55
Current treatments and future prevention of dementia John O’Brien Professor of Old Age Psychiatry University of Cambridge

Current treatments and future prevention of dementia
John O’Brien
Professor of Old Age Psychiatry
University of Cambridge


PM Challenge on dementia 2020. By 2020
• England to be the best place
in the world to undertake dementia research
• 25% of people with diagnosed
dementia on Join Dementia Research (JDR)
• 10% participating in research
(up from 4.5% today)
• On track for cures or disease modifying therapies by 2025

Frau Auguste Deter. (“Auguste D”)
In 1901 aged 51 started accusing husband of having an affair with a
female neighbour
Rapidly increasing memory impairments
“Home life became disordered” for 8 months before Karl asked for help from the family doctor and Auguste was admitted to the
Municipal Asylum for the insane and epileptic in Frankfurt am Main.
Asked to write her name she was unable and said
“I have, so to speak, lost myself.”
Frequently agitated she spent long periods in
the bath and in an isolation room at night
Died April 1906 mute and bedfast with pneumonia and bedsores
Alzheimer reported on a
“peculiar substance in the cerebral cortex”

Cholinergic Loss in AD

Anti-dementia drugs:
a rational therapeutic approach

Currently licenced drugs for AD
• Donepezil (Aricept)• Mild to moderate AD• 5-10 mg od
• Rivastigmine (Exelon)• Mild to moderate AD• 1.5 - 6 mg bd (now daily patch)
• Galantamine (Reminyl)• Mild to moderate AD• now XL dose, 8-24mg od
• Memantine (Ebixa)• NMDA receptor antagonist• Moderate to severe AD• 5- 10 mg bd (now 10-20 mg od)
Broadly similar in efficacy
and side effects
Introduced 1997-2002
No new drug for 15+ years

Treatments since 1997: Donepezil in Mild to Mod AD
Rogers et al, 1998

134 subjects with ADDonepezil 10mg
Placebo
Donepezil
Holmes et al, 2004

Gauthier et al, 2008;
Mecocci et al, 2009
Memantine in Mod to Severe AD: effects on cognition and behaviour
Pooled analysis

The double hurdle
Licensing:
MHRANHS use:
NICE

Effect of dementia severity on ADAS-cog change (n=5216)
Mild
(21+)
N=2218
Moderate
(15-20)
N=2163
Moderately severe
(10-14)
N=835
Meta-analysis
(all drugs)
1.86
(0.83-2.89)
3.98
(3.22-4.74)
5.44
(3.94-6.94)
MCR biostatistics analysis for NICE, Jan 2006, www.nice.org.uk

Benefit of drugs more apparent in non-responders than responders
NICE 2005 re-analysis of responder data
R
NR

0 10 20 30 40 50 60
COG+G+F
COG+G
COG
Patients’ Meeting Definition of Clinical Worsening (%)
P < .0001
* Analysis of clinical worsening at Week 24.
.
51.2%
36.3%
31.4%
16.0%
21.3%
7.2%
Donepezil
Placebo
Proportion With Clinical Worsening (Mild AD, MMSE 18-26)
P < .001
P < .01
Wilkinson D, et al. Dement Geriatr Cogn Disord2009;28:244251

RCT of Rivastigmine in Dementia with Lewy Bodies
-2.0
-1.5
-1.0
-0.5
0.0
0.5
Rivastigmine
Placebo
Change From Baseline–Week 20 on Neuropsychiatric Inventory
Improvement
Apathy
Anxiety
Hallucinations
Delusions
Irritability
McKeith et al. Lancet. 2000;356:2031-2036.NB No drugs are licensed for the treatment
of dementia with Lewy bodies

Cognition Global ADL Neuropsychiatric
symptoms
Galantamine (Gal-INT-06), Erkinjuntti et al,
(n=121 with NINDS/AIREN probable VaD)
No (p=0.06)
-1.8 points on ADAS-Cog
No No No
Galantamine (Gal-INT-26), Auchus et al,
(n=788 with NINDS/AIREN probable VaD)
Yes (p<0.001)
-1.9 points on ADAS-Cog
No No No
Donepezil (307), Black et al
(n=603 with NINDS/AIREN probable or possible VaD)
Yes (p<0.001)
-2.2 points on ADAS-Cog
No Yes N/A
Donepezil (308) , Wilkinson et al
(n=616 with NINDS/AIREN probable or possible VaD)
Yes (p<0.001)
-2.1 points of ADAS-Cog
Yes No N/A
Donepezil (319), Roman et al,
(n=974 with NINDS/AIREN probable or possible VaD)
Yes (p<0.001)
-0.9 points on VADAS-Cog
No No N/A
Rivastigmine (VantageE), Ballard et al
(n=710 with NINDS/AIREN probable VaD)
Yes (p=0.028)
-1.3 points on VADAS-Cog
No No No
RCTs of cholinesterase inhibitors in VaD
O’Brien and Thomas, Lancet 2015

Cognitive side effects
greater in memantine
group
Boxer et al, 2013
Boston naming
test
Digit symbol
substitution
test

Mild Cognitive Impairment
NB No drugs are licensed for the treatment
of Mild Cognitive Impairment
Raschetti et al, 2007


D + M
P
D
M

Lopez et al, 2009

Summary of the 4 current anti-dementia drugs
• Work in AD and DLB; not MCI or VaD; make FTD worse
• CholEI effective in mild, mod and severe AD (only licensed for mild to mod)
• No difference in efficacy between donepezil, rivastigmineand galantamine, but SEs differ
• Memantine effective in mod and severe AD, can be co-prescribed with CholEI with added benefit*
• Efficacy worthwhile but modest; “stabilisation/
improvement” equivalent to 6-9 months natural decline
*EFNS Guidelines on co-prescription 2015

Anti-dementia drugs:beyond modest symptomatic improvement

Control AD at time of diagnosis
AD at loss of independence
Brain changes in Alzheimer’s disease

Adapted from Dodel et
al, Lancet Neurology2003
The amyloid cascade
hypothesis of
AD
Inflammation Transmitter loss

12/12 18/12, no
vaccine
18/12, +
vaccine
Schenk et al, Nature 1999
A vaccine for Alzheimer’s disease?

Holmes et al, Lancet, 2008

Salloway et al, 2009
Vasogenic oedema related to Apo E4
(4% if no E4, 33% if homozygous)

Disease modifying trials in AD
Drug and mechanism of action Phase 3 resultsTramiprosate 2007
Abeta aggregation inhibitor
No benefit (Aisen et al. 2011)
Tarenflurbil 2008
Gamma-secretase modulator
No benefit (Green et al. 2009)
Semagecestat 2010
Gamma secretase inhibitor
Significantly worse than placebo, trials halted
Bapineuzumab 2012
Antibody to acids 1-5 of Abeta peptide
Phase 2 studies positive. No benefit in two phase 3
studies, programme suspended in 2012
Solanezumab 2012
Antibody to 16-24 of Abeta peptide
Failed to meet primary endpoint but signal in mild
patients
Solanezumab 2016 Failed to meet primary endpoint

Ongoing trials in dementia
• 25 Phase 3 studies
• 72 Phase 2 studies
• 27 Phase 1 studies
• Targeting amyloid (38), tau (6), inflammation (13), neurotransmitters (20), other
Alz Forum, November 2017

This mutation reduces the production of
Abeta by 20-40% throughout life
Jonsson et al, Nature, 2012

Biomarkers for AD
CSF measures of
A-beta42 and p-tau
Hippocampal
atrophy on MRI
Increased uptake
on amyloid-PET
Hypometabolism
on FDG PET
Increased uptake
on tau (AV1451) PET

Bateman RJ et al. N Engl J Med 2012;367:795-804.
Relationship between AD biomarkers

Sevigny et al, Nature, 2016
ARIA:
5% - Placebo
6% - 1mg
13% - 3mg
37% - 6mg
47% - 10mg


• 18 month RCT n= 891 mild
to mod AD
• 2 doses 75mg &125mg
• Drug missed its co-primary
end points of ADAS-COG
and ADCS-ADL
• 30% drop out
AAIC Toronto July 2016
LMTX (anti-tau) study in AD

30 subjects with AD, first in man study
29/30 developed anti-tau antibodies
No cases vasogenic oedema
One case worsening microbleeds
Ongoing phase 2 in AD (ADAMANT)

Prevention

Villemagne et al, Lancet Neurol, 2013
Amyloid β deposition in Alzheimer’s disease: a prospective cohort study

PREVENT Dementia study (sporadic dementia)
• 4 site study, Cambridge, Imperial, Oxford, Edinburgh
• Aim to recruit 600-700 cognitively normal 40-59 y.o.
• 50% group at increased risk of dementia (one or both
parents have dementia)
• 50% group at average risk (neither parent has dementia)
• Comprehensive assessment over 3-4 visits
− Baseline physical, cognition, blood, urine and salivary
− Multi-modal 3T MR scan
− Lumbar puncture for CSF
− Additional amyloid imaging and 7T MR planned
• Follow-up at 2 and 5 (and 10) years
Ritchie et al, Alz and Dementia, 2017

No FH n=107 FH n=103 Sig
Age 52.7 53.3 ns
Female 69% 72% ns
Postgrad education 26.4% 39.8% P=0.003
Hypertension 16.8% 17.5% ns
Diabetes 2.8% 6.8% ns
Depressive symptoms 17.8% 15.5% ns
ApoE4 28% 45% P=0.01
Mean age dementia diagnosis in parent = 72 years
Results from first 200 subjects

Hippocampal subfields segmentation
1. Subiculum, 2. Entorhinal cortex (ERC), 3. Cornu Ammonis 1 (CA1) subfield, 4. Cornu
Ammonis 3/dentate gyrus (CA3/DG) subfield 5. Cornu Ammonis 2 (CA2) subfield
Su et al, in preparation

★★★★
• Significant atrophy of the subiculum (p=0.0061) in
subjects with FHSu et al, in preparation
…
…
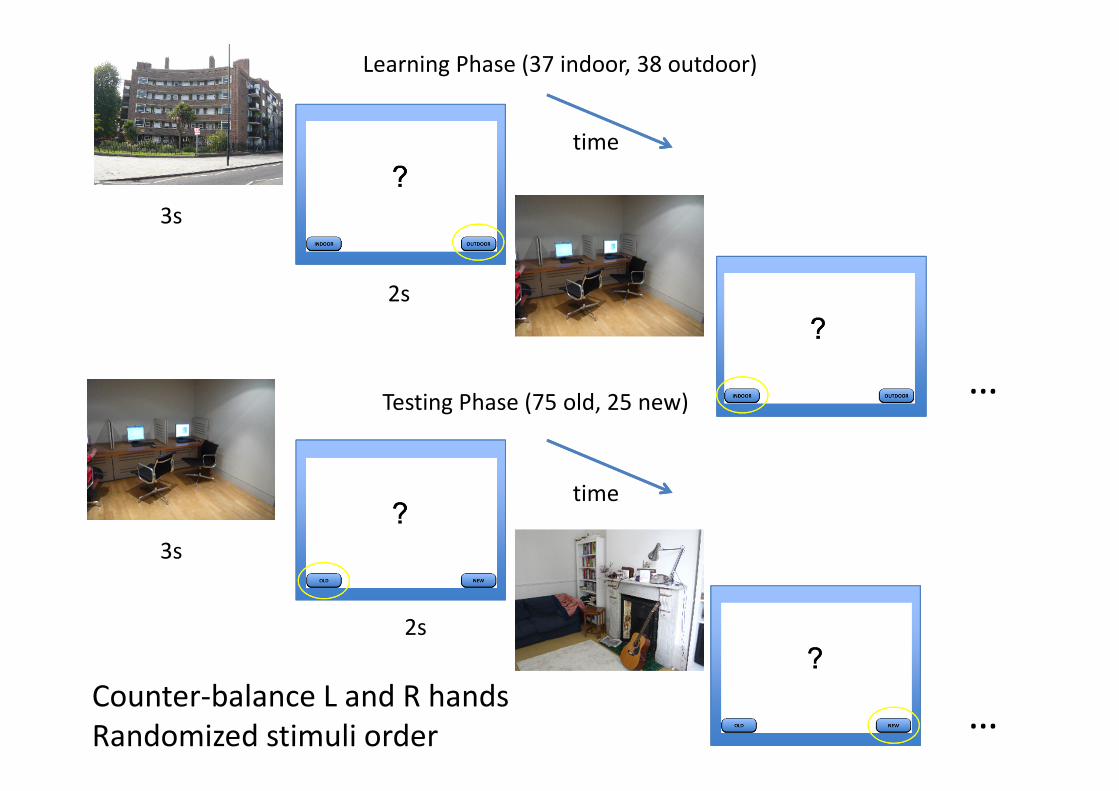
Learning Phase (37 indoor, 38 outdoor)
Testing Phase (75 old, 25 new)
time
time
3s
2s
3s
2s
Counter-balance L and R hands
Randomized stimuli order

ERS Results
hippocampus
parahippocampus
Su et al, in preparation

Risk and protective factors for Alzheimer’s disease (and other dementias)
• Increasing age
• Female sex
• Down’s syndrome
• Autosomal dominant AD genes
• ApoE4 genotype
• Other risk genes
• Previous head injury
• Past history depression
• Hypertension
• Diabetes
• Smoking
• Obesity
• Stroke
• Raised cholesterol
• Raised homocysteine
• Low educational level
Protective factors (?)
• Exercise
• Diet
• Education
• Statins
• Prior NSAID use
• Hormone replacement therapy
• Social/ mental activities

Study of 7,500 people
Odds ratio 0.7
Lancet 2013

Prevalence of dementia decreased from 30% to 22% over 22 year periodRegression analysis showed effect driven by higher education and reduction in dementia after stroke
Skoog et al, Scientific Reports, 2017

Effects of anti-hypertensives on cognition
Levi Marpillat et al J Hypertension, 2013
Angiotensin Receptor blockers (ARBs) most effective

Effects on preventing dementia
Levi Marpillat et al J Hypertension, 2013

Livingston et al, 2017
Estimated that
one third of all dementia due to
potentially
modifiable risk factors
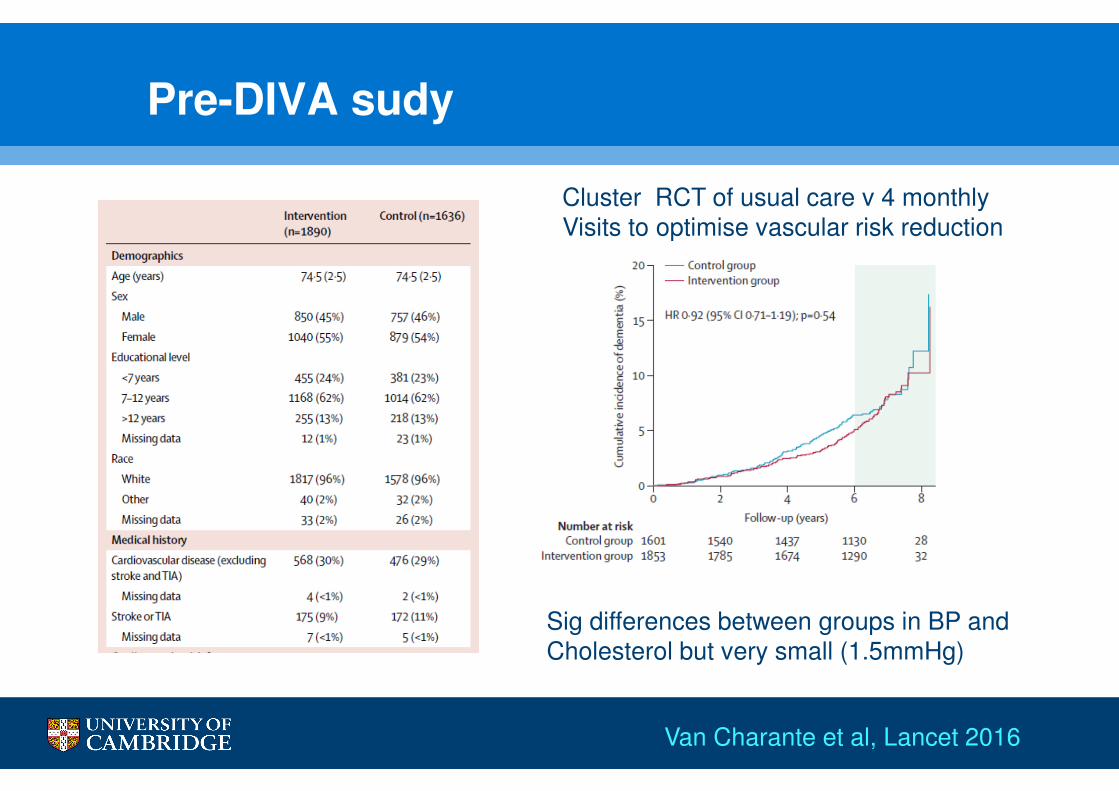
Pre-DIVA sudy
Also 7y outcomeVan Charante et al, Lancet 2016
Cluster RCT of usual care v 4 monthly Visits to optimise vascular risk reduction
Sig differences between groups in BP and Cholesterol but very small (1.5mmHg)

FINGER study
• FINnish Geriatric intervention study to prEvent cognitive impaiRment and disability (FINGER). CI Mia Kivipelto.
• 1260 people aged 60-77, not demented but high “risk score” (> 6)
Also 7y outcomeNgandu et al, Lancet 2015

FINGER study
Also 7y outcomeNgandu et al, Lancet 2015
OR NTB 1.35 (p=0.04)

Conclusions
• Current symptomatic treatments with modest benefit exist for
Alzheimer’s disease and Lewy body dementia only
• Search for disease modifiers has proved elusive – things that
cure Alzheimer’s in mice have not translated to man
• Pipeline remains strong, with studies moving earlier in disease and aimed at other targets (tau, inflammation)
• Argument that new targets are needed (Dementia Research
Institute)
• Preventative strategies likely need to start in or before mid-life
• Best evidence for controlling vascular risk and exercise; curry, red wine, Mediterranean diet and crosswords may help!

















