26
Integrating Data into Practice: Project 1: Assertive Self Care by Chris Potter, M.Ed. December, 2014
| Date post: | 09-Aug-2015 |
| Category: |
Documents |
| Upload: | chris-potter |
| View: | 17 times |
| Download: | 1 times |

Integrating Data into Practice:
Project 1: Assertive Self Care
by Chris Potter, M.Ed.December, 2014

Assertive Self-CareA Solution Focused Coping Skill
approach for therapists designed for clients with Depression or Anxiety
Assisting your client to build coping skills using a Solution Focused Approach
Developed by Chris Potter M.Ed.

What we’ve learned as psychotherapists treating adults in community health settings:
• Individuals often overlook their own abilities and resources when depressed or anxious
• The majority of acute mental health episodes are triggered by extreme stress or conflict
• With guidance and support, individuals can learn to better manage stress and conflict using there own strengths and abilities
• Additional coping tool suggestions can augment these abilities, and can reinforce a client’s confidence

Common Factors in determining positive therapeutic outcomes
• Meta-analysis of research has indicated 4 primary factors contributing to positive outcomes:
1. Clinical relationship2. Client Factors – bio/psycho/social3. Expectancy – (of treatment effectiveness)4. Mastery of problems (strategies that aid patient in
overcoming problems and stress)

Solution Focused Self Care Approach
• Emphasis on Solution focused Therapy reinforcing use of coping strategies
• Two packets are available on ‘Stress’ and ‘Conflict’ Management
• Weekly goals are set by client to build ‘Self Care’ skills
• Patient is encouraged to keep a diary of strategies used and their effect
• Patient ‘self evaluation’ is completed each appointment to evaluate impact

Protocols – 1st visit1. Administer the Self Evaluation Tool to identify client
distress: levels of depression or anxiety, and initial coping ability
2. Review results with patient3. Discuss treatment protocol: Solution Focused Self Care,
care Coordination, and medication options4. Develop Treatment plan with client, focusing on Stress or
Conflict Management (based on SET & interview)5. Develop an initial ‘Self Care Plans’ with the client,
highlighting use of ‘Coping Strategy Tasks’ 6. Schedule follow up appointment within 2 weeks to a month

Protocols – 2nd – 6th visit
• Administer & review the Self Evaluation Tool• Review outcomes and ‘Self Care Plans’• Use SFSC note template to frame next self-care
task• Reinforce strengths and successes• Determine if continuation of SFSC would be
beneficial• Consider offering Alternate Stress or Conflict
Management’ packet if necessary

Self Evaluation Tool* Name: Date:
How much is each of the following bothering you?
0- None
1- Little
2-Moderate
3- Much
4-Very Much
1 Sleep Problems Hours per night: _____ Sp
2 Depression, down mood, hopelessness Dp
3 Anxiety, nervousness, or fears Ax
4 Mood swings, ups and downs Ms
5 Intense anger or irritability Ag
6 Problems concentrating on what you’re doing Cn
7 Thoughts of physically harming yourself Si
8 Recurring thoughts that you feel you can’t control Ob
9 Actions you do over and over that you can’t control Cm
10 Impulsive actions: doing things before thinking Im
11 Unexplainable voices, images, or sensations OP
12 Concerns over your health Sm
How well are you able to: 0-Very Poorly 1-Poorly 2-Fair 3-Well 4-Very Well
1) Manage your time: balancing ‘work and self-care’ 2) Relax: distract yourself from negative thinking 3) Counsel yourself: encourage yourself, finding hope 4) Deal with feelings: ask yourself what you need 5) Overcome problems: focusing on goals and progress 6) Say what you want and don’t want from others

S.E.T. Review* Name: Date: time: Session #: ____
In the past 2 weeks, how well have you: Very Poorly Poorly Fairly well Well Very Well 1) Managed your time: balancing ‘work and self-care’ 0 1 2 3 4
2) Relaxed: distract yourself from negative thinking 0 1 2 3 4
3) Counseled yourself: encourage yourself, finding hope 0 1 2 3 4
4) Dealt with feelings: ask yourself what you need 0 1 2 3 4
5) Overcome problems: focusing on goals and progress 0 1 2 3 4
6) Said what you wanted and didn’t want from others 0 1 2 3 4
How often do you use street drugs? 4 More, 3 Daily, 2 Weekly, 1 Monthly, 0 Don’t
How often did you have over 2 alcoholic drinks? 4 More, 3 Daily 2 Weekly, 1 Monthly, 0 Didn’t
How likely are you to do something that may cause harm to yourself or others? 4 Very likely, 3 Likely, 2 Possibly, 1 Not very likely, 0 Not likely at all
How uncomfortable are you, physically? 4 Extremely, 3 Very, 2 Somewhat, 1 Slightly, 0 Not
Your work status: 4 Employed, 3 Looking, 2 In School/Training, 1 Not looking, 0 On Disability
Do you think things will improve? 4 Very likely, 3 Likely, 2 Possibly, 1 Not likely, 0 No way
How much: Very Little Little Some Much
Very Much
A) Has your therapist understood and been able to help you 0 1 2 3 4
B) Has Medication helped not on meds not taking meds as prescribed 0 1 2 3 4
C) Have you been able to use your resources and support from others 0 1 2 3 4
D) Have you been using Coping Strategies (skills) 0 1 2 3 4
Describe what you think has helped you to feel better, get things done, or take better care of yourself? What’s your current plan to feel better, get things done, or take better care of yourself?

*Assertive Self-Care
Learning to manage Depression and Anxiety by using Effective Coping Tools
The National Institute of Mental Health estimates that 23% of United States Citizens suffer from depression, anxiety, or other mood disorders: 9.5 % depression related, and 13.3% are anxiety related. Anxiety and depression can be triggered by extreme stress or conflict, but can also be a result of biological factors and poor coping skills.
The good news is: there is effective treatment for depression and anxiety! Treatment may include a combination of medication, therapy, and your efforts toward developing effective coping skills. Medication can help reduce levels of depression or anxiety, but development of coping skills can help you manage depression and anxiety by learning to better handle stress and conflict. Psycho-therapy can help you to understand triggers to mood problems, and to find coping tools that can help you feel and function better. A ‘coach’, or a supportive friend, can help you to practice these coping tools on a regular basis. With persistence and practice, you can win the battle against depression and anxiety!
Depression is ‘a deep sadness and hopelessness’. It can interfere with your ability to enjoy life, to sleep or eat well, to concentrate, to perform normal tasks, and to handle relationships. It can literally affect your desire to ‘go on’, and in severe cases, can lead to Suicidal Thinking
Anxiety is an overwhelming feeling of fear or nervousness, of worry or panic. This can be fueled by uncontrollable fears about the future, people, or certain situations. Anxiety is accompanied by physical sensations: rapid heart beat, breathlessness, choking, nausea, shakiness, or irritability. It often triggers the desire to avoid situations due to fears or anxiety.
Stress is an inner tension caused by major changes or losses in life, or by high expectations. Examples: death or loss of a loved one, changes in your job, finances, health, or relationships.
Conflict is a problem between two ‘conflicting’ beliefs or desires. This can occur between you and someone else (interpersonal conflict), or within yourself (internal conflict).
Depression and Anxiety are both affected by stress and conflict Stress and Conflict can be managed by developing Coping Strategies

Assertive Self Care is a Solution Focused approach, building upon your strengths and skills to better handle stress and conflict in you life. This can help to improve your mood, overall. It involves use of a ‘Self-Care Plan’ on a weekly basis, highlighting your strengths/successes, your goal, and the coping tasks that might help you over the upcoming week. You are encouraged to have a ‘Coach’, or a ‘support person’, to help you stay focused on your goals, successes, and coping tools that have been helpful. Each ‘Self-Care Plan’ has daily tasks for you to practice so you can learn to better cope with stress and conflict. Each evening you can track your progress by writing in a ‘Self-Care Diary’, noting how Coping strategies affected your mood.
The Assertive Self-Care Strategies are focused on: Stress Management:
CS 1: Managing your time: pacing yourself, balancing ‘work and self-care’ CS 2: Relaxing yourself: letting go of tension, using your senses to distract yourself CS 3: Counseling yourself: encouraging yourself, focusing on strengths, perspective, and hope
Conflict Management: CS 4: Speaking out: stating what you feel, think, and want, (or don’t want), using ‘I’ statements CS 5: Solving Problems: focusing on goals, working through problems, noticing progress as you go CS 6: Expressing your feelings: using ‘feeling words’, asking yourself what you need to feel better CS 7: Working out conflict: finding common goals, solving problems together, using consequences
At the end of each week, review the comments and your Self-Care Diary. You can then decide which strategies have been most helpful, and what to focus on for the upcoming week. Your ‘Coach’ can help you to recognize successes, and encourage you to keep practicing. Good luck! Remember, success comes with practice, encouragement, and patience. Give yourself credit for all of your efforts and successes!

Assertive Self-Care treatment protocols Proposed by Chris Potter 10/25/2006
1. Choose candidates with Adjustment or Mood Disorder and no imminent self-harm risk factors 2. Use Outcomes Assessment Tool at intake and at each session 3. Treatment Plan objectives should indicate Solution Focused Therapy with Coping Skill Development
Therapists, Care Coordinators, and Prescribers need to buy off on Solution Focused, Coping Strategy Approach Use of terminology – ‘Solution Focused questioning’ and ‘Coping Strategies (strengths, skills)’ Reinforcement of strengths, successes, use of supports, and use of coping strategies Treatment course expectation: within 1 – 4 months. Continual emphasis on moving toward ‘less intensive level of care’ Use of Client Self Evaluation and Clinician Rating of Progress tools for measuring mental status changes.
Treatment Course Example: 1. Initial Assessment - treatment planning – Initial Self Care Plan developed, Referrals made (PCP, etc)
filter out clients more appropriately served by other Evidence Based Approaches orientation to Solution focus, Coping Strategy treatment process – info/SC plan given Use Self Evaluation Tool and Resource Needs Assessment Develop Risk Management Plan for clients at higher risk – incorporating support systems
2. Therapy Services Emphasizing Solution Focused approach Reinforcing Strengths, supports, and encouraging development of Coping Tools Set up 2-5 therapy appointments (moving to ½ hour appointments by 3rd – 5th session) Standardized Treatment Note used to reflect EBP, Progress (data driven), and GAF
3. Care Coordination – scheduled appointment within next week: Supports Self Care Plan (integrated into Treatment Plan)
i. check in with client on Alternative weeks to therapy appointments Provides resource development
i. Assist in finding or coordinating with PCP ii. Look at integrating available supports into treatment process
4. Psychiatric involvement on ‘as need basis’ Bridging medication from hospitalizations Provide ‘stabilization and consultation’ for PCP
5. Therapist, and/or Care Coordinator offer ‘Stress/Conflict management groups as needed 6. Discussion of After Care Plan (ongoing Self-Care Plan) started at session ‘2’ 7. Client encouraged to complete treatment per outreach by Care Coordinators (GAF of ‘55 – 60’ considered
treatment success if no ‘high risk factors’ are present)

Outcome Examples:Change over Treatment Course
- 2005 Outpatient CMH cases5
7%
69%
61%
57%
17%
8%
14%
14%
13% 16%
34% 3
8% 44%
36%
30%
18%
28%
20%
27%
27%
0%
100%
Sleep
Distur
banc
e
Depre
ssion
Anxiet
y
Moo
d ins
tabil
ity
Time
Man
agem
ent
Relaxa
tion
Self E
ncou
rage
men
t
Feelin
g Res
olutio
n
Proble
m S
olving
Asser
tiven
ess
% o
f c
lien
ts w
ith
se
lf-r
ati
ng
s o
f '3
- 4
'
68
67 3.5
Session 1 'N' =
49% 16%
0%
50%
100%
Solution Focused - Stressmanagement
Solution Focused - Conflictmanagement
Per
cen
tag
e o
f cl
ien
ts
'N'/Average session number =

14
Assertive Self-CareAssertive Self-Care By Chris Potter, M.Ed.
Treating Mental Health Patients Treating Mental Health Patients in the PCP Settingin the PCP Setting
Applying Patient Self-Guided Counseling and Applying Patient Self-Guided Counseling and Outcome Analysis ToolsOutcome Analysis Tools
20042004

04/15/23 15
Treatment Effectiveness with Limited Resources
• Evaluating Outcomes:– The benefits or collecting, analyzing, and
integrating outcome data into practice– The Use of Client Report and Clinical Data
• Comparing Intervention Effectiveness– Medications– Behavioral Interventions:
• PCP vs. Mental Health Professional Facilitated • Patient Self Guided Counseling (SGC)

16
Utilization Management: Who does it?EST – Empirically Supported Treatments
Also known as ‘Evidenced Based Treatments’UM references for authorizations of Tx. Manualization of Tx. - Not geared toward clinical settings Limited treatment modalities authorized Ignorance of coexisting conditions
Effectiveness Research: outcome analysis Intervention effectiveness – in practice Clinician/Client rating tools: symptom rating scales, Beck, OQ -45.2, Self Evaluation Tool Comparison Groups:
Profiles Interventions: Medication/Behavioral Interventions Dx. Groups Outcome Groups

17
Utilization Management: • per case, per group• Caseload data sets: entire caseload vs. subgroups
– Demographic Groups– Diagnostic Groups – Outcome Groups
• Treatment Motivation• Symptom Distress• Functioning ability• Treatment Prognosticators• Coping Strategy Utilization• Change attribution• Treatment Response ‘Common Factors’

Client Sessions - 2003
16
13
6
2
5 5
4
3
4 4
1
2
0
2 2
10
6
8
6
4
7 7
4
2
1
0 0
1
0 0
0
10
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15Session Number
Num
ber o
f clie
nts
GAF 55 or less
GAF 60 or more
Number of Adult clients attending therapy by session
number per GAF group
Since most adult clients tend to stay in therapy less that 5 sessions, the treatment plan should emphasize higher impact interventions early in treatment. I made sure my client left each session with something to use, to read, or to attend to. This reality reinforced the application of Solution Focused Treatment techniques.
Percentage of all clients seen at session # with GAF 60 or more - 2003
38%
32%
57%
75%
44%
58%
64%
57%
33%
20%
0%
50%
100%
1 2 3 4 5 6 7 8 9 10
Session number
Percentage of Adult clients with a GAF score of at least ’60’, attending therapy
by session number

19
Major DX Groups at Session 1
17
12
3 3
5
0
4
0 00
2
4
6
8
10
12
14
16
18
Depression Anxiety Mood Swing Attention Deficit Personality AdjustmentDisorder
Alcohol/Drug Psychotic Other
Clients at Session 1: GAF 55 or less
Clients at Session 1: GAF 60 or more

20
Self rating of Symptom Distress - 2002
2.22.6 2.6
3.02.5 2.4
2.8
1.8
2.5
1.4 1.4 1.5 1.6 1.71.3
1.51.2
1.4
0.0
2.0
4.0
Self
Rat
ing
0(no
ne) -
4(s
ever
e)
68
65Clients with GAF 55- N=Clients with GAF 55- N=
21
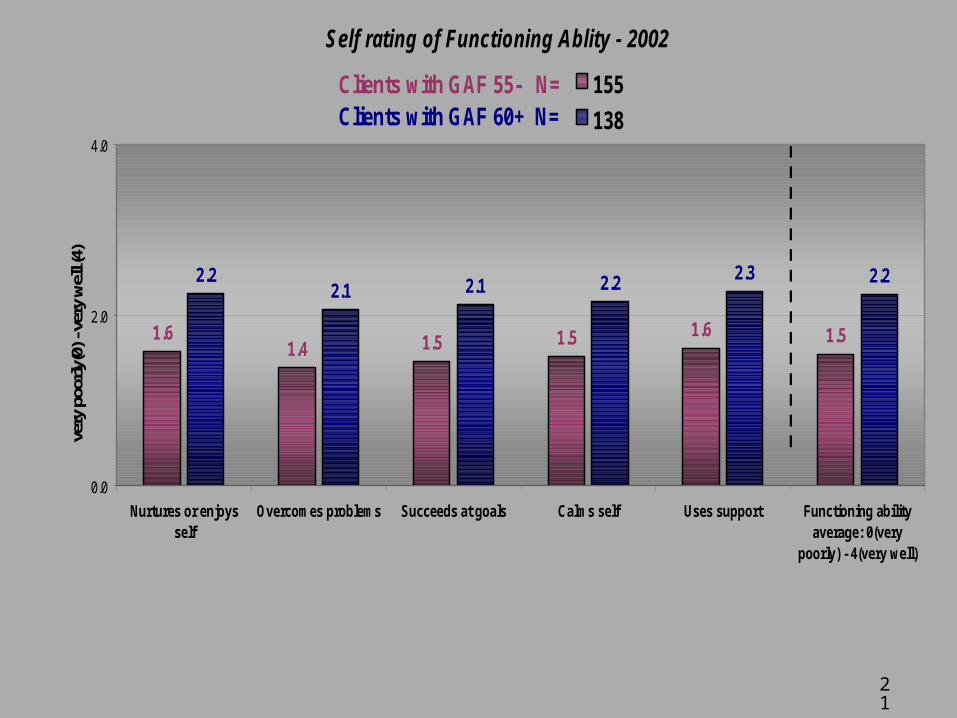
Self rating of Functioning Ablity - 2002
1.61.4 1.5 1.5 1.6 1.5
2.22.1 2.1 2.2 2.3 2.2
0.0
2.0
4.0
Nurtures or enjoysself
Overcomes problems Succeeds at goals Calms self Uses support Functioning abilityaverage: 0(very
poorly) - 4(very well)
very
poo
rly(0
) - v
ery
wel
l (4)
155
138
Clients with GAF 55- N=Clients with GAF 60+ N=

22
Reason for seeking Treatment: 2003 assessments
82%
29%
53%47%
35%
6%
45%
27%
45%
73%
45%
27%
0%
50%
100%
feel better get medication get therapy learn to cope withstress
work on relationshipproblems
unsure - told to comein
Res
po
nd
ant
Per
cen
tag
e
Reasons seeking treatment
GAF 55 or less:GAF 60 or more:

23
Mental Status change attributes - 2003
79%
77%
30%
19%
21%
30%
16%
64%
80%
57%
33% 41
%
64%
41%
0%
20%
40%
60%
80%
100%
Perc
enta
ge o
f ses
sion
s en
dors
ed
GAF 55- GAF 60+

24
Average Severity of obstacles to successful treatment: 2003 assessments
0.6
1.5 1.4
2.5
3.0
2.4
1.5
0.2
0.80.5
1.5
2.6
0.5
1.4
0.81.1
0.30.5 0.6
0.7
0.30.5
0.70.5 0.5
1.8
1.1
0
2
4
Risk of harmto self orothers
Dissatisfactionwith mental
healthtreatment
Alcohol orDrug useproblems
Physicalhealth issues
Major stress Low motivationto learn skills
Vocationalproblems
Poor supportnetwork
Average Tx.obstacle score
Treatment obstacles
Clie
nt s
elf r
atin
gs: 0
(no
obst
acle
) -
4(se
vere
obs
tacl
e)GAF 55 or less GAF 60 or more
Standard Deviation

25
Symptom Distress and Functioning level vs. Therapeutic interventions 2.
5
2.1
1.9
1.6
2.3
1.2
1.9 2.
1 2.4
1.8
1.8
1.6
2.0
2.0
1.6
1.6 1.
8
1.0
1.4
1.4
0.0
2.0
4.0
sc ps ps ps sc st st st st
Therapy Interventions: sm=Self monitor, gf=goal focus, sc=self-care, st=self-talk,
fp=feeling process, ac= assertiveness , rt = Relaxation-Trance
Self
ratin
gs o
f Sx
dist
ress
an
d Fn
c ab
ility
Symptom distress average: 0(none) - 4(severe)Functioning ability average: 0(very poorly) - 4(very well)
2 per. Mov. Avg. (Symptom distress average: 0(none) - 4(severe))2 per. Mov. Avg. (Functioning ability average: 0(very poorly) - 4(very well))

26
Assertive Self-Care SummaryAssertive Self-Care Summary• Limited Resources forces need for:
– Treatment Effectiveness and Efficiency– Strategic interventions requiring minimal effort
• Self Guided Counseling with Strategic Interventions can provide a non-therapist level of care due to limited resources
• Data Collection and Analysis can help to better understand Tx Outcomes
• For more information, contact – Chris Potter, M.Ed.: [email protected]

















