Page 1
CTPA 2009Vassilios Raptopoulos, MD
Longwood Non-invasiveCardiac Imaging Seminar
Beth Israel Beth Israel HarvardHarvardDeaconessDeaconess Medical MedicalMedical CenterMedical Center School School
December 14, 2009
Page 2
CTPA 2009
•64-MDCT•Utilization•I+ delivery•Dual Energy•PE severity•Radiation•MRI - Gad•Venography•Triple R/O
Page 3
CTPA 2009
•Utilization•Technique•DVT•Radiation•In Pregnancy•Large •Small PE•Chronic PE•Triple R/O
Page 5
MDCT for PE “a technological marvel”
• “revolutionized our diagnostic approach”– non-invasive, fast, comfortable, < mm
resolution in < 10sec (4 sec w 64 MDCT)• Massive embolism (surgical planning)
6th order thrombi (? clinical significance)• Lung & chest wall - CT venography• Prognosis
– RV enlargement - Thrombus burden
Goldhaber SZ. (from BWH) N Engl JMed Apr 28 2005; 352:1812 (Editorial)
Page 6
Guidelines for Management Suspected PEBritish Thoracic Society
• D-Dimer– Not in high clinical probability
– A negative test reliably excludes PE
• Imaging– CTPA the recommended initial imaging modality
• A good quality -CTPA does not require additional tests
– Negative isotope scan reliably excludes PE
– Single normal leg US is not reliable to exclude sub-clinical PE
Thorax 2003;58:470
Page 7
Management of suspected Acute PE in the era of CTA A Statement from the Fleischner Society
“multidetector CT angiography has fulfilled the conditions to replace pulmonary angiography as the reference standard for diagnosis of acute PE.”
Remy-Jardin M et al Radiology (Nov) 2007;245: 315-329
Page 8
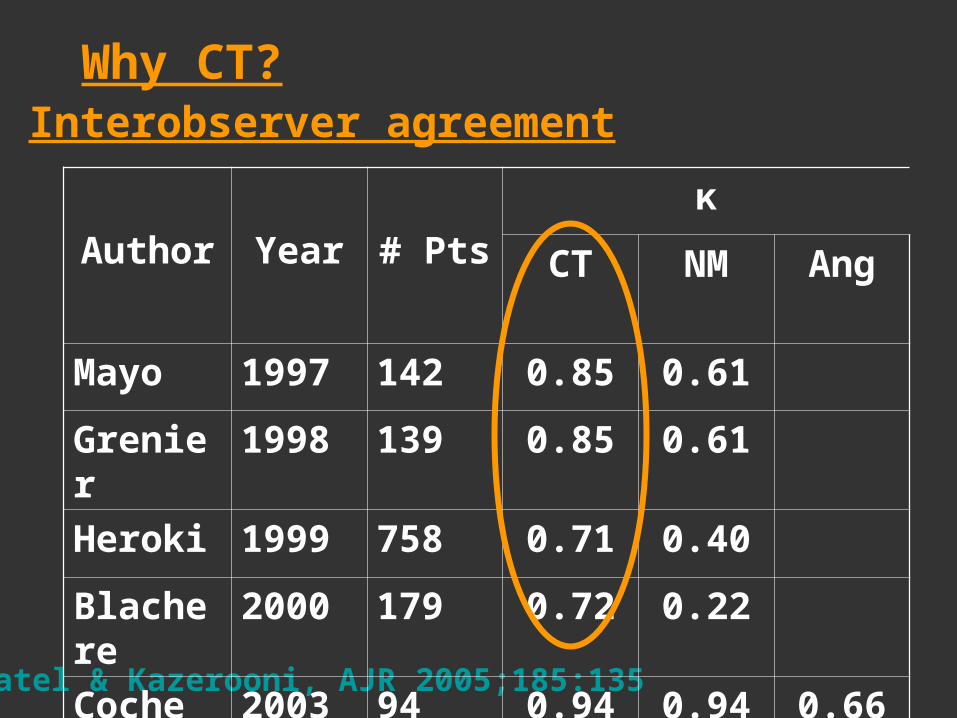
Why CT?
Patel & Kazerooni, AJR 2005;185:135
Author Year # Pts
κ
CT NM Ang
Mayo 1997 142 0.85 0.61
Grenier 1998 139 0.85 0.61
Heroki 1999 758 0.71 0.40
Blachere 2000 179 0.72 0.22
Coche 2003 94 0.94 0.94 0.66
Interobserver agreement
Page 9
© 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 3
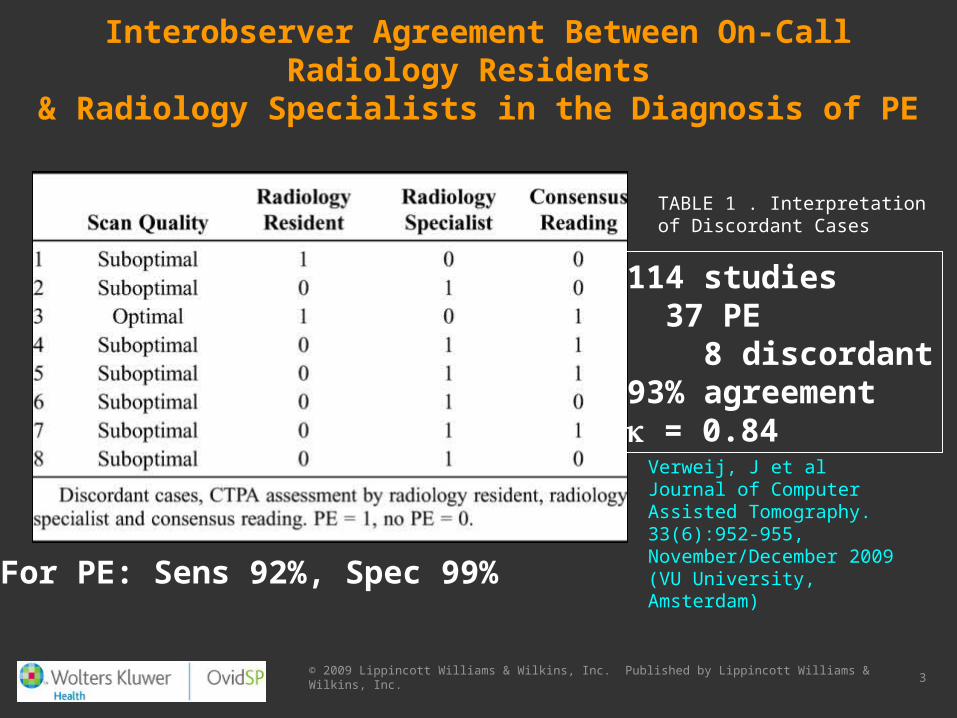
Interobserver Agreement Between On-Call Radiology Residents & Radiology Specialists in the Diagnosis of PE
Verweij, J et alJournal of Computer Assisted Tomography. 33(6):952-955, November/December 2009(VU University, Amsterdam)
TABLE 1 . Interpretation of Discordant Cases
114 studies 37 PE 8 discordant93% agreement = 0.84
For PE: Sens 92%, Spec 99%
Page 10
Discordance between CT and Angiography in the PIOPED II Study• Discordance in 20 of 226 CTA & cath results
• 40 hr interval: thrombi can remain the same, resolve, develop, or result from angio
Wittram C. et al (MGH & Wisc) Radiology (Sep)2007;244:883-889.
Page 11
VARIABLE Points
Clinical DVT 3
No alternative Dx 3
HR > 100 bpm 1.5
Imobil/Surg 4 wks 1.5
Previous DVT/PE 1.5
Hemoptysis 1
Cancer 1
CLINICAL PROBABILITY
points
Low < 2
Intermediate 2-6
High > 6
Wells PS al Thromb Haemost 2000;83:416-420
Predicting probability of PE Diagnostic Approach
Page 12
Predicting probability of PE
CLINICAL PROBABILITY
points
Low < 2
Intermediate 2-6
High > 6
Fedullo & Tapson. NEJM 2003;349:1247 (UCSD)
Recommendation
• D-Dimer
• CTPAif equivocal VQ & US
Page 13
Tapson V. N Engl J Med 2008;358:1037-1052
Diagnostic Approach to Suspected Acute Pulmonary Embolism
2008
Page 14
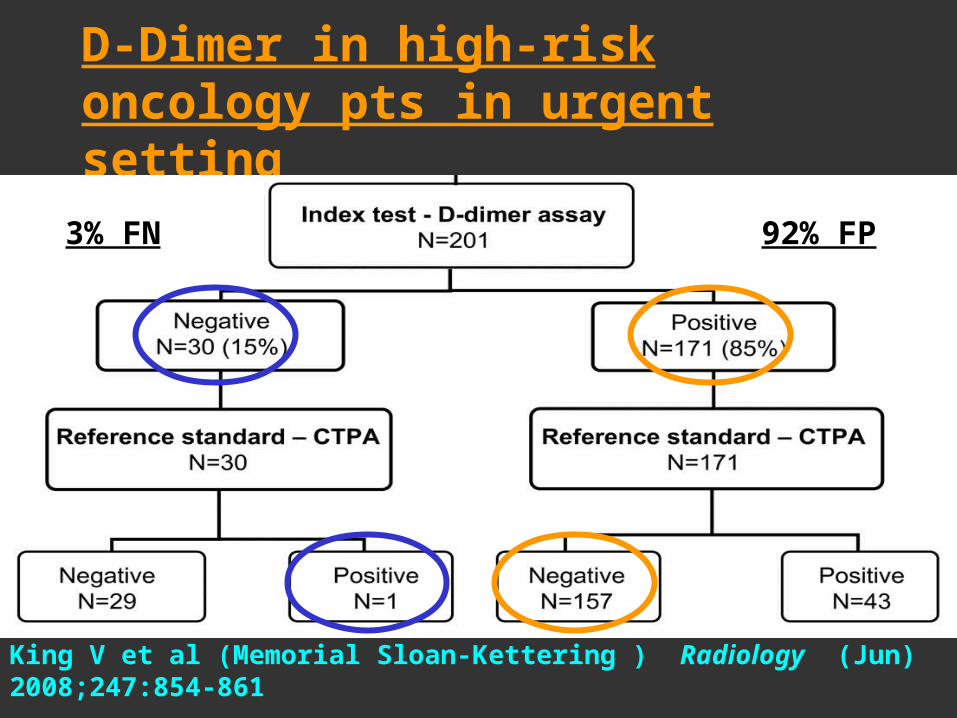
D-Dimer in high-risk oncology pts in urgent setting
King V et al (Memorial Sloan-Kettering ) Radiology (Jun) 2008;247:854-861
92% FP3% FN
Page 15
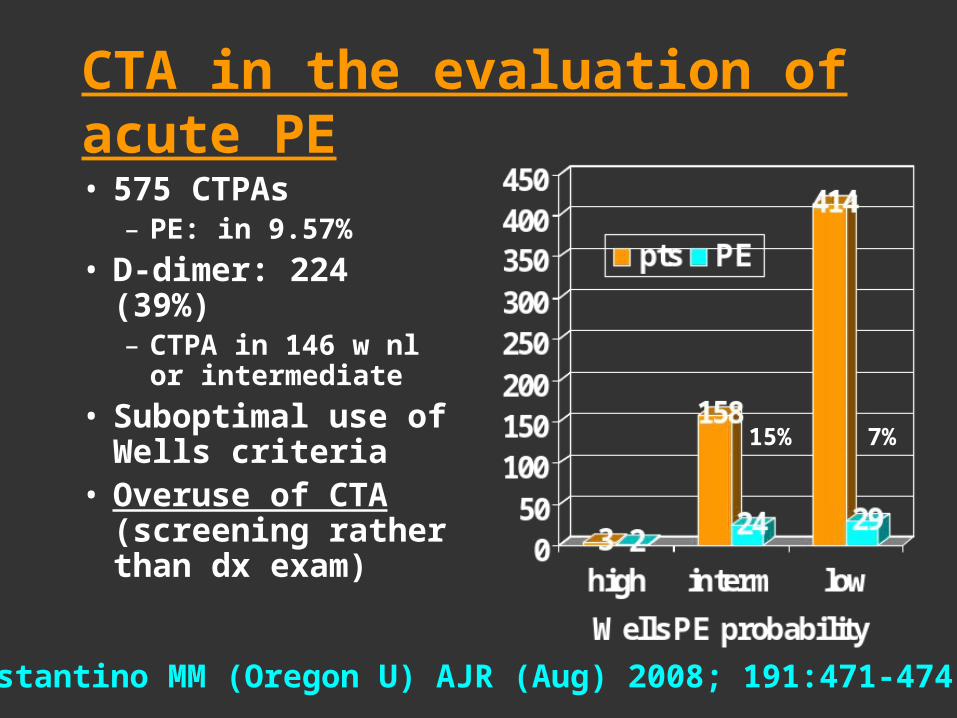
CTA in the evaluation of acute PE
• 575 CTPAs– PE: in 9.57%
• D-dimer: 224 (39%)– CTPA in 146 w nl or
intermediate
• Suboptimal use of Wells criteria
• Overuse of CTA (screening rather than dx exam)
Costantino MM (Oregon U) AJR (Aug) 2008; 191:471-474
15% 7%
Page 16
Copyright © 2009 by the American Roentgen Ray Society
Corwin, M. T. et al. AJR 2009 May;192:1319-1323 (Brown U)
Use of D-Dimer to Determine Need for CT
Page 17
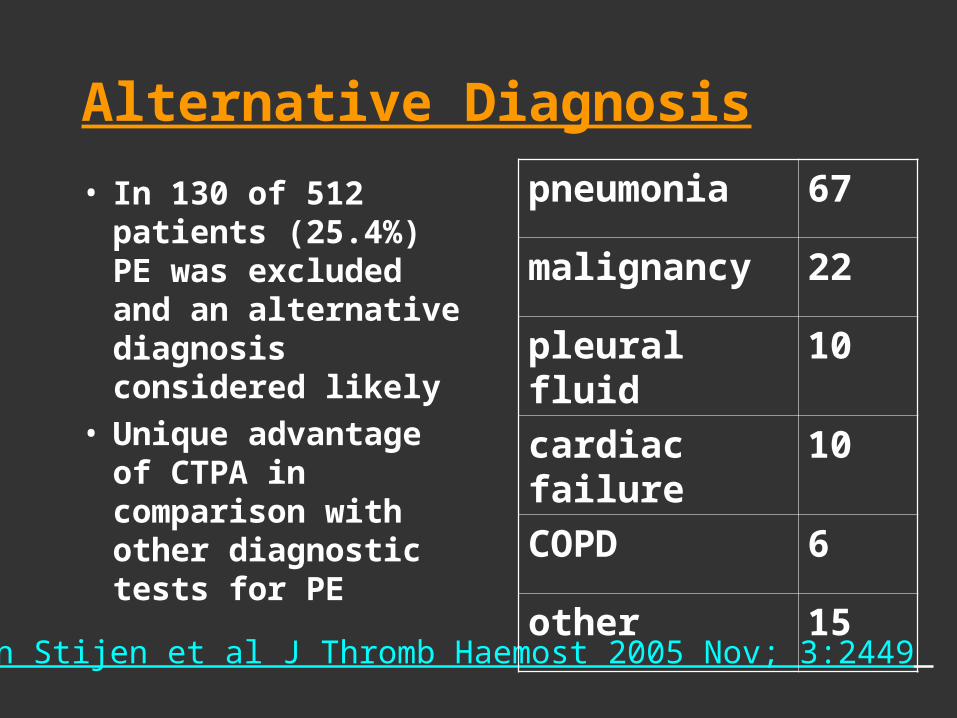
Alternative Diagnosis
• In 130 of 512 patients (25.4%) PE was excluded and an alternative diagnosis considered likely
• Unique advantage of CTPA in comparison with other diagnostic tests for PE
Van Stijen et al J Thromb Haemost 2005 Nov; 3:2449
pneumonia 67
malignancy 22
pleural fluid 10
cardiac failure 10
COPD 6
other 15
Page 18
Copyright © 2009 by the American Roentgen Ray Society
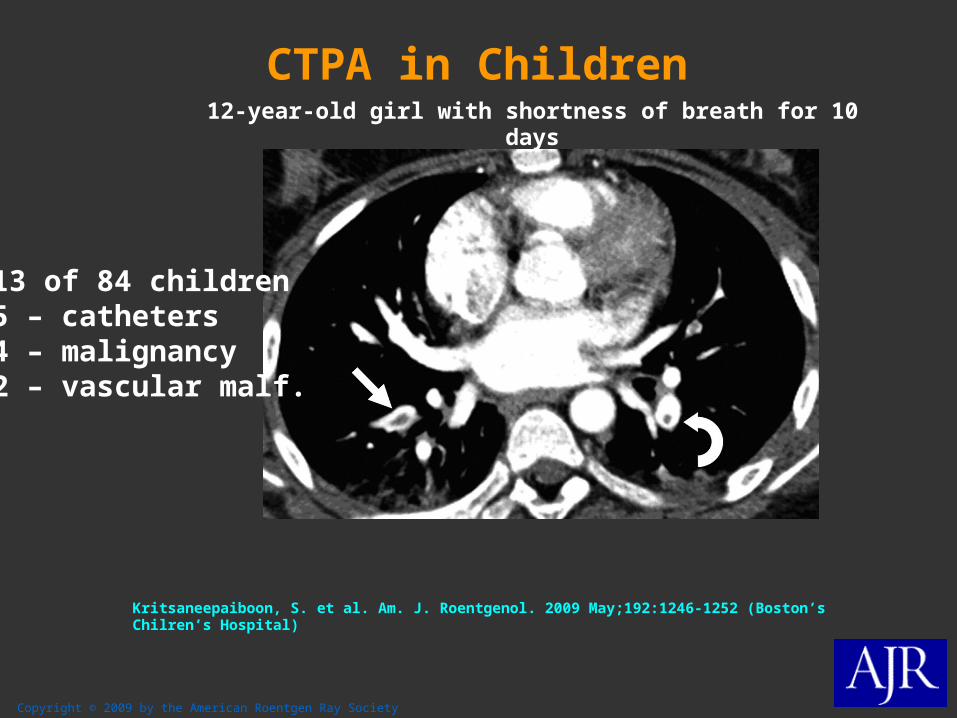
Kritsaneepaiboon, S. et al. Am. J. Roentgenol. 2009 May;192:1246-1252 (Boston’s Chilren’s Hospital)
12-year-old girl with shortness of breath for 10 days
13 of 84 children5 – catheters4 – malignancy2 – vascular malf.
CTPA in Children
Page 19
Copyright © 2009 by the American Roentgen Ray Society
Lee, E. Y. et al. Am. J. Roentgenol. 2009 Sep ;193:888-894 (Boston’s Children’s)
--Bar graph shows frequency and types of alternative diagnoses identified in children
with clinically suspected but excluded pulmonary embolism (n = 96)
CTPA in Children – Alternative Dx
Page 20
Increased use of CTPA
• Pennsylvania: from 1997 to 2001
• Mean 0.004% in CTPA per year
use associated with lower severity of illness and lower mortality(from 13% to 10%)
20.4
30.627.4
38.6
0
5
10
15
2025
30
35
40
PE/100,000 CTs/100 pts
incidence of PE & use of CT in hospitalized patients
1997 2001
DeMonaco NA et al (Pittsburgh) Am J Med (Jul) 2008;121:611-7
Page 21
Role of CT & NM in Work up of PE
3.5 0.6
3.8 0.7
3.4 0.6
2.8 0.3
3.8 0.7
3 0.3
3.9 0.8
0 1 2 3 4 5
All
Academic
Non_Acad
Rural
Urban
Small
Large
% of pts w/ symptoms having tests in 2005 (n= 3.270)
CT
NM
Bhargavan M et al (Johns Hopkins) AJR (Nov) 2009;193:1324-32
Page 22
Technique
MDCT Pulmonary Angiography
Page 23
Technique at BIDMC
• 80 - 100 mL at 4 mL/sec– (Scan duration + 3) x Inj. Rate
• Trigger at LA (100 HU)
• Shallow inspiration
• 1/2 sec rotation
• 120 kVp (?80)
• Variable mA (NI ~16)
• Scan acquire: 0.5 mm
• Scan display: 2.5 – 5 mm
• Axial, Coronal & Sagittal
Page 24
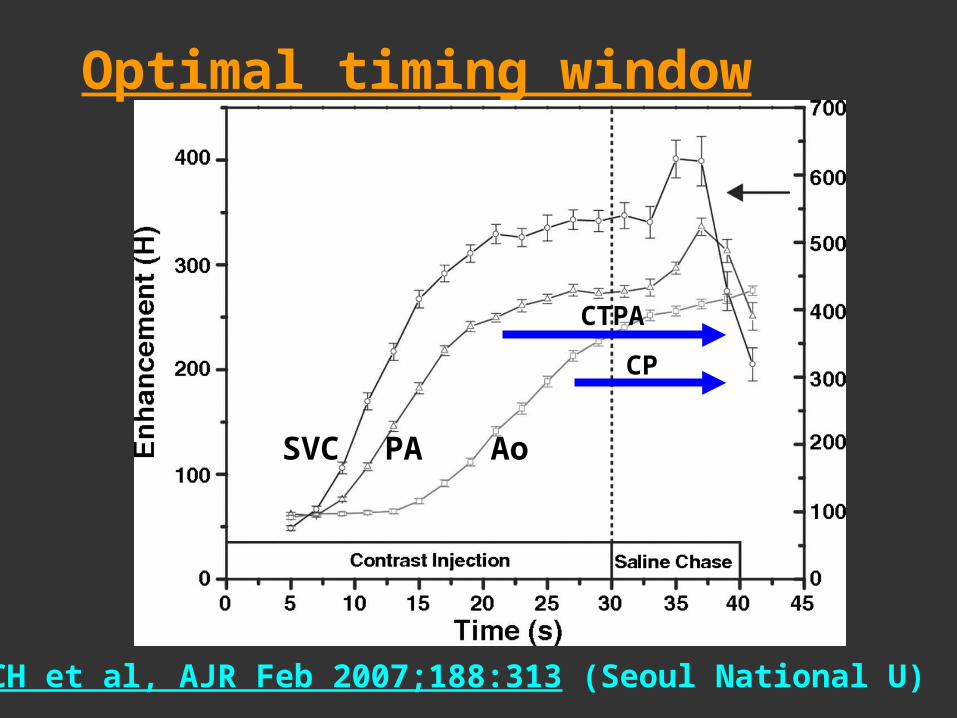
Optimal timing window
Lee CH et al, AJR Feb 2007;188:313 (Seoul National U)
SVC PA Ao
CTPA
CP
Page 25
Deep inspiration Shallow inspiration
Chest pain: Ao & PA
Page 26
Iodine delivery rate
Keil S et al. (Aachen U) Eur Radiol (Aug) 2008;18:1619-5:
A: 148 ml300 mgI/ml @ 4.9 ml/sB: 120 ml:370 mgI/ml @ 4.0 ml/s
Iodine delivery rate:1.47 vs. 1.48 gI/s
Adjust injection rate
I+ consentration & speed of injection Proportional to vessel enhancement
Page 27
Alternative IV contrast: Gadolinium
Remy-Jardin M et al. Radiology 2006; 238:1022
0.3-0.4 mmol/kg at 6 ml/sec – 15 ml saline flush80-100 kVp
Page 28
CAD in PE: Influence on radiologists performance
0
20
40
60
80
100
R1 R2 R3
33 pts w 215 thrombi
Rad R+CAD
Das M et al (U Aachen) Eur Radiol (Jul) 2008; 18:1350-5
Page 29
PE Detection w/ Dual Energy CT
Zhang L et al. Radiology 2009 Jul;252:61-70 (Nanjing U, China)
©2009 by Radiological Society of North America
Page 30
PE Detection w/ Dual Energy CT
Zhang L et al. Radiology 2009 Jul;252:61-70 (Nanjing U, China)
©2009 by Radiological Society of North America
CTPA w/ dual-energy & Blood flow merge
Images show a true-positive case of PE in rabbit
Page 31
Copyright © 2009 by the American Roentgen Ray Society
Thieme, S. F. et al. Am. J. Roentgenol. 2009 Jul;193:144-9 (Ludwig Maximilian U, Munich)
Dual Energy CT for Iodine distribution
--41-year-old woman with pulmonary embolism
Occlussive thrombus
Page 32
Thromboembolic Disease - DVT
Page 33
Indirect CT Venography
Sens & Spec CTA 86% & 96% +Ven 90% & 95%
Stein et al NEJM 2006;354:2317
CTA + Venography Dx VTE by 27%
Ghaye et al Radiology 2006;249:256
Minimal benefit from venography
Johnson et al Emerg Radiol 2006;12:160
Perrier A, Roy P-M, Sanchez O et al. NEJM 2005; 321:1760-8. (Geneva University)
Page 34
Routine indirect CT Venography in patients undergoing CTPA• Pts: 446 high risk - 383 low risk
– malignancy, h/o VTE & CV, post surgery
• Incremental value of CTV: 3.4%– 0.72% in low-risk & 2.6% in high-risk
• CTV may only be useful in patients with a high probability for PE
Andetta R et al (BWH) AJR (Feb) 2008; 190: 322 - 326
Page 35
Indirect CT Venography. Include the pelvis?• no difference in the
detection of VTE whether or not the pelvis is included
• 2074 pts:
• 383 VTE– (237 PEs + 46 DVT only)
• Isolated pelvic DVT: 2
Kalva SP et al. (MGH): Radiology (Feb) 2008;246:605-611
Page 36
CTV and US are diagnostically equivalent: data from PIOPED II
Goodman LR et al AJR (Nov) 2007; 189:1071-1076
Parameter US pos (%) US neg (%) Total
CTV pos 81 (11) 17 (2) 98
CTV neg 15 (2) 598 (84) 613
Total 96 615 711
Page 37
CT Venography 2009 – 64 MDCT
50
3
914
0
10
20
30
40
50
PE- PE+
DVT and PE (n = 306)
DVT-
DVT+
Nazaroglou,H AJR (Mar) 2009; 192:654-661
Page 38
CT Venography 2009 – Selective Use
• High risk patients – Signs of DVT or previous DVT
• Severely ill or ICU patients– Increased suboptimal studies
• Recent surgery in pelvis
• Cast or extremity surgery
• Can not do US
Goodman LR AJR (Feb) 2009; 250:327-330
Page 39
Radiation& Image Quality
Page 40
Brenner D and Hall E. N Engl J Med 2007;357:2277-2284
Estimated Number of CT Scans Performed Annually in the United States
CT
• 1991-96: ~ 0.4% of all cancers in the US
• Adjusting for current use: 1.5 to 2.0%
Estimated cancersfrom CT
Page 41
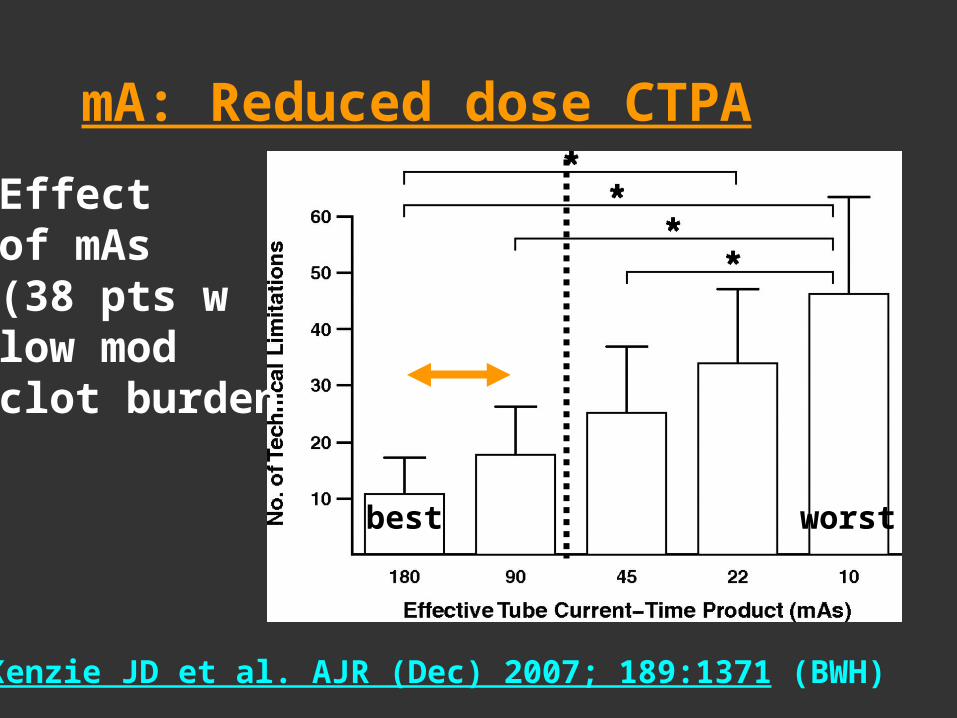
mA: Reduced dose CTPA
MacKenzie JD et al. AJR (Dec) 2007; 189:1371 (BWH)
Effect of mAs(38 pts wlow mod clot burden)
best worst
Page 42
kVp: image quality and radiation at CTPA with 100- or 120-kVp
• Prospective, randomized study
• 2 groups of 30 pts• 200 mA• 80 mL IV contrast
• Effective dose:
1.37 vs 2.44 mSv (↓ 44%)
Heyer CM et al. (U Bochum, Germany) Radiology (Nov) 2007;245:577
Page 43
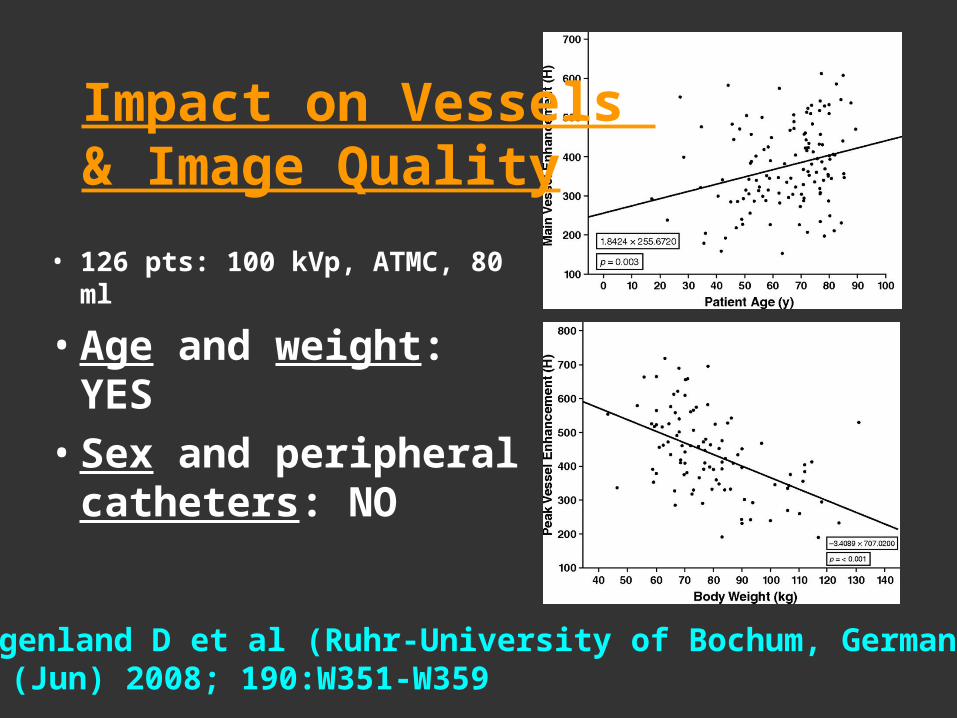
• 126 pts: 100 kVp, ATMC, 80 ml
• Age and weight: YES
• Sex and peripheral catheters: NO
Roggenland D et al (Ruhr-University of Bochum, Germany) AJR (Jun) 2008; 190:W351-W359
Impact on Vessels & Image Quality
Page 44
80 vs 120 kVp
Characteristics 120 kVp 89 kVp P
Main PA HU 309 376 < 0.001
Noise in HU 19 25 <0.001
Image quality 3.8 3.9 NS
n = 400 scans energy attenuation because high atomic # of I and K-edge
Matuoka S et al AJR 2009 Jun; 192:1651-6 (BWH, Harvard U)
Page 45
Copyright © 2009 by the American Roentgen Ray Society
Hurwitz, L. M. et al. Am. J. Roentgenol. 2009 Jan;192:244-253 (Duke U)
Bismuth Breast shields
chest phantom (n1 Lungman, Kyoto Kagaku Company)
May dose to breast by 30%
Page 46
CTPA in Pregnancy
Page 47
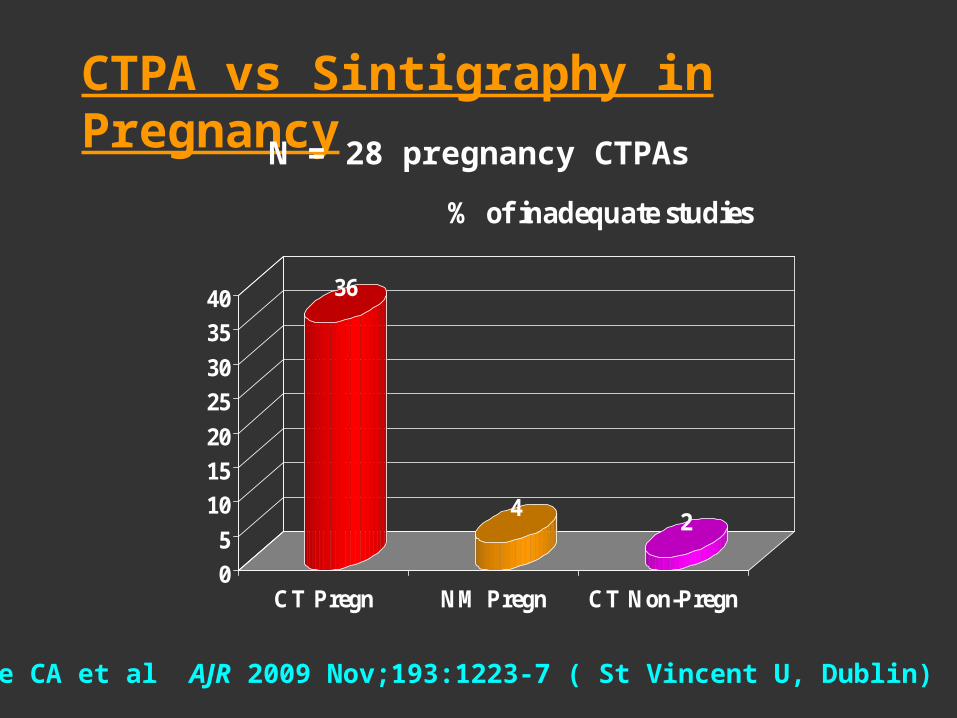
CTPA vs Sintigraphy in Pregnancy
36
42
0
5
10
15
20
25
30
35
40
CT Pregn NM Pregn CT Non-Pregn
% of inadequate studies
Ridge CA et al AJR 2009 Nov;193:1223-7 ( St Vincent U, Dublin)
N = 28 pregnancy CTPAs
Page 48
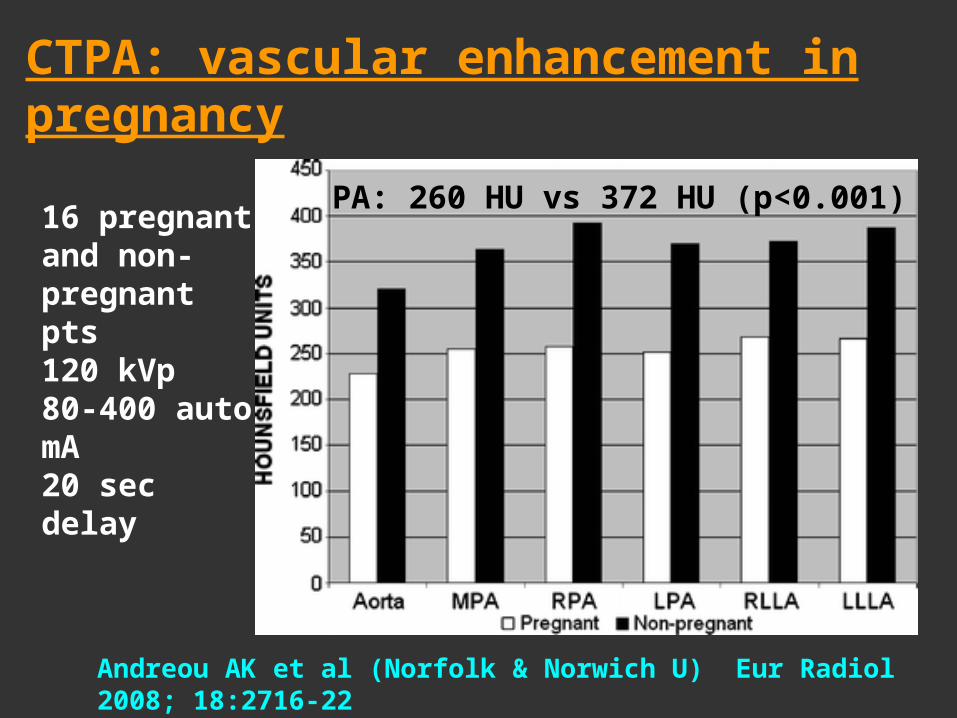
CTPA: vascular enhancement in pregnancy
Andreou AK et al (Norfolk & Norwich U) Eur Radiol 2008; 18:2716-22
16 pregnant and non- pregnant pts120 kVp 80-400 auto mA20 sec delay
PA: 260 HU vs 372 HU (p<0.001)
Page 49
KVP Pregnancy CTPA at BIDMC
• No C-
• 100 mL at 4 mL/sec
• Delay: 15 sec
• 100 kVp
• 200 mA
Litmanovich et al. JCAT (in press)
Page 50
© 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 9
Dose Reduction in Pregnancy
Litmanovich, Diana et al BIDMC JCAT 33(6):961-966, November/December 2009. (BIDMC, Harvard)
FIGURE 2 . Per-patient distribution of DLP values in both the control and the pregnancy groups. Individual DLPs demonstrate substantial difference between the 2 groups, with substantially higher DLPs seen in the control group compared with the pregnancy group.
Effective Dose (mean)105 mGy-cm 576 mGy-cm 1.8 mSv 9.8 mSv
Page 51
Pregnancy CTPA
270
280
290
300
310
320
330
PA LLL Ao
Pregnant Contols
Litmanovitch et al: JCAT 33(6):961-966, November/December 2009 (BIDMC, Harvard)
Vessel Attenuation Signal to noise
Page 52
Pregnancy CTPA – Fetal shielding
• Phantom experiment• 30% barium
Yousefzadeh HT et al. (U Chicago)
Radiology 2006; 239:751
• Pair of lead aprons
Ibal GR et al (Leeds) Br J Radiol (Jun) 2008;81:499-503
Page 53
Guidelines for CT & MRI use in pregnancy (UCSF)
• Appendicitis: US (if neg consider MRI or CT) • PE: CT *• Renal colic: US • Trauma: US &/or CT (if serious injury is suspected)• Low-dose CT pelvimetry • Iodinated contrast seems safe – iv gadolinium is
contraindicated (only when absolutely essential) • Continue breast-feeding immediately after I or gad• Teratogenesis is not a major concern • Carcinogenesis is a potential risk
Chen MM et al (UCSF). Obstet Gynecol (Aug) 2008; 112:333-40
* also Fleischner Society
Page 54
CTPA in Pregnancy
• bolus triggering with short start delays,
• high flow rates or high contrast medium concentration,
• preferential use of fast CT systems and
• the use of low kVp CT techniques.
• shallow respiration
Schaefer-Prokof C & Procof M (Amsterdam & Ultrecht MC)Eur Radiol 18:1705-6
Page 55
CTPA Imaging Findings
Page 56
Acute PE – CTPA Findings
• Occlusion or filling defect– Branching – Multiple – more than 1 level
• Vessel enlargement• Polo-mint or railway track• Acute angle• High attenuation (C-)• Ancillary
– Wedge shape opacities– Linear bands– Oligemia
central, bilateral PE
Wittram C, et al. RadioGraphics 2004; 24:1219Patel S & Kazerooni EA. AJR 2005;185:135
Page 58
Subsegmental PE
polo mint
Page 59
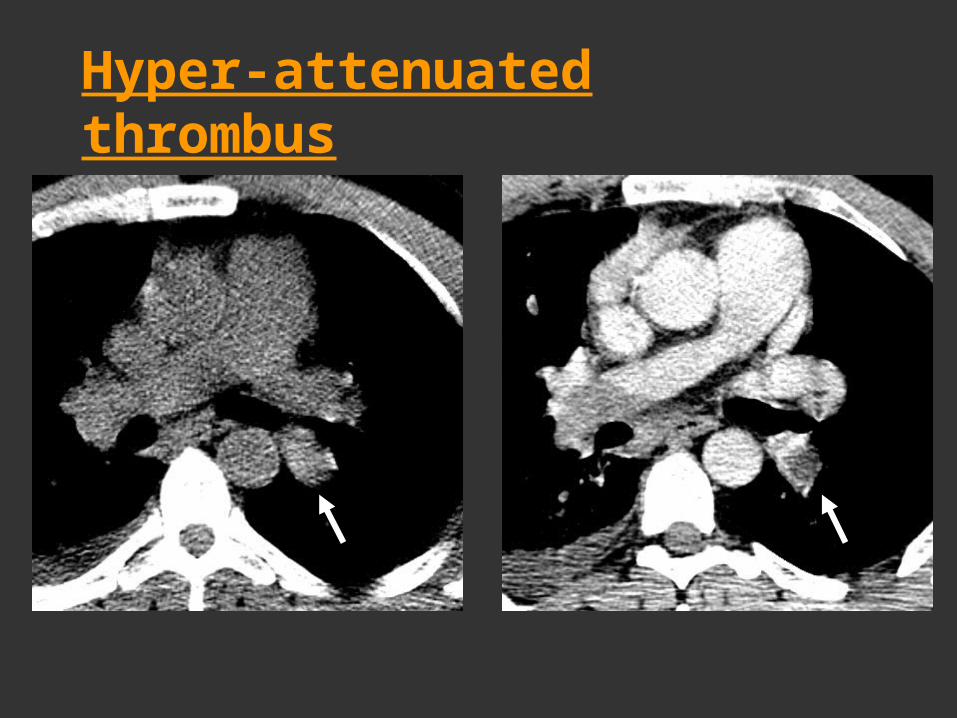
Hyper-attenuated thrombus
Page 60
Pulmonary InfarctionCentral Lucencies: 98% specificity & 46% sensitivity
Revel , MP et al Radiology 2007;244:875-882
Page 61
Pulmonary Infarction
Revel , MP et al (Université Paris Descartes). Radiology (Sep) 2007;244:875-882
0 10 20 30 40 50 60
Vessel sign
Central lucencies
Air bronchogr.
Triangular shape
per cent
PE (50 pts) Ctrl (100 pts)
Page 62
Acute PE: Ground Glass Opacities
Thoma P et al. Radiology 2009 Aug;250:721-729 (Erasmus U)
©2009 by Radiological Society of North America
Acute PE induces GGO in unobstructed lung zones.
Redistribution of blood flow
Given constant cardiac output this happens at a pressure consistent with pulmonary edema
Page 63
Pitfalls – Misdiagnosis
Technical• Poor bolus • Resp & Cardiac motion• High-Res. algorithm • Noisy images (large pts)• Streak artifacts (lines,
tubes, arms)• Beam hardening (SVC
dense contrast)
Interpretation• Lymph nodes• Pulmonary vein,• Mucoid impaction in
bronchi• Partial Volume
averaging • Tumor emboli
Wittram C, et al. RadioGraphics 2004; 24:1219Patel S & Kazerooni EA. AJR 2005;185:135
Page 64
Technical Poor bolus, large patient, noisy imageProblems in subsegmental vessels
Page 65
TechnicalBeam hardening from SVC High-resolution algorithm
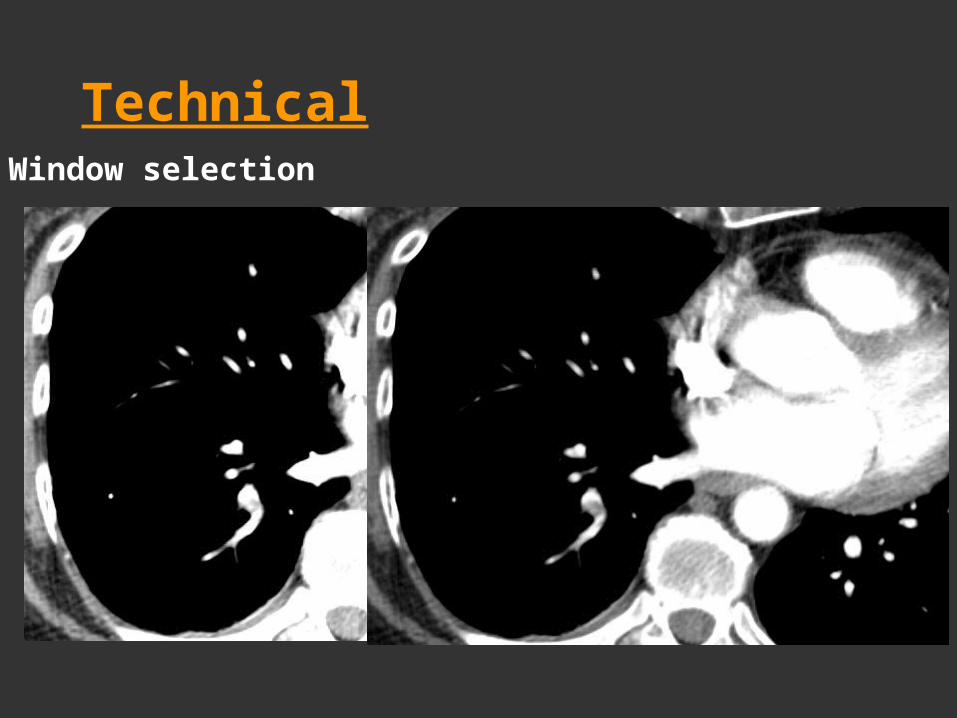
Page 66
TechnicalWindow selection
Page 67
InterpretationLymph nodes
Page 68
InterpretationPartial volume Tumor emboli
Page 69
InterpretationMucoid impaction
Page 71
PE Occlusion Index
Qanadi et al. AJR 2001;176:1415 (U René Decatres, Paris)
• 10 segments in each lung• Obstruction factor (OF):
– 0=no, 1=partial, 2=total
• Max obstruction = 40• Occlusion index:
[(Segments x OF)] / 40
Page 72
PE Outcome: prospective evaluation of CTPA clot burden & ECG score
• 105 PE of 523 CTPA. 13 deaths in 12 mo• No statistically significant association between
ECG score and CTPA clot burden at diagnosis and the 12-month all-cause mortality rate
dead alive
mean ECG score 2.4 2.03
mean clot burden 24% 22%
Subramaniam RM et al (Mayo) AJR (Jun)2008; 190:1599-1604
Page 73
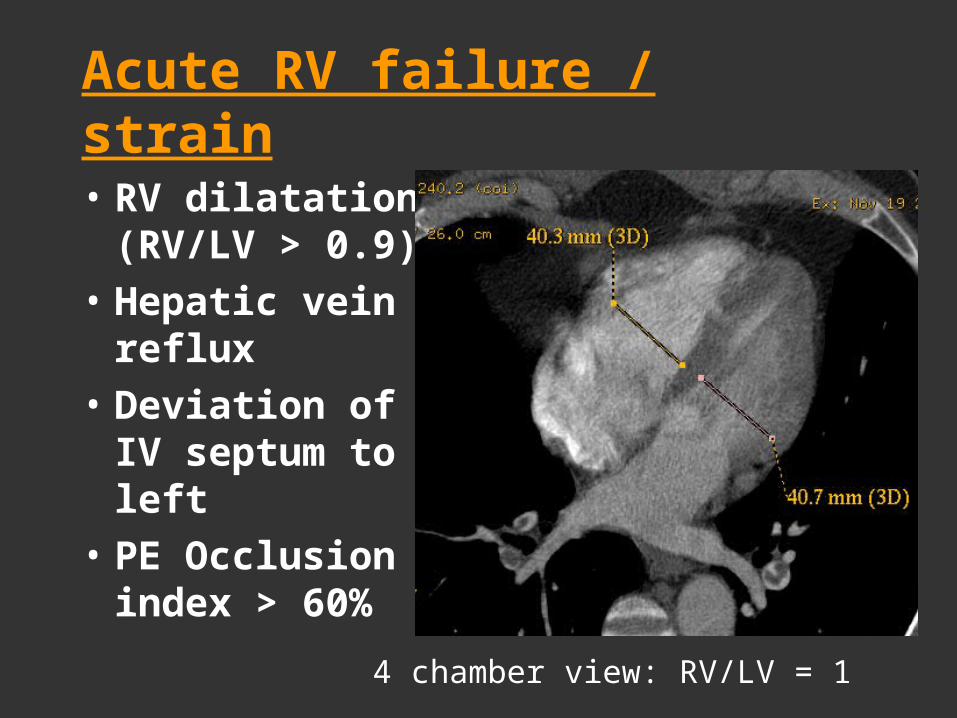
Acute RV failure / strain
• RV dilatation (RV/LV > 0.9)
• Hepatic vein reflux
• Deviation of IV septum to left
• PE Occlusion index > 60%
4 chamber view: RV/LV = 1
Page 74
Acute RV failure / strainDeviation & bowing of septum to left – IVC & hepatic vein reflux
Page 75
Copyright ©Radiological Society of North America, 2008
Lu, M. T. et al. Radiology 2008;246:281-287
Interval increase in RV/LV diameter ratios at CT as mortality predictor
Page 76
Small PE
Incidental Subsegmental PE (ISPE)
Page 77
Small Pulmonary Emboli
25
42
2
106
19
2
61
50
20
40
60
80
100
120
ISPE (67p) Inconcl (125p) Anticoag.
Clinicians' Response to Radiologists' Reports
No RxRXReturned
Eyer BA, et al AJR Feb 2005; 184:623-628. (Medical College of Wisconsin)
Page 78
Small Pulmonary Emboli
Rx• Inadequate
cardiopulmonary reserve
• Acute DVT• Recurrent small PE
Withhold Rx • No or few risk factors
for VTE • Transient (surgery)
rather than persistent (cancer) risk factors
• Other CV disease that can explain symptoms
• Negative D-dimer
Goodman LR. Radiology 2005; 234:654 (Editorial) (Medical College of Wisconsin)
Page 80
Chronic Pulmonary Thromboembolism
Pulmonary artery• Occlusion• Eccentric thrombus• Crescent – obtuse• Thick wall• Band or web• CalcificationCollateral systemic• Bronchial etc
Pulmonary hypertension• ↑ PA > 29 mm (≥Ao)• ↑ RV (≥ LV)Parenchyma• Scars & pleural thickening• Mosaic pattern• Air trapping• Bronchiectasis
Wittram C, et al. RadioGraphics 2004; 24:1219Patel S & Kazerooni EA. AJR 2005;185:135Castaner E, et al. RadioGraphics 2009; 29:31
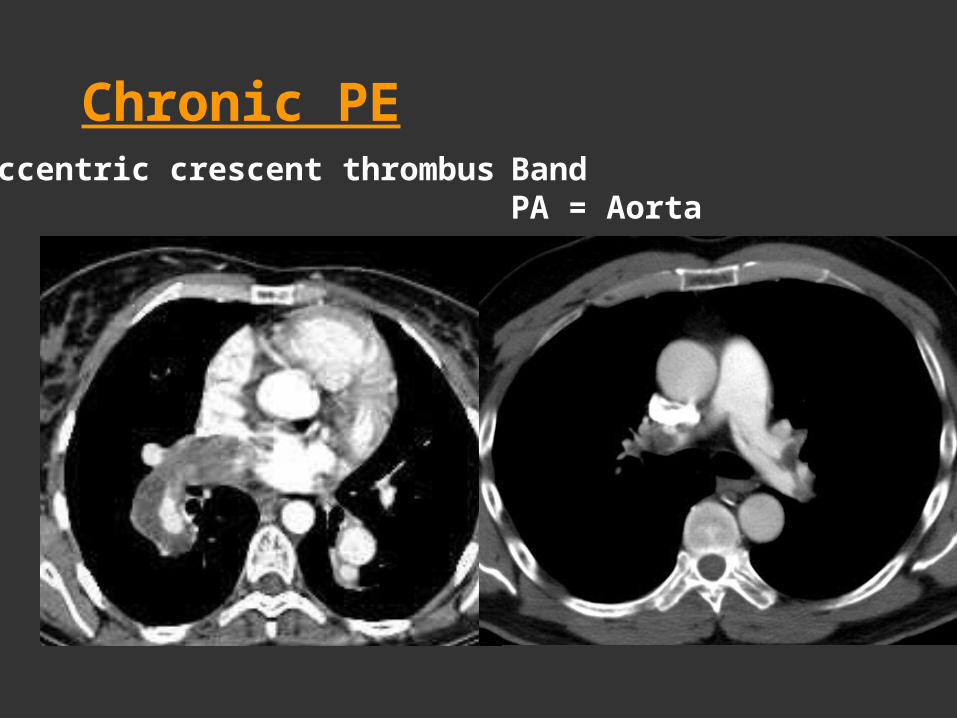
Page 81
Chronic PEEccentric crescent thrombus Band
PA = Aorta
Page 82
Chronic PEBronchial arteries, PA > Ao Thrombus calcification
Page 83
Chronic PEScars & pleural thickening
Page 84
Chronic PEMosaic pattern
Page 86
Triple Rule out: >250 HU PA, Ao & coronaries
Frauenfelder T et al (U Zurich) Eur Radiol 2008;on line
Page 87
Chest pain CTA regiments
0
50
100
150
200
250
300
350
400
HU
PE Dissection Chest pain Gated
Mean attenuation in PA & Aorta
PA
Ao
Raptopoulos et al AJR 2006 (Jun, sup); 186:S346-56 (BIDMC)
Page 88
Retrospective ECG gating
• Continuous data acquisition. Coronary imaging & function
• Only 20% used for coronary imaging (waste)
• Low pitch (~ 0.3) contributes to high radiation
• With ECG modulation mA drops to ~ 45% in the out-of-phase part of the cardiac cycle ( 30% in radiation)
Weustink A C et al. (Erasmus)Radiology 2009;252:53-60
©2009 by Radiological Society of North America
Page 89
Litmanovich D et al, Eur Radiol 2008 (Feb) 18:308-17 (BIDMC)Litmanovich D et al, Eur Radiol 2008 (Feb) 18:308-17 (BIDMC)
ECG Modulated Chest CTA: 25 ± 7 mSv
Gated Chest – triple R/OGated Chest – triple R/O
Page 90
Gated Chest CTA
Litmanovitch et al, Eur Radiol 2008(Feb);18:308-17 (BIDMC)
56 pts (50-80 y)•25 normal •20 lung or pleura•11 vascular•16 coronary
Page 91
"Triple Rule-Out" CoCTA protocol in ED pts w ACS• 197 Low-to-Moderate Risk ED patients
• 30 day follow up
• Important non coronary dx : 22 (11%)
• Important incidental dx : 27 (14%)
• Moderate & severe CAD : 22 (11%)
• Preclude additional cardiac testing in 175 pts
Takakuwa KM & Halpern EJ (Thomas Jefferson U): Radiology (Aug) 2008;248:438-446
Page 92
Prospective ECG gating
• ECG is used to plan timing • 10% - 30% of the cardiac cycle. • 64-row scanner (4 cm scanning
span), 16 cm span for cardiac imaging is scanned in 7 cycles: step and shoot
• dropped radiation of CCTA to <5 mSV ~ Chest CT and < CCA & nuclear medicine.
• CCTA – becomes a viable clinical tool
Earls J P et al. Radiology 2008;246:742-753 (Fairfax)
©2008 by Radiological Society of North America
Page 93
2 separate tests?
Low dose prospective gated64-row MDCTPA
Page 94
Gated Chest – triple R/O
• Fujioka C et al from Hiroshima U (AJR July 2009) 100 kV; 30 pts– estimated effective dose
~7.5 mSv.
• Shuman W et al at the U Washington (AJR June 2009) prospective CTA in 41 pts w/o & 31 w/ prosp gating:– mean effective dose 32 vs
for 9 mSv
0
10
20
30
40
50
60
70
1 2 3 4
Retro Prosp
Copyright © 2009 by the American Roentgen Ray Society
Shuman, W. P. et al. AJR 2009;192:1662-1667
CA image quality.CA image quality.
Page 95
Triple R/O: Scan setup and bolus-tracking images
Halpern E J Radiology 2009;252:332-345 (Thomas Jefferson U, Philadelphia)
©2009 by Radiological Society of North America
Page 96
TRO CT angiogram in 31-year-old woman with chest pain that was atypical for angina but without severe shortness of breath
Halpern E J Radiology 2009;252:332-345 (Thomas Jefferson U, Philadelphia)
©2009 by Radiological Society of North America
Page 97
TRO CT angiogram in 79-year-old woman with recent onset of vague chest discomfort
Halpern E J Radiology 2009;252:332-345 (Thomas Jefferson U, Philadelphia)
©2009 by Radiological Society of North America
Page 98
TRO CT angiogram in 51-year-old athletic man with no relevant cardiac history who presented with atypical chest pain while resting at home
Halpern E J Radiology 2009;252:332-345 (Thomas Jefferson U, Philadelphia)
©2009 by Radiological Society of North America
Page 99
TRO CT angiogram in a 74-year-old man with history of coronary disease and pulmonary embolism who presented with progressive chest pain over 6 months that became acutely
worse on the day of presentation
Halpern E J Radiology 2009;252:332-345 (Thomas Jefferson U, Philadelphia)
©2009 by Radiological Society of North America
Page 100
Conclusions
• CTPA an established test (including in pregnancy)• CTPA over utilized (preferred chest pain test) • Use D-Dimer in high risk pts moderately successful• Indirect venography, Small PE management &
Thrombus burden assessment: controversial• RV size changes: important prognostic sign• Iodine delivery rate, Shallow inspiration• Consider radiation risk, 100 kVp• Triple rule out




























































































![Presented by: [] Prof. Vassilios Makios [ v.makios@corallia.org ] General Manager Mechanisms & Support Measures than can be built within the structural.](https://static.documents.pub/doc/80x56/56649e225503460f94b0f69c/presented-by-prof-vassilios-makios-vmakioscoralliaorg-general-manager.jpg)




