Cosmetic Surgery of the Superficial Musculoaponeurotic System: Principles of Release, Vectors, and Fixation Bryan C. Mendelson, F.R.C.S.E., F.R.A.C.S., F.A.C.S. Melbourne, Australia The SMAS was described more than 25 years ago, yet its full potential in face-lift surgery has become appreci- ated only more recently. A reappraisal of the various as- pects of SMAS surgery is now appropriate. These include aspects of its release from the deep fascia, the several considerations underlying the vectors of flap redistribu- tion, and the rationale underlying the methods of flap fixation. These are unique, compared with the traditional considerations in subcutaneous face lifts and en bloc sub- periosteal lifts. (Plast. Reconstr. Surg. 107: 1545, 2001.) “If you understand something in only one way, then you do not really understand it at all.” —Marvin Minsky, Society of the Mind, 1987 The essence of most rejuvenation surgery of the face and brow is to mobilize the lax and ptotic tissue (skin based flap with a varying depth of the underlying tissue) and then ad- vance that flap to a somewhat higher position relative to the facial skeleton. The question of “preferred direction of lift” is still discussed, although current teaching favors a strong ver- tical lift for best correction. Of necessity, with limited access surgery, vertical traction is all that is possible. The inclusion of the superficial musculoapo- neurotic system (SMAS) has been the most fundamental change in technique since the beginning of face-lift surgery. 1,2 Face-lift sur- gery performed using the traditional subcuta- neous technique has been based on well- established routines. When the SMAS became incorporated in the technique, although it pro- vided a range of enhanced possibilities, it has been associated with some limitations and problems that have only gradually become understood. Chief among these was that, although the basic anatomy of the SMAS (the deeper layer of the superficial fascia of the face) was well described at the outset, other most relevant anatomy was not. Particularly significant is the anatomy of the ligamentous attachments be- tween the SMAS and the facial skeleton. 3–5 The sub-SMAS region of the medial cheek was con- sidered to be a nearly impenetrable jungle. At that time, is was considered unsafe to dissect beneath the superficial fascia of the cheek, other than over the buccal space where dissec- tion is less difficult. 1 Complicating matters is that the SMAS incorporates the muscles of fa- cial expression. Normal function of these mus- cles can be disturbed by SMAS surgery. This complication may arise from nerve damage oc- curring during the dissection or from abnor- mal pulling or distorted movements as a result of incomplete dissection or incorrect fixation. In the 25 years since the introduction of the superficial fascia into face-lift surgery, there has accumulated a sufficient body of experi- ence and of detailed anatomic knowledge to reflect on the basic principles of SMAS surgery. These explain some of the difficulties that have been associated with the procedure in the past. It becomes apparent that the principles that were so well established for traditional face-lift surgery were not necessarily sufficient for the different requirements with surgery of the SMAS. Received for publication September 19, 2000; revised November 6, 2000. Presented in part at the 4th Annual Dallas Aesthetic Surgery Symposium, in Dallas, Texas, on March 6, 2000, and at the Annual Scientific Conference of the Australasian Society of Aesthetic Plastic Surgery, Sanctuary Cove, Australia, on July 10, 2000. 1545
Transcript
Cosmetic
Surgery of the Superficial MusculoaponeuroticSystem: Principles of Release, Vectors, andFixationBryan C. Mendelson, F.R.C.S.E., F.R.A.C.S., F.A.C.S.Melbourne, Australia
The SMAS was described more than 25 years ago, yetits full potential in face-lift surgery has become appreci-ated only more recently. A reappraisal of the various as-pects of SMAS surgery is now appropriate. These includeaspects of its release from the deep fascia, the severalconsiderations underlying the vectors of flap redistribu-tion, and the rationale underlying the methods of flapfixation. These are unique, compared with the traditionalconsiderations in subcutaneous face lifts and en bloc sub-periosteal lifts. (Plast. Reconstr. Surg. 107: 1545, 2001.)
“If you understand something in only one way,then you do not really understand it at all.”
—Marvin Minsky, Society of the Mind, 1987
The essence of most rejuvenation surgery ofthe face and brow is to mobilize the lax andptotic tissue (skin based flap with a varyingdepth of the underlying tissue) and then ad-vance that flap to a somewhat higher positionrelative to the facial skeleton. The question of“preferred direction of lift” is still discussed,although current teaching favors a strong ver-tical lift for best correction. Of necessity, withlimited access surgery, vertical traction is allthat is possible.
The inclusion of the superficial musculoapo-neurotic system (SMAS) has been the mostfundamental change in technique since thebeginning of face-lift surgery.1,2 Face-lift sur-gery performed using the traditional subcuta-neous technique has been based on well-established routines. When the SMAS becameincorporated in the technique, although it pro-vided a range of enhanced possibilities, it hasbeen associated with some limitations and
problems that have only gradually becomeunderstood.
Chief among these was that, although thebasic anatomy of the SMAS (the deeper layerof the superficial fascia of the face) was welldescribed at the outset, other most relevantanatomy was not. Particularly significant is theanatomy of the ligamentous attachments be-tween the SMAS and the facial skeleton.3–5 Thesub-SMAS region of the medial cheek was con-sidered to be a nearly impenetrable jungle. Atthat time, is was considered unsafe to dissectbeneath the superficial fascia of the cheek,other than over the buccal space where dissec-tion is less difficult.1 Complicating matters isthat the SMAS incorporates the muscles of fa-cial expression. Normal function of these mus-cles can be disturbed by SMAS surgery. Thiscomplication may arise from nerve damage oc-curring during the dissection or from abnor-mal pulling or distorted movements as a resultof incomplete dissection or incorrect fixation.
In the 25 years since the introduction of thesuperficial fascia into face-lift surgery, therehas accumulated a sufficient body of experi-ence and of detailed anatomic knowledge toreflect on the basic principles of SMAS surgery.These explain some of the difficulties that havebeen associated with the procedure in the past.It becomes apparent that the principles thatwere so well established for traditional face-liftsurgery were not necessarily sufficient for thedifferent requirements with surgery of theSMAS.
Received for publication September 19, 2000; revised November 6, 2000.Presented in part at the 4th Annual Dallas Aesthetic Surgery Symposium, in Dallas, Texas, on March 6, 2000, and at the Annual Scientific
Conference of the Australasian Society of Aesthetic Plastic Surgery, Sanctuary Cove, Australia, on July 10, 2000.
1545
The discussion that follows is a synthesis ofempiric observation and established fact. Itcovers the related topics of extent of releaserequired, vectors of lift, and principles offixation.
RELEASE
The matter of “the extent of surgical releaserequired” continues to engage the mind ofaesthetic plastic surgeons. When face lifts areperformed at the subcutaneous and subperios-teal levels, this is a relatively simple matter, asthese face-lift flaps have a relatively uniformattachment to the deeper layer. Considerationsof surgical release are more complex in SMASflap surgery due to the nature of the attach-ment of the SMAS to the underlying perios-teum and deep fascia. There are specific areasof strong ligamentous fixation that require de-finitive surgical release and that contrast withintervening areas of loose adherence, whichseparate readily, such as the buccal and prezy-gomatic spaces. Those techniques of SMAS sur-gery that involve plication or imbrication of theexposed surface of the SMAS6–8 are fundamen-tally different from SMAS flap surgery, as theydo not involve mobilization of a SMAS flap withthe attendant surgical release of the areas ofligamentous fixation.
The effect of complete surgical release of thedeep ligamentous fixation of the SMAS in thevicinity of the area requiring correction is to
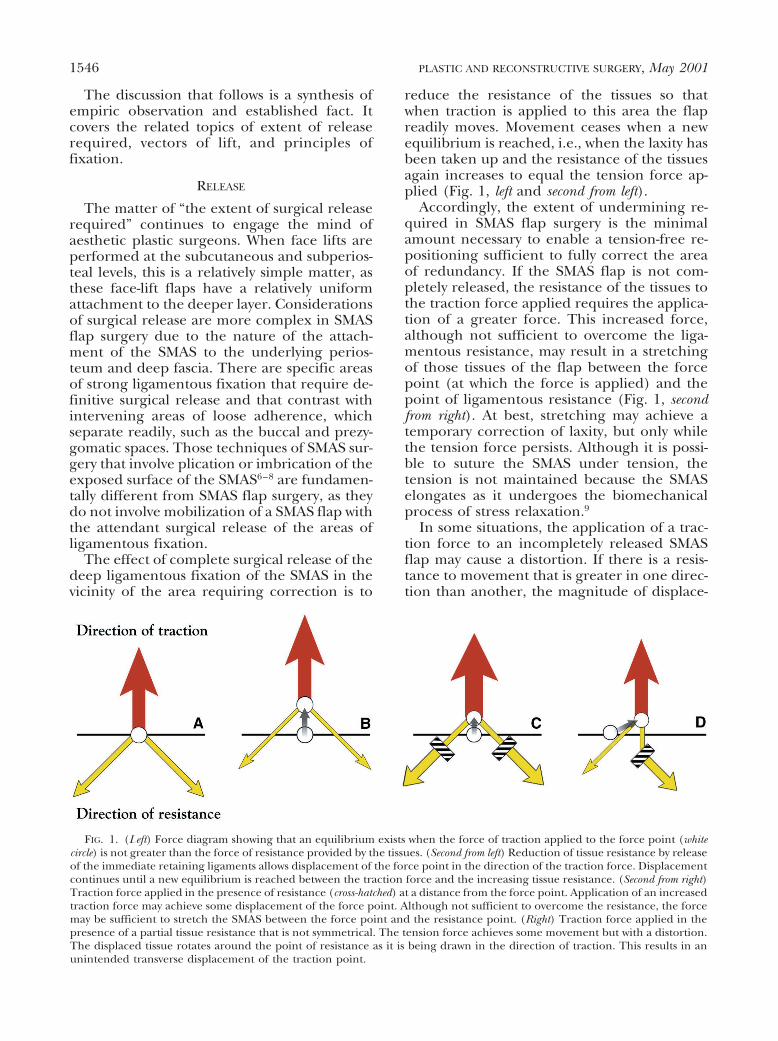
reduce the resistance of the tissues so thatwhen traction is applied to this area the flapreadily moves. Movement ceases when a newequilibrium is reached, i.e., when the laxity hasbeen taken up and the resistance of the tissuesagain increases to equal the tension force ap-plied (Fig. 1, left and second from left).
Accordingly, the extent of undermining re-quired in SMAS flap surgery is the minimalamount necessary to enable a tension-free re-positioning sufficient to fully correct the areaof redundancy. If the SMAS flap is not com-pletely released, the resistance of the tissues tothe traction force applied requires the applica-tion of a greater force. This increased force,although not sufficient to overcome the liga-mentous resistance, may result in a stretchingof those tissues of the flap between the forcepoint (at which the force is applied) and thepoint of ligamentous resistance (Fig. 1, secondfrom right). At best, stretching may achieve atemporary correction of laxity, but only whilethe tension force persists. Although it is possi-ble to suture the SMAS under tension, thetension is not maintained because the SMASelongates as it undergoes the biomechanicalprocess of stress relaxation.9
In some situations, the application of a trac-tion force to an incompletely released SMASflap may cause a distortion. If there is a resis-tance to movement that is greater in one direc-tion than another, the magnitude of displace-
FIG. 1. (Left) Force diagram showing that an equilibrium exists when the force of traction applied to the force point (whitecircle) is not greater than the force of resistance provided by the tissues. (Second from left) Reduction of tissue resistance by releaseof the immediate retaining ligaments allows displacement of the force point in the direction of the traction force. Displacementcontinues until a new equilibrium is reached between the traction force and the increasing tissue resistance. (Second from right)Traction force applied in the presence of resistance (cross-hatched) at a distance from the force point. Application of an increasedtraction force may achieve some displacement of the force point. Although not sufficient to overcome the resistance, the forcemay be sufficient to stretch the SMAS between the force point and the resistance point. (Right) Traction force applied in thepresence of a partial tissue resistance that is not symmetrical. The tension force achieves some movement but with a distortion.The displaced tissue rotates around the point of resistance as it is being drawn in the direction of traction. This results in anunintended transverse displacement of the traction point.
1546 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001
ment no longer relates just to the applied forceand the angle of traction as an additional fac-tor comes into play, i.e., rotation of the flaparound the point of remaining fixation. Theflap does not advance in the direction of theapplied force and to the extent expected.Rather, there is an angular displacement suchthat there may be excessive movement of theflap in the “wrong” direction relative to thelimited movement in the intended direction(Fig. 1, right). A classic example of this distor-tion is the lateral sweep of the cheek.10 Thisundesirable sequela of face lifts can result fromSMAS flap surgery when the anterior masseteric-cutaneous ligaments remain intact and blockthe intended vertical displacement of the mid-cheek. Instead, the more mobile lower part ofthe flap along the jaw line rotates around thelowest of these ligaments and is displaced pos-teriorly (Fig. 2).
A similar situation is prone to occur aroundthe lateral canthus when vertical traction isapplied to the suborbicularis oculi fascia in thisarea. If the resistance inferolateral to the forcepoint has been released but the medial restric-tion persists (due to the orbicularis retainingligament remaining intact), an oblique fold ofthe flap may result. The outer part of the lowerlid remains uncorrected until the restriction tomobility imposed by the resistance of that lig-ament has been released. These examples illus-trate a key principle of SMAS flap surgery thatwhere there is a block between the force pointand the area requiring correction, it is notpossible for SMAS flap surgery to improve thatarea.
When SMAS flap surgery was introduced, itwas not appreciated that there is a key func-tional differentiation of the cheek into twoparts. The outer or lateral cheek (preauricu-lar) is separated from the medial cheek by aninternal vertical ligamentous boundary. Thisboundary is located along the line formed bythe angulation of the underlying facial skele-ton at the superior temporal line, the lateralorbital rim, and at the lateral border of thebody of the zygoma. The key ligamentous at-tachments of the superficial fascia to the un-derlying skeleton occur along this line. Theimportant muscles of facial expression are lo-cated medial to this line, and it is here wheremost of the facial aging occurs.5,11,12
As surgery of the SMAS was originally de-scribed, the release was restricted to the outerpart of the face. Specifically, it did not release
the vertical ligamentous boundary to allow aneffect on the medial part of the cheek. Theextended SMAS technique, which was a keyevolution of SMAS surgery, continues the re-lease beyond this ligamentous line, i.e., it takes
FIG. 2. (Above) The lateral sweep deformity of the cheekthat can occur in SMAS flap surgery, despite vertical traction.This outcome occurs from the failure to properly release theanterior masseteric-cutaneous ligaments. These ligamentsare inherently stronger above, nearer the zygoma, and weakerbelow. Rotation of the more mobile lower part of the flapresults in an excessive posterior displacement, which con-trasts with the insufficient vertical lift. Point X, the pivot point,is the lowest intact ligamentous resistance. (Below) Completerelease of the midcheek retaining ligaments allows an evenredraping of the superficial fascia of the cheek in the direc-tion of the traction force.
Vol. 107, No. 6 / SURGERY OF THE SMAS 1547
up the release at the level at which it was dis-continued when performing the traditionalSMAS release.13
VECTORS: BASIC PRINCIPLES
According to Oxford, vector is defined as aquantity having direction as well as magnitude,denoted by a line drawn from its original to itsfinal position.
• In the face-lift context, a vector diagram maybe used to illustrate the force applied to theflap, or alternatively to illustrate the resultanteffect, namely the displacement of the flap.
• When a force is applied in a particular di-rection (e.g., vertical) the result is maximalin that direction, but there is also an effect atan angle to the primary force (Fig. 3, left).
• If the force is applied at an angle to thevertical, the resultant effect has both a ver-tical and horizontal component (Fig. 3).This effect can be demonstrated by use of
the X-Y coordinates of classic two-dimen-sional geometry. These show how the rela-tive distribution of effect between the verti-cal and horizontal varies according to theangle at which the force is applied. With a45-degree angle of traction, there is as muchvertical lift as posterior displacement (Fig. 3,right). Although vertical lifting is paramountfor a successful face lift, it is important torealize that a component of vertical lift alsooccurs with face-lift flaps, which have otherthan directly vertical traction. As a corollary,a major vertical lift can be achieved while atthe same time providing a significant com-ponent of posterior displacement. Whenoblique traction is applied to the lateral face(i.e., lateral to the body of the zygoma), thisreduces the distortions that are prone toresult from a purely vertical lift, such ascrowding of the lateral canthus crow’s foot,area, and excessive upward displacement ofthe sideburn.
FIG. 3. Classic two-dimensional geometry X-Y coordinates (length of arrow denotes magnitude offorce).(Left) Force vectors: I, vertical traction; II, force applied at an angle has a vertical component and ahorizontal component. The proportional distribution between vertical and horizontal varies according tothe angle of the primary vector. A vertical lift occurs without a directly vertical force. (Right) Movementvectors (length of arrow denotes magnitude of displacement): I, vertical displacement. II, Movement at anangle (green arrow) follows the direction of force if there is no restriction. There are accompanying vectorsof vertical and horizontal displacement. III, Restriction of the vertical displacement due to a partial,symmetrical resistance. Shaded arrow indicates the reduction from expected displacement. IV, Resistance todisplacement, which is unequal. The magnitude of displacement no longer relates just to the magnitudeand angle of the applied force. The unpredictable variable of the unseen and unequal resistance causes areduction of the expected displacement in one direction (vertical) more than the other (horizontal).
1548 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001
FIXATION
The dermis of the face is attached to thefacial skeleton by a multilink fibrous supportsystem that comprises the retaining ligamentsand the superficial fascia, which includes theSMAS and the retinacula cutis.11 A taut andintact retinacula cutis faithfully transmits theshape and movement of the superficial fasciato the skin. The function of the face imposesunique and conflicting requirements on its su-perficial fascia, namely the need for both fixa-tion and movement. The functions of facialexpression demand precisely controlled move-ment such as occurs with lip control in articu-lation. To restrict the amount of movement tothe degree intended and to the area of the faceintended, stability of the tissues is required,which takes the form of the deeper fixation ofthe superficial fascia. An example of the local-ization of movement is the prevention of trac-tion on the lower lid when the muscles aroundthe mouth contract. Strong fixation is also re-quired to resist the external forces of gravityand of traction, such as occurs in sleeping withthe cheek buried in a pillow.
The anatomic pattern of ligamentous fixa-tion of the superficial fascia to the facial skel-eton defines boundaries that compartmental-ize the face into several regions (Fig. 4). Threeof these are component parts of what is exter-nally visualized as the cheek, i.e., the lateralcheek and the prezygomatic and infrazygo-matic parts of the medial cheek, in addition tothe other regions, the lower lid, lower temple,
upper lid, and forehead. The stabilizing effectthat occurs at these ligamentous boundariesquarantines the movement resulting from mus-cle contraction within each region so that, atleast in youth, movement does not transmitinto the superficial fascia of adjacent areas.The ligamentous fixation has a shock absorber-like effect, which modulates the degree of tis-sue displacement upon muscle contraction.
The laxity that develops in the multilink fi-brous support system of the face is due to aprogressive weakening of the supporting con-nective tissue. This presumably arises from thecombination of intrinsic, age-related atrophyand degeneration of the connective tissue com-pounded by the “wear and tear” effect from therepeated displacement of the soft tissues con-sequent on the action of the facial muscles.Once some initial laxity develops, an exponen-tial effect would occur as the laxity places morestrain on the remaining and slowly diminishingligamentous support. Whereas, in youth a bal-ance exists between fixation and movement,the reduction of effective fixation means thatthe effect of the same muscle contraction tendsto produce a greater displacement of the softtissue with aging. The increased displacementfurther strains and weakens the ligamentoussupport.
These events would account for the acceler-ation of the rate of aging changes commonlyseen in a woman in about her mid-forties. Theyalso account for the apparent hyperactivity ofmuscle contraction, e.g., smile lines and gla-bella lines, at an age when muscle mass andstrength are, in fact, beginning to weaken. Ob-viously, the influence of gravity is the same inyouth as it is in age, but tissue displacementwith gravity is limited in youth. Descent of tis-sues from the effect of gravity only occurs whenthe tissues have become lax. The displacementof the tissues from gravity tends to furtherweaken the ligamentous support. Although thevertical descent of the face so characteristic ofaging14 reflects the obvious effect of gravity, thecause of the underlying laxity reflects the in-creasing mobility of the tissues as a result of themuscular activity rather than the laxity havingarisen primarily from the long-standing influ-ence of gravity (Fig. 5). Notwithstanding, thatlaxity can occur in the absence of muscle activ-ity (and muscle tone) as seen in long-standingfacial nerve palsy.
The direction of the weakening and of dis-placement of the connective tissues from repet-
FIG. 4. Regions of the face. Compartmentalization occursfrom the pattern of ligamentous fixation of the superficialfascia to the periosteum and deep fascia. The boundary ofeach region is formed by a ligament.
Vol. 107, No. 6 / SURGERY OF THE SMAS 1549
itive muscle shortening and stretching differsaccording to the configuration of each muscle(Fig. 6). For linear muscles, e.g., zygomaticusmajor and corrugator supercilii, the laxitytends to be parallel to the direction of short-ening of the muscle fibers. Whereas, for thosemuscles in which the fibers follow a curve, e.g.,orbicularis oculi pars orbitalis and medialplatysma, contraction of the muscle fiberscauses a radial, or centripetal displacementforce on the supporting connective tissue.Over time, medial platysma contraction even-tually pulls the supporting tissue away from thedepth of the neck concavity. It is not the mus-cle contraction that changes over time but thelaxity of the fascial support that allows theplatysma banding. Similarly, the part of orbic-ularis oculi that courses over the temple even-tually becomes displaced toward the lateralcanthus as a result of a weakening of its fibroussupport, as does the part of orbicularis oculithat directly overlies the body of the zygoma.The action of orbicularis oris, the most power-ful muscle of facial expression, is the major
factor contributing to laxity of the medialcheek, which is the most mobile and least sup-ported part of the face. The tissue displace-ment is directed medially, but when laxity de-velops, it is held up at the nasolabial furrow.
There are multiple vectors of displacementin the aging face. This is because each of themuscles of facial expression has its own direc-tion of connective tissue laxity. The correctionof each vector of displacement requires its ownvector of fixation. Fortunately, use of the SMASprovides increased opportunities for control-ling the directions of lift. This situation is quitedifferent from that in subcutaneous and sub-periosteal flap surgery in which a single, mostlyvertical, vector is used. Once the retaining lig-aments have been fully released, several ana-tomic regions have been entered into and havebecome as one. With the original, limited re-lease SMAS surgery, it was considered to be anadvantage to have two vectors; one directionfor the SMAS, and a different vector for theskin flap.15 When a properly released SMASflap is used, multiple vectors are possible.16,17
The use of multiple vectors enables the appro-priate vectors of correction for each region ofthe face.
If strong, nonabsorbable sutures are used forthe surgical fixation, what is effectively beingperformed is a replication of the original typeof ligamentous fixation akin to that in jointsurgery.17 These sutures can hold a substantial,ligament-like, strength into the superficial fas-cia if they are placed where the fascia is rein-forced. This reinforced area occurs where theretaining ligaments pass through the SMASinto the retinacula cutis. Rather than suturingthe mobilized SMAS to a mobile area, as occursin suturing to the nonmobilized SMAS, theSMAS flap can be fixed rigidly if it is suturedback to the appropriate part of the underlyingperiosteum or deep fascia. In restoring theanatomy of ligamentous fixation, the suturesappose the SMAS directly to the periosteum,which is in contradistinction to the use oflooped suspension sutures. The closer theforce point for application of tension to thefixation point on the skeleton, the less poten-tial for subsequent loss of position as a result ofrelaxation of the intervening bridge of SMAS.The use of multiple sutures spreads the loadand reduces the force per unit area at eachfixation point.
The sutures into the SMAS flap need not berestricted to the cut edge of the flap. With the
FIG. 5. The displacement of soft tissue that occurs underthe influence of gravity is conditional on laxity being present.The correction of laxity in the vector of displacement (seenhere as taking the slack out of the chain) nullifies the apparenteffect of gravity.
1550 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001
intact flap raised, the sutures can be placedthrough the underside of the appropriate partsof the flap. This method is not unlike theexternal SMAS technique where multiple su-tures are placed into the outer surface of theintact SMAS layer at selected locations. Thedirection of placement of each suture providesa directional effect to the connective tissuesupport.
The horizontal line of the zygomatic liga-ments is located in relation to the origins of thezygomatic and levator muscles of the upper lip(Fig. 4). As the series of suture/ligaments arereplaced along the lower part of the body ofthe zygoma, the ligamentous boundary separat-ing the prezygomatic and infrazygomatic re-gions is reconstituted. The orientation of eachsuture into the zygoma is parallel to the direc-tion of the fibers of each individual musclewhich, of course, varies (Fig. 7). Adjacent tolevator labii superioris, the vector of correctionis directly vertical, whereas laterally, the orien-tation of the sutures is more oblique commen-surate with the orientation of zygomaticus ma-jor. Accordingly, in the correction of themedial infrazygomatic cheek and nasolabialfold, there is not one but several vectors (Fig.7). Overlying the zygoma, the vectors for orbic-ularis oculi are more complex. Lateral to thelateral canthus, the sutures are oriented partlyparallel to the muscle fibers but with an out-ward vector. In the temple, the direction of thesutures follows the direction of the superiortemporal line to reverse the centripetal dis-placement of the muscle with its related con-nective tissue support. The sutures into thesuperficial fascia are placed in the connectivetissue of the SMAS between the muscles or intothe suborbicularis oculi fascia.
The periosteum of the zygoma varies in itsability to hold sutures. Where the periosteum isnot strongly attached to the bone, sutures areprone to cut through the weak periosteum orelse to detach the periosteum from the bone.
The Sharpey’s fibers from ligament and muscleorigins reinforce the periosteum as they coursethrough this layer to embed into the corticalbone. The much stronger periosteal attach-ment to the lower part of the zygoma enablesstrong fixation exactly where it is required, inthe vicinity of the zygomatic ligaments adjacentto the origins of the strong muscles to the lip.The other area of strengthened periosteum isalong the orbital rim where the arcus margina-lis is formed as a reinforcement of the perios-teum where it is fused with the periorbita andseptum orbitale.
The concept of positioning the fixation atthe location of the original ligamentous fixa-tion is quite different from that in the originalSMAS surgery, when the SMAS release was dis-continued before the midcheek ligamentswere exposed. The SMAS fixation in that situ-ation could only be peripheral and was undertension. Nowadays, with the recognition thatrelease of these ligamentous attachments is thekey to correction of the medial cheek, the fix-ation can also be at this level.
By reattaching the support of each anatomicregion separately to the facial skeleton at thelocation of the original ligamentous fixation,tension across the entire SMAS flap is avoided.An incremental recontouring of the shape ofthe face results. Tension is an anathema to acorrect result, because it produces a flatnesswith loss of contour.18 Such a flap would tentacross the depth of the infrazygomatic concav-
FIG. 6. Linear muscles undergo linear displacement oncontraction, whereas radial muscles undergo centripetaldisplacement.
FIG. 7. Vectors of fixation. Each arrow indicates a point ofsuture fixation of the superficial fascia to the periosteum. Thevector of each is opposite to the vector of displacement arisingfrom laxity.
Vol. 107, No. 6 / SURGERY OF THE SMAS 1551
ity and thin and flatten over the prominence ofthe zygoma.
Using multiple-level and central rather thanperipheral fixation allows the three-dimensionalshape of the face to be restored. This methodresults in an increased surface area of the face incontrast to the flattening and shortening effectassociated with straight out tightening proce-dures. There is a reduction in the amount ofredundant facial skin to be excised because ofthis recontouring as well as from the reduction ofskin closing tension in front of the ear.
SUMMARY
• The principles underlying SMAS face-lift sur-gery are different from those of traditionalface lifts.
• SMAS flap surgery works at the level atwhich mobility and aging laxity areoccurring.
• SMAS flaps tighten connective tissue laxityto reposition and restore tone to the super-ficial fascia. This approach reduces apparentmuscular hyperactivity.
• Complete SMAS release is necessary to avoidtension and distortion.
• SMAS flap fixation should replicate the orig-inal fixation of the superficial fascia.
• Nonabsorbable sutures mimic ligaments.• The fixation respects the natural boundaries
between facial regions.• Fixation at the several original locations
avoids the need for a mass tightening andflattening of the SMAS.
Bryan C. Mendelson, F.R.C.S.E., F.R.A.C.S.,F.A.C.S.
1. Skoog, T. Plastic Surgery: New Methods and Refinements.Philadelphia: Saunders, 1974.
2. Mitz, V., and Peyronie, M. The superficial musculoapo-neurotic system (SMAS) in the parotid and cheekarea. Plast. Reconstr. Surg. 58: 80, 1976.
3. Bosse, J. P., and Papillon, J. Surgical anatomy of theSMAS on the malar region. In Transactions of the 9thInternational Congress of Plastic and Reconstructive Sur-gery. New York: McGraw-Hill, 1987. P. 348.
4. Furnas, D. W. The retaining ligaments of the cheek.Plast. Reconstr. Surg. 83: 11, 1989.
5. Stuzin, J. M., Baker, T. J., and Gordon, H. L. The re-lationship of the superficial and deep facial fascias.relevance to rhytidectomy and aging. Plast. Reconstr.Surg. 89: 441, 1992.
6. Robbins, L. B., Brothers, D. B., and Marshall, D. M. An-terior SMAS plication for the treatment of prominentnasomandibular folds and restoration of normalcheek contour. Plast. Reconstr. Surg. 96: 1279, 1995.
7. Furnas D. W. Strategies for nasolabial levitation. Clin.Plast. Surg. 22: 265, 1995.
8. Hoefflin, S. M. The extended supraplatysmal plane(ESP) face lift. Plast. Reconstr. Surg. 101: 494, 1998.
9. Har-Shai, Y., Bodner, S. R., Egozy-Golan, D., et al. Me-chanical properties and microstructure of the super-ficial musculoaponeurotic system. Plast. Reconstr. Surg.98: 59, 1996.
10. Hamra, S. T. Frequent face-lift sequelae: Hollow eyesand the lateral sweep. Cause and repair. Plast. Reconstr.Surg. 102: 1658, 1998.
11. Mendelson, B. C. Extended sub-SMAS dissection andcheek elevation. Clin. Plast. Surg. 22: 325, 1995.
12. Moss, C. J., Mendelson, B. C., and Taylor, G. I. Surgicalanatomy of the ligamentous attachments in the tem-ple and periorbital regions. Plast. Reconstr. Surg. 105:1475, 2000.
13. Hamra, S. T. Deep-plane rhytidectomy. Plast. Reconstr.Surg. 86: 53, 1990.
14. Yousif, N. J. Changes of the midface with age. Clin. Plast.Surg. 22: 213, 1995.
15. Owsley, J. Q., Jr. Platysma-facial rhytidectomy: A pre-liminary report. Plast. Reconstr. Surg. 60: 843, 1977.
16. Owsley, J. Q. SMAS-platysma facelift: A bidirectionalcervico facial rhytidectomy. Clin. Plast. Surg. 10: 429,1983.
17. Mendelson, B. C. SMAS fixation to the facial skeleton:Rationale and results. Plast. Reconstr. Surg. 100: 1834,1997.
18. Little, J. W. Volumetric perceptions in midfacial agingwith altered priorities for rejuvenation. Plast. Reconstr.Surg. 105: 252, 2000.