n engl j med 365;19 nejm.org november 10, 2011 1801
current concepts
Sudden, Unexpected Death in EpilepsyOrrin Devinsky, M.D.
From the Department of Neurology, NYU Langone School of Medicine, New York. Address reprint requests to Dr. Devinsky at the Department of Neurology, NYU Lan-gone School of Medicine, 223 E. 34th St., New York, NY 10016, or at [email protected].
Epilepsy is characterized by both recurrent seizures and clini-cal uncertainty. Paroxysmal symptoms unpredictably punctuate life. Although most people with epilepsy live full and productive lives, doctors may too read-
ily assure patients that seizures “never hurt the brain” and “are never fatal.” Over time, convulsive seizures can progressively impair cognition and behavior and alter brain structure.1 In rare cases, seizures can be fatal.
Sudden, unexpected death in epilepsy refers to a death in a patient with epilepsy that is not due to trauma, drowning, status epilepticus, or other known causes but for which there is often evidence of an associated seizure. The event may be un-witnessed, and the person is often found dead in bed. A finding of sudden, unex-pected death in epilepsy is definite when clinical criteria are met and autopsy re-veals no alternative cause of death, such as stroke, myocardial infarction, or drug intoxication, although there may be evidence of a seizure (e.g., a bitten tongue or pulmonary edema).2 Sudden, unexpected death in epilepsy is probable when clinical criteria are met but there is no autopsy, and it is possible when there is an alternative cause of death or when clinical data are lacking.3
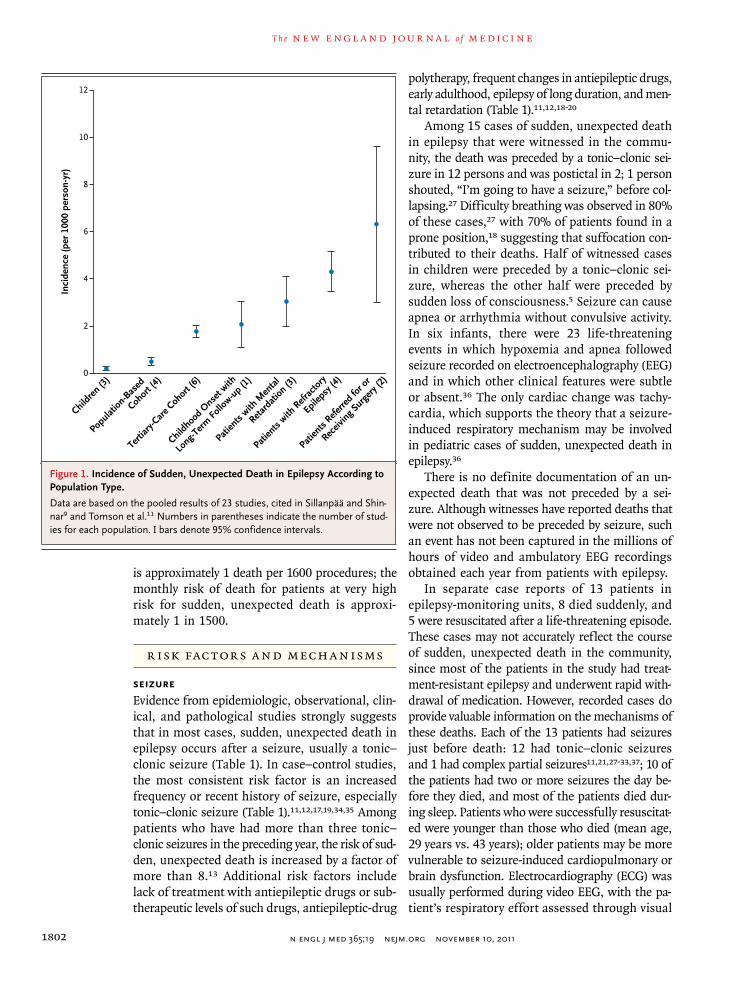
The incidence of sudden, unexpected death in epilepsy is probably underestimated because records and databases are incomplete and because it often goes unrecognized by coroners, medical examiners, and physicians who are unaware of the disorder or its diagnostic criteria. The incidence per 1000 patient-years varies with the sample population, increasing from 0.09 to 2.65 in community samples to 1.2 to 5.9 in tertiary care epilepsy centers to 6.0 to 9.3 among patients evaluated for or treated with surgery or vagus-nerve stimulation for epilepsy (Fig. 1).3-13 The rate of sudden, unexpected death increases with the duration and severity of epilepsy. It is much less common in children than in adults5,9,14; among children with epilepsy who are younger than 14 years of age, cases of sudden, unexpected death are rare and are largely restricted to children who have a major neurologic impairment or a history of a major neurologic insult.5,9,14 Like adults, most children in whom sudden, unexpected death in epilepsy is diagnosed die in bed and have a history of gener-alized tonic–clonic seizure.5 Sudden, unexpected death contributes to the increased mortality among children with disorders associated with both treatment-resistant epilepsy and developmental delay, such as autism, the Dravet syndrome, tuberous sclerosis complex, and chromosome 15q11-13 duplication.9,15,16
The magnitude of the problem of sudden, unexpected death in epilepsy is un-recognized in the medical and lay communities. In a population-based cohort of children with epilepsy who were followed for 40 years, sudden, unexpected death occurred in 9% of patients and accounted for 38% of all deaths.9 Although the epilepsy began in childhood, almost all the deaths occurred in adulthood. Among high-risk patients with major neurologic disorders (e.g., mental retardation or cere-bral palsy) or treatment-resistant epilepsy, rates of sudden, unexpected death can ex-ceed 10% per decade.4,9 By comparison, the risk of death from surgery for epilepsy
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 365;19 nejm.org november 10, 20111802
is approximately 1 death per 1600 procedures; the monthly risk of death for patients at very high risk for sudden, unexpected death is approxi-mately 1 in 1500.
R isk Fac t or s a nd Mech a nisms
SeizureEvidence from epidemiologic, observational, clin-ical, and pathological studies strongly suggests that in most cases, sudden, unexpected death in epilepsy occurs after a seizure, usually a tonic–clonic seizure (Table 1). In case–control studies, the most consistent risk factor is an increased frequency or recent history of seizure, especially tonic–clonic seizure (Table 1).11,12,17,19,34,35 Among patients who have had more than three tonic–clonic seizures in the preceding year, the risk of sud-den, unexpected death is increased by a factor of more than 8.13 Additional risk factors include lack of treatment with antiepileptic drugs or sub-therapeutic levels of such drugs, antiepileptic-drug
polytherapy, frequent changes in antiepileptic drugs, early adulthood, epilepsy of long duration, and men-tal retardation (Table 1).11,12,18-20
Among 15 cases of sudden, unexpected death in epilepsy that were witnessed in the commu-nity, the death was preceded by a tonic–clonic sei-zure in 12 persons and was postictal in 2; 1 person shouted, “I’m going to have a seizure,” before col-lapsing.27 Difficulty breathing was observed in 80% of these cases,27 with 70% of patients found in a prone position,18 suggesting that suffocation con-tributed to their deaths. Half of witnessed cases in children were preceded by a tonic–clonic sei-zure, whereas the other half were preceded by sudden loss of consciousness.5 Seizure can cause apnea or arrhythmia without convulsive activity. In six infants, there were 23 life-threatening events in which hypoxemia and apnea followed seizure recorded on electroencephalography (EEG) and in which other clinical features were subtle or absent.36 The only cardiac change was tachy-cardia, which supports the theory that a seizure-induced respiratory mechanism may be involved in pediatric cases of sudden, unexpected death in epilepsy.36
There is no definite documentation of an un-expected death that was not preceded by a sei-zure. Although witnesses have reported deaths that were not observed to be preceded by seizure, such an event has not been captured in the millions of hours of video and ambulatory EEG recordings obtained each year from patients with epilepsy.
In separate case reports of 13 patients in epilepsy-monitoring units, 8 died suddenly, and 5 were resuscitated after a life-threatening episode. These cases may not accurately reflect the course of sudden, unexpected death in the community, since most of the patients in the study had treat-ment-resistant epilepsy and underwent rapid with-drawal of medication. However, recorded cases do provide valuable information on the mechanisms of these deaths. Each of the 13 patients had seizures just before death: 12 had tonic–clonic seizures and 1 had complex partial seizures11,21,27-33,37; 10 of the patients had two or more seizures the day be-fore they died, and most of the patients died dur-ing sleep. Patients who were successfully resuscitat-ed were younger than those who died (mean age, 29 years vs. 43 years); older patients may be more vulnerable to seizure-induced cardiopulmonary or brain dysfunction. Electrocardiography (ECG) was usually performed during video EEG, with the pa-tient’s respiratory effort assessed through visual
Data are based on the pooled results of 23 studies, cited in Sillanpää and Shin-nar9 and Tomson et al.11 Numbers in parentheses indicate the number of stud-ies for each population. I bars denote 95% confidence intervals.
current concepts
n engl j med 365;19 nejm.org november 10, 2011 1803
inspection. Respiratory problems predominated in 8 patients, who underwent postictal hypoventila-tion, apnea, cyanosis, inspiratory stridor, laryngo-spasm, pulmonary edema, or suffocation.11,21,32,33,38 Shutdown of brain function, with severe, diffuse EEG attenuation, was considered the primary cause of death in 2 cases; 1 patient showed “no move-ment” while lying prone postictally and had a pulse of 47 beats per minute; an autopsy revealed pulmonary edema.11,29 Cardiac abnormalities, such
as peaked T waves, ST-segment elevation, and asys-tole, usually followed collapse or, less often, co-incided with respiratory problems.11,28-31 Ven-tricular arrhythmia came close to causing sudden death in 1 patient, who had a convulsion that lasted 4.5 minutes, at which point ventricular tachycardia progressed to fibrillation.30 In 2 patients, multiple mechanisms may have led to sudden death.21,37
The view that terminal seizure plays a role in cases of sudden, unexpected death in epilepsy is
Frequent seizures, recent seizure, long postictal EEG suppression
Yes Yes Yes
Terminal seizure Yes Yes Yes
Prone position after seizure Yes Yes Yes
Postictal breathing problem Yes Yes Yes
Postictal cardiac arrhythmia No Yes No
Environment
Lack of nighttime supervision or monitoring Yes No No
Location (in bed or sleeping) Yes Yes Yes
Antiepileptic-drug therapy
Lack of use or subtherapeutic levels Yes Yes No
Polytherapy Yes No No
Frequent changes in regimen¶ Yes No No
Rapid withdrawal No Yes No
Other factors or mechanisms
Early adulthood Yes Yes Yes
Early onset of epilepsy! Yes No No
Long duration of epilepsy** Yes No No
Neurologic status
Intelligence quotient <70 Yes No No
Nonambulatory Yes No No
Major neurologic insult Yes No No
Carbamazepine or lamotrigine Yes No No
* The term “No” indicates that there is a lack of evidence for the risk factor or mechanism. EEG denotes electroencephalog-raphy, and GTCS generalized tonic–clonic seizure.
† The epidemiologic data were reported by Sillanpää and Shinnar,9 Tomson et al.,11,12 Walczak et al.,13 Camfield and Camfield,14 Hitiris et al.,17 Kloster and Engelskjøn,18 Nilsson et al.,19 Langan et al.,20 Lhatoo et al.,21 Nei et al.,22 Ryvlin et al.,23 Aurlien et al.,24 Opeskin et al.,25 and Nilsson et al.26
‡ The video EEGs were summarized or reported by Tomson et al.,11 Langan et al.,27 Bateman et al.,28 Bird et al.,29 Espinosa et al.,30 So et al.,31 Tao et al.,32 and Thomas et al.33
§ The witnessed cases of sudden death were reported by Annegers,3 Donner et al.,5 and Langan et al.27
¶ The addition of treatment with an antiepileptic drug in the preceding 3 months is associated with a lower risk of sud-den death.23
! Early onset refers to onset before 15 years of age.** Long duration refers to a duration of more than 15 to 30 years.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 365;19 nejm.org november 10, 20111804
supported by the fact that levels of heat-shock protein 70 in hippocampal neurons are elevated in such cases.39 Seizure can cause pulmonary edema,40,41 which is the most common autopsy finding in such cases.7,17,18 It remains uncertain whether sudden death occurs without a terminal seizure. Excluding cases in which there is a termi-nal seizure, the rate of sudden, unexpected death among patients with epilepsy may be similar to that in the general population.
Determining the precise mechanism of death is difficult, even for cases that were recorded on video EEG. In most cases, there is no monitoring of blood pressure or respiratory function, and the findings on ECG are often restricted to a single channel riddled with artifact. A respiratory dis-order such as hypoventilation could go unnoticed while cardiac arrhythmia, which is actually sec-
ondary, is considered causative (or vice versa). In addition to cardiorespiratory causes and cerebral shutdown, genetic, drug, metabolic, and environ-mental factors, as well as multifactorial processes, may contribute to sudden, unexpected death in patients with epilepsy (Fig. 2).
Respiratory FactorsThe concept of impaired respiration as a cause of death is supported by data from studies in ani-mals and evidence from most witnessed and re-corded instances of sudden, unexpected death in epilepsy (Table 2).27,28-33 Seizure-induced respira-tory changes can be lethal and may involve pul-monary dysfunction and suppression of brain-stem respiratory and arousal centers.40 In sheep, prolonged seizures cause elevated pressure in the left atrial and pulmonary arteries, pulmonary ede-
Increased seizures
Acquired changes in brain function
Acquired autonomic dysfunction
Genetics
Cardiac!arrhythmia
Death
Simple!or!complexpartial!seizure
Chronic!epilepsy
Generalizedtonic–clonic
seizure
Hypoventilation!or!hypoxia
Prolonged postictal state
AEDs or abrupt changes in AEDs
Asphyxia
Pulmonary edema
Obstructive apnea
Central apnea
Cerebral shutdown
Figure!2.!Mechanisms!of!Seizure-Induced!Death.
Sudden, unexpected death often follows a seizure in patients with chronic epilepsy (orange). Potential risk factors associ-ated with chronic epilepsy (blue) and direct effects from seizures (green, pink, and purple) probably interact in various ways to cause death, which is probably a result of cerebral shutdown, hypoventilation and hypoxia, cardiac arrhythmia, or some combination thereof. AED denotes antiepileptic drug.
current concepts
n engl j med 365;19 nejm.org november 10, 2011 1805
ma, tachycardia, and death from hypoventilation.42 Serotonergic neurons that modulate breathing and arousal may be involved in sudden, unexpected death in epilepsy, as is the case with sudden in-fant death syndrome.40,43 Some serotonergic neu-rons stimulate respiratory nuclei in the brain stem, whereas others, activated by hypercapnia, contrib-ute to the ascending arousal system.44 Postictal depression of serotonergic activity can impair res-piration and reflexive repositioning if the mouth and nose are obstructed by bedding. In some mouse strains, sound-induced seizure arrests respiration — an effect that is reduced by selective serotonin-reuptake inhibitors (SSRIs) and 5-HT2C–receptor agonists.45 Among patients with epilepsy, use of an SSRI is associated with reduced oxygen desatu-ration during partial seizure but not during tonic–clonic seizure.46
Cerebral ShutdownSeizure and the postictal state can affect brain-stem respiratory centers. Central apneas or hypop-neas complicate most seizures.38 In one study, pa-tients with epilepsy who died suddenly had longer periods of postictal generalized EEG suppression than did patients with epilepsy who did not die suddenly.21 Respiration depends on brain-stem activity; prolonged suppression of activity stops respiration. Postictal shutdown of cerebral and brain-stem function may be related to the mech-anisms that stop seizures. Postictal hypercapnia and hypoxemia can occur despite increased respi-
ratory effort, possibly from ventilation–perfusion inequality, which is caused by right-to-left pulmo-nary shunting or neurogenic pulmonary edema.47 Sudden, unexpected death has been reported in a patient with epilepsy who had postictal pulmo-nary edema.36 Postictal hypercapnia can cause severe acidosis that is arrhythmogenic.48 The ef-fects of prolonged postictal EEG suppression, ap-nea, pulmonary shunting and edema, suffoca-tion in the prone position, impaired arousal to hypercapnia, laryngeal spasm, and respiratory aci-dosis probably combine and cascade with cardiac factors to cause many cases of sudden, unexpect-ed death in patients with epilepsy (Table 2 and Fig. 2).
Cardiac FactorsCardiac events are considered to be likely culprits in some instances of sudden, unexpected death in patients with epilepsy.4,11,12,30,48,49 Seizure-induced arrhythmias occur in animals and humans,49,50 but in 13 case studies of near and actual sudden death in patients with epilepsy, only 1 incident was clearly due to a cardiac event.30 Hypoxemia could lower the threshold for cardiac arrhythmias dur-ing seizure, especially in patients with channelo-pathies affecting both brain and cardiac tissue (e.g., long-QT syndrome type 2).51 Mice lacking the Kv1.1 potassium channel have severe seizures and die prematurely, possibly because of cardiac ar-rhythmias.48 Interictal and ictal cardiovascular changes occur in patients with epilepsy,49,50 in-
Respiratory problems (respiratory arrest, labored breathing, suffocation in prone position, laryngeal spasm) are recorded in most instances of near and actual SUDEP on video EEG.
Tomson et al.,11 Langan et al.,27 Bateman et al.,28
Thomas et al.33
Respiratory problems are reported in most witnessed incidents of SUDEP. Langan et al.27
Most incidents occur during sleep and patient is usually found prone, supporting suffocation as contributing cause of death.
Kloster and Engelskjøn,18 Langan et al.27
Lack of monitoring increases risk (repositioning and stimulation can improve respiration but cannot relieve arrhythmia).
Nashef et al.,7 Langan et al.20
Hypercarbia and hypoxemia are common after seizures. Hewertson et al.,36 Bateman et al.28
Prolonged generalized EEG suppression is a risk factor (brain stem initiates breathing and arousal; the heart can function autonomously).
Lhatoo et al.21
Infants with seizure-induced life-threatening events have hypoxemia and apnea, not arrhythmias.
Hewertson et al.36
Pulmonary edema is the most common autopsy finding. Nashef et al.,7 Hitiris et al.,17 Kloster and Engelskjøn18
Video-EEG recordings infrequently show cardiac problem as primary cause of SUDEP.
Langan et al.,27 Bateman et al.,28 Bird et al.,29 Espinosa et al.,30 So et al.,31 Tao et al.,32 Thomas et al.33
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 365;19 nejm.org november 10, 20111806
cluding prolongation of the QT interval corrected for heart rate (QTc) during the ictal and interictal periods and shortening of the QTc interval post-ictally.52-54 Ictal asystole occurs during video EEG in 0.1 to 0.4% of patients, but recurrence is rare after pacemaker implantation.49,55 Patients with epilepsy who die suddenly have rates of cardiac repolarization abnormalities and arrhythmias that are similar to those among other patients with epilepsy,22,53 but sudden death is associated with more severe tachycardia during nocturnal sei-zures.22 Intense seizures may cause greater acti-vation of the sympathetic nervous system, possibly contributing to cardiopulmonary dysfunction56 and to prolonged suppression of brain activity,38 which can in turn cause apnea and impair arousal while the heart functions independently. Intense seizures may also trigger greater compensatory responses (e.g., elevated adenosine levels), and these responses may contribute to sudden death.57
Other Risk FactorsThe severity of epilepsy partly explains some of the risk factors for sudden death, such as tonic–clonic seizures, frequent seizures, early onset and long duration of epilepsy, and polytherapy, but some factors probably contribute to the risk of sudden death directly. Tonic–clonic seizure is often documented immediately before sudden death, suggesting that seizures are responsible for many cases. The association of early onset and long duration of epilepsy with an increased risk of sudden death suggests that progressive neural changes contribute to the risk. Although polytherapy is a mark of treatment-resistant epi-lepsy, treatment with three or more antiepileptic drugs has been found to increase the risk of sud-den death by a factor of more than 8 after adjust-ment for seizure frequency.19 However, in ran-domized, controlled trials involving patients with treatment-resistant epilepsy, the rate of sud-den death was increased by a factor of more than 7 among patients who received placebo as com-pared with those who received an additional anti-epileptic drug.23 The effects of the number of drugs taken, the frequency of dose changes, and the recent removal or addition of drugs on the risk of sudden death require further investigation.
Sudden, unexpected death in epilepsy usually occurs in chronic, severe cases of epilepsy, often in patients with a history of neurologic insult. Thus, such deaths may result from the cumulative
effects of seizures compounded by a tonic–clonic seizure (i.e., the additive effect of acute injury after chronic injury). Frequent tonic–clonic sei-zures can progressively damage brain structure (e.g., atrophy of the hippocampus) and function (e.g., impairment of short-term memory).1 Since greater interictal autonomic changes occur in pa-tients with chronic epilepsy than in those with recent-onset epilepsy,35 there may also be progres-sive changes in the brain-stem areas that regulate cardiorespiratory function and arousal. However, sudden death can occur early in the course of epilepsy and in patients who have seizures only rarely. It is not known why sudden death occurs in some patients after only a few seizures, where-as others are spared despite a lifetime of tonic–clonic seizures. Genetic susceptibility (e.g., cardiac channelopathy), alcohol use, medication with-drawal, and fever may increase the risk of sud-den death after a seizure, but these potential risk factors have not been adequately studied. Regard-ing genetic susceptibility, mutations in the ion-channel genes expressed in brain and cardiac tissue may underlie susceptibility to epilepsy, brain-stem autonomic dysfunction, and cardiac arrhyth-mias.51 Abnormalities in the serotonergic system have been found in patients with epilepsy or de-pression and in cases of sudden death.40 Patients with epilepsy who have been treated for depres-sion within the past 12 months have a 40% in-crease in the risk of death, as compared with those who have not been treated for depression.58 Car-bamazepine, which has been associated with sud-den death among patients with epilepsy in some studies,11,22 can suppress autonomic functions.59 Lamotrigine is also associated with an increased risk of sudden death among patients with epilepsy in some studies.24,60
Sudden, Une x pec ted, Seizur e-Induced De ath
In most cases, when sudden death occurs after a seizure, it is more precisely defined as sudden, unexpected, seizure-induced death. Use of this term can be important in helping to make patients and their families aware of the potential danger of sei-zure and to increase public awareness of the disorder. The phrase “sudden, unexpected death in epilepsy” communicates the message that some people with epilepsy die unexpectedly for un-known reasons, but sudden death also occurs
current concepts
n engl j med 365;19 nejm.org november 10, 2011 1807
in people who are or appear to be healthy and complicates our understanding of many medical disorders. In contrast, the use of the phrase “sud-den, unexpected, seizure-induced death” under-scores the fact that seizure is involved in death and thereby lays the path for education about prevention. Sudden, unexpected, seizure-induced death should be considered to be a type of sei-zure-induced death, along with those due to sta-tus epilepticus, drowning, motor-vehicle accidents, trauma, burns, and suicide during a postictal psychosis.
Pr e v en tion
We do not know how to prevent sudden, unex-pected death in epilepsy. No prospective or con-trolled studies have evaluated interventions to reduce its incidence. Since a tonic–clonic seizure precedes most sudden deaths in patients with epilepsy, seizure control — and the appropriate use of medication as well as counseling on life-style — is the focus of prevention (Table 3). The lack of therapeutic levels of antiepileptic drugs, nonadherence to treatment regimens, and fre-quent changes in regimens are all risk factors for sudden death.9,11,12,19,20,25 For patients who have never been treated with antiepileptic drugs, the risk of sudden death may be more than 20 times as high as that for treated patients.20 A discus-sion of sudden, unexpected death in epilepsy may be worthwhile for patients with tonic–clonic sei-zures who are beginning an antiepileptic-drug regimen and for patients at high risk for recur-rent tonic–clonic seizures who are discontinuing such a regimen.
Thirty percent of patients with epilepsy have treatment-resistant epilepsy, and these patients — who are at high risk for sudden death — present the greatest challenge. Frequent changes in multidrug regimens are commonly under-taken to reduce the frequency of seizure or the side effects of medication, but the potential ef-fects of regimen changes on the risk of sudden death are rarely considered and remain unknown. Patients who are free of seizures after surgery for epilepsy have reduced rates of sudden death,8,10,62 with mortality approaching that in the general population. In contrast, patients with postoperative seizures have very high rates of sudden death.62
Patients should be informed about the funda-mentals of seizure prevention: observance of a
healthful lifestyle (e.g., avoiding sleep deprivation and excessive consumption of alcohol), adherence to their antiepileptic-drug regimen (e.g., avoiding and identifying missed doses with the use of weekly pill boxes and watch alarms), knowledge of how to make up for missed doses and of fac-tors influencing drug levels, and avoidance of drugs that lower the threshold for seizure. Patients should also be asked whether they have symptoms of nocturnal tonic–clonic seizure. For patients who do have nocturnal tonic–clonic seizure, bedtime medication doses can be increased and seizure-detection devices (discussed below) considered.
Educating persons who live with patients with epilepsy may also help to prevent sudden death. Knowledge of how to perform the appropriate first-aid responses to seizure (repositioning the patient and protecting the airway after a tonic–clonic seizure) may prevent death. A case–control study of adults showed that as compared with unmonitored controls, patients who were moni-tored while they slept had a reduced risk of sud-den death by a factor of 2.5 if another person older than 10 years of age was in the room and by a factor of 10 if there were frequent nighttime checks or if a sound-monitoring device was used.20 In a study of 14 residents at a special-needs school who had severe epilepsy and died suddenly, all 14 died at home, and most of them were not be-ing monitored.7 None died at school, where they were monitored during sleep by four attendants and an on-call nurse and a sound-monitoring device was used. The manufacturers of several commercial devices state that their products can detect tonic–clonic seizure, but very limited data are available on the sensitivity and specificity of these devices for the detection of tonic–clonic seizure,63 and there is no evidence that their use prevents sudden death. Patients with nocturnal tonic–clonic seizure may want to consider the use of motion-detection devices (e.g., the Emfit monitor [Emfit]) that have a configurable sens-ing unit that is placed under the mattress and a receiver located in another room with audiovisual alarms. Pulse oximeters and heart-rate monitors may detect seizure-induced hypoxemia and tachy-cardia. Nonetheless, sudden death occurs in hos-pitals and other medical environments, despite prompt attempts at resuscitation.11
The effectiveness of strategies intended to pre-vent sudden death by improving respiration or oxygenation remain unproven. Since many pa-
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 365;19 nejm.org november 10, 20111808
Tabl
e!3.!P
reve
ntio
n!of!S
udde
n,!U
nexp
ecte
d!D
eath!in!E
pile
psy.
Risk!F
acto
rPr
even
tive!
Stra
tegy
Com
men
t
Gen
eral
ized
toni
c–cl
onic
sei
zure
and
un
cont
rolle
d se
izur
eIm
prov
e ad
here
nce
to m
edic
atio
n re
gim
en; r
ecom
men
d lif
esty
le
mod
ifica
tions
— re
gula
r, re
stor
ativ
e sl
eep
and
limita
tion
of a
lco-
hol c
onsu
mpt
ion;
opt
imiz
e an
tiepi
lept
ic-d
rug
regi
men
; con
side
r ep
ileps
y su
rger
y, d
ieta
ry th
erap
y, o
r neu
rost
imul
atio
n
Seiz
ure
clus
ters
, pro
long
ed s
eizu
reC
onsi
der u
se o
f res
cue
med
icat
ions
Resc
ue m
edic
atio
ns in
clud
e cl
onaz
epam
(ora
l, di
ssol
ving
waf
er),
di
azep
am (
bucc
al s
olut
ion
or re
ctal
gel
), lo
raze
pam
(or
al ta
b-le
t or l
iqui
d), a
nd m
idaz
olam
(nas
al s
pray
, buc
cal s
olut
ion)
*C
onsi
der u
se o
f ben
zodi
azep
ine
resc
ue m
edic
atio
ns; u
rge
patie
nt to
se
ek p
rom
pt m
edic
al a
tten
tion
whe
n ap
prop
riate
Fluc
tuat
ing
leve
ls o
f ant
iepi
lept
ic d
rugs
Educ
ate
patie
nt a
bout
dru
g in
tera
ctio
ns (e
.g.,
oral
con
trac
eptiv
es
low
er la
mot
rigin
e le
vels
)61 a
nd th
e ef
fect
s of
vom
iting
and
dia
r-rh
ea o
n dr
ug a
bsor
ptio
n
A re
dosi
ng s
trat
egy
is re
com
men
ded
for m
isse
d m
edic
atio
ns
or m
edic
atio
ns lo
st to
vom
iting
or s
ever
e di
arrh
ea
Noc
turn
al s
eizu
re
Uni
dent
ified
Indi
catio
ns th
at a
pat
ient
may
be
havi
ng n
octu
rnal
sei
zure
s w
ithou
t aw
aren
ess
of th
em a
re u
rinar
y in
cont
inen
ce, t
ongu
e or
che
ek
bite
s, u
nusu
al h
eada
ches
, mus
cle
sore
ness
, let
harg
y, o
r con
fu-
sion
on
awak
enin
g; a
sk th
e pa
tient
whe
ther
any
of t
hese
con
di-
tions
app
ly
Iden
tifie
dRe
dist
ribut
e or
incr
ease
eve
ning
or b
edtim
e m
edic
atio
n
Slee
ping
alo
ne, e
spec
ially
with
his
tory
of
noc
turn
al s
eizu
reD
evel
op s
trat
egie
s to
ens
ure
adhe
renc
e to
med
icat
ion
regi
men
, es
peci
ally
eve
ning
and
bed
time
dose
sA
soun
d or
sei
zure
mon
itor m
ay b
e co
nsid
ered
, but
the
sens
itivi
ty
and
spec
ifici
ty o
f the
se m
onito
rs fo
r sei
zure
det
ectio
n is
un-
cert
ain,
as
is th
eir r
ole
in p
reve
ntin
g su
dden
dea
th
Brea
kthr
ough
sei
zure
Educ
ate
the
patie
nt a
bout
the
impo
rtan
ce o
f adh
erin
g to
med
icat
ion
regi
men
and
obs
ervi
ng h
ealth
y lif
esty
leD
rugs
that
low
er th
e se
izur
e th
resh
old
(e.g
., ph
enyl
ephr
ine,
pse
u-do
ephe
drin
e, b
upro
pion
) sho
uld
be a
void
ed
Low
leve
ls o
f ant
iepi
lept
ic d
rugs
Con
side
r dos
e in
crea
se; a
dvis
e pa
tient
to a
dher
e to
med
icat
ion
regi
-m
en a
nd e
xpla
in w
hat s
houl
d be
don
e if
med
icat
ions
are
mis
sed
or if
pat
ient
has
gas
troi
ntes
tinal
illn
ess
that
cau
ses
vom
iting
or
diar
rhea
†
A re
dosi
ng s
trat
egy
is re
com
men
ded
for m
isse
d m
edic
atio
ns
or m
edic
atio
ns lo
st to
vom
iting
or s
ever
e di
arrh
ea
Freq
uent
cha
nges
in a
ntie
pile
ptic
dru
gsO
ptim
ize
and
sim
plify
the
regi
men
and
avo
id fr
eque
nt c
hang
es
Men
tal r
etar
datio
n, n
onam
bula
tory
sta
tus
Reco
mm
end
that
car
egiv
ers
mon
itor t
he p
atie
nt (e
.g.,
with
a s
ound
m
onito
r)C
onsi
der u
se o
f a s
eizu
re m
onito
r‡
Pron
e po
sitio
n, s
uffo
catio
n af
ter s
eizu
reRe
posi
tion
the
patie
nt to
lie
on s
ide
or s
timul
ate
patie
nt; f
or a
pnea
or
sev
ere
hypo
vent
ilatio
n, in
itiat
e ca
rdio
pulm
onar
y re
susc
itatio
nC
onsi
der u
se o
f a s
eizu
re o
r res
pira
tory
mon
itor o
r lat
tice
pillo
ws‡
Car
diac
arr
hyth
mia
, asy
stol
eRe
com
men
d a
card
iac
mon
itor o
r, fo
r pat
ient
s w
ith li
fe-th
reat
enin
g ar
rhyt
hmia
, a p
acem
aker
* Re
scue
med
icat
ions
hav
e a
rapi
d on
set a
nd a
re u
sed
to tr
eat p
rolo
nged
sei
zure
or
seiz
ure
clus
ters
. The
nas
al a
nd b
ucca
l for
ms
of m
idaz
olam
hav
e no
t bee
n ap
prov
ed in
the
Uni
ted
Stat
es.
† In
pre
gnan
cy, m
any
drug
leve
ls d
eclin
e; le
vels
sho
uld
be c
lose
ly m
onito
red
and
dose
incr
ease
d to
mai
ntai
n a
ther
apeu
tic le
vel.
‡ Th
e ef
ficac
y of
sei
zure
and
resp
irato
ry m
onito
rs h
as n
ot b
een
prov
ed fo
r the
det
ectio
n of
sei
zure
or t
he p
reve
ntio
n of
sud
den,
une
xpec
ted
deat
h in
epi
leps
y. T
he e
ffica
cy o
f lat
tice
pillo
ws
has
not b
een
prov
ed fo
r the
pre
vent
ion
of s
uffo
catio
n.
current concepts
n engl j med 365;19 nejm.org november 10, 2011 1809
tients are found prone, some practitioners advo-cate the use of antisuffocation pillows (e.g., see www.sleep-safe.co.uk) for the prevention of sud-den death in epilepsy, but data on their clinical value are lacking. The potential role of oxygen administration during and after a tonic–clonic seizure — a common practice in hospitals but not in patients’ homes — deserves study.
Routine ECG screening of all patients with epilepsy is of uncertain value. Patients with tonic–clonic seizure or episodic loss of consciousness who have normal or nonspecific findings on mag-netic resonance imaging of the brain and EEG should undergo ECG to rule out the long-QT syn-drome, a lethal disorder that mimics epilepsy64; these patients may also benefit from Holter ECG monitoring to rule out arrhythmia. Misdiagnosis of the long-QT syndrome as epilepsy precludes the use of effective therapy, and the inappropriate administration of antiepileptic drugs can induce arrhythmias.51
One additional preventive step is to discuss sud-den, unexpected death in epilepsy with patients — a step few physicians initiate because it may cause stress about an uncommon problem for which there is no proven means of prevention. However, most patients with epilepsy and their families want information about sudden death.65,66 Although national guidelines in the United King-dom recommend that all patients with epilepsy and their families be provided with information about sudden, unexpected death in epilepsy,66 most neurologists cited in the study discuss it only with high-risk patients or when specifi-cally asked.65,66 Guidelines and tools are needed to assist physicians and patients and their fami-lies in becoming educated about sudden, unex-pected death in epilepsy, and outcome measures
are needed to assess the effectiveness of this edu-cation. Patients with risk factors that can be modi-fied — such as nonadherence to antiepileptic-drug regimen, tonic–clonic seizure, nocturnal seizure, and treatment-resistant epilepsy — may benefit most from counseling. When patients ask whether seizures can injure their brain or kill them, a simple “no” is insufficient. Epilepsy is associated with significant risks of morbidity and death.
Fu t ur e Dir ec tions
Reductions in sudden deaths among patients with epilepsy may be achieved by increasing awareness on the part of the general public and the medical community, improving the prevention and treat-ment of epilepsy, further developing and encour-aging the use of devices that detect seizure and can alert caretakers, improving our understanding of the mechanisms of sudden, unexpected death in epilepsy, and conducting interventional trials to prevent the progression of life-threatening sei-zure to sudden death. If patients are aware that seizure can be deadly, they may be more moti-vated to adhere to antiepileptic-drug regimens and to avoid lifestyle choices that increase the likeli-hood of seizure. Patients with seizures that re-main uncontrolled after the administration of two different drug regimens should be referred to an epilepsy center for evaluation. Preventing seizures can be lifesaving.
Dr. Devinsky reports providing expert testimony in legal medical proceedings regarding possible sudden, unexpected death in epilepsy and receiving lecture fees from UCB. No other potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the author are available with the full text of this article at NEJM.org.
I thank Drs. Daniel Friedman and Ion-Florin Talos and Brigid Staley, M.P.H., for providing invaluable input on earlier ver-sions of the manuscript.
References
1.! Hermann B, Seidenberg M, Bell B. The neurodevelopmental impact of child-hood onset temporal lobe epilepsy on brain structure and function and the risk of pro-gressive cognitive effects. Prog Brain Res 2002;135:429-38.2.! Nashef L. Sudden unexpected death in epilepsy: terminology and definitions. Epilepsia 1997;38:Suppl:S6-S8.3.! Annegers JF. United States perspective on definitions and classifications. Epilepsia 1997;38:Suppl:S9-S12.4.! Dasheiff RM. Sudden unexpected death in epilepsy: a series from an epilepsy sur-gery program and speculation on the rela-
tionship to sudden cardiac death. J Clin Neurophysiol 1991;8:216-22.5.! Donner EJ, Smith CR, Snead OC III. Sudden unexplained death in children with epilepsy. Neurology 2001;57:430-4.6.! Ficker D, So E, Shen WK, et al. Popula-tion-based study of the incidence of sudden unexplained death in epilepsy. Neurology 1998;51:1270-4.7.! Nashef L, Fish DR, Garner S, Sander JW, Shorvon SD. Sudden death in epilepsy: a study of incidence in a young cohort with epilepsy and learning difficulty. Epi-lepsia 1995;36:1187-94.8.! Nilsson L, Ahlbom A, Farahmand BY,
Tomson T. Mortality in a population-based cohort of epilepsy surgery patients. Epi-lepsia 2003;44:575-81.9.! Sillanpää M, Shinnar S. Long-term mortality in childhood-onset epilepsy. N Engl J Med 2010;363:2522-9.10.! Sperling MR, Feldman H, Kinman J, Liporace JD, O’Connor MJ. Seizure con-trol and mortality in epilepsy. Ann Neurol 1999;46:45-50.11.! Tomson T, Nashef L, Ryvlin P. Sudden unexpected death in epilepsy: current knowledge and future directions. Lancet Neurol 2008;7:1021-31.12.! Tomson T, Walczak T, Sillanpaa M,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 365;19 nejm.org november 10, 20111810
Sander JW. Sudden unexpected death in epilepsy: a review of incidence and risk factors. Epilepsia 2005;46:Suppl 11:54-61.13.! Walczak TS, Leppik IE, D’Amelio M, et al. Incidence and risk factors in sudden unexpected death in epilepsy: a prospective cohort study. Neurology 2001;56:519-25.14.! Camfield P, Camfield C. Special con-siderations for a first seizure in childhood and adolescence. Epilepsia 2008;49:Suppl 1:40-4.15.! Gillberg C, Billstedt E, Sundh V, Gill-berg IC. Mortality in autism: a prospective longitudinal community-based study. J Au-tism Dev Disord 2010;40:352-7.16.! Le Gal F, Korff CM, Monso-Hinard C, et al. A case of SUDEP in a patient with Dravet syndrome with SCN1A mutation. Epilepsia 2010;51:1915-8.17.! Hitiris N, Suratman S, Kelly K, Ste-phen LJ, Sills GJ, Brodie MJ. Sudden unex-pected death in epilepsy: a search for risk factors. Epilepsy Behav 2007;10:138-41.18.! Kloster R, Engelskjøn T. Sudden un-expected death in epilepsy (SUDEP): a clini-cal perspective and a search for risk factors. J Neurol Neurosurg Psychiatry 1999;67: 439-44.19.! Nilsson L, Farahmand BY, Persson PG, Thiblin I, Tomson T. Risk factors for sud-den unexpected death in epilepsy: a case-control study. Lancet 1999;353:888-93.20.! Langan Y, Nashef L, Sander JW. Case-control study of SUDEP. Neurology 2005; 64:1131-3.21.! Lhatoo SD, Faulkner HJ, Dembny K, Trippick K, Johnson C, Bird JM. An electro-clinical case-control study of sudden un-expected death in epilepsy. Ann Neurol 2010;68:787-96.22.!Nei M, Ho RT, Abou-Khalil BW, et al. EEG and ECG in sudden unexplained death in epilepsy. Epilepsia 2004;45:338-45.23.! Ryvlin P, Cucherat M, Rheims S. Risk of sudden unexpected death in epilepsy in patients given adjunctive antiepileptic treatment for refractory seizures: a meta-analysis of placebo-controlled randomised trials. Lancet Neurol 2011 September 19 (Epub ahead of print).24.! Aurlien D, Larsen J, Taubøll E, Gjer-stad L. Increased incidence of sudden un-expected death in epilepsy (SUDEP) with lamotrigine in Rogaland County, Norway. Epilepsia 2010;51:Suppl 3:136. abstract.25.! Opeskin K, Burke MP, Cordner SM, Berkovic SF. Comparison of antiepileptic drug levels in sudden unexpected deaths in epilepsy with deaths from other causes. Epilepsia 1999;40:1795-8.26.! Nilsson L, Bergman U, Diwan V, Farah-mand BY, Persson PG, Tomson T. Antiepi-leptic drug therapy and its management in sudden unexpected death in epilepsy: a case-control study. Epilepsia 2001;42:667-73.27.! Langan Y, Nashef L, Sander JW. Sud-den unexpected death in epilepsy: a series of witnessed deaths. J Neurol Neurosurg Psychiatry 2000;68:211-3.
28.! Bateman LM, Spitz M, Seyal M. Ictal hypoventilation contributes to cardiac ar-rhythmia and SUDEP: report on two deaths in video-EEG-monitored patients. Epilepsia 2010;51:916-20.29.! Bird J, Dembny K, Sandeman D, But-ler S. Sudden unexplained death in epi-lepsy: an intracranially monitored case. Epilepsia 1997;38:Suppl 11:S52-S56.30.! Espinosa PS, Lee JW, Tedrow UB, Bromfield EB, Dworetzky BA. Sudden un-expected near death in epilepsy: malig-nant arrhythmia from a partial seizure. Neurology 2009;72:1702-3.31.! So EL, Sam MC, Lagerlund TL. Postictal central apnea as a cause of SUDEP: evi-dence from near-SUDEP incident. Epilepsia 2000;41:1494-7.32.! Tao JX, Qian S, Baldwin M, et al. SUDEP, suspected positional airway ob-struction, and hypoventilation in postictal coma. Epilepsia 2010;51:2344-7.33.! Thomas P, Landre E, Suisse G, Bre-looin J, Dolisi C, Chatel M. Syncope anoxo-ischemique par dyspne: le obstructive au cours d’une crise partielle complexe tem-porale droite. Epilepsies 1996;8:339-46.34.! Opeskin K, Berkovic SF. Risk factors for sudden unexpected death in epilepsy: a controlled prospective study based on coroners cases. Seizure 2003;12:456-64.35.! Sevcencu C, Struijk JJ. Autonomic al-terations and cardiac changes in epilepsy. Epilepsia 2010;51:725-37.36.! Hewertson J, Poets CF, Samuels MP, Boyd SG, Neville BG, Southall DP. Epilep-tic seizure-induced hypoxemia in infants with apparent life-threatening events. Pe-diatrics 1994;94:148-56.37.! Dasheiff RM, Dickinson LJ. Sudden unexpected death of epileptic patient due to cardiac arrhythmia after seizure. Arch Neurol 1986;43:194-6.38.! Bateman LM, Li CS, Seyal M. Ictal hy-poxemia in localization-related epilepsy: analysis of incidence, severity and risk factors. Brain 2008;131:3239-45.39.! Thom M, Seetah S, Sisodiya S, Koepp M, Scaravilli F. Sudden and unexpected death in epilepsy (SUDEP): evidence of acute neuronal injury using HSP-70 and c-Jun immuno histochemistry. Neuropathol Appl Neurobiol 2003;29:132-43.40.! Richerson GB, Buchanan GF. The sero-tonin axis: shared mechanisms in seizures, depression, and SUDEP. Epilepsia 2011; 52:Suppl 1:28-38.41.! Swallow RA, Hillier CE, Smith PE. Sudden unexplained death in epilepsy (SUDEP) following previous seizure-related pulmonary oedema: case report and review of possible preventative treatment. Seizure 2002;11:446-8.42.! Johnston SC, Siedenberg R, Min JK, Jerome EH, Laxer KD. Central apnea and acute cardiac ischemia in a sheep model of epileptic sudden death. Ann Neurol 1997;42:588-94.43.! Duncan JR, Paterson DS, Hoffman JM,
et al. Brainstem serotonergic deficiency in sudden infant death syndrome. JAMA 2010; 303:430-7.44.! Buchanan GF, Hodges MR, Richerson GB. Contribution of chemosensitive sero-tonergic neurons to interactions between the sleep-wake cycle and respiratory con-trol. In: Monti JM, Pandi-Perumal SR, Ja-cobs BL, Nutt DJ, eds. Serotonin and sleep: molecular, functional and clinical aspects. Basel, Switzerland: Birkhäuser Verlag, 2008: 529-54.45.! Uteshev VV, Tupal S, Mhaskar Y, Fain-gold CL. Abnormal serotonin receptor ex-pression in DBA/2 mice associated with susceptibility to sudden death due to respi-ratory arrest. Epilepsy Res 2010;88:183-8.46.! Bateman LM, Li CS, Lin TC, Seyal M. Serotonin reuptake inhibitors are associ-ated with reduced severity of ictal hypoxe-mia in medically refractory partial epilep-sy. Epilepsia 2010;51:2211-4.47.! Seyal M, Bateman LM, Albertson TE, Lin TC, Li CS. Respiratory changes with seizures in localization-related epilepsy: analysis of periictal hypercapnia and air-flow patterns. Epilepsia 2010;51:1359-64.48.! Glasscock E, Yoo JW, Chen TT, Klassen TL, Noebels JL. Kv1.1 potassium channel deficiency reveals brain-driven cardiac dys-function as a candidate mechanism for sud-den unexplained death in epilepsy. J Neuro-sci 2010;30:5167-75.49.! Schuele SU. Effects of seizures on car-diac function. J Clin Neurophysiol 2009; 26:302-8.50.! Devinsky O. Effects of seizures on auto-nomic and cardiovascular function. Epilepsy Curr 2004;4:43-6.51.! Johnson JN, Hofman N, Haglund CM, Cascino GD, Wilde AA, Ackerman MJ. Identification of a possible pathogenic link between congenital long QT syn-drome and epilepsy. Neurology 2009;72: 224-31.52.! Brotherstone R, Blackhall B, McLel-lan A. Lengthening of corrected QT dur-ing epileptic seizures. Epilepsia 2010;51: 221-32.53.! Surges R, Adjei P, Kallis C, et al. Pathologic cardiac repolarization in phar-macoresistant epilepsy and its potential role in sudden unexpected death in epi-lepsy: a case-control study. Epilepsia 2010; 51:233-42.54.! Surges R, Scott CA, Walker MC. En-hanced QT shortening and persistent tachycardia after generalized seizures. Neurology 2010;74:421-6.55.! Rugg-Gunn FJ, Simister RJ, Squirrell M, Holdright DR, Duncan JS. Cardiac ar-rhythmias in focal epilepsy: a prospective long-term study. Lancet 2004;364:2212-9.56.! Dünser M, Hasibeder W. Sympathetic overstimulation during critical illness: ad-verse effects of adrenergic stress. J Inten-sive Care Med 2009;24:293-316.57.! Shen HY, Li T, Boison D. A novel mouse model for sudden unexpected death in epi-
current concepts
n engl j med 365;19 nejm.org november 10, 2011 1811
lepsy (SUDEP): role of impaired adenosine clearance. Epilepsia 2010;51:465-8.58.! Ridsdale L, Charlton J, Ashworth M, Richardson MP, Gulliford MC. Epilepsy mortality and risk factors for death in epilepsy: a population-based study. Br J Gen Pract 2011;61:271-8.59.! Persson H, Ericson M, Tomson T. Car-bamazepine affects autonomic cardiac control in patients with newly diagnosed epilepsy. Epilepsy Res 2003;57:69-75.60.! Hesdorffer D, Tomson T, Benn E, et al. Combined analysis of risk factors for SUDEP. Epilepsia 2011;52:1150-9.
61.! Reddy DS. Clinical pharmacokinetic interactions between antiepileptic drugs and hormonal contraceptives. Expert Rev Clin Pharmacol 2010;3:183-92.62.! Sperling M, Durhakula S, Scott L, et al. Mortality after epilepsy surgery. Epilepsia 2010;51:Suppl 2:320. abstract.63.! Carlson C, Arnedo V, Cahill M, Devin-sky O. Detecting nocturnal convulsions: efficacy of the MP5 monitor. Seizure 2009; 18:225-7.64.! Pacia SV, Devinsky O, Luciano DJ, Vazquez B. The prolonged QT syndrome presenting as epilepsy: a report of two