Page 1
CTCL Treatment AlgorithmsHow I treat advanced stage CTCL
Francine Foss MD
Professor of Medicine
Hematology and Bone Marrow Transplantation
Yale University School of Medicine
New Haven, CT USA
Page 2
DISCLOSURES
• SEATTLE GENETICS, SPECTRUM- consultant, speaker
• MIRAGEN- consultant
• MALLINRODT- consultant
• KYOWA – investigator, consultant
Page 3
WHO-EORTC Classification of Cutaneous T-cell and NK Lymphomas-Incidence in US by SEER Registry Data
Willemze R, et al. Blood. 2005;105:3768-3785.
Mycosis fungoides
MF variants and subtypes (3836)Folliculotropic MFPagetoid reticulosisGranulomatous slack skin
Sézary syndrome (117)Adult T-cell leukemia/lymphoma
Primary cutaneous CD30+ lymphoproliferative disorders (858)Primary cutaneous anaplastic large cell lymphomaLymphomatoid papulosis
Subcutaneous panniculitis-like T-cell lymphomaExtranodal NK/T-cell lymphoma, nasal type
Primary cutaneous peripheral T-cell lymphoma, pleomorphic (1840) Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma (provisional)Cutaneous γ/δ T-cell lymphoma
Page 4
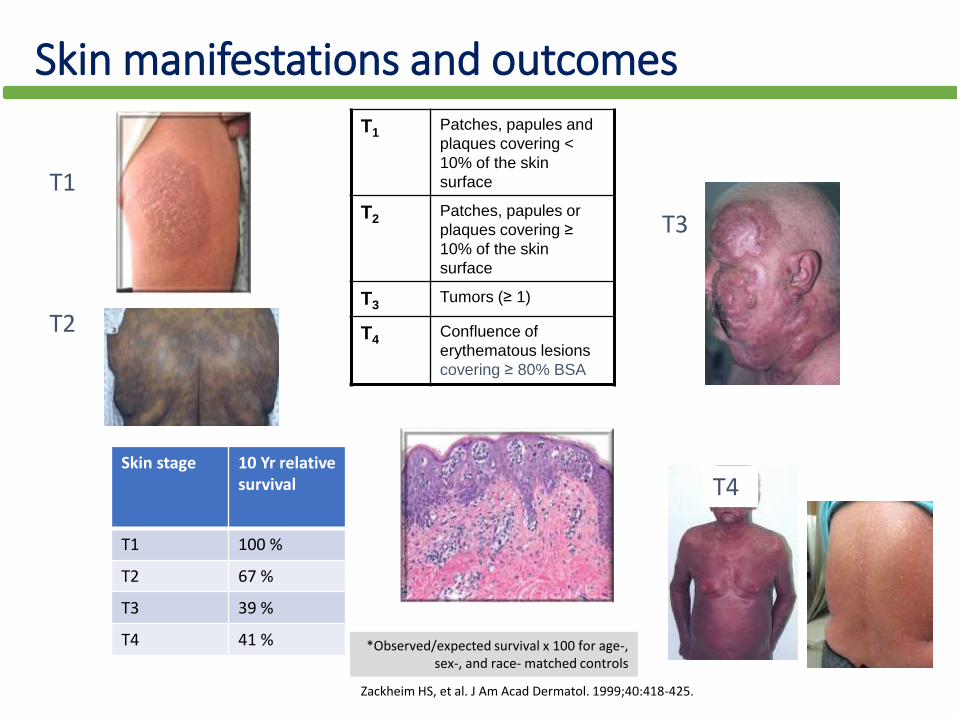
Skin manifestations and outcomes
T1
T2
T3
T4Skin stage 10 Yr relative
survival
T1 100 %
T2 67 %
T3 39 %
T4 41 % *Observed/expected survival x 100 for age-, sex-, and race- matched controls
Zackheim HS, et al. J Am Acad Dermatol. 1999;40:418-425.
T1Patches, papules and
plaques covering <
10% of the skin
surface
T2Patches, papules or
plaques covering ≥
10% of the skin
surface
T3Tumors (≥ 1)
T4Confluence of
erythematous lesions
covering ≥ 80% BSA
Page 5
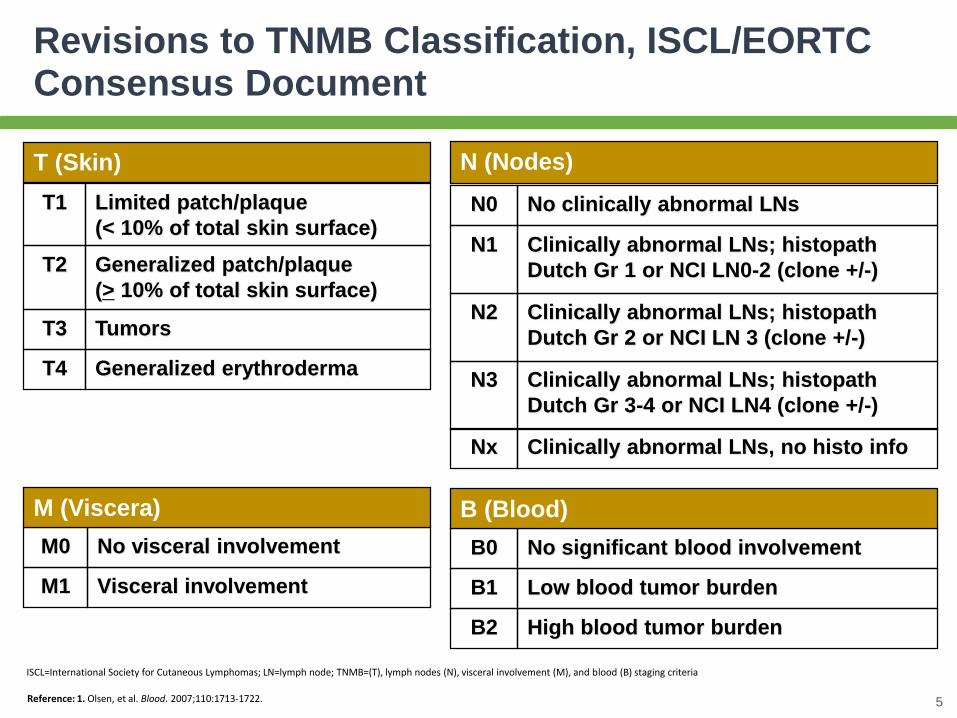
B0 No significant blood involvement
B (Blood)
B1 Low blood tumor burden
B2 High blood tumor burden
T1 Limited patch/plaque
(< 10% of total skin surface)
T (Skin)
T2 Generalized patch/plaque
(> 10% of total skin surface)
T3 Tumors
T4 Generalized erythroderma
M0 No visceral involvement
M (Viscera)
M1 Visceral involvement
N0 No clinically abnormal LNs
N (Nodes)
N1 Clinically abnormal LNs; histopath
Dutch Gr 1 or NCI LN0-2 (clone +/-)
N2 Clinically abnormal LNs; histopath
Dutch Gr 2 or NCI LN 3 (clone +/-)
N3 Clinically abnormal LNs; histopath
Dutch Gr 3-4 or NCI LN4 (clone +/-)
Nx Clinically abnormal LNs, no histo info
Revisions to TNMB Classification, ISCL/EORTC Consensus Document
Reference: 1. Olsen, et al. Blood. 2007;110:1713-1722. 5
ISCL=International Society for Cutaneous Lymphomas; LN=lymph node; TNMB=(T), lymph nodes (N), visceral involvement (M), and blood (B) staging criteria
Page 6
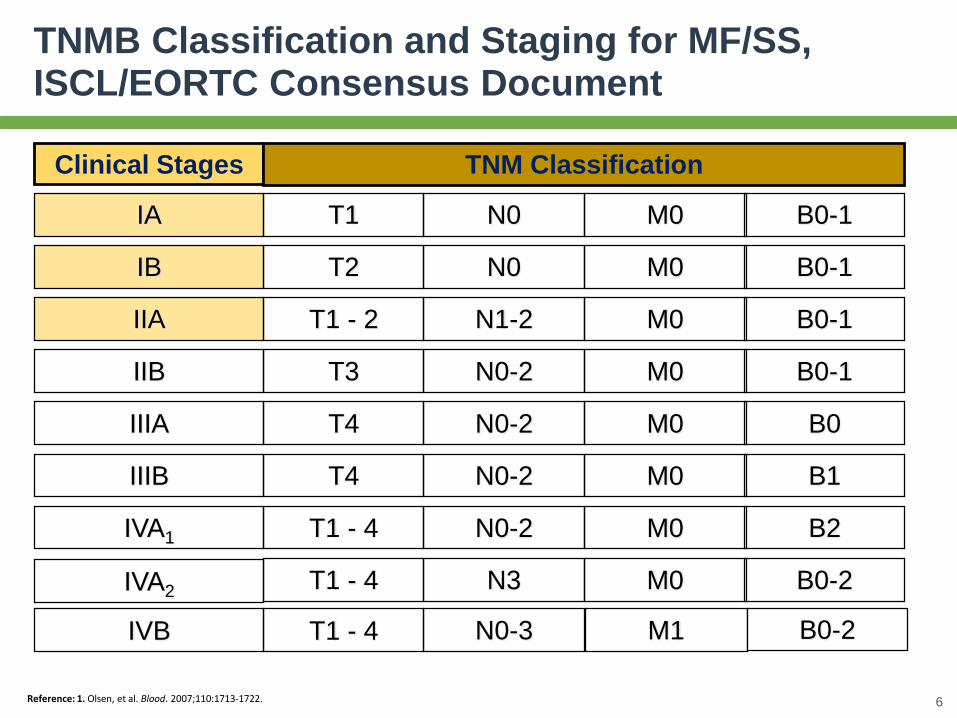
Clinical Stages TNM Classification
IA T1 N0 M0
IB T2 N0 M0
IIA T1 - 2 N1-2 M0
IIB T3 N0-2 M0
IIIA T4 N0-2 M0
IIIB T4 N0-2 M0
IVA1 T1 - 4 N0-2 M0
IVB
T1 - 4 N3 M0
B0-1
B0-1
B0-1
B0-1
B0
B1
B2
B0-2IVA2
T1 - 4 N0-3 M1 B0-2
TNMB Classification and Staging for MF/SS, ISCL/EORTC Consensus Document
Reference: 1. Olsen, et al. Blood. 2007;110:1713-1722. 6
Page 7
Disease-Specific Survival by Clinical Stage
1,398 patients with MF
104 patients with SS
Time Since Diagnosis (yrs)
Pro
bab
ilit
y o
f S
urv
ival
(%)
0 10 20 30
100
80
60
40
20
0
7Agar NS, et al. J Clin Oncol. 2010;28:4730-4739.
Retrospective, 525 patients
Kim YH, et al. Arch Dermatol. 2003;139:857-66.
UK
US
Page 8
• Physical Exam
• Skin extent & type, photodocumentation
• LN, organomegaly/masses
• Laboratory studies
• CBC , LDH, metabolic panel
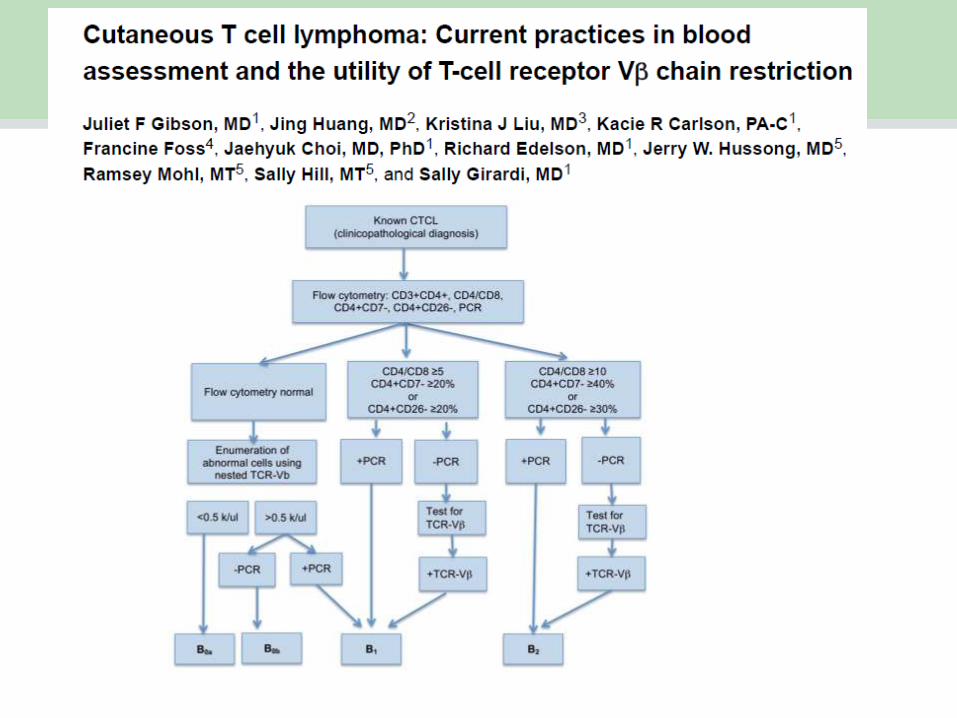
• Flow cytometry: CD3, CD4, CD7, CD8, CD26 to
assess for ↑CD4+, CD4/CD8 or abnormal phenotype
(CD7- or CD26-)
• VBeta panel by flow cytometry to identify clone(s)
• T cell gene rearrangement and FISH for CTCL panel
• HTLV-1 if risk factors
• Imaging studies
• whole body PET/CT or CT with contrast
• MRI if appropriate
• Biopsy of suspicious LNs (>2 cm or sig. PET+) or
suspected
visceral involvement. Core needle or excisional
• Bone marrow biopsy if B2 or clinical suspicion
My Staging Evaluation for MF/SS
8
Image courtesy of A.Moskowitz, MD
with image permissions
Page 9
• 161 patients at Yale who had Vbeta analysis studied
• 34 had B2 by flow cytometry• Vbeta detected 25 of 34 (73%)• 12 of the 127 B1 patients had
Vbeta positivity, 10 of these had +TCRR
Page 11
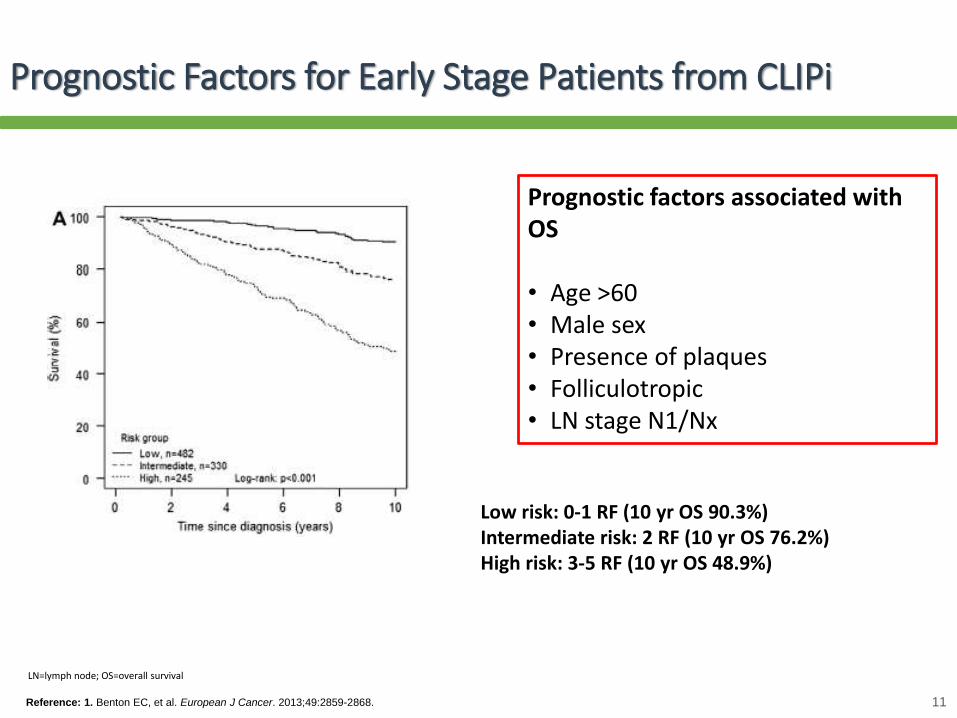
Prognostic Factors for Early Stage Patients from CLIPi
Low risk: 0-1 RF (10 yr OS 90.3%)Intermediate risk: 2 RF (10 yr OS 76.2%)High risk: 3-5 RF (10 yr OS 48.9%)
Reference: 1. Benton EC, et al. European J Cancer. 2013;49:2859-2868. 11
Prognostic factors associated with OS
• Age >60• Male sex• Presence of plaques• Folliculotropic• LN stage N1/Nx
LN=lymph node; OS=overall survival
Page 12
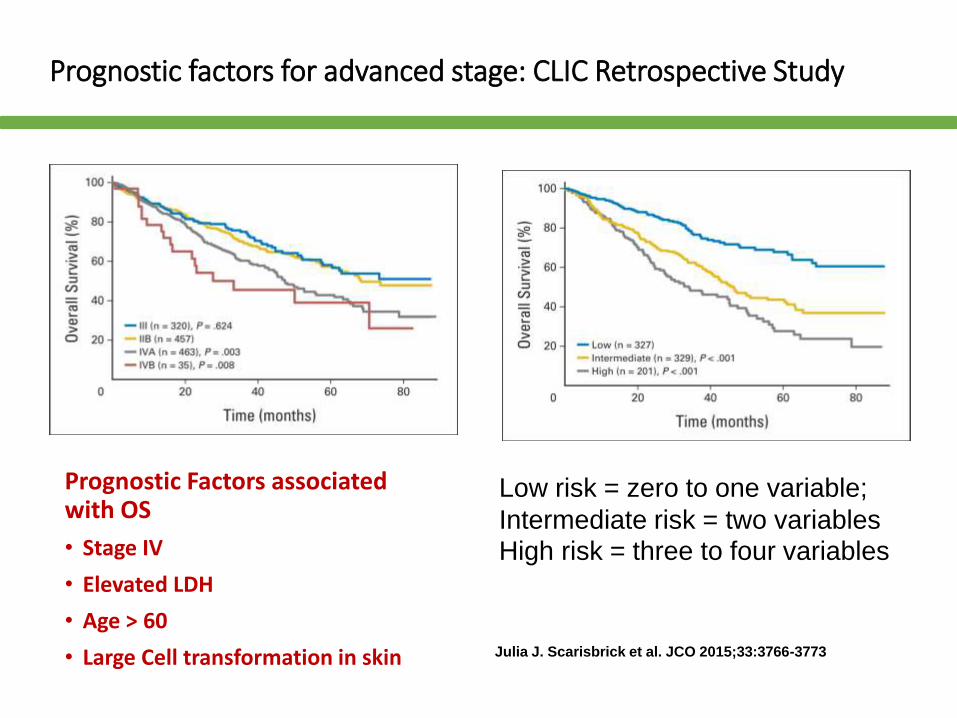
Prognostic factors for advanced stage: CLIC Retrospective Study
Prognostic Factors associated with OS
• Stage IV
• Elevated LDH
• Age > 60
• Large Cell transformation in skin Julia J. Scarisbrick et al. JCO 2015;33:3766-3773
Low risk = zero to one variable;
Intermediate risk = two variablesHigh risk = three to four variables
Page 13
13
T1: Limited
patch/plaque
(<10% BSA)
T2: Generalized
patch/plaque
(≥10% BSA)
T3: TumorT4:
Erythroderma
N0: Nodes clinically
uninvolved M0 IA IBIIB
IIIAN1: Nodes enlarged,
histologically uninvolvedM0 IIA IIIB
N2-3: Nodes clinically
normal (N2) or enlarged
(N3), histologically
involved
M0 IVA
N0-3: Visceral
involvement M1 IVBB0: Absence of significant peripheral blood Sézary cells
B1: Low tumor burden that does not meet the criteria of B2 cells
B2: Significant peripheral blood >1000/μL Sézary cells with positive clone
1. Olsen E, et al. Blood. 2007;110:1713-1722.
2. Lansigan F and Foss FM. Drugs 2010;70:273-86.
Clinical Approach By Stage
= Early-stage disease = Advanced disease
Folliculotrophic type
Large Cell Transformation unilesional
Large Cell Transformation visceral site or node
Sezary with high risk genetics/cytogenetics
-Others
Page 14
Current status of treatment in a nutshell
• MF is an immunologically responsive disease
• Most new approved therapies have CR rate (≤ 10%) and 30% ORR (PR + CR)
• Most patients require multiple therapies over the course of their disease and often treatments are repeated
• Many patients receive combinations of agents and both systemic and topical therapy
• Stable disease is a meaningful endpoint for patients if relief of pruritus and skin symptoms
• Infections are a major cause of morbidity and mortality Kim YH, et al. Arch Dermatol. 2003;139:857-866.
Risk for progression in 525 patients
Page 15
Stage-based Approach to Treatment
IALimited
patch/plaque
IB/IIAGeneralizedpatch/plaque
IIBTumors
IIIErythroderma
IVExtracutan
disease
Combinationchemo
Clinical Trials
Bexarotene, methotrexate, IFN vorinostat, romidepsin
Allo-HSCT
Alemtuzumab
**Brentuximab vedotin, pralatrexate, liposomal doxorubicin, gemcitabine, other
Photopheresis
bexarotene or IFN
TSEBT + ECP, IFN
Topical steroid, retinoid (bex), NM
phototherapy, local RT, imiquimod
New targeted or cytotoxic systemic therapy**
15This slide represents expert opinion, no source reference is available
ECP=extracorporeal photopheresis
Checkpoint therapies and other novel immunomodulatory approaches
Precision medicine approach
Page 16
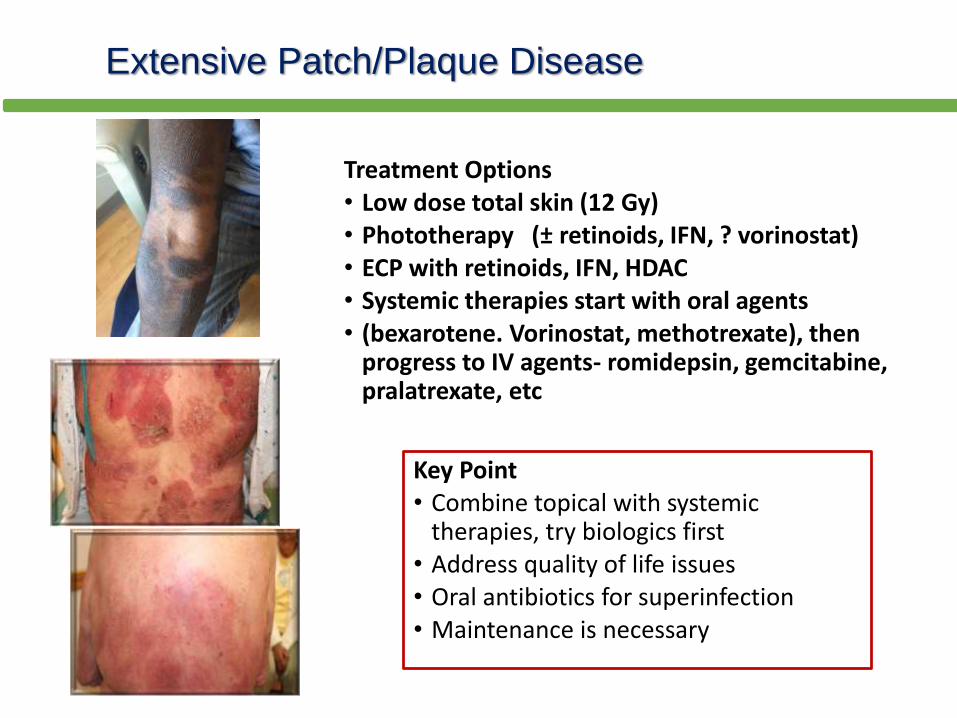
Extensive Patch/Plaque Disease
Treatment Options• Low dose total skin (12 Gy) • Phototherapy (± retinoids, IFN, ? vorinostat)• ECP with retinoids, IFN, HDAC• Systemic therapies start with oral agents • (bexarotene. Vorinostat, methotrexate), then
progress to IV agents- romidepsin, gemcitabine, pralatrexate, etc
Key Point• Combine topical with systemic
therapies, try biologics first• Address quality of life issues• Oral antibiotics for superinfection• Maintenance is necessary
Page 17
Management of Tumor Stage MF
Treatment Options
• Important to know if LCT or CD30+
• Local radiotherapy for immediate palliation
• Systemic therapies: oral and IV, brentuximab if CD30+
• May require more aggressive multi-agent chemotherapy to debulk (Gem Doxil or Gem Ox or other regimens, EPOCH)
• For multiple tumors, aggressive clinical features, high LDH, consider stem cell transplant after remission is achieved
Key Points
• Outcomes poor for most with multiple tumors
• May have large cell transformation
• Maintenance is necessary if patient not going to transplant
• Think about transplant earlier in course of disease
Page 18
NCCN Guidelines for Tumor Stage MF
Page 19
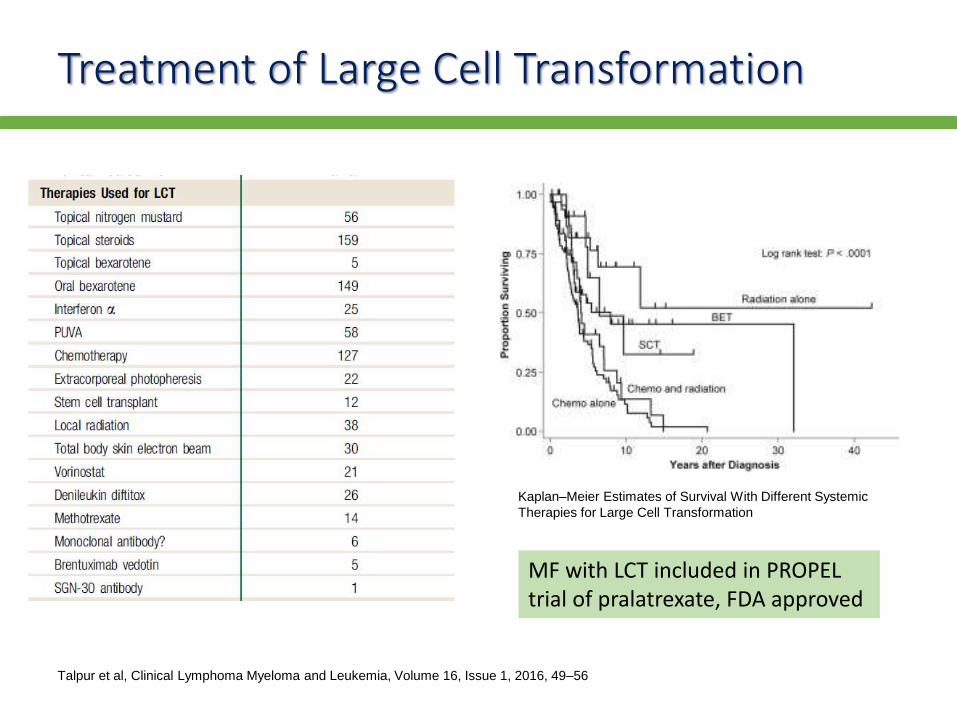
Treatment of Large Cell Transformation
Talpur et al, Clinical Lymphoma Myeloma and Leukemia, Volume 16, Issue 1, 2016, 49–56
Kaplan–Meier Estimates of Survival With Different Systemic
Therapies for Large Cell Transformation
MF with LCT included in PROPEL trial of pralatrexate, FDA approved
Page 20
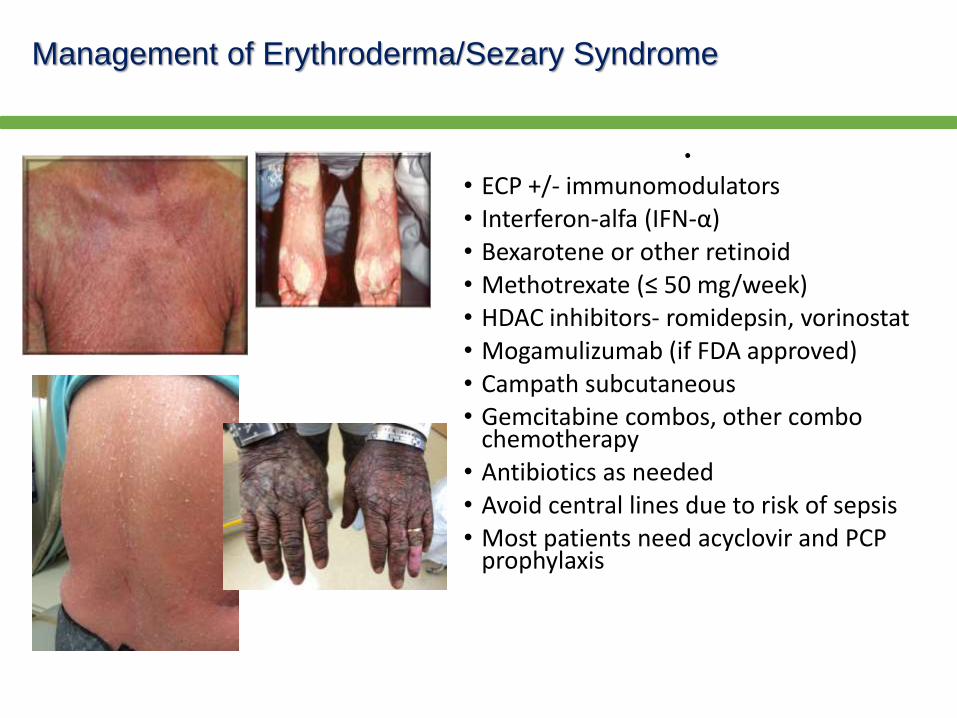
Management of Erythroderma/Sezary Syndrome
•
• ECP +/- immunomodulators• Interferon-alfa (IFN-α)• Bexarotene or other retinoid• Methotrexate (≤ 50 mg/week)• HDAC inhibitors- romidepsin, vorinostat• Mogamulizumab (if FDA approved)• Campath subcutaneous• Gemcitabine combos, other combo
chemotherapy• Antibiotics as needed• Avoid central lines due to risk of sepsis• Most patients need acyclovir and PCP
prophylaxis
Page 21
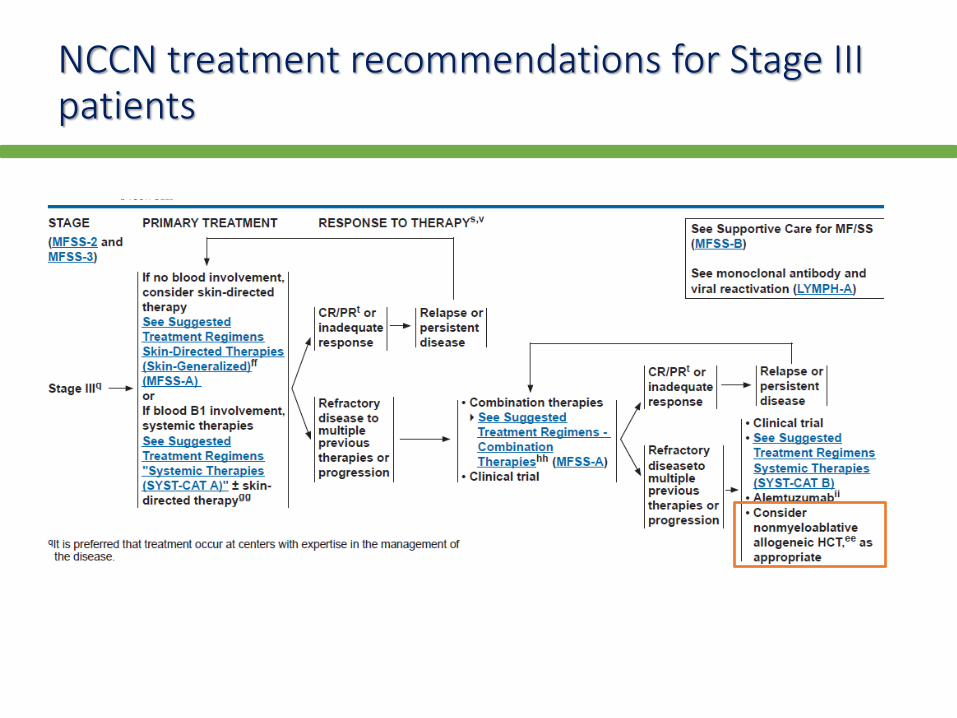
NCCN treatment recommendations for Stage III patients
Page 22
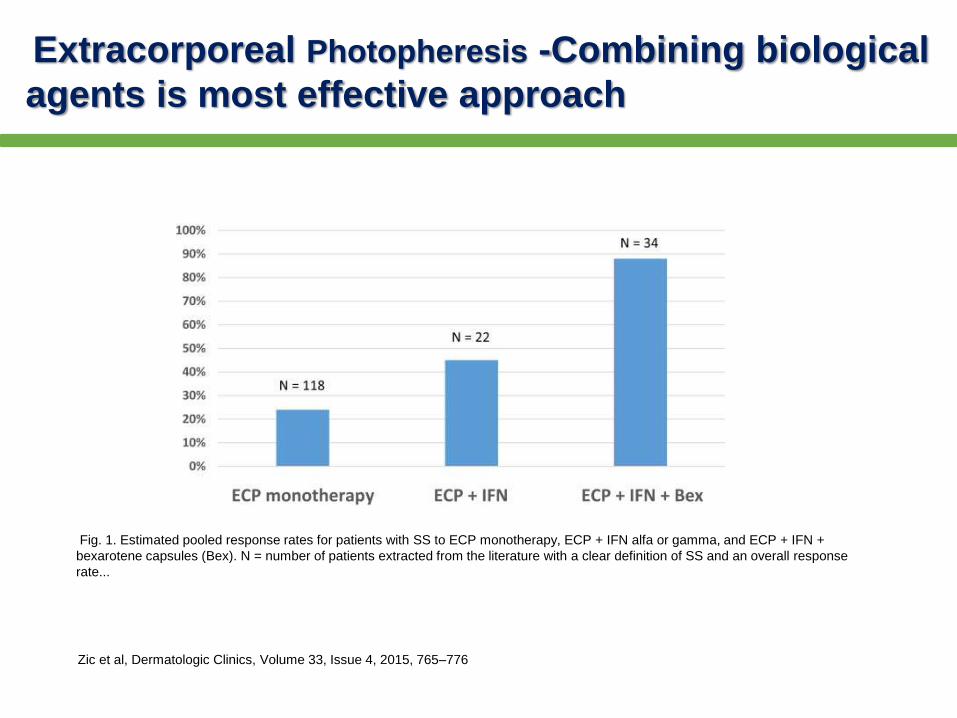
Fig. 1. Estimated pooled response rates for patients with SS to ECP monotherapy, ECP + IFN alfa or gamma, and ECP + IFN +
bexarotene capsules (Bex). N = number of patients extracted from the literature with a clear definition of SS and an overall response
rate...
Extracorporeal Photopheresis -Combining biological
agents is most effective approach
Zic et al, Dermatologic Clinics, Volume 33, Issue 4, 2015, 765–776
Page 23
NCCN Guidelines for Stage IV Mycosis Fungoides
Page 24
FDA approved agents for CTCLEfficacy data
Agent (Class) Indication Study N ORR DOR
RomidepsinPatients with CTCL
who have received
systemic therapy
Pivotal 96 34% 15 mo
Supportive 71 35% 11 mo
Denileukin diftitox
(Fusion protein)
Tumors that express
CD25Pivotal 71 30% 4 mo
Bexarotene
(Retinoid x-receptor
activator)
Cutaneous
manifestationsPivotal 62 32% 5+ mo
Vorinostat
(HDAC inhibitor)
Cutaneous
manifestationsPivotal 74 30% 6+ mo
Supportive 33 24% 4 mo
Brentuximab vedotin CD30+ CTCL
Randomized
trial with
vorinostat
64 60% 14 mo
(pfs)
Page 25
Responses by stage for chemotherapy agents
Agent Stage IIA Stage IIb Stage III Stage IV
Romidepsin 25 43 39 8
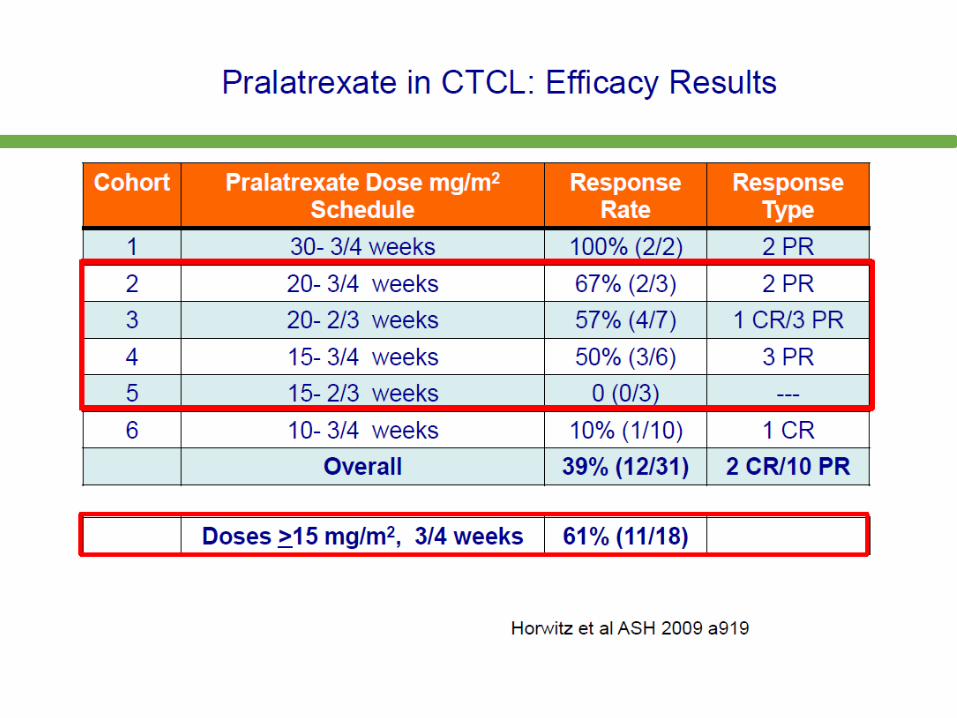
Pralatrexate 50 53 50
Bexarotene 30 23 33
Vorinostat 30 29 33
Brentuximab
vedotin
Gemcitabine
Page 27
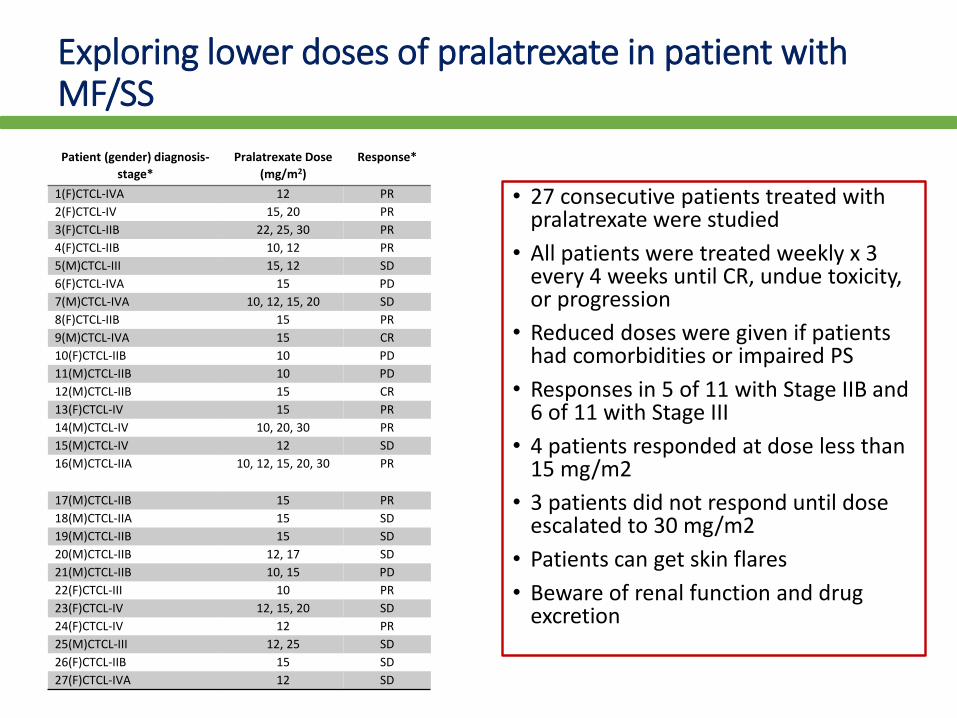
Exploring lower doses of pralatrexate in patient with MF/SS
Patient (gender) diagnosis-
stage*
Pralatrexate Dose
(mg/m2)
Response*
1(F)CTCL-IVA 12 PR
2(F)CTCL-IV 15, 20 PR
3(F)CTCL-IIB 22, 25, 30 PR
4(F)CTCL-IIB 10, 12 PR
5(M)CTCL-III 15, 12 SD
6(F)CTCL-IVA 15 PD
7(M)CTCL-IVA 10, 12, 15, 20 SD
8(F)CTCL-IIB 15 PR
9(M)CTCL-IVA 15 CR
10(F)CTCL-IIB 10 PD
11(M)CTCL-IIB 10 PD
12(M)CTCL-IIB 15 CR
13(F)CTCL-IV 15 PR
14(M)CTCL-IV 10, 20, 30 PR
15(M)CTCL-IV 12 SD
16(M)CTCL-IIA 10, 12, 15, 20, 30 PR
17(M)CTCL-IIB 15 PR
18(M)CTCL-IIA 15 SD
19(M)CTCL-IIB 15 SD
20(M)CTCL-IIB 12, 17 SD
21(M)CTCL-IIB 10, 15 PD
22(F)CTCL-III 10 PR
23(F)CTCL-IV 12, 15, 20 SD
24(F)CTCL-IV 12 PR
25(M)CTCL-III 12, 25 SD
26(F)CTCL-IIB 15 SD
27(F)CTCL-IVA 12 SD
• 27 consecutive patients treated with pralatrexate were studied
• All patients were treated weekly x 3 every 4 weeks until CR, undue toxicity, or progression
• Reduced doses were given if patients had comorbidities or impaired PS
• Responses in 5 of 11 with Stage IIB and 6 of 11 with Stage III
• 4 patients responded at dose less than 15 mg/m2
• 3 patients did not respond until dose escalated to 30 mg/m2
• Patients can get skin flares
• Beware of renal function and drug excretion
Page 28
Activity of Romidepsin in tumor stage and folliculotropic MF
Overall
(N = 96)
Patients with
cutaneous
tumors
(n = 20)a
Patients with
folliculotropic
involvement
(n = 10)a,b
Median treatment duration (range),
months 3.6 (< 0.1-21.9) 3.6 (0.5-21.9) 4.3 (0.5-8.0)
Best response, n (%)
ORR 33 (34) 9 (45) 6 (60)
CR 6 (6) 2 (10) 1 (10)
SD 45 (47) 9 (45) 3 (30)
SD90 28 (29) 3 (15) 2 (20)
Median time to response (range),
months
1.9 (0.9-4.8) 1.9 (1.9-4.7) 2.1 (1.0-4.8)
Median DOR (range), months 15.0
(< 0.1+ to 19.8+)
NR
(1.4 to 18.7+)
3.6
(2.1 to 5.0+)
Best change in pruritus VAS, mean (standard deviation)c
Moderate to severe pruritus at
baselined
−38 (28) −43 (27) −53 (35)
Severe pruritus at baselinee −49 (28) −45 (29) −60 (42)
Median time to progression (range),
months
8.3
(< 0.1+ to 21.7+)
3.8
(0.9+ to 21.7+)
8.3
(< 0.1+ to 8.3+)
CR, complete response; DOR, duration of response; NR, not reached; ORR, objective response rate; SD,
stable disease; SD90, stable disease for ≥ 90 days; VAS, visual analog scale.
a Two patients had both cutaneous tumors and folliculotropic involvement, and are included in both
columns.
b Response data were missing for 1 patient with folliculotropic involvement.
Foss et al, Clin Lymph Myeloma 2016
Page 29
Charlotte F. M. Hughes et al. Blood 2015;125:71-81
How to pick a therapy- time to next treatment by
stage
Page 30
CIBMTR Review of Outcomes for CTCL patients undergoing Allogeneic Stem Cell Transplantation
• Real world experience, unselected patients, heterogeneous
• 133 pts in registry had diagnosis of CTCL
• No data on stage
• Only 8 were in CR at transplant
• Reduced intensity regimens used in 64%
• 100 day transplant related mortality was 16%
• PFS and OS 36% and 44% at 2 yrs
• Grade II-IV aGVHD in 36%
• cGVHD in 31%
Lechowicz M, et al BBMT 2014
Page 31
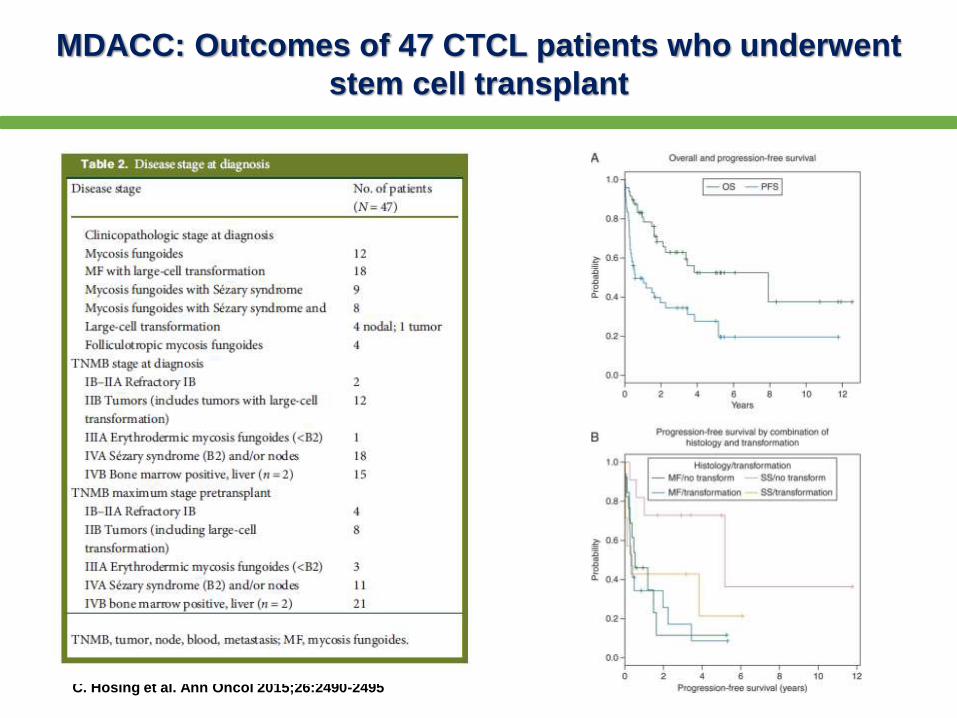
MDACC: Outcomes of 47 CTCL patients who underwent
stem cell transplant
C. Hosing et al. Ann Oncol 2015;26:2490-2495
Page 32
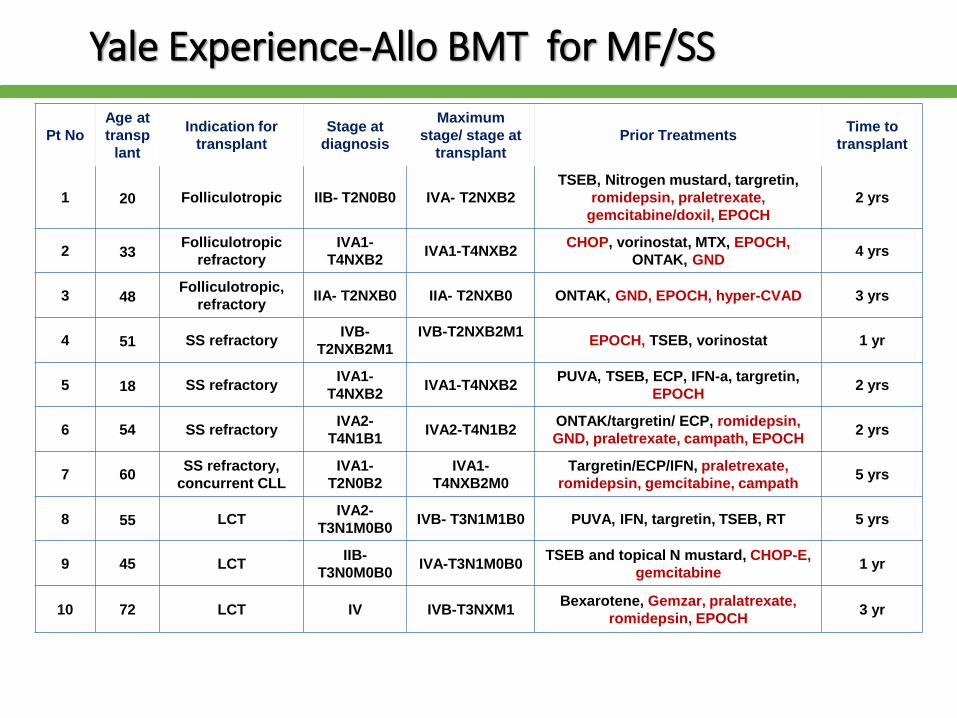
Yale Experience-Allo BMT for MF/SS
Pt No
Age at
transp
lant
Indication for
transplant
Stage at
diagnosis
Maximum
stage/ stage at
transplant
Prior TreatmentsTime to
transplant
1 20 Folliculotropic IIB- T2N0B0 IVA- T2NXB2
TSEB, Nitrogen mustard, targretin,
romidepsin, praletrexate,
gemcitabine/doxil, EPOCH
2 yrs
2 33Folliculotropic
refractory
IVA1-
T4NXB2IVA1-T4NXB2
CHOP, vorinostat, MTX, EPOCH,
ONTAK, GND4 yrs
3 48Folliculotropic,
refractory IIA- T2NXB0 IIA- T2NXB0 ONTAK, GND, EPOCH, hyper-CVAD 3 yrs
4 51 SS refractoryIVB-
T2NXB2M1
IVB-T2NXB2M1EPOCH, TSEB, vorinostat 1 yr
5 18 SS refractoryIVA1-
T4NXB2IVA1-T4NXB2
PUVA, TSEB, ECP, IFN-a, targretin,
EPOCH2 yrs
6 54 SS refractoryIVA2-
T4N1B1IVA2-T4N1B2
ONTAK/targretin/ ECP, romidepsin,
GND, praletrexate, campath, EPOCH2 yrs
7 60SS refractory,
concurrent CLL
IVA1-
T2N0B2
IVA1-
T4NXB2M0
Targretin/ECP/IFN, praletrexate,
romidepsin, gemcitabine, campath5 yrs
8 55 LCTIVA2-
T3N1M0B0IVB- T3N1M1B0 PUVA, IFN, targretin, TSEB, RT 5 yrs
9 45 LCTIIB-
T3N0M0B0IVA-T3N1M0B0
TSEB and topical N mustard, CHOP-E,
gemcitabine1 yr
10 72 LCT IV IVB-T3NXM1Bexarotene, Gemzar, pralatrexate,
romidepsin, EPOCH3 yr
Page 33
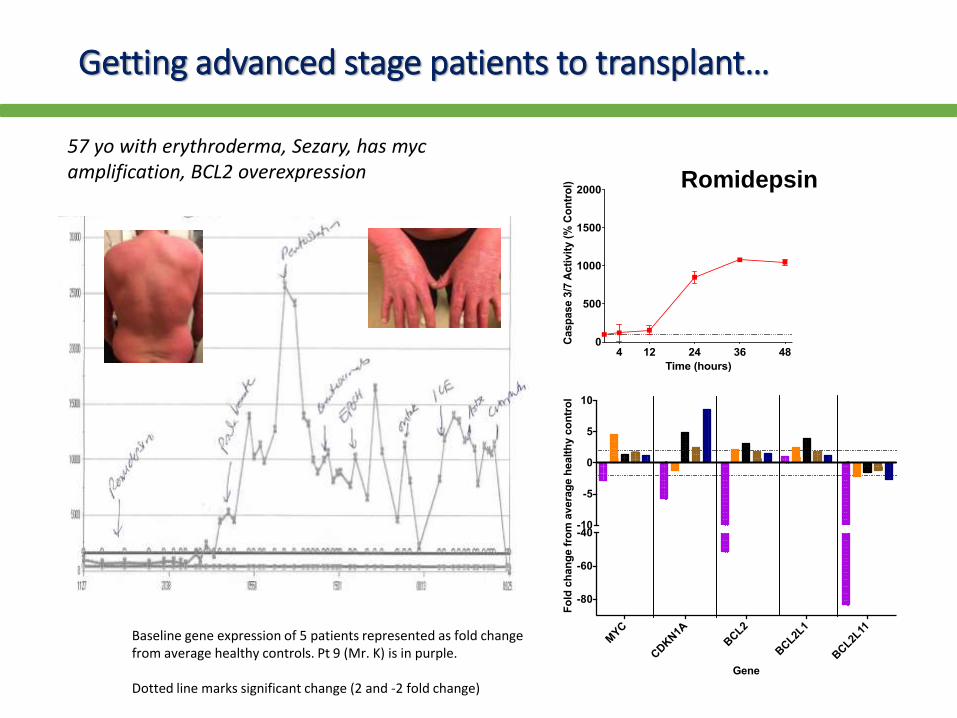
Getting advanced stage patients to transplant…
4 12 24 36 480
500
1000
1500
2000
Time (hours)
Casp
ase 3
/7 A
cti
vit
y (
% C
on
tro
l) Romidepsin
MYC
CDKN1A
BCL2
BCL2L
1
BCL2L
11
-80
-60
-40-10
-5
0
5
10
Gene
Fo
ld c
han
ge f
rom
avera
ge h
ealt
hy c
on
tro
l
Baseline gene expression of 5 patients represented as fold change from average healthy controls. Pt 9 (Mr. K) is in purple.
Dotted line marks significant change (2 and -2 fold change)
57 yo with erythroderma, Sezary, has mycamplification, BCL2 overexpression
Page 34
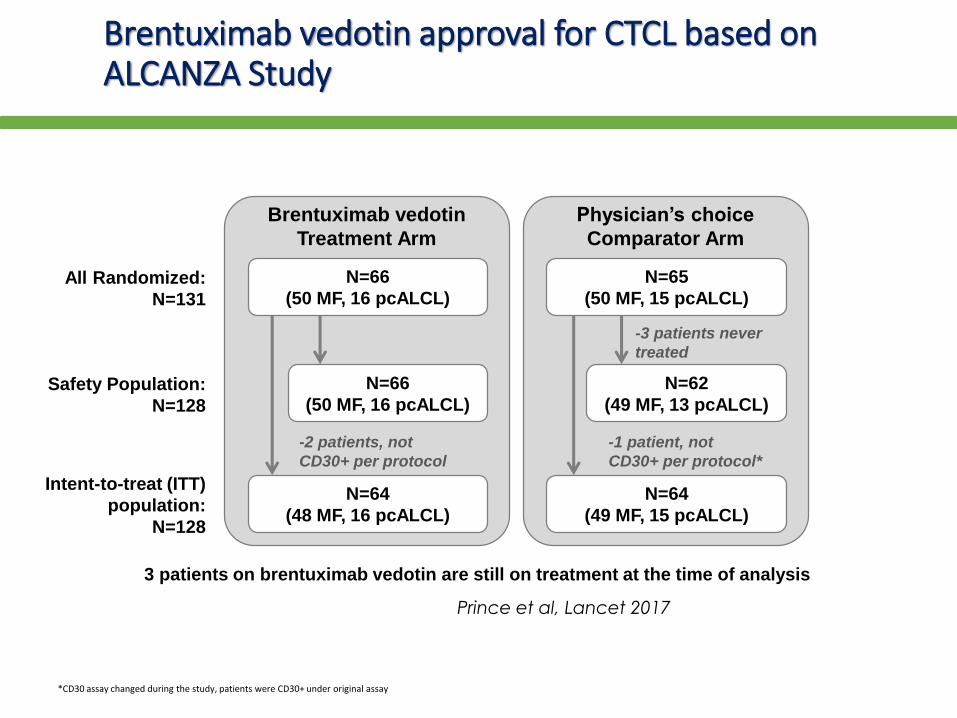
Brentuximab vedotin approval for CTCL based on ALCANZA Study
*CD30 assay changed during the study, patients were CD30+ under original assay
Brentuximab vedotin
Treatment Arm
N=66
(50 MF, 16 pcALCL)
N=66
(50 MF, 16 pcALCL)
N=64
(48 MF, 16 pcALCL)
All Randomized:
N=131
Safety Population:
N=128
Intent-to-treat (ITT)
population:
N=128
-2 patients, not
CD30+ per protocol
Physician’s choice
Comparator Arm
N=65
(50 MF, 15 pcALCL)
N=62
(49 MF, 13 pcALCL)
N=64
(49 MF, 15 pcALCL)
-3 patients never
treated
-1 patient, not
CD30+ per protocol*
3 patients on brentuximab vedotin are still on treatment at the time of analysis
Prince et al, Lancet 2017
Page 35
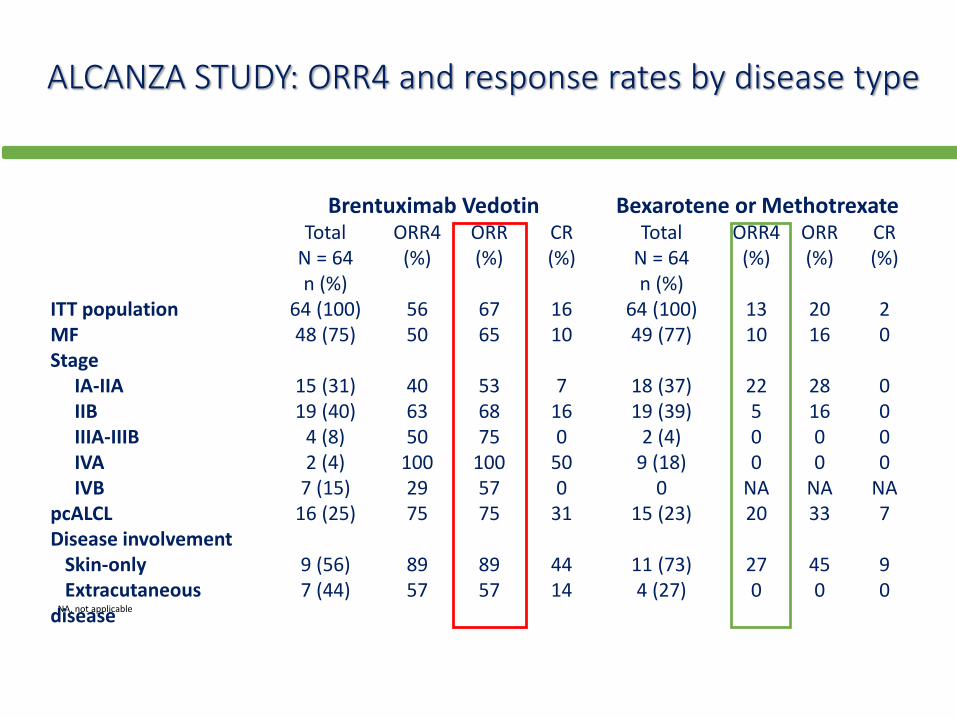
ALCANZA STUDY: ORR4 and response rates by disease type
NA, not applicable
Brentuximab Vedotin Bexarotene or MethotrexateTotal
N = 64n (%)
ORR4(%)
ORR(%)
CR(%)
TotalN = 64n (%)
ORR4(%)
ORR(%)
CR(%)
ITT population 64 (100) 56 67 16 64 (100) 13 20 2MF 48 (75) 50 65 10 49 (77) 10 16 0Stage
IA-IIA 15 (31) 40 53 7 18 (37) 22 28 0IIB 19 (40) 63 68 16 19 (39) 5 16 0IIIA-IIIB 4 (8) 50 75 0 2 (4) 0 0 0IVA 2 (4) 100 100 50 9 (18) 0 0 0IVB 7 (15) 29 57 0 0 NA NA NA
pcALCL 16 (25) 75 75 31 15 (23) 20 33 7Disease involvement
Skin-only 9 (56) 89 89 44 11 (73) 27 45 9Extracutaneous
disease 7 (44) 57 57 14 4 (27) 0 0 0
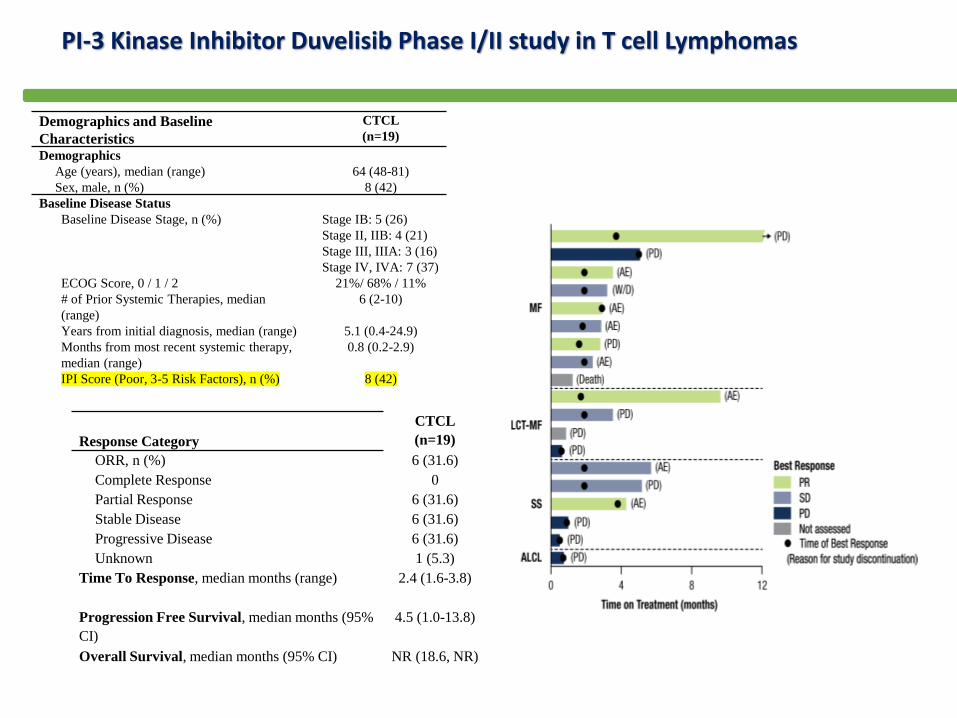
Page 38
Demographics and Baseline
Characteristics
CTCL
(n=19)
Demographics
Age (years), median (range) 64 (48-81)
Sex, male, n (%) 8 (42)
Baseline Disease Status
Baseline Disease Stage, n (%) Stage IB: 5 (26)
Stage II, IIB: 4 (21)
Stage III, IIIA: 3 (16)
Stage IV, IVA: 7 (37)
ECOG Score, 0 / 1 / 2 21%/ 68% / 11%
# of Prior Systemic Therapies, median
(range)
6 (2-10)
Years from initial diagnosis, median (range) 5.1 (0.4-24.9)
Months from most recent systemic therapy,
median (range)
0.8 (0.2-2.9)
IPI Score (Poor, 3-5 Risk Factors), n (%) 8 (42)
Response Category
CTCL
(n=19)
ORR, n (%) 6 (31.6)
Complete Response 0
Partial Response 6 (31.6)
Stable Disease 6 (31.6)
Progressive Disease 6 (31.6)
Unknown 1 (5.3)
Time To Response, median months (range) 2.4 (1.6-3.8)
Progression Free Survival, median months (95%
CI)
4.5 (1.0-13.8)
Overall Survival, median months (95% CI) NR (18.6, NR)
PI-3 Kinase Inhibitor Duvelisib Phase I/II study in T cell Lymphomas
Page 39
• Responders and nonresponders had markedly different changes in serum cytokine profiles induced by duvelisib.
• In vitro, duvelisib potently killed 3 of 4 TCL lines with constitutive phospho-AKT (pAKT) vs 0 of 7 lines lacking pAKT (P = .024) and exceeded cell killing by the PI3K-δ-specific inhibitor idelalisib.
• Administration of duvelisib to mice engrafted with a PTCL patient-derived xenograft resulted in a shift among tumor-associated macrophages from the immunosuppressive M2-like phenotype to the inflammatory M1-like phenotype
Blood. 2018 Feb 22;131(8):888-
898.
Page 40
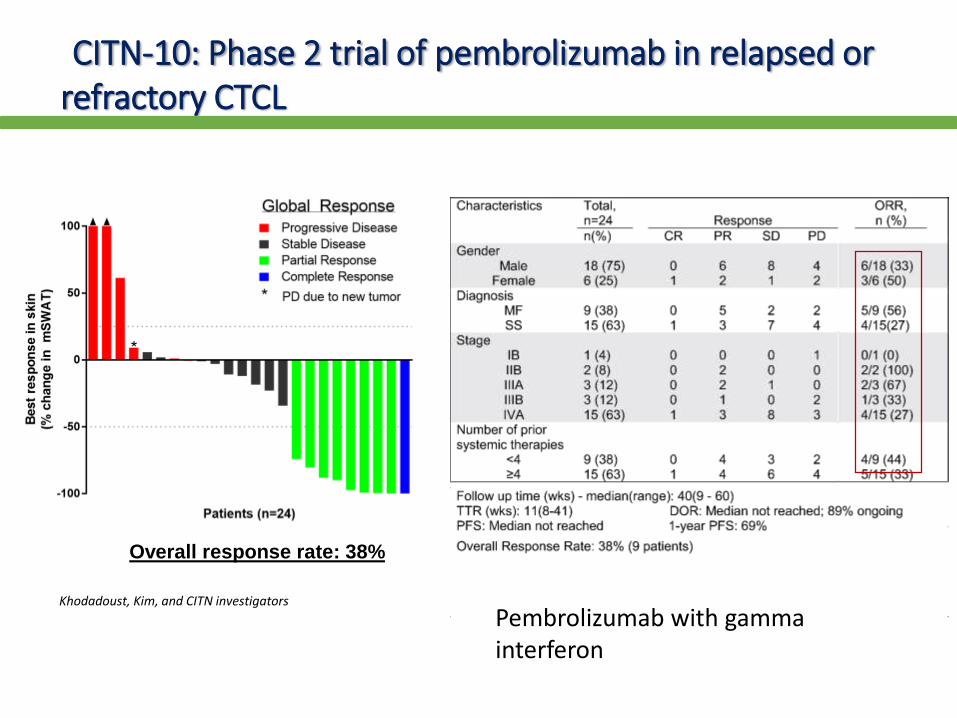
CITN-10: Phase 2 trial of pembrolizumab in relapsed or refractory CTCL
Overall response rate: 38%
Khodadoust, Kim, and CITN investigators
Pembrolizumab with gamma interferon
Page 41
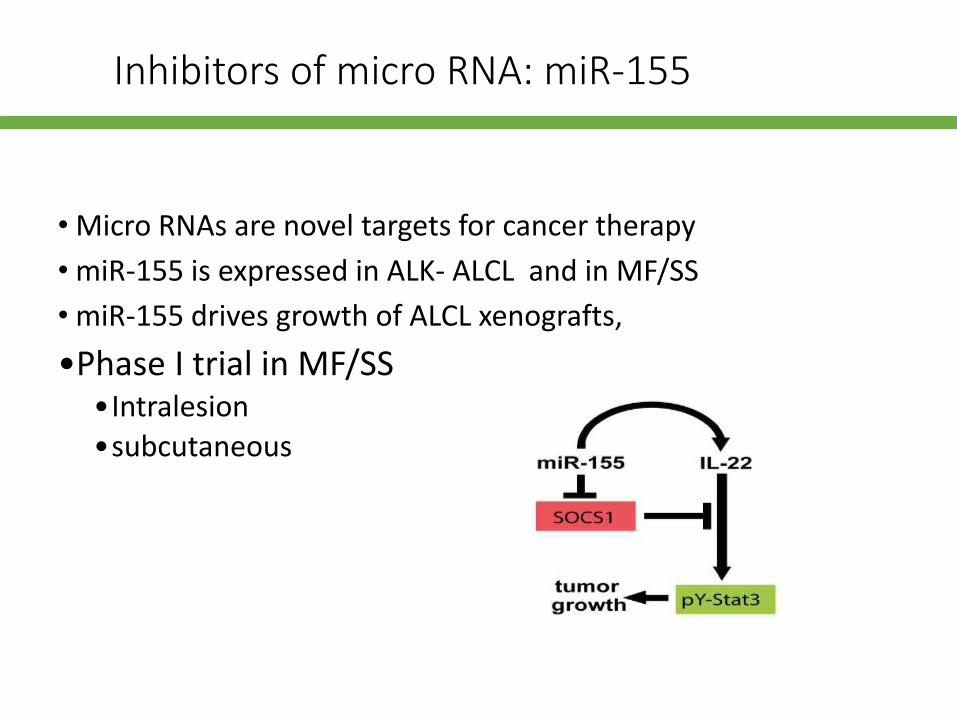
Inhibitors of micro RNA: miR-155
• Micro RNAs are novel targets for cancer therapy
• miR-155 is expressed in ALK- ALCL and in MF/SS
• miR-155 drives growth of ALCL xenografts,
•Phase I trial in MF/SS •Intralesion
•subcutaneous
Page 42
New studies in CTCL
• KIR antibodies (ongoing)
• Duvelisib with romidepsin
• Romidepsin with pralatrexate
• Romidepsin with azacytidine
• Pembrolizumab with Interferon gamma (CITN)
• Multiple new pathway drugs
• Prospective registry collaboration USCLC/ProCLIPI
Page 43
Conclusions
• Most patients will not be cured• Quality of life issues, including cost of treatment are
significant considerations• Monitoring for infections remains a key issue• Many treatments for a few patients, yet still unmet
medical need for many• Need to match up biological features, data from gene
profiling studies, with response to treatment through international collabortions and ultimately develop individual patient algorithms for rational treatment strategies
Page 44
International and US Collaborations
• Cutaneous Lymphoma Foundation
• USCLC- includes medical oncologist, dermatologists, radiation oncologists
• USCLC registry open
• Has patient interface
• Partnership with EORTC, Pro CLIPI
• T Cell Forum- international meeting including aggressive and cutaneous T cell lymphomas