National costing report: Lower limb peripheral arterial disease (August 2012) 1 of 24 Costing report Lower limb peripheral arterial disease Implementing NICE guidance NICE clinical guideline 147 August 2012
Transcript
National costing report: Lower limb peripheral arterial disease (August 2012) 1 of 24
Costing report
Lower limb peripheral arterial disease
Implementing NICE guidance
NICE clinical guideline 147
August 2012
National costing report: Lower limb peripheral arterial disease (August 2012) 2 of 24
This costing report accompanies the clinical guideline: ‘Lower limb peripheral arterial disease: diagnosis and management’ (available online at www.nice.org.uk/guidance/CG147).
Issue date: August 2012
This guidance is written in the following context
This report represents the view of NICE, which was arrived at after careful consideration of the available data and through consulting with healthcare professionals. It should be read in conjunction with the NICE guideline. The report is an implementation tool and focuses on the recommendations that were considered to have a significant impact on national resource utilisation.
Assumptions used in the report are based on assessment of the national average. Local practice may be different from this, and the impact should be estimated locally.
Implementation of the guidance is the responsibility of local commissioners and/or providers. Commissioners and providers are reminded that it is their responsibility to implement this guidance, in their local context, in light of their duties to avoid unlawful discrimination and to have regard to promoting equality of opportunity. Nothing in the costing assessment should be interpreted in a way that would be inconsistent with compliance with those duties
National Institute for Health and Clinical Excellence Level 1A City Tower Piccadilly Plaza Manchester M1 4BT
National costing report: Lower limb peripheral arterial disease (August 2012) 6 of 24
1.3.2 The incidence of peripheral arterial disease increases with age.
Other risk factors include smoking, diabetes mellitus, pre-existing
cardiovascular disease, renal insufficiency and a sedentary
lifestyle. Men are more likely to be affected by peripheral arterial
disease.
1.3.3 The symptoms of peripheral arterial disease include pain on
exercise (intermittent claudication), pain while resting (critical limb
ischaemia), skin ulceration and gangrene. All people with
peripheral arterial disease are at increased risk of mortality,
myocardial infarction and stroke.
1.3.4 Table 1 shows the prevalence in England of peripheral arterial
disease, intermittent claudication and critical limb ischaemia among
people aged 60 years or over.
Table 1 Number of people in England aged 60 years and over with peripheral arterial disease
Proportion of people
Number of people
Population of England 51,573,132
People aged 60 years and over 11,536,529
People aged 60 years or over with peripheral arterial diseasea
20% 2,307,306
People with peripheral arterial disease who have symptoms of intermittent claudicationb
25% 576,826
People with intermittent claudication who are likely to develop critical limb ischaemiaa
20% 115,365
a. Taken from ‘Lower limb peripheral arterial disease: diagnosis and management’ (NICE clinical guideline 147). b. Taken from ‘Cilostazol, naftidrofuryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication in people with peripheral arterial disease’ (NICE technology appraisal guidance 223).
1.3.5 As the prevalence of peripheral arterial disease is significantly
greater in people aged 60 years and over, only this group are
National costing report: Lower limb peripheral arterial disease (August 2012) 8 of 24
1.4.7 There has been a move away from invasive investigations for
people who are referred to secondary care, with catheter
angiography being replaced by duplex ultrasonography, magnetic
resonance angiography or computed tomography angiography.
Treadmill walking tests and segmental pressures are other
commonly used investigations.
1.4.8 Endovascular treatments include balloon angioplasty, endovascular
stents and a range of new adjunct or alternative treatments and
techniques such as drug-eluting stents, modified balloons, laser
angioplasty, atherectomy, cryotherapy and brachytherapy.
1.4.9 Surgical reconstruction may be carried out to unblock or bypass
occluded or narrowed arteries.
1.4.10 There has been a recent trend towards increasing
subspecialisation of vascular surgery and this is likely to continue.
The increasing development of multidisciplinary teams is likely to
accompany this, and such teams will already be available in many
of the centres that currently provide a full vascular service. There
will continue to be a small number of centres where there are
general surgeons with a vascular interest working in relative
isolation. These centres may be affected to a greater extent by the
recommendations in the guideline, as more changes to practice are
likely to be needed to allow multidisciplinary working.
2 Costing methodology
2.1 Process
2.1.1 We use a structured approach for costing clinical guidelines (see
appendix A).
2.1.2 We have to make assumptions in the costing report. These are
tested for reasonableness with members of the Guideline
National costing report: Lower limb peripheral arterial disease (August 2012) 9 of 24
Development Group (GDG) and key clinical practitioners in the
NHS.
2.2 Scope of the cost-impact analysis
2.2.1 The guideline offers best practice advice on the diagnosis and
management of lower limb peripheral arterial disease.
2.2.2 The guideline does not cover:
acute ischaemia of the lower limb
methods of amputation
rehabilitation after amputation
management of diabetic foot problems
use of topical treatments and dressings.
Therefore, these issues are outside the scope of the costing work.
2.2.3 Rather than cost each individual recommendation, costing work
has focused on the areas that will potentially need the most
resources to implement or generate the biggest savings. These
areas were determined in discussion with the clinical guideline
project team and the members of the GDG.
National costing report: Lower limb peripheral arterial disease (August 2012) 10 of 24
3 Analysis of the potential resource impact
Table 2 Analysis of the potential resource impact of recommendations
Recommendation type
Recommendation numbers
Expected to have a resource impact?
Information requirements
1.1.1–1.1.2 Information provision is expected to form part of routine healthcare practice. Any impact on time and resource use is expected to be minimal and would be likely to be offset by an improvement in quality of life.
Secondary prevention of cardiovascular disease in people with peripheral arterial disease
1.2.1 See section 3.1 below.
Diagnosis 1.3.1–1.3.3 There are not expected to be significant costs associated with implementing the recommendations on diagnosis. Ankle brachial pressure index is typically performed by a practice nurse or podiatrist while taking a clinical history. It may add between 5 and 15 minutes to the time needed for the clinical examination. The Guideline Development Group considered the incremental resource needs associated with measuring ankle brachial pressure index to be small compared with the benefit of accurately identifying people with suspected peripheral arterial disease. Accurate diagnosis would be expected to improve quality of life and reduce costs by ensuring that the person’s condition is managed appropriately.
Imaging for revascularisation
1.4.1–1.4.3 See section 3.2.
Management of intermittent claudication
1.5.1–1.5.8 In general, the recommendations in this section are not expected to be significantly different from current practice. However, there will be some degree of regional variation and there will be differences between larger centres that provide a full vascular service and smaller units. The recommendation on supervised exercise is discussed in section 3.3.
Management of critical limb ischaemia
1.6.1–1.6.11 The recommendations on multidisciplinary teams and revascularisation are not expected to be
National costing report: Lower limb peripheral arterial disease (August 2012) 11 of 24
significantly different from current practice. However, there will be some variation between larger centres that provide a full vascular service and smaller units. Vascular multidisciplinary teams currently exist in many organisations and therefore it is expected that new teams will not need to be formed to implement the recommendation relating to this. However, more formal network meetings and increased communication between existing staff may be needed. Drug treatment included in the recommendations is not expected to be significantly different from current practice. Chemical sympathectomy is not considered here as it is recommended in the context of clinical trials only.
See section 3.4 for discussion about the costs of major amputation.
3.1 Secondary prevention of cardiovascular disease in
people with peripheral arterial disease
Recommendation 1.2.1
Offer all people with peripheral arterial disease information, advice, support
and treatment regarding the secondary prevention of cardiovascular disease,
in line with published NICE guidance on:
smoking cessation
diet, weight management and exercise
lipid modification and statin therapy
the prevention, diagnosis and management of diabetes
the prevention, diagnosis and management of high blood pressure
antiplatelet therapy.
Background
3.1.1 Peripheral arterial disease is strongly associated with
cardiovascular disease, and the modifiable and non-modifiable risk
factors are the same for both conditions. Many people with
peripheral arterial disease will have evidence of cardiovascular
National costing report: Lower limb peripheral arterial disease (August 2012) 12 of 24
disease, and people diagnosed with peripheral arterial disease are
at high risk of further cardiovascular events such as stroke and
myocardial infarction.
3.1.2 Treatments for secondary prevention of cardiovascular disease are
less commonly offered to people with peripheral arterial disease
than to people with other cardiac and cerebrovascular risk factors.
3.1.3 The GDG recognised that there are existing NICE
recommendations covering the secondary prevention of
cardiovascular disease that are relevant for people with peripheral
arterial disease. These recommendations should be applied when
treating people with peripheral arterial disease to avoid
inconsistency.
3.1.4 Appropriate and consistent implementation of NICE
recommendations on the secondary prevention of cardiovascular
disease may have a high impact on patient outcomes and help to
reduce variations in care and outcome.
Potential costs
3.1.5 There may be additional costs associated with providing the
infrastructure for information, advice, support and treatment
because of staff time, materials, drug costs and other services.
3.1.6 The approximate numbers of people likely to need information,
advice, support and treatment for the secondary prevention of
cardiovascular disease in line with existing NICE guidance in each
of the recommended areas is shown in table 3.
National costing report: Lower limb peripheral arterial disease (August 2012) 13 of 24
Table 3 Prevalence of peripheral arterial disease and number of people who would be affected by the recommendation on secondary prevention of cardiovascular disease
Risk factor Prevalence for people with peripheral arterial disease based on data from 2011/12a (%)
Approximate number of people aged 60 years or over with peripheral arterial disease plus risk factorb
Smoker 9.7 55,952
Obesity 28.3 163,242
Raised cholesterol 20.0 115,365
Statin therapy 68.3 393,972
Type 2 diabetes 53.9 310,909
High blood pressure 62.9 362,824
Antiplatelet therapy 51.2 295,335 a Prevalence data, based on the ICD-10 definition of peripheral arterial disease, were taken
from the IMS disease Analyzer (Information Centre: unpublished data 2012), which collects data from a sample of GP practice systems. Around 100 are currently delivering data and the database has about 2.7 million patient records, around 0.85 million of which were registered for the whole of the study year (2011/12). b Percentage prevalence applied to the number of people aged 60 years or over with
symptoms of intermittent claudication (576,826 people, taken from table 1).
3.1.7 Some elements of these interventions could be provided in primary
care, reducing costs associated with referring people to vascular
surgical units in secondary care for advice and support. Table 4
shows that an outpatient appointment in secondary care costs
significantly more than an appointment in primary care.
Table 4 Costs of appointments for people with peripheral arterial disease in primary and secondary care
Appointment Cost (£)
Primary care
Surgery appointment with a GP lasting 11.7 minutes 36a
Clinic appointment with a GP lasting 17.2 minutes 53a
Secondary care – Vascular surgery treatment function 107
WF01B first attendance 234b
WF01A follow-up attendance 116b
a From personal social services research unit – unit costs of health and social care 2011
(Curtis, 2011). Includes qualification costs. b From payment by results tariff for 2012/3.
National costing report: Lower limb peripheral arterial disease (August 2012) 14 of 24
3.1.8 The cost of implementing the recommendation about secondary
prevention of cardiovascular disease is not quantified in this report.
Some people with peripheral arterial disease are likely to be
receiving such information, advice, support and treatment already,
but for many people this could represent a change to current
practice. Local commissioners and providers are advised to
consider current provision of services for secondary prevention of
cardiovascular disease and the varying needs of people with
peripheral arterial disease in order to assess the potential costs of
implementing the recommendation.
3.2 Imaging for revascularisation
Recommendations 1.4.1–1.4.3
Offer duplex ultrasound as first-line imaging to all people with peripheral
arterial disease for whom revascularisation is being considered.
Offer contrast-enhanced magnetic resonance angiography to people with
peripheral arterial disease who need further imaging (after duplex ultrasound)
before considering revascularisation.
Offer computed tomography angiography to people with peripheral arterial
disease who need further imaging (after duplex ultrasound) if
contrast-enhanced magnetic resonance angiography is contraindicated or not
tolerated.
Background
3.2.1 Assessment by diagnostic imaging is indicated in people with
peripheral arterial disease when interventional treatment is being
considered.
3.2.2 The choice of imaging modality used will be influenced by local
expertise and the availability of imaging equipment. Less invasive
and lower cost strategies are generally preferred.
National costing report: Lower limb peripheral arterial disease (August 2012) 15 of 24
3.2.3 GDG opinion is that the recommendations are likely to reflect
current practice in some centres, although not all centres will offer
imaging techniques in the order set out in the recommendations.
Potential costs
3.2.4 Implementation of the guideline will not result in a resource impact
for many centres, but for some centres there may be implications
for training and the availability of expertise and experience. Costs
associated with these should be determined locally.
3.2.5 The costs of the imaging techniques included in the
recommendations are shown in Table 5. Costs are taken from the
payment by results tariff for 2012/3.
Table 5 Cost of imaging techniques
HRG description HRG code
Cost (£)
Duplex ultrasound
Ultrasound – less than 20 minutes RA23Z 47
Ultrasound – more than 20 minutes RA24Z 63
Contrast-enhanced magnetic resonance angiography
Magnetic Resonance Imaging Scan, one area, pre and post contrast
RA03Z 207
Magnetic Resonance Imaging Scan, two - three areas, with contrast
RA05Z 213
Computed tomography angiography
Computerised Tomography Scan, one area, pre and post contrast
RA10Z 108
Computerised Tomography Scan, two areas with contrast
RA12Z 130
Computerised Tomography Scan, three areas with contrast
RA13Z 144
3.2.6 For people in whom revascularisation may be beneficial, duplex
ultrasound is the least costly and least invasive method of
determining the location and extent of the lesion, and may provide
sufficient information. If the results of duplex ultrasound are not
suitable for planning an intervention, contrast-enhanced magnetic
resonance imaging or computed tomography angiography can
provide more detailed information.
National costing report: Lower limb peripheral arterial disease (August 2012) 16 of 24
Potential savings
3.2.7 There may be savings in centres that do not currently use duplex
ultrasound for first-line imaging, as this is the least costly method.
3.2.8 The imaging techniques included in the recommendations are
considered by the GDG to be the most cost-effective. The
avoidance of unnecessary reduplication of imaging will save time
and cash resources.
3.3 Supervised exercise programmes
Recommendations 1.5.1–1.5.2
Offer a supervised exercise programme to all people with intermittent
claudication.
Consider providing a supervised exercise programme for people with
intermittent claudication which involves:
2 hours of supervised exercise a week for a 3-month period
encouraging people to exercise to the point of maximal pain.
Background
3.3.1 Supervised exercise is not defined in the recommendations, but is
likely to be a community-based exercise programme supervised by
healthcare professionals.
3.3.2 The GDG agreed that the risks associated with a supervised
exercise programme for people with peripheral arterial disease are
minimal, while the benefits include an increase in walking distance,
quality of life and a decreased risk of cardiovascular events.
3.3.3 Based on experience of GDG members, no more than 30% of
people with intermittent claudication are currently offered the
opportunity to participate in a supervised exercise programme. Of
those who do have the opportunity, less than half choose to join an
exercise programme.
National costing report: Lower limb peripheral arterial disease (August 2012) 17 of 24
3.3.4 Based on information provided by GDG members, supervised
exercise programmes aimed at people with peripheral arterial
disease are typically supervised by 2 physiotherapists and have
approximately 10 people per group. The programme consists of
approximately 2 hours of classes per week for 3 months in an
outpatient setting. People exercise until the onset of symptoms,
then rest. They may walk on treadmills or outside, complete
circuits, etc. The details are likely to vary between supervised
exercise programmes.
3.3.5 At the end of a programme, people are then encouraged to
exercise independently.
3.3.6 Other exercise programmes also exist and may include different
amounts of support, such as regular telephone calls, an exercise
diary or an education component. The GDG noted that increased
support may encourage people to follow unsupervised exercise
programmes.
Potential costs
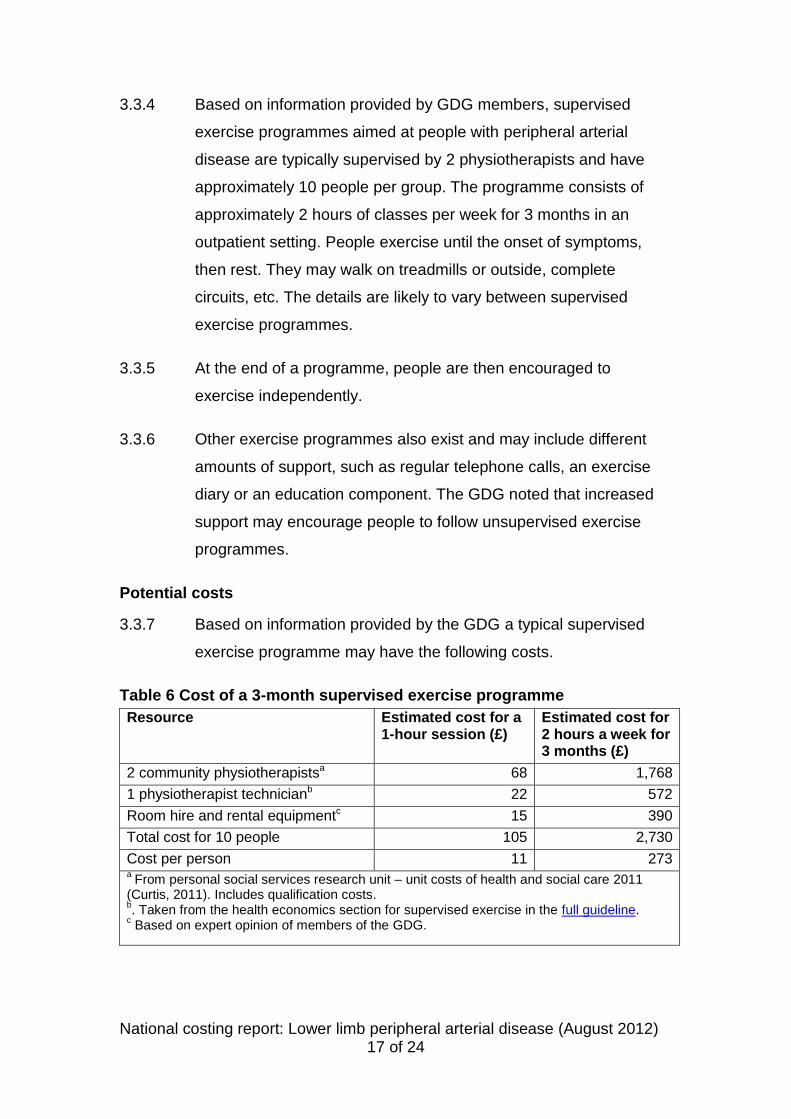
3.3.7 Based on information provided by the GDG a typical supervised
exercise programme may have the following costs.
Table 6 Cost of a 3-month supervised exercise programme
Resource Estimated cost for a 1-hour session (£)
Estimated cost for 2 hours a week for 3 months (£)
2 community physiotherapistsa 68 1,768
1 physiotherapist technicianb 22 572
Room hire and rental equipmentc 15 390
Total cost for 10 people 105 2,730
Cost per person 11 273 a From personal social services research unit – unit costs of health and social care 2011
(Curtis, 2011). Includes qualification costs. b. Taken from the health economics section for supervised exercise in the full guideline.