Creating a Culture of Safety: Challenges in Ophthalmology James P. Bagian, MD, PE Director, Center for Health Engineering University of Michigan Founding Director, VA National Center for Patient Safety [email protected]
Transcript
Creating a Culture of Safety:Challenges in Ophthalmology
James P. Bagian, MD, PEDirector, Center for Health Engineering
University of MichiganFounding Director, VA National Center for Patient
• Steps Prior to Day of Surgery• “clinic and surgery areas…specific data be
passed between sites via written documentation rather than verbal”
• Steps On the Day of Surgery• “…proper eye should clearly be notated on
the consent form. “• “person who marks the eye should use written
documentation with verbal verification” • Timeout – All team members, patient, side,
implant, etc. Use “Hard Stop” if required
American Academy of Ophthalmology
• Checklist for the Surgery Chart • Pre-Op Area
• Patient ID, Procedure, Side• Eye marked
• Operating Room• Patient ID – name and birth date• Procedure & Side• Proper Implant – Style and Power• “Prior to draping, circulating nurse ensures that
operative plan is visible (post drape) so that the surgeon can read it while gowned and gloved. “
• “The circulating nurse writes the patient's name, operative eye, IOL style, and IOL power on the white board. “
How Have We Done?
• Problems still exist
How Have We Done? - VA
• 2001-2006 Experience (All Specialties)• 108 OR adverse events reported• Ophthalmology and Orthopedics the highest
reports although not most common procedures
• Communication (inadequate timeout) and Patient Mis-Identification played major role
• Wrong side >40%• Wrong Implant >30%• Wrong Site/Patient/Procedure each approx.
10%Neily et al. Incorrect Surgical Procedures …Arch Surg 2009 Nov;144(11):1028-34
What Have We Learned? - VA
• Actions needed well before entering the OR• Timeout period is too late in many cases• Systems-based approaches beyond individual
• Involvement of all disciplines
• Structured communication that drives discussion• Briefings & debriefings, Medical Team
Training essential
Supporting Long Term Memory
• Checklists• Put knowledge in the world vs. in the head • Recognition is better than recall
• Checklist Philosophy• “Read and Verify” checklists• “Read and Do” checklists
Checklist-Driven Preoperative Briefing
Antibiotic Prophylaxis
DVT Prophylaxis
Vertical Hierarchy
• “Silence Kills”. Team members uncomfortable “speaking up” when something does not seem right in a patient’s care, leading to patient harm.
• Poor communication between team members leading to a lack of situational awareness and a poor clinical decision resulting in patient harm.
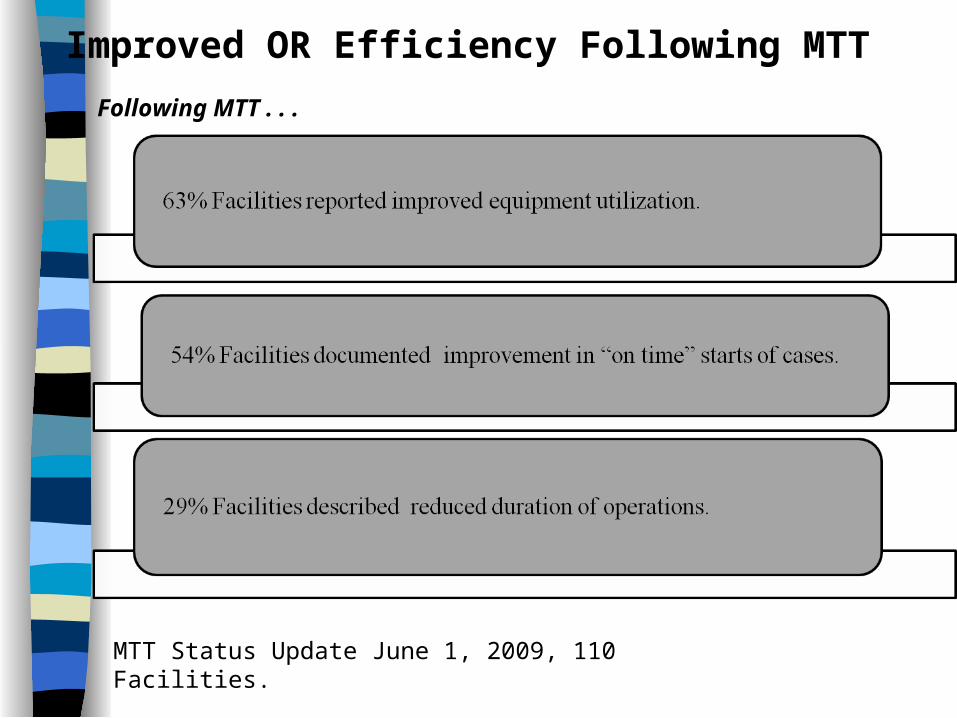
• Did Medical Team Training (MTT) improve either of these baseline healthcare problems in our Organization?