CURICULUM VITAE. Name : Suharyo Hadisaputro, Prof.Dr.dr..Sp.PD-KPTI, FINASI Borne : Juana, March 10 , 1945 ; Position : Professor in Medicine Medical Faculty Diponeoro Univ Education : Doctoral in Medical (Public Helath),1990; - PowerPoint PPT Presentation
CURICULUM VITAE • Name :Suharyo Hadisaputro, Prof.Dr.dr..Sp.PD-KPTI, FINASI • Borne : Juana, March 10 , 1945; • Position : Professor in Medicine Medical Faculty Diponeoro Univ • Education : Doctoral in Medical (Public Helath),1990; Cosultan of Tropical Infectious Disease, 1986; Internal Medicine Spesialist, 1981; Medical Doctor, 1972; • Job Description (History) : Chief I of Researcher Tropical Infectious Disease Jkt; Chief of Researcher Tropical Infectious Disease Semg Chief of Program of Doctoral Medical & Health Undip. Chief Program of Magister Epidemiologiy Undip.
Transcript
CURICULUM VITAE • Name :Suharyo Hadisaputro, Prof.Dr.dr..Sp.PD-KPTI, FINASI• Borne : Juana, March 10 , 1945;• Position : Professor in Medicine Medical Faculty Diponeoro Univ• Education : Doctoral in Medical (Public Helath),1990; Cosultan of Tropical Infectious Disease, 1986; Internal Medicine Spesialist, 1981; Medical Doctor, 1972;• Job Description (History) : Chief I of Researcher Tropical Infectious Disease Jkt; Chief of Researcher Tropical Infectious Disease Semg Chief of Program of Doctoral Medical & Health
Undip. Chief Program of Magister Epidemiologiy Undip. Director of Postgraduate Program Diponegoro Univ;• Interest of Science : Field and Clinical Epidemiology Tropical I nfectious Disease; Epidemiology of Communicable Disease; Epidemiologiy of Non Communicable Disease; Epidemiology of Iodine Disorder Deficiency
International Seminar of Food and Water Borne Disease
September 17, 2012 in Semarang, Indonesia
Suharyo Hadisaputro
Outline of Presentation Introduction Significance & prevalence High Risk Circumstances &
(1) TYPHOID DAN SALMONELLOSIS : The sanitary factor and hygienic food and water take was responsibility on the increase of the morbidity of typhoid fever.
(2)DIARRHOEA : Many causes of diarrhoea, and the strain of Cholera Vibrio O 139 from Bangladesh was a potentially factor to increase the case of diarrhoea in Indonesia.
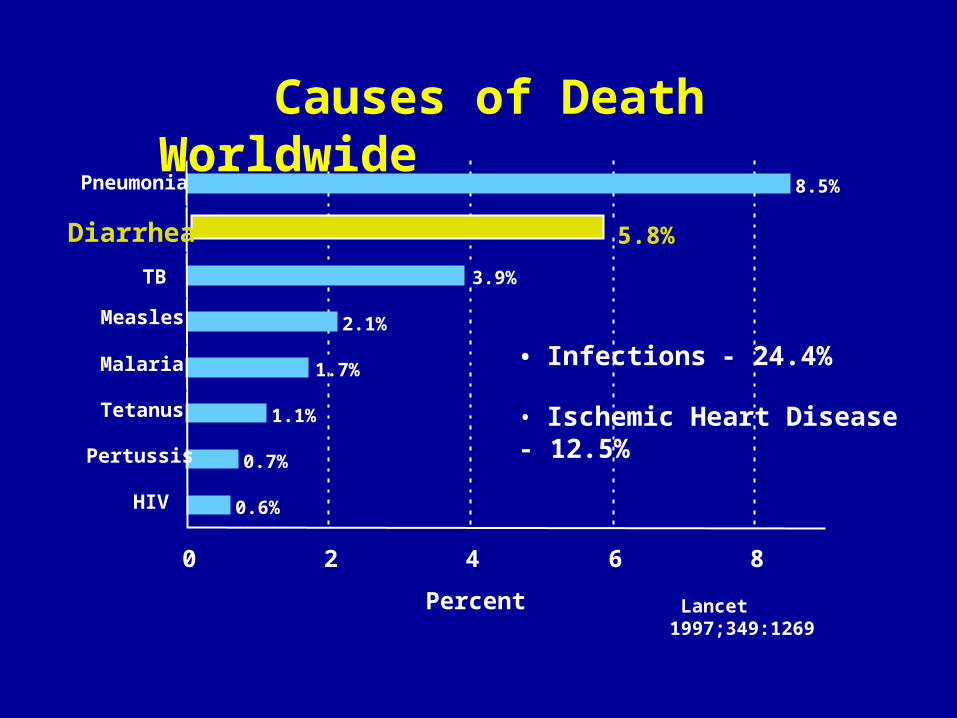
0.6%
0.7%
1.1%
1.7%
2.1%
3.9%
5.8%
8.5%
Lancet 1997;349:1269Percent0 2 4 6 8
HIV
Pertussis
Tetanus
Malaria
Measles
TB
Diarrhea
Pneumonia
• Infections - 24.4%
• Ischemic Heart Disease - 12.5%
Causes of Death Worldwide
TEN MAIN DISEASES IN INDONESIA URBAN/RURAL AREA
0 5 10 15 20 25
Metabolic D
Respiratory Inf
Other Inf
Trauma- Accident
Diarrhea
Bron-Emp-Asthma
Neoplasma
Digestive S
TBC
Circulatory S
UrbanRural
TEN MAIN DISEASES OF CAUSED OF DEATH IN INDONESIA
0 5 10 15 20
Malaria
Neoplasma
Sist Pencernaan
Trauma- Kerac-Kcl
Bronc-asma-emp
Peny Infeksi lain
Diare
Inf Sal Nafas
TBC
Peny Sist Sirkulasi
Risks in 3rd World Lack of safe water supply Contaminated foods Poor sanitation Overcrowding Malnutrition
Global Risks in the World
Traveller Diarrhoea HIV infection &
immunosuppression Day Care Centers: fomite spread
– Also affects staff, household contacts Nursing Home/Chronic Care
Facilities Antibiotics Achlorhydria/H2 blocker
Factors in Emergencies Lack of safe, clean water
supply Contamination of food supply Poor sanitation Overcrowding Malnutrition HIV infection &
immunosuppression
Overall Significance One of most common diseases in
world 3-5 billion cases of acute infectious
diarrhea annually Kills 5-10 million people/year In the U.S., more than 8 million
seek medical attention for diarrhea; costs $23 billion in medical expenses & lost wages
DIARRHEADiarrhea is a common
symptom that can range in severity from an acute, self-
limited annoyance to a severe, life-threatening illness.
Patients may use the term "diarrhea" to refer to increased
frequency of bowel movements, increased stool
liquidity, a sense of fecal urgency, or fecal incontinence
Definition διάρροια; literally meaning "through-
flowing" Stool looses its normal consistence Weight usually increases: >235g/d (♂),
>175g/d (♀) Frequency increases: >2/d Often associated with imperative urge to
defecate Can contain blood, pus and mucous
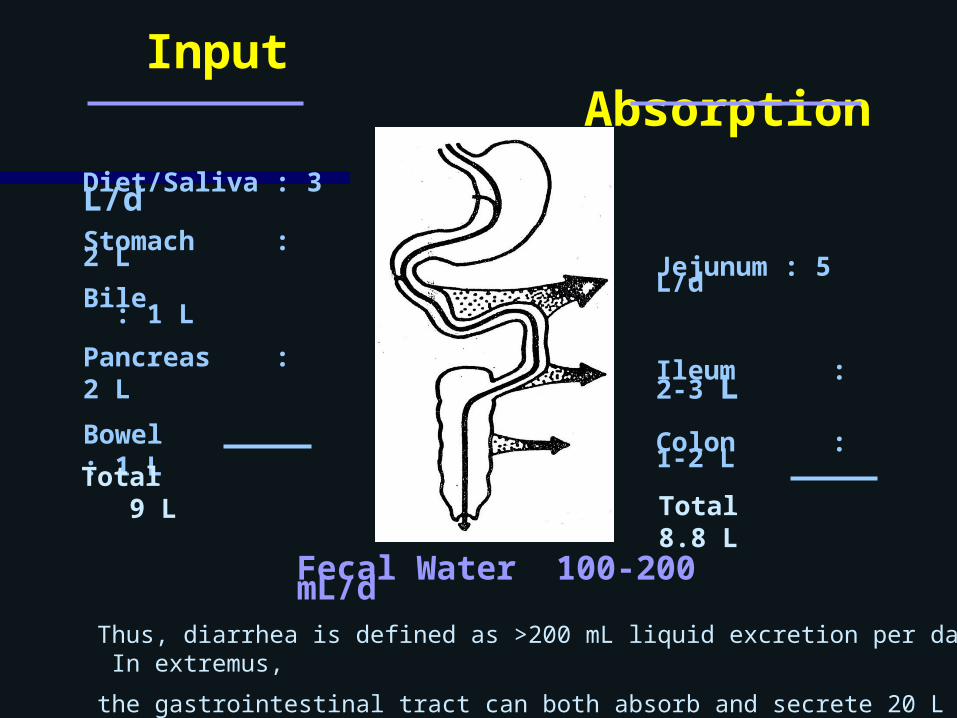
Definition In the normal state, approximately
10 L of fluid enter the duodenum daily, of which all but 1.5 L are absorbed by the small intestine. The colon absorbs most of the remaining fluid, with only 100 mL lost in the stool. From a medical standpoint, diarrhea is defined as a stool weight of more than 250 g/24 h
Input Absorption
Diet/Saliva : 3 L/dStomach : 2 L
Bile : 1 LPancreas : 2 LBowel : 1 L
Jejunum : 5 L/d
Ileum : 2-3 L
Colon : 1-2 L
Fecal Water 100-200 mL/d
Thus, diarrhea is defined as >200 mL liquid excretion per day. In extremus,
the gastrointestinal tract can both absorb and secrete 20 L of water per day.
Total 9 L Total 8.8 L
ACUTE DIARRHEA Diarrhea that is acute in onset
and persists for less than 3 weeks is most commonly caused by infectious agents, bacterial toxins (either ingested preformed in food or produced in the gut), or drugs
manifested initially by prolonged high fevers, prostration, confusion, respiratory symptoms followed by abdominal tenderness, diarrhea, and a rash is due to infection with Salmonella typhi or Salmonella paratyphi, which causes bacteremia and multiorgan dysfunction
Campylobacter Spread by contaminated water or
raw milk Causes patchy destruction of walls
of small and large intestines Diarrhea +/- blood, fever,
Applying the principle of hygiene Depend of the improvement of
income Cultural changes of personal
hygiene Many effort for control of TF, are : (1) Treatment and control of
sources infection : Adequate antibiotic treatment for active patients and carriers, special isolation in the hospital ?, desinfections of the excreta, sterilization of the patient’s linen etc.
CONTROL OF ENTERIC FEVER
(2) Improved on environment health
. To trace the source infection . To investigate of routes
transmis . Water purification/chlorination . Control of all exposed foods for sale in the market and store. . Reduction the house-flies
density . To avoid of having open
garbage pail etc.
CONTROL OF ENTERIC FEVER
(3) Supervision on food industries and restaurant
. Supervision on sanitation of places work and
food processin, equipment etc. . Prohibition to employ people who
infected . Routine examination of stool culture . To trace of food, if as medium
suspected . All milk and milk products should be pasteurized or boiled.
CONTROL OF ENTERIC FEVER
(4) Control of healthy population
. Supervision on hygiene of food and drink . Serving the food in hot condition . Health education for community . Providing the places for washing
hand . Conducting vaccination of EF in
endemic area, however, improvement of sanitation and health system is
very important role.
CONTROL OF ENTERIC FEVER
Choose foods processing for safety. Cook food thoroughly. Eat cooked food immediately. Store cooked food thoroughly. Reheat cooked food thoroughly. Avoid contact between raw and cooked
foods. Wash hands repeately. Keep all kitchen surfaces meticolously
clean. Protect foods from insects, rodents &
animals. Use pure water.
THE WHO GOLDEN RULES FOR SAVE FOOD PREPARATION
NO DISEASE
ASYMPTOMATIC DISEASE
CLINICAL COURSE
ONSETORDINARY DETECTION
LEVEL OF PREVENTION
PRIMARYRemove of risk factors
SECONDARYEarly detec-tion & prompt treatment
TERTIARYReduce complications
PREMORDUnderlying risk factors
Diarrheal disease most prevalent in developing countries, and costly.
In Indonesia incidence still high.
Transmission most of direct route.
Empiric treatment with ORT most often effective
The strategies of Diarrhea Control
SUMMARY OF DIARRHEA CONTROL
The strategies of Diarrhea Control are :
. Detection and control of source, . Disease surveillance, . Health education in community, . Improvement of hygiene