19
Current Diagnosis and Management of ADHF in an Acute Setting Dallas, TX December 13, 2008 8:30 AM – 9:45 AM

Current Diagnosis and Management of ADHF in an Acute Setting
Dallas, TX
December 13, 2008 8:30 AM – 9:45 AM

Session 10: Current Diagnosis and Management of ADHF in an Acute Setting Learning Objectives
• Identify at least 3 risk factors for the development of acute decompensated heart failure (ADHF) and outline the role of neurohormonal activation in ADHF.
• Implement evidence-based treatment plans for the management of patients with ADHF with attention to collaboration among the multidisciplinary team members that treat patients with ADHF.
Faculty J. Thomas Heywood, MD Director, Heart Failure Recovery and Research Center Scripps Clinic La Jolla, California Clinical Professor of Medicine Loma Linda School of Medicine Loma Linda, California Currently, Dr J. Thomas Heywood is the director of the Heart Failure Recovery and Research Center at Scripps Clinic in La Jolla, California and a clinical professor of medicine at the Loma Linda School of Medicine in Loma Linda, California. Dr Heywood received his undergraduate degree from Loyola University in Chicago, Illinois and his medical degree from the University of California at San Diego. He completed a residency in internal medicine in San Diego, California and worked as a cardiology registrar at the University of Auckland in New Zealand. He completed a cardiology fellowship at Loma Linda University Medical Center in Loma Linda, California. Following his fellowship, he spent a year as a cardiovascular research fellow at the University of Zurich in Zurich, Switzerland. In 1995 Dr Heywood was appointed the director of the Cardiomyopathy Program and Adult Heart Transplant Program at Loma Linda University Medical Center and in 2001 was promoted to professor of medicine at the Loma Linda School of Medicine in Loma Linda, California. He has been a principle investigator in many pivotal heart failure trials and is very active in clinical heart failure research. He is the author of numerous articles, abstracts and book chapters on congestive heart failure. Faculty Financial Disclosure Statement Dr Heywood receives honoraria from GlaxoSmithKline; Scios Inc.; Medtronic; Guidant; AstraZeneca Pharmaceuticals LP; and Novartis Pharmaceuticals Corporation. He receives research grants from and serves as a consultant to GlaxoSmithKline; Scios Inc.; and Medtronic. Drug and Device Lists Generic Trade captopril Capoten carvedilol Coreg dobutamine Dobutrex enalapril Vasotec furosemide Lasix milrinone Primacor
Generic Trade metolazone Zaroxolyn metoprolol Toprol-XL nesiritide Natrecor spironolactone Aldactone
Suggested Reading List Abraham WT, Adams KF, Fonarow GC, et al. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am Coll Cardiol. 2005;47:57-64.
Session 10
Adams KF, Lindenfeld J, Arnold JMO, et al. Executive summary: HFSA 2006 comprehensive heart failure practice guidelines. J Card Fail. 2006;12:10-38. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001;37:379-385. Elkayam U, Tassisa G, Binanay C, et al. Use and impact of inotropes and vasodilator therapy in hospitalized patients with severe heart failure. Am Heart J. 2007;153:98-104. Eshaghian S, Horwich TB, Fonarow GC. Relation of loop diuretic dose to mortality in advanced heart failure. Am J Cardiol. 2006;97:1759-1764. Fonarow GC, Adams KF Jr, Abraham WT, et al. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA. 2005;293:572-580. Gottlieb SS, Abraham W, Butler J, et al. The prognostic importance of different definitions of worsening renal function in congestive heart failure. J Card Fail. 2002;8:136-141. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult – summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). Circulation. 2005;112:1825-1852. Koelling TM, Johnson ML, Cody RJ, et al. Discharge education improves clinical outcomes in patients with chronic heart failure. Circulation. 2005;111:179-185. Mehra MR. Optimizing outcomes in the patients with acute decompensated heart failure. Am Heart J. 2006;151:571-579. Mentzer RM Jr, Oz MC, Sladen RN, et al: NAPA Investigators. Effects of perioperative nesiritide in patients with left ventricular dysfunction undergoing cardiac surgery: the NAPA Trial. J Am Coll Cardiol. 2007;49:716-726. Peacock WF 4th, Fonarow GC, Emergman CL, et al, for the ADHERE Study Group. Impact of early initiation of intravenous therapy for acute decompensated heart failure on outcomes in ADHERE. Cardiology. 2007;107:44-51. Peacock WF 4th, Emerman CL, Silver MA. Nesiritide added to standard care favorably reduces systolic blood pressure compared with standard care alone in patients with acute decompensated heart failure. Am J Emerg Med. 2005;23:327-331. Publication Committee for the VMAC Investigators (Vasodilation in the Management of Acute CHF). Intravenous nesiritide vs. nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial. JAMA. 2002;287:1531-1540. Sackner-Bernstein JD, Kowalski M, Fox M, et al. Short-term risk of death after treatment with nesiritide for decompensated heart failure: a pooled analysis of randomized controlled trials. JAMA. 2005;293:1900-1905. Stevenson LW. Tailored therapy to hemodynamic goals for advanced heart failure. Eur J Heart Fail. 1999;1:251-257.
Yancy CW, Krum H, Massie BM, et al: FUSION II Investigators. The Second Follow-up Serial Infusions of Nesiritide (FUSION II) trial for advanced heart failure: study rationale and design. Am Heart J. 2007;153:478-484.
Session 10

®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
1
Current Diagnosis and Management
of ADHF in the Acute SettingJ. Thomas Heywood, MD, FACC
Scripps Clinic
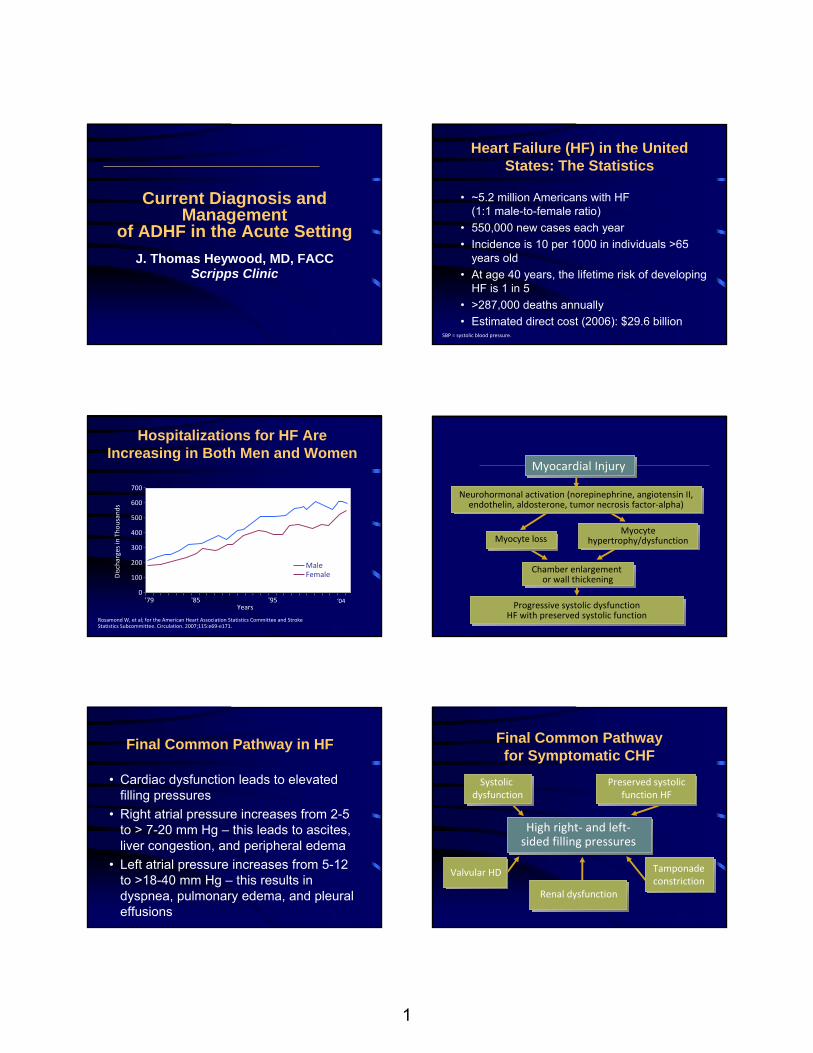
Heart Failure (HF) in the United States: The Statistics
• ~5.2 million Americans with HF (1:1 male-to-female ratio)
• 550,000 new cases each year• Incidence is 10 per 1000 in individuals >65
years old• At age 40 years, the lifetime risk of developing
HF is 1 in 5• >287,000 deaths annually• Estimated direct cost (2006): $29.6 billion
SBP = systolic blood pressure.
'79 '85 '95
Discharges in Tho
usands
MaleFemale
‘04
Rosamond W, et al; for the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69‐e171.
Hospitalizations for HF Are Increasing in Both Men and Women
0
100
200
300
400
500
700
600
Years Progressive systolic dysfunctionHF with preserved systolic function
Chamber enlargement or wall thickening
Myocytehypertrophy/dysfunction Myocyte loss
Neurohormonal activation (norepinephrine, angiotensin II, endothelin, aldosterone, tumor necrosis factor‐alpha)
Myocardial Injury
Final Common Pathway in HF
• Cardiac dysfunction leads to elevated filling pressures
• Right atrial pressure increases from 2-5 to > 7-20 mm Hg – this leads to ascites, liver congestion, and peripheral edema
• Left atrial pressure increases from 5-12 to >18-40 mm Hg – this results in dyspnea, pulmonary edema, and pleural effusions
Final Common Pathway for Symptomatic CHF
High right‐ and left‐sided filling pressures
Systolic dysfunction
Preserved systolicfunction HF
Valvular HD
Renal dysfunction
Tamponadeconstriction
2
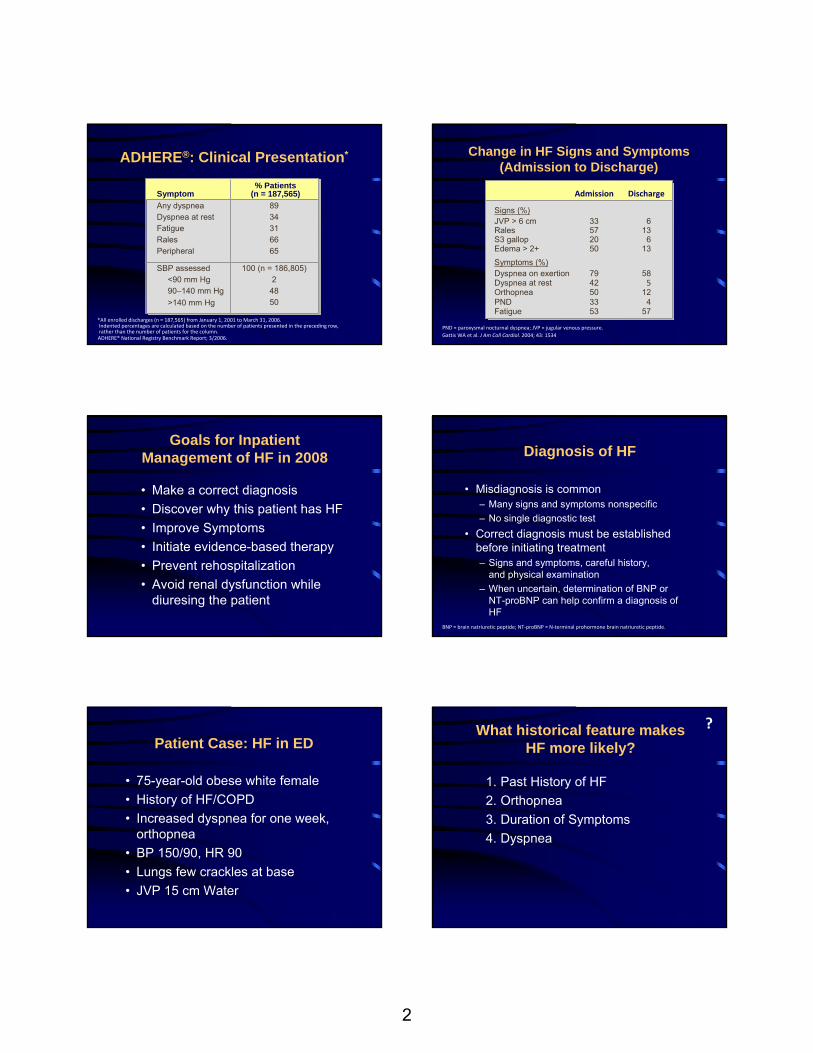
100 (n = 186,805)2
4850
8934316665
SBP assessed<90 mm Hg 90–140 mm Hg >140 mm Hg
Any dyspneaDyspnea at rest Fatigue RalesPeripheral
*All enrolled discharges (n = 187,565) from January 1, 2001 to March 31, 2006.Indented percentages are calculated based on the number of patients presented in the preceding row, rather than the number of patients for the column.
ADHERE®: Clinical Presentation*
% Patients(n = 187,565)Symptom
ADHERE® National Registry Benchmark Report; 3/2006.
Discharge
S3 gallop
Signs (%)JVP > 6 cm Rales
Edema > 2+ 6
6
13Symptoms (%)
Fatigue
Dyspnea at rest
PNDOrthopnea
Dyspnea on exertion
57
5
412
58
20
3357
50
53
42
3350
79
Admission
Change in HF Signs and Symptoms (Admission to Discharge)
13
PND = paroxysmal nocturnal dyspnea; JVP = jugular venous pressure.Gattis WA et al. J Am Coll Cardiol. 2004; 43: 1534
Goals for Inpatient Management of HF in 2008
• Make a correct diagnosis• Discover why this patient has HF• Improve Symptoms• Initiate evidence-based therapy • Prevent rehospitalization• Avoid renal dysfunction while
diuresing the patient
Diagnosis of HF
• Misdiagnosis is common– Many signs and symptoms nonspecific– No single diagnostic test
• Correct diagnosis must be established before initiating treatment– Signs and symptoms, careful history,
and physical examination– When uncertain, determination of BNP or
NT-proBNP can help confirm a diagnosis of HF
BNP = brain natriuretic peptide; NT‐proBNP = N‐terminal prohormone brain natriuretic peptide.
Patient Case: HF in ED
• 75-year-old obese white female• History of HF/COPD• Increased dyspnea for one week,
orthopnea• BP 150/90, HR 90• Lungs few crackles at base• JVP 15 cm Water
What historical feature makes HF more likely?
1. Past History of HF2. Orthopnea3. Duration of Symptoms4. Dyspnea
?

3
Framingham Criteria for the Diagnosis of CHF
• Major criteria– PND or orthopnea– Neck vein distention– Rales– Cardiomegaly– Acute pulmonary
edema– S3 gallop
• Minor criteria– Ankle edema– Night cough– Dyspnea on exertion– Hepatomegaly– Pleural effusion– Vital capacity ⇓ 1/3 from max– Heart rate >120 bpm
• Either major or minor– Weight loss >4.5 kg in 5 days in
response to treatmentbpm = beats per minute; CHF = congestive heart failure; CVP = central venous pressure; PND = paroxysmal nocturnal dyspnea; S3 = third heart sound Kannel WB, et al. Arch Intern Med. 1999;159(11):1197-1204.Marantz PR, et al. Circulation. 1988;77(3):607-612.McKee PA, et al. N Engl J Med. 1971;285(26):1441-1446. Redfield MM. Evaluation of congestive heart failure. In: Giuliani ER, et al, eds. Cardiology: Mayo Clinic Practice of Cardiology. 3rd ed. St Louis, Mo: Mosby; 1996:569-587.
(1) Concurrent presence of 2 major OR (2) Concurrent presence of 1 major and 2 minor criteria
Bedside Cardiovascular Examination in Patient With Severe CHF
• Only 3 of 15 with a low wedge had a high JVP or positive abdominojugular reflux test, spec of 80%
• 30 of 37 with a high wedge had either a high JVP or positive abdominojugular reflux test, sensitivity of 81%
• So a careful examination of the neck veins is the best physical exam technique for determining the fluid status in heart failure
Butman SM et al. J Am Coll Cardiol. 1993;22:955‐962.
ADHERE®: Clinical Presentation*
*All enrolled discharges (n = 187,565) from January 1, 2001 to March 31, 2006.
100 (n = 186,805)2
4850
SBP assessed<90 mm Hg 90–140 mm Hg >140 mm Hg
8934316665
Any dyspneaDyspnea at rest Fatigue RalesPeripheral edema
% Patients (n = 187,565)Symptom
ADHERE® National Registry Benchmark Report; 3/2006.
In the ER a BNP is ordered and is 400
1. This level of BNP confirms the diagnosis of HF
2. This level of BNP is in the “grey zone”; need to correlate it with the clinical picture
3. BNP not needed here because diagnosis of HF is already clear
4. This level of BNP is artificially low because the patient is obese
?
What correlates best with BNP levels?
1. The Ejection Fraction2. Level of Systolic Wall Stress3. The Wedge Pressure4. End Diastolic Wall Stress
?

4
Dao Q, et al. J Am Coll Cardiol. 2001;37:379‐385.
Mean BN
P Co
ncen
tration
(pg/mL)
AsymptomaticLV Dysfunction
(n = 14)
141 ± 3138 ± 4
No CHF(n = 139)
1076 ± 138
CHF(n = 97)
0
200
400
600
800
1000
1200
1400P < .001
BNP Levels of Patients Without CHF, With Baseline LV Dysfunction, and With CHF BNP Levels and ADHF Diagnosis
BNP level > 100 pg/mL: sensitivity of 90%, specificity 76%, and accuracy of 83% for differentiating CHF from other
causes of dyspnea
Mueller C, et al. N Engl J Med. 2004;350:647‐654.
HF likely>500
Use clinical judgment>100 but <500
HF DiagnosisPlasma BNP (pg/mL)
<100 HF unlikely
BNP and NT-proBNP Release
H P L G S PG S A SY T L RA P R S P
KMVQ
GSGCF
CRKMDR I S S
SSG
LCCKVL RRH
H2N—1
1070
7680
90
100
108proBNP
Cleavage by enzyme corin
H2N——COOH
S PKM
VQGS
GCF
CRKMDR I S S
SSGLCCK VL RRH
—COOH
H2N—HP L G S P G S A S Y T L RA P R1 10 70 76
BNPNT‐proBNP
—COOH
Inactive Metabolite Active Hormone
Adapted from Costello‐Boerrigter, et al. Nat Clin Pract Cardiovasc Med. 2005;2:194‐201.
B-Type Natriuretic Peptide Strongly Reflects Diastolic Wall Stress in Patients With Chronic Heart Failure
Comparison Between Systolic and Diastolic Heart Failure
Iwanaga, et al. JACC. 2006;47(4):742‐8.
“We have shown here conclusive
evidence that a widely used Point of Care Testing for measuring BNP‐32 is identifying forms of BNP different from the biologically active BNP‐32.”
Other Causes of Elevated BNP Levels
• LV systolic dysfunction• LVH with diastolic abnormalities• Significant pulmonary embolism• Cor pulmonale• Pulmonary hypertension• Aging (modest increases)• Renal insufficiency
LVH = left ventricular hypertrophy.Loke I, et al. Eur J Heart Fail. 2003;5:599. Schwam E. Acad Emerg Med. 2004;11:686.

5
Patient with dyspnea or other CHF signs/symptoms
Diagnostic for CHF Acute/chronic
CHF management(echocardiography,
if not done previously)Nondiagnostic
PositiveBNP blood test
Negative
Evaluate for non‐CHF etiologies(echocardiography usually not indicated)
Adapted from Maisel A. Rev Cardiovasc Med. 2002;3(suppl 4):S10‐S17.
ADHF Diagnostic Algorithm
History/physicalexam/ECG/chest x‐ray
Long-Term Goals Short-Term Goals
Ventricular RemodelingVascular Remodeling
Increased PCWPDecreased CO
Prevent CHF ProgressionAnd Death
Relief of Symptoms Stabilization of Organ
Functions
NeurohormonalAntagonists
HemodynamicAgents
Goals of Therapy:Chronic Versus Acute HF
PCWP = pulmonary capillary wedge pressure.
0 6 12 18 24Months
0
10
20
30
40
50
60Total Mortality Risk (%)
257
PCWP > 16 mm Hg
PCWP ≤ 16 mm Hg
P = .001
12Months
Total Mortality Risk (%)
n = 236
n = 220
Cardiac Index > 2.6 L/min/m2
Cardiac Index ≤ 2.6 L/min/m2
Final hemodynamic measurement in 456 patients with advanced HF after tailored vasodilator therapy
P = NS
Fonarow GC, et al. Circulation. 1994;90(4 pt 2):I488.
Early Response of PCWP But Not CI Predicts Subsequent Mortality in Advanced HF
0 6 12 18 240
10
20
30
40
50
60
n = 199
n = 257
ADHERE®: Evidence of Incomplete Symptom Relief at Discharge
*All enrolled discharges (n=150,745) from October 2001 to December 2004.
Asymptomatic 44%
Improved (but still symptomatic)
40%
No mention11%
No Change <1%No Change <1%Worse <1%Worse <1%Not applicable 4%Not applicable 4%
ADHERE® National Registry Benchmark Report; 12/2004.
Augmentcontractility
Diuretics Vasodilators Inotropes
Reducefluid
volume
Decreasepreloadand
afterload
Natriureticpeptides
ADHF Management: Pharmacologic Options
• Improve hemodynamic status of patient to relieve symptoms and stabilize organ functions
– Reduce right and left heart filling pressures
– Reduce systemic vascular resistance
– Increase cardiac output
• Pharmacologic options
Reduce fluid volume;Decrease
preload and afterload
Rapid Assessment of Hemodynamic Status and Treatment Options
LowPerfusionat Rest
Yes
No Yes
NoVasodilatorsNitroprussideNitroglycerin
orNatriuretic Peptide
Nesiritide
Inotropic drugsDobutamineMilrinone
DiureticsLoop diuretics
NormalSVR
HighSVR
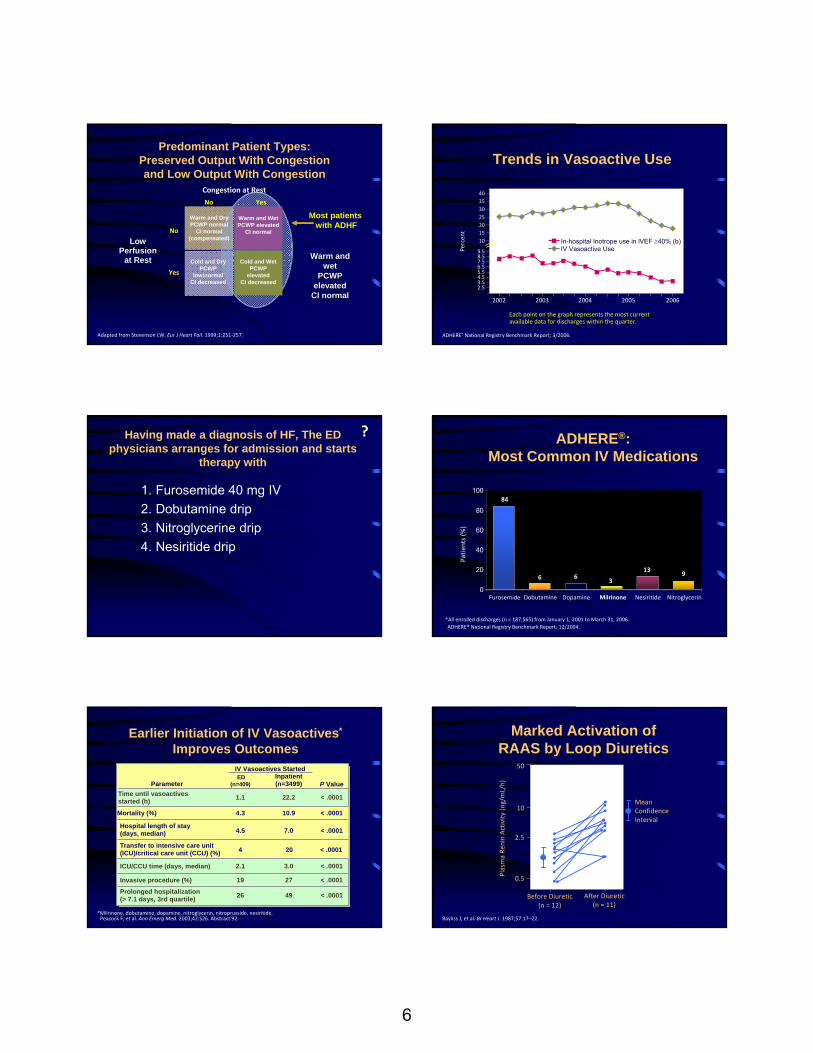
Congestion at Rest
Warm and DryPCWP normal CI normal
(compensated)
Warm and WetPCWP elevated
CI normal
Cold and WetPCWP elevatedCI decreased
Cold and DryPCWP
low/normalCI decreased
CI = cardiac index; SVR = systemic vascular resistance.Adapted from Stevenson LW. Eur J Heart Fail. 1999;1:251‐257.
6
Warm and DryPCWP normal
CI normal (compensated)
Warm and WetPCWP elevated
CI normal
Cold and WetPCWP
elevatedCI decreased
Cold and DryPCWP
low/normalCI decreased
Warm and Warm and wetwet
PCWP PCWP elevatedelevated
CI normalCI normal
Adapted from Stevenson LW. Eur J Heart Fail. 1999;1:251‐257.
Predominant Patient Types: Preserved Output With Congestion and Low Output With Congestion
Most patients with ADHF
LowPerfusion
at RestYes
No Yes
No
Congestion at Rest
3.54.55.56.57.58.5
Trends in Vasoactive Use
2.5
9.5
10
2025303540
15
In-hospital Inotrope use in lVEF ≥40% (b)IV Vasoactive UsePe
rcen
t
2002 2003 2004 2005 2006
Each point on the graph represents the most current available data for discharges within the quarter.
ADHERE® National Registry Benchmark Report; 3/2006.
Having made a diagnosis of HF, The ED physicians arranges for admission and starts
therapy with
1. Furosemide 40 mg IV2. Dobutamine drip3. Nitroglycerine drip4. Nesiritide drip
? ADHERE®: Most Common IV Medications
84
6 63
139
0
20
40
60
80
100
Patie
nts (%
)
Furosemide Dobutamine Dopamine Milrinone Nesiritide Nitroglycerin
*All enrolled discharges (n = 187,565) from January 1, 2001 to March 31, 2006.ADHERE® National Registry Benchmark Report; 12/2004.
< .0001
< .0001204Transfer to intensive care unit (ICU)/critical care unit (CCU) (%)
< .00017.04.5
< .000110.94.3Mortality (%)
Hospital length of stay(days, median)
< .0001
< .0001
< .0001
P Value
IV Vasoactives Started
Peacock F, et al. Ann Emerg Med. 2003;42:S26. Abstract 92.
Earlier Initiation of IV Vasoactives*
Improves Outcomes
22.21.1Time until vasoactivesstarted (h)
4926Prolonged hospitalization(> 7.1 days, 3rd quartile)
2719Invasive procedure (%)
3.02.1ICU/CCU time (days, median)
ED (n=409)Parameter
*Milrinone, dobutamine, dopamine, nitroglycerin, nitroprusside, nesiritide.
Inpatient (n=3499)
Bayliss J, et al. Br Heart J. 1987;57:17–22.
Plasma Re
ninActivity
(ng/mL/h)
Before Diuretic(n = 12)
After Diuretic(n = 11)
50
10
2.5
0.5
Mean Confidence Interval
Marked Activation of RAAS by Loop Diuretics

7
On the Other Hand, Diuretics May Impair Renal Function More Than Has Been Appreciated
BG9719 BG9719 Furosemide
FurosemideAlone
Placebo
15
5
‐5
‐15
‐25
GFR(% change)(1‐8 hours)
Urine Output (mL)(0‐8 h, Day 1 – Baseline)
500 1000 1500 2000 2500
GFR = glomerular filtration rate.Gottlieb SS, et al. Circulation. 2002;105:1348‐1353.
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16
Survival (%
)
P < .00010‐40 (n = 465)
40‐80 (n = 365)
80‐160 (n = 320)
>160 (n = 204)
18
Relation of Loop Diuretic Dose to Mortality in HF
20 24
Time (months)
80
Eshaghian S, et al. Am J Cardiol. 2006:97:1759‐1764.
22
Renal Insufficiency and Chronic Diuretic Therapy
Data from ADHERE; 46,599 patients with ADHF; > 260 participating hospitals
2.73.3
5.5
7.8
5.5 5.8 6.16.9
0
2
4
6
8
10
No Chronic Diuretic Tx Chronic Diuretic Tx
SCr <2.0 SCr ≥2.0 SCr <2.0 SCr ≥2.0
P < .0001
Mortality(% Patients)
Length of Hospital Stay(Days)
P < .0001
ADHERE® National Registry Benchmark Report; 12/2004.
Continuous Infusion Versus Bolus IV Doses of Diuretics
• A meta-analysis by the Cochrane Collaborative in 2005 found that continuous infusion of diuretics resulted in benefit over bolus IV doses with respect to total urine output, length of stay, mortality, and effect on creatinine levels
• Benefit is that lower doses of diuretics can be used
Salvador DR, et al. Cochrane Database Syst Rev. 2005;(3):CD003178.
Fluid Removal by Ultrafiltration
H2O
• Ultrafiltration removes fluid from blood at same rate fluid can be naturally recruited from tissue
• This “balanced diuresis”maintains sufficient intravascular volume during restoration of body’s fluid balance, decreasing risk of hypotension
• In addition, electrolyte composition of blood and ultrafiltrate remains in balance, resulting in removal of excess fluid
Resource Allocation for Patients With HF 90 Days After Discharge
18
32
21
44
0
10
20
30
40
50UltrafiltrationStandard care
Rehospitalization Unscheduled Officeand/or ER Visits
Patie
nts (%
)
Costanzo MR, et al. J Am Coll Cardiol. 2007;49:675‐683.
UNLOAD
Open Label (N = 200)

8
Summary: Diuretic Therapy ADHF
• First-line treatment in patients with fluid overload
• End point of diuretic therapy is the resolution of congestive symptoms
• Limited data on long-term use in HF• Complications associated with diuretics include
diuretic resistance, neurohormonal activation, and reduced GFR
• Ultrafiltration therapy may be viable alternative
IV Milrinone During Hospitalization for ADHF
12.5
2.1
10.7
3.21.5
0.4
4.6
1.53.8
2.3
0
5
10
15
20
MilrinonePlacebo
Treatment Failure From Adverse Event
(48 h)
SustainedHypotension
A Fib Mortality
P < .0001
Even
t Rate (%
)
OPTIME‐CHF: In‐Hospital Adverse Events
P < .0001
Acute MI
P < .018
P < .004P < .19
Cuffe MS, et al. JAMA. 2002;287:1541‐1547.
Inotropic Therapy in Patients With ADHF
• Routine use not indicated in short- or long-term setting (despite low EF)
• Rather, inotropes should only be used in patients with:– Cardiogenic shock– Decompensated patients refractory to diuretics– Short-term bridge to definitive treatment such as
revascularization or cardiac transplantation
Felker GM, et al. Am Heart J. 2001;142:393‐401.
Role of the Kidney in Congestive Heart Failure: Relationship of CI to Kidney Function
Group AGroup An=12n=12
Group BGroup Bn=13n=13
Group C Group C n=9n=9
Pvalue
Car. Index 2.42.4±±.15.15 1.781.78±±.17*.17* 1.351.35±±.14*.14* * <.001
SVR 13131313±±296296 18661866±±455*455* 24642464±±956**956** * <.01** <.001
RA 77±±88 1010±±55 1414±±88 ns
Wedge 1919±±1111 2929±±7*7* 3030±±8*8* * <.01
Ljungman, Cody Drugs 1990;39 Suppl 4:10-21
Role of the Kidney in Congestive Heart Failure: Relationship of CI to Kidney Function
Ljungman, Cody Drugs 1990;39 Suppl 4:10-21
0
100
200
300
400
500
A, CI> 2 B, CI>1.5<2.0
C, CI <1.5
Renal BFRV Resistance
Renal Blood Flow
RenovascularResistance
RBF, p<.05 with Group A
RVR, p<.01 with Group A
Role of the Kidney in Congestive Heart Failure: Relationship of CI to Kidney Function
Ljungman, Cody Drugs 1990;39 Suppl 4:10-21
0
10
20
30
40
50
60
70
A, CI> 2 B, CI>1.5 <2.0 C, CI <1.5
GFRBUN
GFR/
BUN
CI, p<.001 with Group A BUN, p<.01 with Group A
Creatinine was not different between the groups. BUN better indicated low CI and GFR than creatinine

9
Pharmacologic Actions of Human BNP
• Hemodynamic(balanced vasodilation)– Veins
– Arteries
– Coronary arteries
• NeurohumoralAldosterone
Endothelin
• RenalDiuresis
Natriuresis
DR I
MKRG
S SSSGLG
FC CS SG
SGQVMK V L R R
H
KPS
ADHERE®: Use of IV Diuretics and IV Vasoactive Treatments*
IV Vasoactive28%2.7 d21.9 h51%2.2 h
Discharges who were given IV vasoactive txMean duration of IV vasoactive txMean time to first IV vasoactive tx
IV therapy started in ED and/or OUMean time to first IV vasoactive tx
88%3.0 d8.1 h75%2.2 h
Discharges who were given IV diuretic txMean duration of IV diuretic txMean time to first IV diuretic tx
IV therapy started in ED and/or OUMean time to first IV diuretic tx
The Nation (n = 187,565)IV Diuretic
*All enrolled discharges (n = 187,565) from January 1, 2001 to March 31, 2006.ADHERE® Q1 2006 Final Cumulative National Benchmark Report. www.adhereregistry.com. Accessed April 10, 2007.
P < .01
P < .01
P < .05
Placebo Nesiritide
PAP = peak airway pressure; MAP = mean airway pressure; RAP = right atrial pressure.Marcus LS, et al. Circulation. 1996; 94:3184‐3189.
20
30
40
50
0 0.003 0.01 0.03 0.1
5
10
15
20
25
30
0 0.003 0.01 0.03 0.1
0
5
10
15
0 0.003 0.01 0.03 0.1
657075808590
0 0.003 0.01 0.03 0.1
1.75
2
2.25
2.5
2.75
0 0.003 0.01 0.03 0.1
60
70
80
90
100
0 0.003 0.01 0.03 0.1
Mean PAP
PCWP
RAP
MAP
CI
HR
Dose µg/kg/min Dose µg/kg/min
Hemodynamics of Nesiritide
P < .01
P < .01
P < .01
VMAC: Nesiritide vs IV NTG on PCWPCh
ange From Baseline in PCW
P (m
m Hg)
End of Placebo‐Controlled Period
Time on Study Drug (h)
During 3‐h placebo period:Placebo, n = 62 IV NTG, n = 60Nesiritide, n = 124
† P ≤ .05 vs IV NTG* P ≤ .05 vs Placebo
†*
0 0.25 0.5 1 2 3 6 9 12 24 36 48
‐9
‐8
‐7
‐6
‐5
‐4
‐3
‐2
‐1
0PCWP - Placebo
PCWP - IV NTG
PCWP - Nesiritide
†*
†* †
** †
* †
††
†
*
VMAC = Vasodilatation in the Management of Acute CHF; NTG = nitroglycerin.Publication Committee for the VMAC Investigators. JAMA. 2002:287:1531‐1540.
After 3‐h periodIV NTG, n = 92Nesiritide, n = 154
Cardiac Output = VTI x Area of Outflow Tract x Heart Rate

10
Hemodynamic Echo-The Noninvasive Swan
• Right Atrial pressure (Inferior Vena Cava)• Pulmonary Artery Pressure (TR Velo + RA)• Estimated mean left atrial pressure (E/E�)• Cardiac Output (VTI x Area x HR)• Systemic Vascular Resistance
(MAP-RA)x80/CO
Impact of Early Initiation of Nesiritide for ADHF
3.13.9
5.2
6.9
3.0 3.5
2.0
7.0
0
2
4
6
8
10
Mortality(%)
Mean HospitalLOS (days)
Mean ICU/CCULOS (days)
ICU Transfers(%)
P = .03
P < .001P < .001
LOS = length of stay.Peacock WF, et al. Cardiology. 2007;107:44‐51.
EDInpatient
Despite 80 Mg Furosemide IV, The Patient Remains Very Short Of Breath, What May Be
Done At This Point?
1. Digoxin 0.25 mg IV2. Repeat 80 mg furosemide IV3. Add nitroglycerin drip4. Add nesiritide5. Add dobutamine
?
Odds Ratio (95% CI)
Nesiritide Better Nesiritide Worse
0.01 μg/kg/min1.35 (0.88‐2.06); P = .17
0 1 2 3 4 5
Relative Risk of SCr > 0.5 mg/dL by Nesiritide Initiation Dose
Sackner‐Bernstein JD, et al. Circulation. 2005;111:1487‐1491.
0.015 μg/kg/min
0.03 μg/kg/min
1.90 (1.02‐3.54); P = .02
2.58 (1.40‐4.74); P = .001
Nesiritide Dose
Nesiritide and SCr Relationship to Diuretic Dose in VMAC
21 20.2 21.4
32.9
0
10
20
30
40NTGNesiritide
Low‐/Moderate‐DoseDiuretic
High‐DoseDiuretic
Patie
nts With
SCr> 0.5 mg/dL
(%)
P = .044
Heywood JT. Presented at: 9th Annual Meeting of the Heart Failure Society of America; Sept. 18‐21, 2005; Boca Raton, FL. Abstract 240.
2
1 100.1
Mills et al
Efficacy
Comparative
PRECEDENT
VMAC
PROACTION
FUSION I
Pooled (6 Studies*)
Pooled (7 Studies)
Hazard Ratio (95% Confidence Interval)
9
Study
30-Day Mortality Hazard Ratios
HR (95% CI)0.38 (0.05, 2.67)1.25 (0.24, 6.45)1.43 (0.52, 3.97)0.60 (0.18, 1.97)1.56 (0.75, 3.24)7.03 (0.87, 57.15)0.49 (0.07, 3.46)1.41 (0.88, 2.26)1.34 (0.85, 2.11)
* Excludes FUSION INesiritide Prescribing Information, January 2007
11
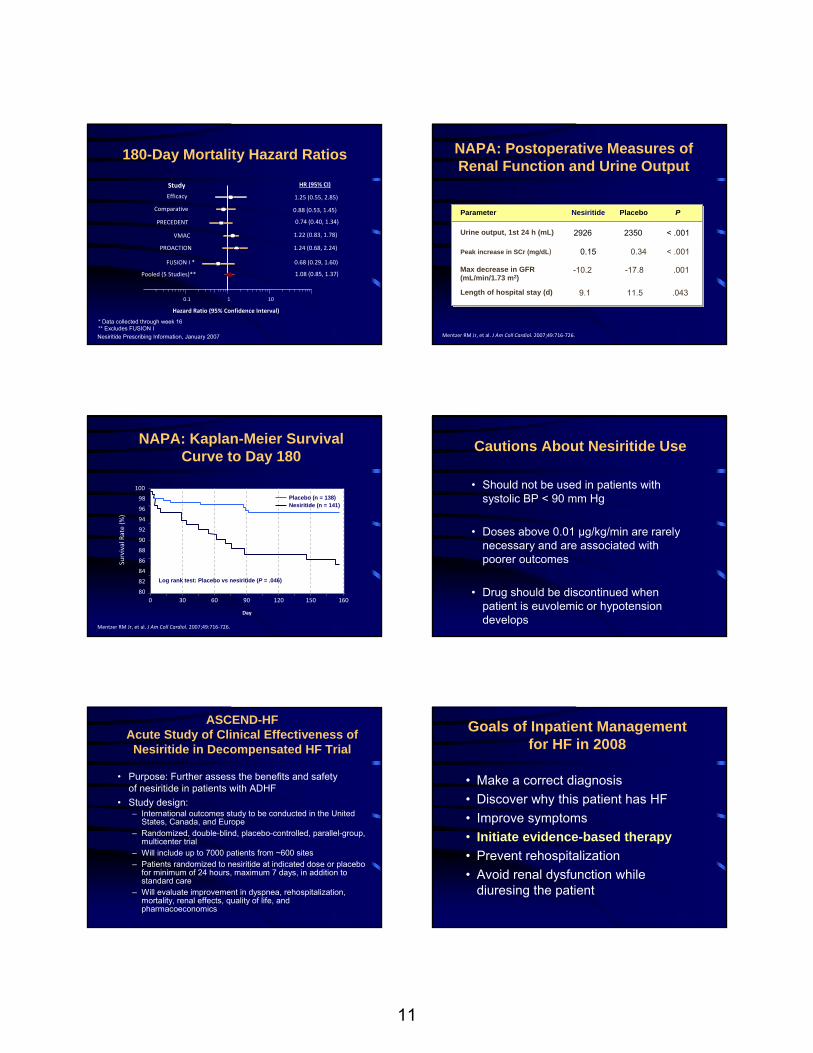
* Data collected through week 16** Excludes FUSION I
180-Day Mortality Hazard Ratios
Nesiritide Prescribing Information, January 2007
1 100.1
Hazard Ratio (95% Confidence Interval)
FUSION I *
PRECEDENT
Efficacy
Comparative
PROACTION
Pooled (5 Studies)**
VMAC
HR (95% CI)
1.25 (0.55, 2.85)
0.88 (0.53, 1.45)
0.74 (0.40, 1.34)
1.22 (0.83, 1.78)
1.24 (0.68, 2.24)
0.68 (0.29, 1.60)
1.08 (0.85, 1.37)
Study
NAPA: Postoperative Measures of Renal Function and Urine Output
.04311.59.1Length of hospital stay (d)
< .0010.340.15Peak increase in SCr (mg/dL)
< .00123502926Urine output, 1st 24 h (mL)
PPlaceboNesiritideParameter
Mentzer RM Jr, et al. J Am Coll Cardiol. 2007;49:716‐726.
.001-17.8-10.2Max decrease in GFR (mL/min/1.73 m2)
Log rank test: Placebo vs nesiritide (P = .046)
92
80
82
84
86
88
90
0 30 60 90 120 150
Survival Rate (%
)
Placebo (n = 138)Nesiritide (n = 141)
160
NAPA: Kaplan-Meier Survival Curve to Day 180
94
96
98
100
Day
Mentzer RM Jr, et al. J Am Coll Cardiol. 2007;49:716‐726.
Cautions About Nesiritide Use
• Should not be used in patients with systolic BP < 90 mm Hg
• Doses above 0.01 µg/kg/min are rarely necessary and are associated with poorer outcomes
• Drug should be discontinued when patient is euvolemic or hypotension develops
ASCEND-HFAcute Study of Clinical Effectiveness of
Nesiritide in Decompensated HF Trial
• Purpose: Further assess the benefits and safety of nesiritide in patients with ADHF
• Study design:– International outcomes study to be conducted in the United
States, Canada, and Europe– Randomized, double-blind, placebo-controlled, parallel-group,
multicenter trial – Will include up to 7000 patients from ~600 sites– Patients randomized to nesiritide at indicated dose or placebo
for minimum of 24 hours, maximum 7 days, in addition to standard care
– Will evaluate improvement in dyspnea, rehospitalization, mortality, renal effects, quality of life, and pharmacoeconomics
Goals of Inpatient Management for HF in 2008
• Make a correct diagnosis• Discover why this patient has HF• Improve symptoms• Initiate evidence-based therapy• Prevent rehospitalization• Avoid renal dysfunction while
diuresing the patient

12
Digoxin
• Reduces hospitalization for HF, no reduction in mortality (Class IIa, Level B)
• Digoxin should not be used in asymptomatic patients in sinus rhythm with LV dysfunction because the risk of harm not balanced by benefit (Class III)
• In new guidelines, digoxin has fallen from a Class 1 drug for HF to Class IIa
Hunt SA, et al. Circulation. 2005;112:e154‐e235. Epub 2005 Sep 13.
0
0.2
0.3
0.4
0.5
0.6
0.8
0 3 6 9
Cumulative
Prob
ability of D
eath
PlaceboEnalapril
12
CONSENSUS
Consensus Trial Study Group. N Engl J Med. 1987;316:1429‐1435.
0.1
0.7
Months
Guidelines
• ACEI first choice• Use ARB if ACEI intolerant• CHARM and ValHeft trials show that ARB
reduces mortality in patients taking ACEI • May add ARB to ACEI if patient remains
symptomatic• Do not use ACEI, ARB, and
spironolactone together
RALES Trial
0
.50
.55
.60
.65
.70
.80
Survival
Placebo
Spironolactone
12
.45
.75
15 18 21 24 27 30 33 36
.85
.90
1.00.95
0 3 6 9
RALES Study Group. Am J Cardiol. 1996;78:902‐907.
Months
Aldosterone Antagonists Recommendations
• Addition of an aldosterone antagonist is reasonable in selected patients with NYHA Class III-IV HF, SCr < 2.5 in men, ≤ 2 in women, K+ < 5.0
• Must be carefully monitored 3 days after starting, then 1 week and at least monthly for 3 months
• Usually discontinue oral potassium• May start at very low dose of spironolactone or
eplerenone, 6.25 or 12.5 mg per day or every other day
• Use of ACEI, ARB, and aldosterone receptor blocker notrecommended (Class III recommendations)
All‐Cause Mortality
0 3 6 9 12 15 18 21
35% in riskP = .00013
% Survival
Carvedilol
Placebo
100
90
80
60
70
0
Months
↓
COPERNICUS
Krum H, et al. JAMA. 2003;289:712‐718.

13
Number at risk
Carvedilol 1511 1367 1259 1155 1002 383Metoprolol 1518 1359 1234 1105 933 352
Time (years)
Mortality (%
)
Poole‐Wilson PA, et al. Lancet. 2003;362:7‐13.
COMET
0
10
20
30
40
0 1 2 3 4 5
Metoprolol
Carvedilol
Hazard ratio 0.83, 95% CI 0.74-0.93, P = .0017
Summary: Evidence-Based Therapies in HF
• Beta blockers (BBs) are recommended for all stages of HF for those who tolerate them
• Only BBs which have been shown to reduce mortality in large trials should be used: bisoprolol, carvedilol, and long-acting metoprolol
• It is not necessary to up-titrate ACEI to maximum doses before starting BB
Fonarow GC, et al. J Card Fail. 2007;13(9):722‐31.
Goals of Inpatient Management for HF in 2008
• Make a correct diagnosis• Discover why this patient has HF• Improve symptoms• Initiate evidence-based therapy • Improve compliance• Prevent rehospitalization• Avoid renal dysfunction while diuresing
the patient
To Reduce Hospitalizations…
• Appropriate medical therapy• Patient education• Risk-factor modification• Close follow-up (1 week or less)
Discharge Education Improves Clinical Outcomes in Patients With CHF
Benefits of 1 h of inpatient education
for patients admitted with HF
Koelling TM, et al. Circulation. 2005;111:179-185. Epub 2005 Jan 10.
Event-free survival defined as time to first hospitalization or death for control (blue) and education (red) subjects. For log-rand comparison, P = .012.
Cum
ulat
ive
Even
t-Fre
eSu
rviv
al
.3
.5
.6
.4
.7
.8
1.0
.9
0 60 120 180Days

14
What Are Goals of Inpatient Management for HF in 2008?
• Make a correct diagnosis• Discover why this patient has HF• Improve symptoms• Initiate evidence-based therapy • Prevent rehospitalization• Avoid renal dysfunction while
diuresing the patient 0
20
40
60
80
100
The Prognostic Importance of Different Definitions of Worsening
Renal Function in CHF
0
20
40
60
80
100
≥ 0.2 ≥ 0.3 ≥ 0.4 ≥ 0.5
Increase in Creatinine (mg/dL)
SensitivitySpecificity
≥ 0.1
Risk of Death or
Hospitalization> 10 days
Gottlieb SS, et al. J Card Fail. 2002;8:136‐141.
How to Avoid Worsening Renal Function While Treating ADHF
• Use smallest dose of diuretic that is effective• Continuous infusions of diuretics may be
preferred• Careful monitoring of BUN, creatinine
(twice daily preferred)• Stop diuretics when neck veins are normal or
25% increase in BUN, creatinine• If nesiritide is used, same principles apply;
most patients should require only 24 h of the drug
Diur
Concept of Plasma Refill Rate in ADHF
Diuretics to increase
sodium loss and decrease
venous pressures
Nesiritide to reduce venous pressure
Diur
Concept of Plasma Refill Rate in ADHF
Nesiritide to reduce venous pressure
Diuretics to increase
sodium loss and decrease
venous pressures
When do you stop IV diuretics in Acute Decompensated Heart Failure?
1. When the patients symptoms are improved
2. When the neck veins have returned to normal
3. When rales are gone4. When edema is resolved5. When the BUN or creatinine have risen
by 50%
?

15
My Preferred Management for Hospitalized Patients With HF
(Normotensive, Fluid Overload)
• 20 mg IV furosemide• Metolazone if significant edema• IV nesiritide for selected patients• Furosemide drip 100 mg/100 mL, 3 mg/h• Captopril 6.25 mg tid, double dose as
tolerated q8H if not already on an ACEI or ARB
• Target urine output 300 cc/h
AJR = abdominal jugular reflux.
My Preferred Management for Hospitalized Patients with HF
(Normotensive, Fluid Overload) (cont’d)• Replace K+ 30 mEq KCl per liter of urine
produced• Start carvedilol when neck veins normal• Switch to once a day ACEI or ARB• Monitor electrolytes, BUN, creatinine q12h• Stop furosemide when JVP is normal or >20%
increase in BUN, creatinine• Decrease or stop nesiritide when AJR is normal• Home
![European Respiratory Society guidelines for the diagnosis ... · standard diagnostic test for PCD [1]. Current diagnosis requires a combination of technically demanding Current diagnosis](https://static.documents.pub/doc/80x56/5e0b785e5afa7874a7215a8f/european-respiratory-society-guidelines-for-the-diagnosis-standard-diagnostic.jpg)
















