Pete Dodd TB background TB today TB natural history HIV TB in kids Overview Approach Results Drug-resistant TB Definitions & data Algorithm Results Latent TB ARI trends Prevalence Mortality Conclusion 1 Counting children with TB: the role of modelling. CHE seminar, York Thursday, 19 January 2017 Health Economics & Decision Science School of Health & Related Research University of Sheffield
Transcript
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
1
Counting children with TB:the role of modelling.CHE seminar, York
Thursday, 19 January 2017
Health Economics & Decision ScienceSchool of Health & Related ResearchUniversity of Sheffield
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
2
Overview
This talk:
• Step through various aspects of TB natural history and epi• Burden estimation for paediatric TB• Drug-resistance patterns in children• Modelling to inform the burden of latent infection• Modelling the burden of TB mortality in children
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
3
TB history
Figure: TB in the UK (credit: HPA)
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
4
TB Globally
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
1990 1995 2000 2005 2010 2015year
Glo
bal T
B in
cide
nce
WHO regionAFRAMREMREURSEAWPR
WHO GTB estimates, 2015
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
5
TB Globally
TB incidence(per 100,000y)
0 − 50 50 − 100100 − 200200 − 300300 − 400500 − 852 No data
WHO GTB estimates, 2015
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
6
What makes TB different?
Distinction between infection and disease
Most infections do not result in disease.
Figure: Tuberculin skin test for latentM.tb infection(credit:Greg Knobloch)
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
7
What makes TB different?
Delays to disease
Fast and slow.
187Natural history of TB
0 10 20Age at infection (years)
(a)
d p(a
,0)
1·000
0·410
0·1300·0860·028
0 1 2 3 4 5Years since ‘conversion’
“Rel
ativ
e ris
k”
1·0
0·8
0·6
0·4
0·2
00 10 20 30 40 50 60 70 80 90
Age (years)
Prop
ortio
n sp
utum
-pos
itive
(d+(
a))
1951–53
Value used in model1960–62
1954–561963–66
1957–591967–69
(b)
(c)
Fig. 2. (a) Relationship between the risk of developing the first primary disease episode and the age at infection assumed inthe model. The relationship (i) between the risk of developing exogenous disease and the age at reinfection, and (ii) betweenthe risk of developing endogenous disease and the current age of an individual are assumed to follow this basic pattern. Notethat the rates of disease onset for 10–20 year olds can be expressed in terms of those for individuals aged 0–10 years, andthose aged over 20 years. (b) Observed and assumed relationship between the rate at which individuals experience their firstprimary episode}exogenous disease in each year following infection}reinfection relative to that during the first year afterinfection}reinfection. These were estimated from the distribution of the time interval between ‘tuberculin conversion’ anddisease onset of those who were tuberculin-negative at the start of the UK MRC BCG trial [34]. The ‘relative risk’ for a givenyear after ‘conversion’ is taken to be the ratio between: (i) the proportion of the total disease incidence among initiallytuberculin-negative individuals which occurred in that year following ‘conversion’, and (ii) the corresponding proportionwhich occurred during the first year after ‘conversion’. (c) Observed and assumed proportion of total respiratory diseaseincidence among cases of age a attributable to sputum-positive forms, d
+
(a). All lines (excluding the heavy solid line) showthe relative contribution of sputum-positive disease to age-specific notifications of pulmonary tuberculosis in males inNorway (1951–69). Source: Dr K. Styblo (TSRU) and Dr K. Bjartveit (Norwegian National Health Screening Service).
Figure: Vynnycky & Fine, 1997
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
8
What makes TB different?
Reinfection
Reinfection puts individuals at renewed risk of TB disease, withpartial protection from previous infection.
Figure 1, Risk of tuberculosis infection in the Netherlands (1880-1970) (showing annual percentage decreases in og risk).
The incidence of clinical tuherculosis in the Netherlands, 1951 to 1970 Tuberculosis incidence rates are available in the Netherlands for males and females separately in each of the above age-groups for each of the years 1951 to 1970. Immigrants (non-Dutch nationals) and cases of tuberculosis among them were excluded from the incidence data from 1965 onwards (the numbers previously were small). The rates are tabulated for all forms of tuberculosis, for all forms of pulmonary tuberculosis, for bacillary pulmonary tuberculosis and for smear-positive pu{monary tuberct~losis, The a~alyses below are coniined to two of these clinical categories, namely to "all forms of pulmonaw tuberculosis', which is the major type of the disease, and to 'bacillary pulmonary tuberculosis', namely the epidemiologieally important sub-group of infectious cases.
In all, therefore, there are 11 9 20 .-220 linear equations for each sex, from which to estimate the risks of development of each type of clinical tuberculosis, In addition to separate estimates of the risks for males and for females, estimates for both sexes were also calculated from the pooled data, that is from all 440 equations.
Results Risks of development of tuberculosis in the two sexes Table i shows the estimated risks of developmerlt of tuberculosis according to the history of infection. The estimated risks of development of all forms o[ pulmonary tuberculosis, expressed as annual percentages, are considerably greater following recent primary infection (5.06 for males, 5.85 for females) than following the recent reinfection of a subject with a distant primary infection (1.91 and 1.1 0 respectively). These estimates, in turn, are much greater than
Fig. 2. (a) Relationship between the risk of developing the first primary disease episode and the age at infection assumed inthe model. The relationship (i) between the risk of developing exogenous disease and the age at reinfection, and (ii) betweenthe risk of developing endogenous disease and the current age of an individual are assumed to follow this basic pattern. Notethat the rates of disease onset for 10–20 year olds can be expressed in terms of those for individuals aged 0–10 years, andthose aged over 20 years. (b) Observed and assumed relationship between the rate at which individuals experience their firstprimary episode}exogenous disease in each year following infection}reinfection relative to that during the first year afterinfection}reinfection. These were estimated from the distribution of the time interval between ‘tuberculin conversion’ anddisease onset of those who were tuberculin-negative at the start of the UK MRC BCG trial [34]. The ‘relative risk’ for a givenyear after ‘conversion’ is taken to be the ratio between: (i) the proportion of the total disease incidence among initiallytuberculin-negative individuals which occurred in that year following ‘conversion’, and (ii) the corresponding proportionwhich occurred during the first year after ‘conversion’. (c) Observed and assumed proportion of total respiratory diseaseincidence among cases of age a attributable to sputum-positive forms, d
+
(a). All lines (excluding the heavy solid line) showthe relative contribution of sputum-positive disease to age-specific notifications of pulmonary tuberculosis in males inNorway (1951–69). Source: Dr K. Styblo (TSRU) and Dr K. Bjartveit (Norwegian National Health Screening Service).
Figure: Vynnycky & Fine, 1997
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
10
What makes TB different?
Duration of disease
Figure: Indian National Tuberculosis Institute, Bull. WHO (51), 1974.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
11
What makes TB different?
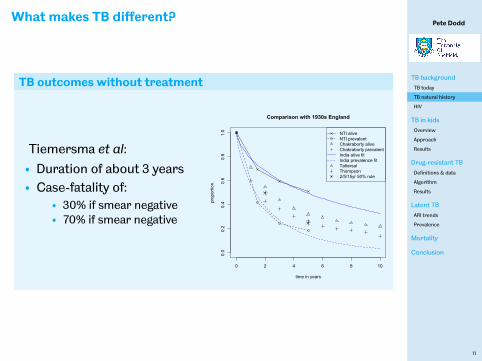
TB outcomes without treatment
Tiemersma et al:• Duration of about 3 years• Case-fatality of:
• shorter in duration• more likely to result in death• less infectious
Outcomes with TB treatment are still good…
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
15
What makes TB different?
Summary:
• Distinction between infection and disease:• most infections do not result in disease• disease may result after a long delay• but is more likely after a short one• with age-dependent characteristics
• Reinfection:• individuals may be infected again• but appear to have partial protection from developingdisease
• heterogeneity in infectiousness (& diagnosability)• interactions with HIV (& diabetes, BMI, smoking, …)• rareness and difficulty in diagnosing infection→uncertainty in epi/natural history
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
16
Styblo
Figure: Karel Styblo,1921-1998: the ‘fatherof TB control’
• ARI of 1% corresponds withsmr+ incidence 50/100,00 per yearI.e.β ≈ (1%/y)/(2y× 50× 10−5/y) = 10 y−1
• With a 10% lifetime risk of disease, 50%of it smear positive1 smr+ case→ 20 infections→ 2 cases =1 smr+ caseI.e. Stable situation, Rn = 1
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
17
TB in children‡
‡with James Seddon @ Imperial
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
18
Background
Tuberculosis in kids
• Children are at higher risk of developing disease soon afterinfection
• Children are at higher risk of extrapulmonary disease,and are much less infectious
• Difficult diagnosis & low chance of transmission has led toneglect by public health community
• 1st time 2012:GTB @WHO estimate global burden for kids
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
19
TB GloballyBOX 2.2
The burden of TB disease among childrenFor many years, the prevention, diagnosis and treatment of TB among children have been relatively neglected. Greatest attention has been given to the detection and treatment of infectious cases, most of which occur in adults. The Stop TB Strategy launched by WHO in 2006 includes case-fi nding in high-risk or vulnerable groups such as children and prevention of TB in children who live in the same household as newly detected TB cases. To help to address the burden of TB in children (defi ned as those aged <15 years) and monitor progress, robust data on childhood TB are necessary. This is the fi rst WHO report on global TB care and control to include estimates of the burden of TB disease among children, with best estimates of 490 000 cases and 64 000 deaths per year.1 The reasons why it remains diffi cult to estimate the burden of TB disease in children, the methods used to produce this fi rst set of estimates and the next steps needed to improve them are discussed below.
Challenges in assessing the number of TB cases and deaths among childrenThere is no easy-to-use and accurate diagnostic test for TB in children. Most children have paucibacillary TB that is harder to diagnose with sputum smear microscopy and culture. Many children, especially younger children, are also not able to expectorate sputum. Diagnosis is usually made using a combination of clinical (as opposed to laboratory) criteria and a non-specifi c test for tuberculous infection, but there is no universally applied diagnostic algorithm. The defi nitive diagnosis of extrapulmonary TB requires specialised services that are usually available only in referral hospitals, and thus often not accessible to those in need. Besides diagnostic challenges, children diagnosed with TB are not always reported to national surveillance systems because of the lack of linkages among individual paediatricians, paediatric hospitals and national TB programmes, and data from national surveys including children are limited. Many countries lack VR systems in which deaths from TB are disaggregated and reported by age.
Estimates of TB noti! cations and TB incidence in children in 2011 – methods and resultsThe global number of new TB case notifi cations among children (aged <15 years) is estimated at 327 000 in 2011 (Table B2.2.1). This includes cases reported among children and an estimate of the number of cases among children in countries that did not report notifi cations disaggregated by age. For countries that did not report age-disaggregated data (Figure B2.2.1), it was assumed that the child:adult ratio among notifi ed cases was the same (for each case type) as the ratio in countries that did report notifi cations disaggregated by age (an alternative method using the assumption that the child:adult ratio of notifi cation rates was the same gave
similar results). WHO does not request age-disaggregated data for relapse cases or those reported as of unknown treatment history; the number of children in these categories was assumed to be zero.
To estimate TB incidence among children, it was assumed that the ratio of notifi ed to incident cases at the global level in 2011 (best estimate 66%, range 64%–69%) was the same for adults and children. On this basis, TB incidence among children was estimated at 490 000 (range, 470 000–510 000) in 2011, equivalent to about 6% of the total number of 8.7 million incident cases.
Limitations of the methods used include:
! The assumption that the ratio of notifi ed to incident cases is the same for adults and children, in the absence of any data on levels of under-reporting of diagnosed cases for children and adults separately;
! The assumption that reported cases were true cases of TB. Misdiagnosis is possible, especially given the diffi culties of diagnosing TB in children; and
! The proportion of cases among children may be different in countries for which age-disaggregated data are not available.
Estimates of TB mortality in children in 2011 – methods and resultsMortality data disaggregated by age from VR systems that have been reported to WHO were analysed. TB death rates per 100 000 population were calculated for children and adults, after adjustment for incomplete coverage and ill-defi ned causes (see Annex 1 for further details). For countries without VR data, an ecological statistical model was used to predict the ratio of childhood to adult TB mortality rates. The model included a set of risk factors known to be associated with TB mortality (for example, GDP per capita, the percentage of new cases with MDR-TB, HIV prevalence in the general population and the treatment success rate). The total number of deaths from TB among HIV-negative children was estimated at 64 000 (range, 58 000–71 000) in 2011, equivalent to 6% of the 990 000 TB deaths among HIV-negative TB cases in 2011. The main limitation in the methods is that the countries reporting usable VR data were all middle or high-income countries. Predictions for low-income countries had to be extrapolated from these countries.
Besides the direct impact of TB on children themselves, parental deaths from TB have created large numbers of orphans. In 2009, there were almost 10 million children who were orphans as a consequence of losing at least one of their parents to TB.
Estimates of TB prevalence in children Data on the prevalence of TB in children are limited to a few
nationwide surveys conducted before 2001. Examples include a survey in India in 1956, and surveys in China in 1980, 1990, and 2000. The 2007 survey in the Philippines included children aged 10–14 years. These surveys consistently found a low burden of bacteriologically-confi rmed TB in children compared with adults.
There has been impressive progress in the implementation of nationwide prevalence surveys to measure bacteriologically-confi rmed TB since 2008 (see Section 2.5.2). These surveys are focusing on adults (aged !15 years) and the typical sample size is 50 000–
14 WHO REPORT 2012 GLOBAL TUBERCULOSIS CONTROL
TABLE B2.2.1 Reporting of TB case notifi cations disaggregated by age, 2011
SMEAR-POSITIVE SMEAR-NEGATIVEa EXTRAPULMONARY
Total notifi cations 2 621 049 1 872 745 813 636Countries disaggregating by age 2 601 032 1 582 235 684 233Countries not disaggregating by age 20 017 290 510 129 403(% total notifi cations disaggregated) (99%) (84%) (84%)
Number of countries that reported notifi cations disaggregated by age (number of HBCs)b 197 (22) 171 (15) 171 (15)
Total estimated childhood notifi cations 327 000
a This includes reported cases for whom smear results were unknown or smears were not done.b An additional 9 countries reported zero TB cases in 2011 and two countries had not reported data to WHO
by July 2012.
1210.0020_P_001_272.indd 14 03/10/12 21:53
Figure:WHO TB report 2012
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
20
Overview∗
Comments:
• Starting from adult estimates allows comparison withdirect estimates from child notifications.
• Uncertainty in every stage needs to be appropriatelydescribed and propagated.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
20
Overview∗
Comments:
• Starting from adult estimates allows comparison withdirect estimates from child notifications.
• Uncertainty in every stage needs to be appropriatelydescribed and propagated.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
21
Overview
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
22
Data inputs
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
23
Demography
Afghanistan Bangladesh Brazil Cambodia China
Democratic Republic of Congo Ethiopia India Indonesia Kenya
Mozambique Myanmar Nigeria Pakistan Philippines
Russian Federation South Africa Thailand Uganda United Republic of Tanzania
Viet Nam Zimbabwe
010002000300040005000
0
5000
10000
15000
0
5000
10000
15000
0
500
1000
1500
0e+00
5e+04
1e+05
0
3000
6000
9000
0
5000
10000
0250005000075000
100000125000
05000
10000150002000025000
0
2000
4000
6000
01000200030004000
010002000300040005000
0
10000
20000
05000
100001500020000
0
3000
6000
9000
0
4000
8000
12000
0
2000
4000
0
2000
4000
0
2000
4000
6000
0
2000
4000
6000
8000
0
2500
5000
7500
0
500
1000
1500
2000
0−4
5−9
10−
1415
−19
20−
2425
−29
30−
3435
−39
40−
4445
−49
50−
5455
−59
60−
6465
−69
70−
7475
−79
80−
0−4
5−9
10−
1415
−19
20−
2425
−29
30−
3435
−39
40−
4445
−49
50−
5455
−59
60−
6465
−69
70−
7475
−79
80−
Age
Num
ber
(tho
usan
ds)
2010
data: UN ESA Population Division
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
24
TB prevalence
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
Afghanistan
Bangladesh
Brazil
Cambodia
China
Democratic Republic of Congo
Ethiopia
India
Indonesia
Kenya
Mozambique
Myanmar
Nigeria
Pakistan
Philippines
Russian Federation
South Africa
Thailand
Uganda
United Republic of Tanzania
Viet Nam
Zimbabwe
0 500 1000TB prevalence per 100,000
coun
try
2010
data: WHO
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
25
Infection risks
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
26
Infection risks
0.00
0.05
0.10
0.15
0.20
0 5 10 15Transmission parameter, β
dens
ity
Styblo/β
• Styblo’s rule of thumb was that asmear-positive case of TB infectedabout 10 individuals per year(β ∼ 10yr−1)
• Modern reviews of theARI:prevalence ratio have foundlower values (e.g. Bourdin Trunzet al., van Leth et al.).
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
27
Progression
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
28
Progression
Risks of disease following infection
Separated by 5 age groups and type of disease:
age quantity median LQ UQ0 probability of disease 0.500 0.298 0.7021 probability of disease 0.215 0.108 0.360
2-4 probability of disease 0.016 0.002 0.0645-9 probability of disease 0.001 0.000 0.01310-14 probability of disease 0.110 0.043 0.2190 probability disease is EP 0.255 0.112 0.4511 probability disease is EP 0.295 0.107 0.557
2-4 probability disease is EP 0.060 0.017 0.1455-9 probability disease is EP 0.085 0.029 0.18310-14 probability disease is EP 0.000 0.000 0.008
distributions based on Marais et al., 2004 review of thepre-chemotherapy literature.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
29
BCG
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
Afghanistan
Bangladesh
Brazil
Cambodia
China
Democratic Republic of Congo
Ethiopia
India
Indonesia
Kenya
Mozambique
Myanmar
Nigeria
Pakistan
Philippines
Russian Federation
South Africa
Thailand
Uganda
United Republic of Tanzania
Viet Nam
Zimbabwe
70 80 90 100% BCG coverage in 2010
coun
try
data: WHO
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
30
BCG
Modelling approach
• Wemodelled BCG protection for EPTB ≥ PTB
quantity median LQ UQProtection against EPTB 70% 52% 84%Protection against PTB 54% 38% 69%
• We considered a model variant where 41% of protectionwaned towards the equator.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
31
HIV
●
●
●
●
●
●
●
●
●
Democratic Republic of Congo
Ethiopia
Kenya
Mozambique
Nigeria
South Africa
Uganda
United Republic of Tanzania
Zimbabwe
1 2 3 4Percent of those aged <15 years with HIV (%)
coun
try
Modelling approach
• Effect modelled as an IRR:
median LQ UQ20.000 10.118 39.261
based on few studies.• Age distribution, ART, householdclustering all neglected.
HIV prevalence data: UNAIDS AIDSinfo
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
32
Results
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
33
TB incidence: top 50 countries, 2014
Russian FederationDemocratic People's Republic of Korea
www.thelancet.com/lancetgh Published online July 9, 2014 http://dx.doi.org/10.1016/S2214-109X(14)70245-1 5
association between tuberculosis burden in adults and children by setting means these countries are likely to have a higher proportion of global paediatric tuberculosis, extrapolation of our approach would suggest a global burden that is up to 25% higher than our prediction for the 22 HBCs.
Our model has identifi ed large populations that could benefi t from preventive treatment, although not all children would be eligible. In view of the effi cacy of isoniazid preventive therapy,21,22 children who progress to disease after household exposure should be thought to have developed preventable tuberculosis; screening of individuals sharing a household with an adult who has been diagnosed with tuberculosis and treatment of child contacts would probably substantially reduce the numbers of children who develop the disease. The large numbers predicted by our model also represent the present and accumulated result of a failure to identify and treat adults with tuberculosis eff ectively.
These estimates of child tuberculosis burden are somewhat higher than those in the 2012 WHO report,6 similar to the notifi cation-based estimates of Nelson and colleagues (although these estimates are from more than 10 years ago),23 and lower than the value of 1 million cases suggested by some commentators24,25 and the estimates of Jenkins and colleagues.26 The comparison of notifi cations and model estimates suggests under-reporting, most notably in children younger than 5 years. However, some countries do have notifi cation rates similar to estimated incidence. Further investigation is necessary to improve understanding of the reasons for the diff erence between the number of estimated and notifi ed cases in every country. In our model, India had by far the highest burden of paediatric tuberculosis, which is probably a result of its large size, demographic composition, and moderate tuberculosis prevalence.
The proportion of tuberculosis burden occurring in children has frequently been used to estimate probable paediatric burden where direct measurements do not exist.6 Local estimates for the proportion of tuberculosis burden in children vary widely, with some investigators reporting up to 39% of the burden in children.27 Donald28 pointed out that increased proportions would be expected in countries where overall burden is highest, because of the correlation with younger-skewed demographics. He also noted that a high force of infection leads to a younger average age at infection, when risks of progression are highest.28 Our model reproduces this expected trend, with proportions predicted in a similar range to estimates by Nelson and colleagues.23 However, the countries with the largest contribution from HIV to tuberculosis incidence (South Africa and Zimbabwe) do not follow this pattern, refl ecting the lower HIV prevalence in children than adults.
As with any model, our approach involved assumptions and has limitations. The limiting assumptions were
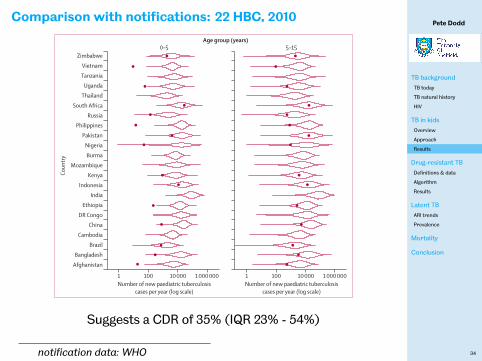
Figure !: Violin plot comparing model estimates of paediatric tuberculosis incidence in 2010, with numbers of cases in each age group reported to WHO by each countryDots show the numbers of cases reported to WHO. The absence of a dot means paediatric notifi cations were not reported by that country in 2010. The violins give a visual representation of the range and distribution of model estimates for each country on the basis of the community model. DR=Democratic Republic.
Figure ": Numbers of new paediatric tuberculosis cases in 2010, by countryEstimates were calculated with the community model. Error bars show IQRs. DR=Democratic Republic.
ZimbabweVietnamTanzania
UgandaThailand
South AfricaRussia
PhilippinesPakistan
NigeriaBurma
MozambiqueKenya
IndonesiaIndia
EthiopiaDR Congo
ChinaCambodia
BrazilBangladesh
Afghanistan
1 100 10 000 1 000 000 1 100 10 000 1 000 000
Coun
try
Number of new paediatric tuberculosiscases per year (log scale)
Number of new paediatric tuberculosiscases per year (log scale)
0–5 5–15Age group (years)
Zimbabwe
Vietnam
Tanzania
Uganda
Thailand
South Africa
Russia
Philippines
Pakistan
Nigeria
Burma
Mozambique
Kenya
Indonesia
India
Ethiopia
DR Congo
China
Cambodia
Brazil
Bangladesh
Afghanistan
0 100 000 200 000
Coun
try
Median number of new paediatric tuberculosis cases per year
Suggests a CDR of 35% (IQR 23% - 54%)
notification data: WHO
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
35
Pattern by incidence
Articles
6 www.thelancet.com/lancetgh Published online July 9, 2014 http://dx.doi.org/10.1016/S2214-109X(14)70245-1
approximations in representation of HIV infection in children and uncertainties surrounding the nature, size, and variation of protection conferred by BCG vaccination.
We did not have data for the age distribution of HIV infection in children, antiretroviral therapy coverage, or CD4 cell count in infected individuals; we treated HIV infection as one risk factor uniformly spread between children. Exposure to M tuberculosis and infection were not aff ected by HIV in our model, but, in reality, household clustering of HIV means that children with HIV infection could be expected to have more exposure to tuberculosis than do children without HIV infection. Although the crudeness of the approach to HIV means that our conclusions for countries with high HIV prevalences should be treated with caution, the estimate that HIV contributes to 5% of the total incidence means that this issue is likely have little eff ect on the overall estimate.
The effi cacy of BCG vaccination and the causes of recorded variability remain controversial,18 and could be aff ected by the variation in vaccine strain used.29 In addition to incorporation of uncertain distributions that characterise the effi cacy of BCG vaccination against pulmonary and extrapulmonary tuberculosis, we considered structural model variants with unvarying BCG effi cacy by latitude. This approach might refl ect an interpretation that perceived variation of BCG vaccination effi cacy is due to masking by heterologous immunity from non-tuberculous mycobacteria. Overall disease estimates were 27% lower under this assumption (infection estimates were unaff ected).
Neither our model nor the studies on which estimates of progression were based diff erentiated between M tuberculosis infection and a positive test of M tuberculosis sensitisation. Some children are anergic and can progress to tuberculosis without ever showing evidence of sensitisation. Risks of progression were based on reports from the early 20th century in white people and might not fully apply to populations that we assessed, which can diff er systematically in factors aff ecting risks of progression, such as host genetics, dominant M tuberculosis strain types, malnutrition, or vitamin D levels. We did not consider possible correlations between risk of exposure and infection, did not take account of any previous infection protecting against reinfection, and assumed that risks of progression were concentrated in the 1–2 years after infection. We did not consider subnational heterogeneity in transmission of tuberculosis, assuming that risks of infection were proportional to prevalence. Although some of this variation will average out for overall estimates, it could be important for specifi c countries and country-level estimates, which should therefore be viewed with caution.
All model variants started from WHO estimates of adult tuberculosis prevalence, and therefore inherited their limitations. The most recent underlying demographic data were for 2010, and so we used tuberculosis, HIV, and BCG vaccination estimates for that year. We did not consider transmission of M tuberculosis from children, diff erentiate between drug-resistant and drug-susceptible tuberculosis, or include preventive treatment.
Figure !: Proportion of total tuberculosis burden that occurs in children and tuberculosis incidence in 2010 for 22 high-burden countriesProportions are based on mean model estimates from the community method. Incidences are based on WHO point estimates. DR=Democratic Republic.
Afghanistan
Bangladesh
Brazil
Cambodia
China
DR Congo
Ethiopia
India
Indonesia
Kenya
Mozambique
Burma
Pakistan
Philippines
Russia
South Africa
Thailand
Uganda
Tanzania
Vietnam
Zimbabwe
0 300 600 9000
5
10
15
20
Prop
ortio
n of
tube
rcul
osis
incid
ence
in ch
ildre
n ag
ed <
15 ye
ars (
%)
Tuberculosis incidence per 100 000 per year
Panel: Research in context
Systematic reviewWe did a literature review of English language publications in PubMed, employing no date restrictions. Search terms included combinations of “mycobac*”, “tuberc*”, “tb”, “child*”, “ped*”, “paed*”, “burden”, “epidemiology”, “global”, “model”. We identifi ed no previous studies which had used a mechanistic model to estimate the burden of tuberculosis in children. In our model, we used o! cial estimates from WHO, the UN, DHS data and UNAIDS, and combined them with several systematic reviews to inform transitions. The reviews by Bourdin Trunz and colleagues8 and Van Leth and colleagues9 informed the association between tuberculosis prevalence and force of infection. The review by Fox and colleagues12 informed risk of infection after household exposure, and the review by Marais and colleagues15 informed the risk of progression to disease after infection. The e" ect of BCG vaccination was informed by several reviews and the e" ect of HIV was informed by the study from Hesseling and colleagues.20
InterpretationOur model predicts that about 650 000 children developed tuberculosis in 2010 in the 22 countries with a high burden of the disorder. Because our estimates do not use paediatric notifi cations as a starting point, the estimates can be compared with reported cases in each country to identify shortfalls. Our model also identifi es vast numbers of children predicted to be exposed to tuberculosis every year and the even greater number of children who harbour latent tuberculosis infection.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
36
Results
Summary (2014)
quantity measure median LQ UQinfection incidence/yr 9.0 million 6.9 million 11.7 millioninfection prevalence 62.9 million 49.1 million 81.1 milliondisease incidence/yr 827,000 547,000 1,238,000
• Method used in combination with notification-basedapproach for WHO estimates in past 2 years.
• Most recently, estimate was 1 million (0.9m - 1.1m) cases inchildren.
• Only around 1/3 of children with TB are diagnosed andnotified
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
37
Limitations (& opportunities)
Many limitations…
Key limitations
• Inherits any limitations of WHO TB prevalence estimates.• Uncertainties in parameters around progression andtransmission.
• Variation in BCG efficacy.• Simplified treatment of HIV.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
38
Drug-resistant TBin children*
*with Babis Sismanidis @WHO & James Seddon @ Imperial
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
39
Drug-resistance
Background
• Around 5% of all incident TB is multi-drug resistant (MDR)• ∼ 111K of 480K were started on appropriate treatment• Cost of treatment 50 - 200 × higher than DS-TB
Approach
• Surveillance & survey data on DR in adults• Sample uncertainty from numbers• Nearest-neighbour based resampling when data missing
• DS - susceptible to isoniazid and rifampicin;• HMR - isoniazid mono-resistant;• RMR - rifampicin mono-resistant;• MDR - multidrug-resistant (resistant to at least isoniazidand rifampicin);
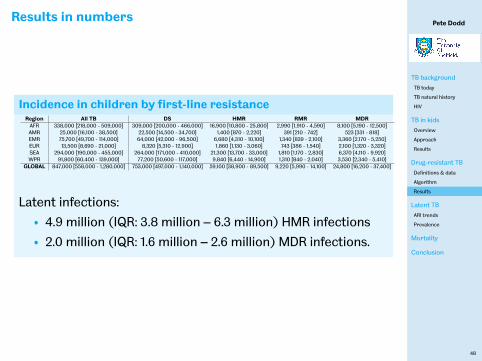
• Current LTBI→ TB incidence of• 15 / 100,000 y in 2035• 9 / 100,000 y in 2050
• 10 per million y 2050 elimination target needs to addressLTBI
• 97 m (92m - 103m) children under 15 infected
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
61
TB mortality in children§(draft & not for dissemination)
§work with Courtney Yuen@ Harvard, Babis Sismanidis @WHO,James Seddon @Imperial, & Helen Jenkins @ Boston U.
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
62
Methods
…redacted untilpublication…
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
63
Conclusion
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
64
Acknowledgements
Thanks to collaborators:
• James Seddon @ Imperial• Rein Houben @ LSHTM• Babis Sismanidis @WHO• Helen Jenkins @ Boston University• Courtney Yuen @ Harvard• Andy Prendergast @ QMUL, Beate Kampmann @ Imperial,& Claire Beecroft @ ScHARR
Special thanks also to:• TB Alliance for funding• the DRTB surveillance unit at WHO for data, advice andreview
Pete Dodd
TB background
TB today
TB natural history
HIV
TB in kids
Overview
Approach
Results
Drug-resistant TB
Definitions & data
Algorithm
Results
Latent TB
ARI trends
Prevalence
Mortality
Conclusion
65
References
Including me…
• P.J. Dodd, A.J. Prendergast, C. Beecroft, B. Kampmann, J.A. Seddon, The impact of HIV and antiretroviral therapy on TBrisk in children: a systematic review and meta-analysis, Thorax, 2017, doi:10.1136/thoraxjnl-2016-209421 [inpress]
• R.C. Harris, P.J. Dodd, RG White, The potential impact of BCG vaccine supply shortages on global paediatrictuberculosis mortality, BMC Medicine, 2016, doi:10.1186/s12916-016-0685-4
• R.M.G.J. Houben and P.J. Dodd, The global burden of latent tuberculosis infection - a re-estimation usingmathematical modelling, PLOS Medicine, 2016, doi:10.1371/journal.pmed.1002152
• P.J. Dodd, C. Sismanidis, J.A. Seddon, Global burden of drug-resistant tuberculosis in children: a mathematicalmodelling study, Lancet Infectious Dis, 2016, doi:10.1016/S1473-3099(16)30132-3
• J.A. Seddon, H.E. Jenkins, L. Liu, T. Cohen, R.E. Black, T. Vos, M.C. Becerra, S.M. Graham, C. Sismanidis, Countingchildren with tuberculosis: why numbers matter, P.J. Dodd, Int J Tuberc Lung Dis 2015, doi:10.5588/ijtld.15.0471
• P.J. Dodd, E. Gardiner, R. Coghlan, J.A. Seddon, Estimating the burden of childhood tuberculosis in the twenty-twohigh-burden countries using mathematical modelling study, Lancet Global Health, 2014,doi:10.1016/S2214-109X(14)70245-1
Other:• Jenkins HE, Yuen CM, Rodriguez CA, Nathavitharana RR, McLaughlin MM, Donald P, Marais BJ, Becerra MC,Mortality in
children diagnosed with tuberculosis: a systematic review and meta-analysis., Lancet Infectious Dis,2016,doi:10.1016/S1473-3099(16)30474-1
• Yuen CM, Jenkins HE, Rodriguez CA, Keshavjee S, Becerra MC,Global and Regional Burden of Isoniazid-ResistantTuberculosis., Pediatrics, 2015,doi:10.1542/peds.2015-0172
• Jenkins HE, Tolman AW, Yuen CM, Parr JB, Keshavjee S, Pérez-Vélez CM, Pagano M, Becerra MC, Cohen T,Incidence ofmultidrug-resistant tuberculosis disease in children: systematic review and global estimates., Lancet,2014,doi:10.1016/S0140-6736(14)60195-1










































































![Modelling TB and Atherosclerosis using Multi-Agents · Modelling TB and Atherosclerosis using Multi-Agents Jaspreet Deo ... (TB) simulation. Although paper [1] provided details of](https://static.documents.pub/doc/80x56/5f0b18bb7e708231d42ed4dc/modelling-tb-and-atherosclerosis-using-multi-modelling-tb-and-atherosclerosis-using.jpg)






