 6 months post-operatively. There was an average 10.5-cmreduction in waist size, ranging from 6 to 18 cm(Figs. 8 through 10).
DISCUSSION
Most patients with a small lower abdominal“pouch” will benefit from a smaller proceduresuch as a suction lipectomy,9 mini-abdomino-plasty,10 or an endoscopic abdominoplasty.11
However, patients with a large abdominal“apron,” severe laxity, or wide diastasis of therectus muscles represent a completely differentclinical problem that requires a more radicalapproach. This group of patients usually haveseveral aesthetic and functional problems,each of which requires attention. The proce-dures described in this study were designed tocorrect most of those problems: to remove theexcess abdominal skin, to tighten the lax an-terolateral thigh skin, to rejuvenate the ptotic
pubis, to improve the waistline, and to tightenthe lax abdominal wall musculature. This cor-rection in turn helped to improve the postureof the torso and in many cases improved theback pain in patients affected by this condition.Because the location of the final scars was aesthetically pleasing, many patients were ableto wear two-piece bathing suits, which theywere unwilling to do before surgery (Fig. 9).
The method of umbilicoplasty gave a naturalappearance without a constricting scar or nar-rowing of the opening. The midline abdominaletching produced a xiphoumbilical depressiongiving the appearance of an athletic abdominalwall with an illusion of a “prominent” rectusmuscle.
The four procedures described here, i.e.,U-M abdominoplasty, suction lipectomy, rectusmyofascial release, and umbilicoplasty, are in-tertwined procedures. Although each of thedescribed procedures could be individually in-tegrated into each surgeon’s preferred ab-dominoplasty approach, they work best if doneall four together. Each facilitates the accom-plishment of the other procedure, and theycomplement each other. The U-M abdomino-plasty component allows easy removal of tissue(skin and fat) around the waistline, allowingthe creation of a smaller waistline. Suction li-pectomy helps to better contour the abdomenand gives better definition to the distal ends ofthe line of closure. The myofascial release alsoallows better definition of the waistline becauseof the pull of the internal oblique and externaloblique muscles toward the midline. The myo-fascial release and repair also decreases theentire surface of the abdominal wall, which inturn permits removal of more skin/fat fromthe abdominal wall. The myofascial release alsoallows shortening and telescoping of the longumbilical stalk. The V-umbilicoplasty, in addi-tion to making the navel scar less conspicuous,allows anchoring of the upper abdominal flapto decrease tension on the pubic line closure.This method allows the safe removal of enoughskin to provide the optimal aesthetic result.
The location of the final incision medial andsuperior to the anterosuperior iliac spine al-lows the abdominal flap to rest in better con-tact with the musculofascial layer of the abdo-men. Incisions located at or below theanterosuperior iliac spine produce a tentingeffect on the flap, and this does not lie flat onthe abdominal wall musculature, creating a po-tential space for the formation of seroma. This
FIG. 8. (Above, left) Preoperative anteroposterior view of a 54-year-old woman with folding ofskin in the lower abdomen, significant weakness of the abdominal wall, and poor body posture.Observe the triangular senescent pubic area. (Above, right) Postoperative anteroposterior view.Observe the rejuvenation of the entire abdomen with re-creation of a nice waistline, re-creationof highlights and shadows of the abdominal wall, elevation of the anterolateral thigh skin, andrejuvenation of the pubis. The incision is inside the bikini line. (Below, left) Preoperative lateralview. Observe the pouchy, weak abdominal wall with poor body posture. Also, observe the ptosisof the pubis and groin areas. (Below, right) Postoperative lateral view. Observe the significantimprovement of the patient’s abdomen. The rectus muscle looks tight. The excess skin on theanterolateral thigh has been elevated and the pubis rejuvenated.
432 PLASTIC AND RECONSTRUCTIVE SURGERY, January 2000
FIG. 9. (Above, left) Preoperative anteroposterior view of a 42-year-old woman who presentedwith significant abdominal wall laxity, poor body posture, and back pain. Observe the excess skinover the groin and the triangular pubis. (Above, right) Postoperative anteroposterior view. Observethe significant improvement of the patient’s abdomen with decrease of the waistline and re-creation of the aesthetic lines of the abdomen. Observe that the U-M incision has ended up insidethe bikini line. Also, observe the lifting effect over the anterolateral thigh skin and pubisrejuvenation. The patient also had an augmentation/mastopexy procedure. (Below, left) Preop-erative lateral view. Observe this patient’s poor body posture with excessive lordosis. Observe thebulging abdominal wall. (Below, right) Postoperative lateral view. Notice the tight, athletic ab-domen. There is a supraumbilical concavity. The lordosis has been corrected. The pubis and thegroin skin have been lifted.
may be one of the reasons for a low rate ofseroma formation in this series, despite theroutine use of suction lipectomy.
It may be argued that the more curvilinearincision of the U-M abdominoplasty may leavea flap with a relatively higher length/width
FIG. 10. (Above, left) Preoperative anteroposterior view of 40-year-old man with significanttruncal obesity. The patient has a huge abdominal girth and excess abdominal panniculus. Also,observe the ptosis of the pubis and excess tissues over the groin. (Above, right) Postoperativeanteroposterior view. Observe the reduction of the waistline, the elimination of the excess skinon the abdomen, and elevation of the pubis. The patient also had a concomitant suctionlipectomy of the male breasts. (Below, left) Preoperative lateral view. Observe the huge abdominalpanniculus, laxity of the abdomen, excess tissue on the groin, and ptosis of the pubis. (Below,right) Observe the tight abdominal wall musculature, elimination of excess skin, and lifting ofthe structures neighboring the lower abdomen.
434 PLASTIC AND RECONSTRUCTIVE SURGERY, January 2000
ratio and that the collateral blood flow to thedistal flap may be diminished compared with amore horizontal incision. However, this theo-retical happenstance has not occurred. Therate of skin necrosis has been less in this seriesthan when using horizontal incisions, despite amore liberal use of concomitant suction lipec-tomy. This finding is probably because the ten-sion of closure is more lateral than central.Although not proved, it is also feasible that thelateral portions of the flap may “steal” bloodsupply from the central portions in the morehorizontal incisions.
Because of the significant redefinition ofmuscle tension in the abdomen, the symptomsof all of the patients with a history of back painhave improved. This relief is probably due toan indirect pull of the internal oblique-transversus abdominis muscles over the lum-bodorsal fascia with reduction of stress at theintervertebral joint as postulated by Graco-vetzky et al.12 and clinically demonstrated byToranto13 and also observed by us.5 The signif-icant reduction of weight on the abdominalapron and the abdominal muscle tighteningaccounts for the improvement in body posture.This improvement has been observed in themajority of patients, and they have emphasizedthis fact too.
CONCLUSIONS
A comprehensive approach for the treat-ment of complex abdominal wall aesthetic de-fects is presented. Many of those patients alsohave associated functional defects. Correctionof these problems requires multiple tech-niques. The procedures described here, i.e.,U-M abdominoplasty, suction lipectomy, V um-bilicoplasty, and the rectus myofascial release/repair, are integrated procedures. Each of theprocedures helps maximize the positive influ-
ence of the other. These have allowed us tohave predictable, reproducible, and aestheti-cally pleasing results. The rate of patient satis-faction has been extremely high.
Oscar M. Ramirez, M.D.Esthetique International2219 York Road, Suite 100Timonium, Md. [email protected]
REFERENCES
1. Ramirez, O. M. “U-M abdominoplasty.” Aesthetic Surg. J.19: 279, 1999.
2. Baroudi, R., and Ferreira, C. A. Contouring the hip andthe abdomen. Clin. Plast. Surg. 23: 551, 1996.
3. Lockwood, T. High-lateral-tension abdominoplastywith superficial fascial system suspension. Plast. Recon-str. Surg. 96: 603, 1995.
4. Juri, J., Juri, G., and Raiden, G. Reconstruction of theumbilicus in abdominoplasty. Plast. Reconstr. Surg. 63:580, 1979.
5. Ramirez, O. M., Ruas, E., and Dellon, A. L. “Compo-nent separation” method for closure of abdominal-wall defects: An anatomic and clinical study. Plast.Reconstr. Surg. 86: 519, 1990.
6. Nahas, F. X., Ishida, J., Gemperli, R., and Ferreira, M. C.Abdominal-wall closure after selective aponeurotic in-cision and undermining. Ann. Plast. Surg. 41: 606,1998.
7. Matarasso, A. Liposuction as an adjunct to a full ab-dominoplasty. Plast. Reconstr. Surg. 95: 829, 1995.
8. Ramirez, O. M., and Galdino, G. Does tumescent infil-tration have a deleterious effect on undermined skinflaps? Plast. Reconstr. Surg. 104: 2269, 1999.
9. Lewis, C. M. Early experience with aspirative lipoplastyof the abdomen. Aesthetic Plast. Surg. 11: 33, 1987.
10. Greminger, R. F. The mini-abdominoplasty. Plast. Re-constr. Surg. 79: 356, 1987.
11. Faria-Correa, M. A. Abdominoplasty: The South Amer-ican Style. In O. M. Ramirez and R. K. Daniel (Eds.),Endoscopic Plastic Surgery. New York: Springer-Verlag,1996.
12. Gracovetzky, S., Farfan, H., and Helleur, C. The ab-dominal mechanism. Spine 10: 317, 1985.
13. Toranto, I. R. Resolution of back pain with the wideabdominal rectus plication abdominoplasty. Plast. Re-constr. Surg. 81: 777, 1988.