Current Current Treatments in Treatments in MDS; the MDS; the Scottish Scottish Perspective Perspective Dr Dominic Culligan Dr Dominic Culligan Aberdeen Royal Infirmary Aberdeen Royal Infirmary
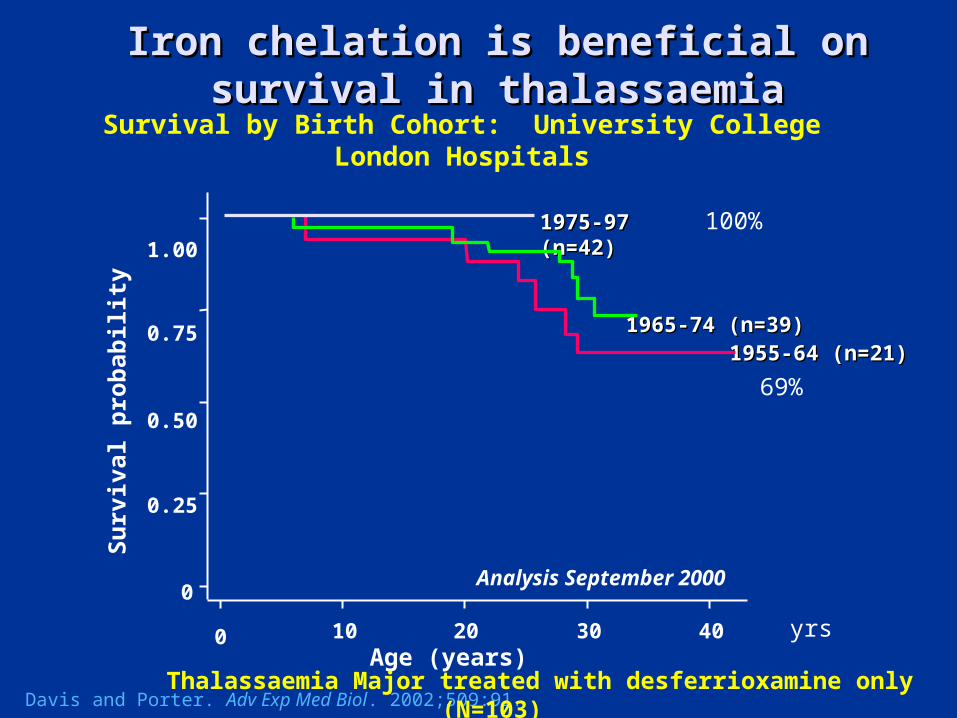
Thalassaemia Major treated with desferrioxamine only (N=103)
Survival by Birth Cohort: University College London Hospitals
69%
yrs
100%
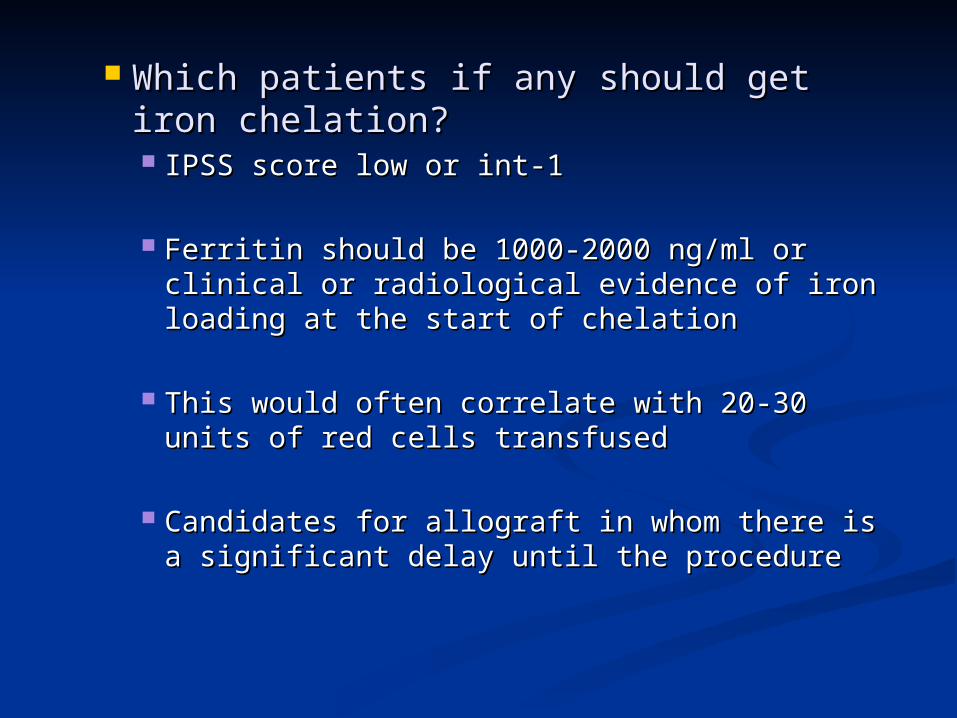
Which patients if any should get iron Which patients if any should get iron chelation?chelation? IPSS score low or int-1IPSS score low or int-1
Ferritin should be 1000-2000 ng/ml or clinical Ferritin should be 1000-2000 ng/ml or clinical or radiological evidence of iron loading at the or radiological evidence of iron loading at the start of chelationstart of chelation
This would often correlate with 20-30 units of This would often correlate with 20-30 units of red cells transfusedred cells transfused
Candidates for allograft in whom there is a Candidates for allograft in whom there is a significant delay until the proceduresignificant delay until the procedure
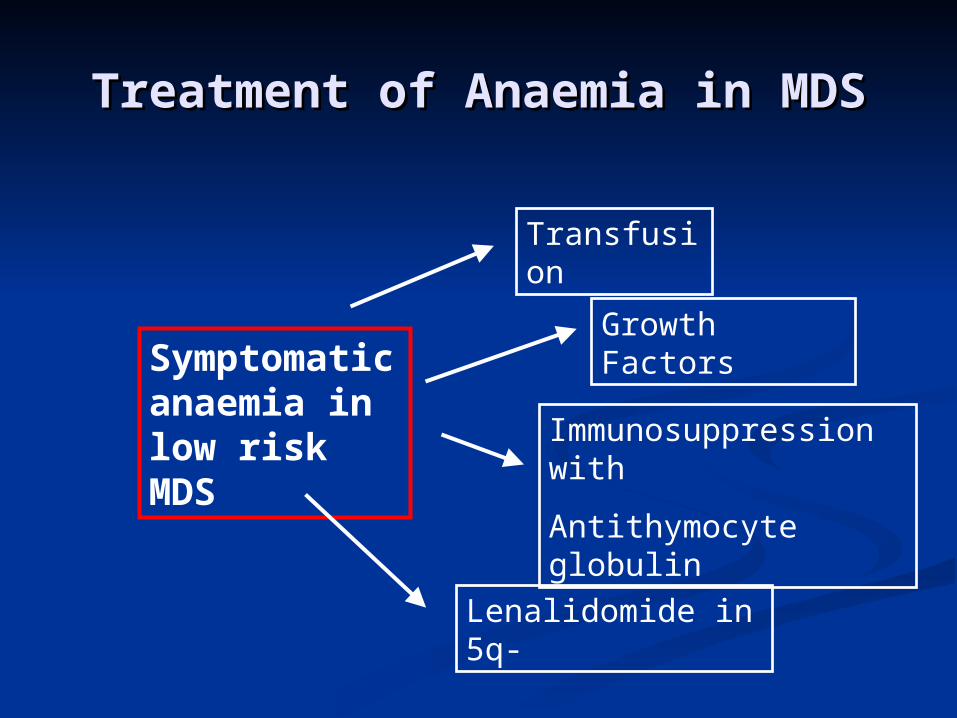
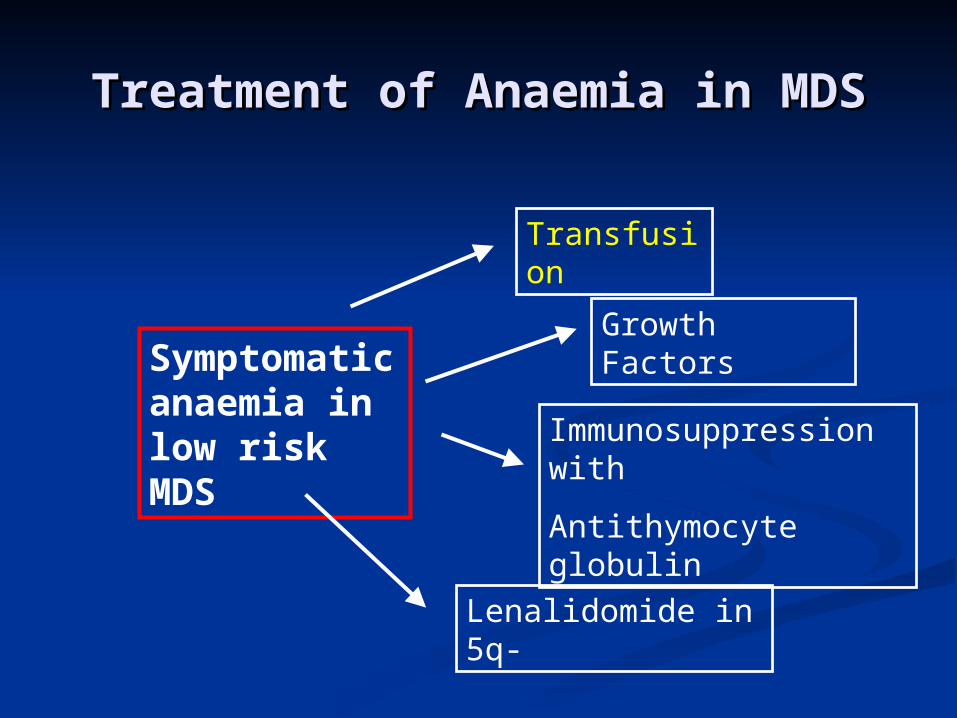
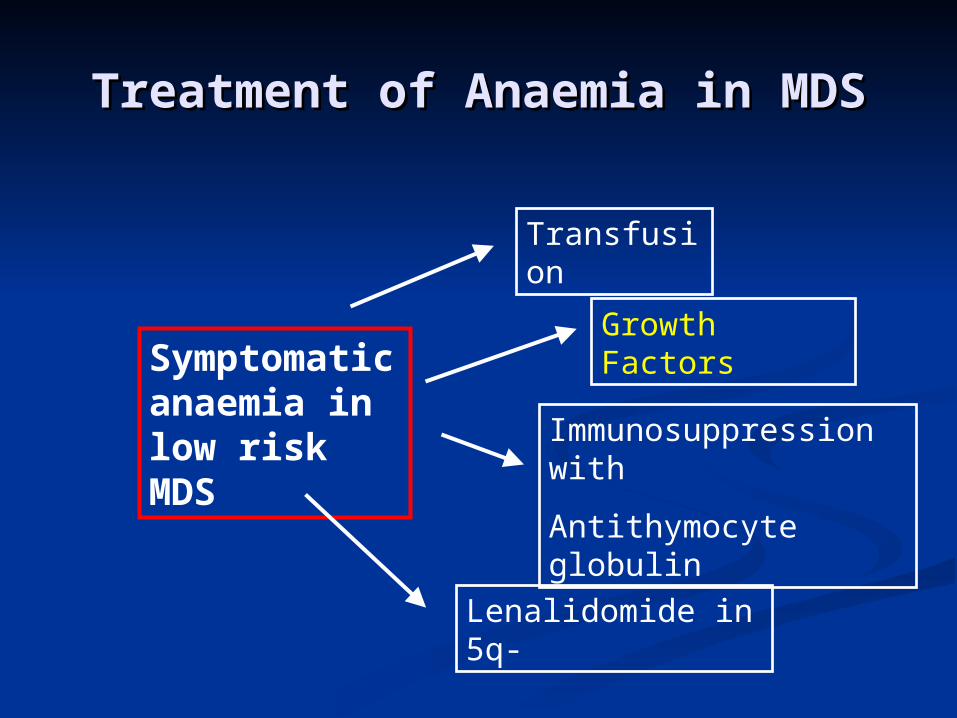
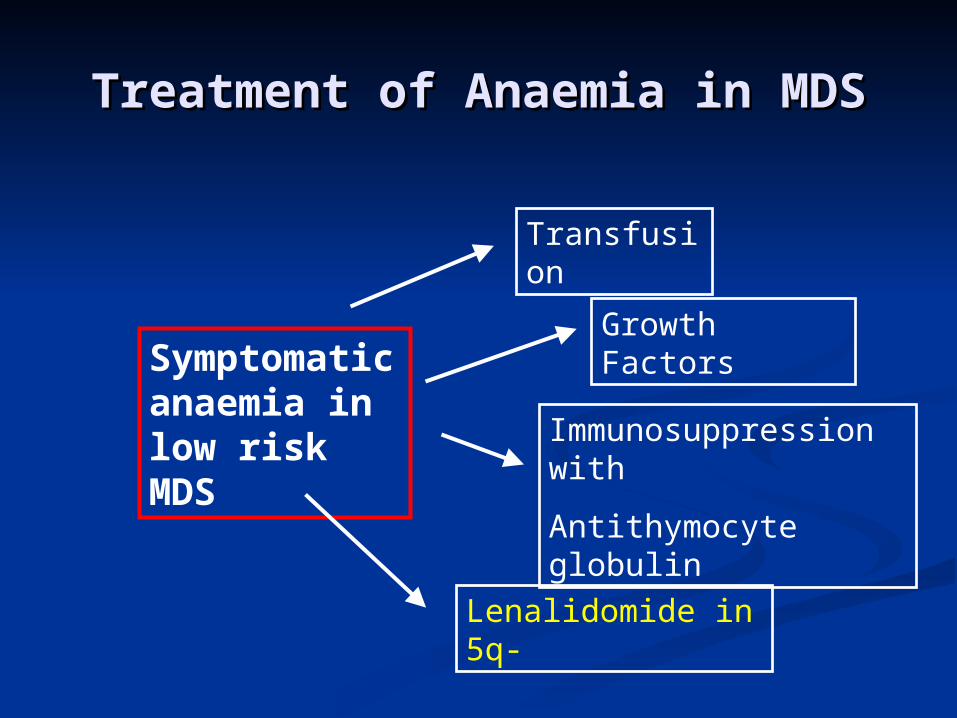
Treatment of Anaemia in MDSTreatment of Anaemia in MDS
Symptomatic anaemia in low risk MDS
Transfusion
Growth Factors
Immunosuppression with
Antithymocyte globulin
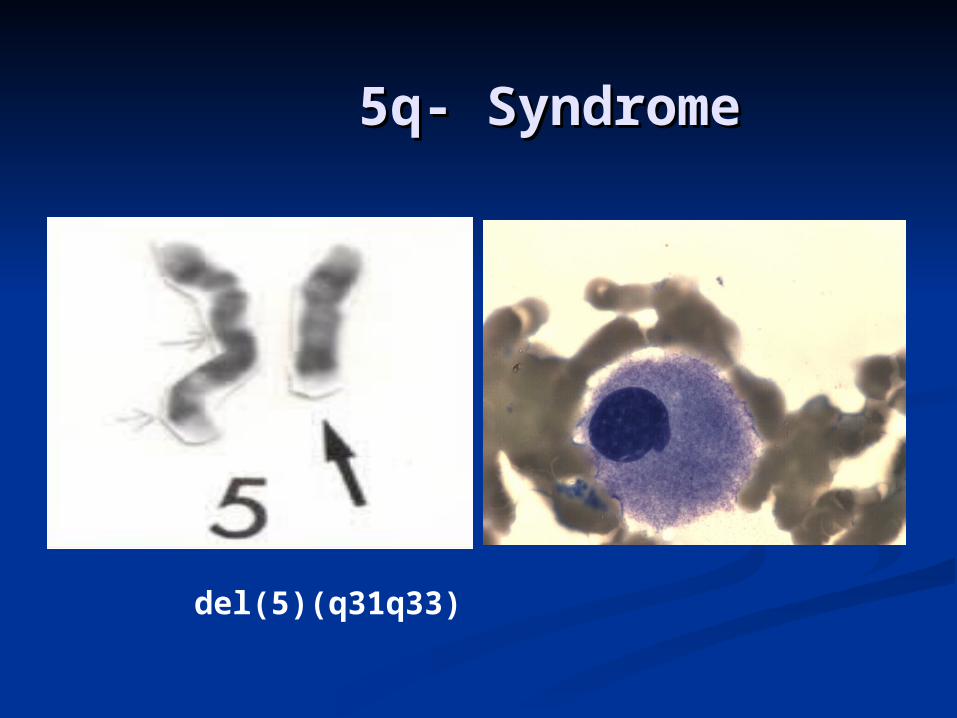
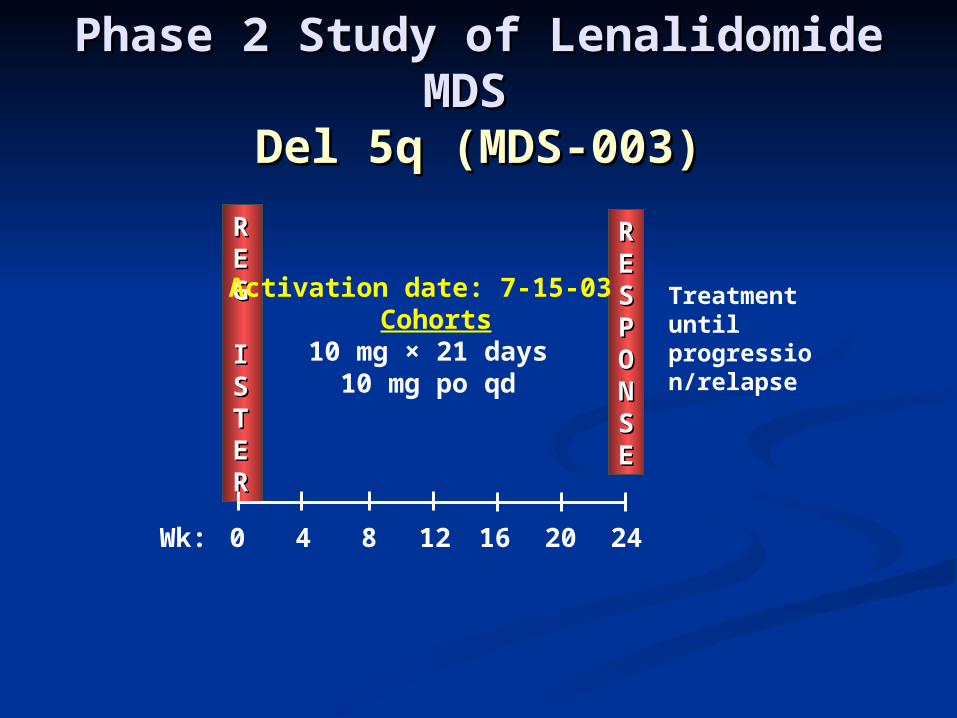
Lenalidomide in 5q-
20 Years experience of 20 Years experience of erythropoietin erythropoietin
Known three vessel coronary artery Known three vessel coronary artery diseasedisease 2 months more frequent angina2 months more frequent angina Increasing breathlessnessIncreasing breathlessness
Laboratory findingsLaboratory findings
FBC:FBC:
Hb Hb 9.1 g/dl;9.1 g/dl; MCV 96flMCV 96fl WCC WCC 2.6 x 102.6 x 1099/l/l NeutsNeuts 1.2 x 101.2 x 1099/l/l PlatsPlats 117 x 10117 x 1099/l/l
Refractory cytopenia with multilineage Refractory cytopenia with multilineage dysplasia (WHO)dysplasia (WHO)
Follow up visitFollow up visit
Cytogenetics failed:Cytogenetics failed:
Not keen on repeat bone marrowNot keen on repeat bone marrow
Hb 8.5 g/dlHb 8.5 g/dl
ManagementManagement
Jehovah’s Witness!Jehovah’s Witness!
Case 1 Question 2Case 1 Question 2
What would you recommend?What would you recommend?
1)1) Tell him not to be so daft and have a Tell him not to be so daft and have a blood transfusion?blood transfusion?
2)2) Tell his wife and daughter (not JWs) to Tell his wife and daughter (not JWs) to persuade him to have a blood persuade him to have a blood transfusion?transfusion?
3)3) Treat him with a trial of erythropoietic Treat him with a trial of erythropoietic stimulants (EPO, Darbopoietin)?stimulants (EPO, Darbopoietin)?
4)4) Try something else?Try something else?
Case 1 Answer 2Case 1 Answer 2
What would you recommend?What would you recommend?1)1) Tell him not to be so daft and have a Tell him not to be so daft and have a
blood transfusion?blood transfusion?
2)2) Tell his wife and daughter (not JWs) to Tell his wife and daughter (not JWs) to persuade him to have a blood persuade him to have a blood transfusion?transfusion?
3)3) Treat him with a trial of erythropoietic Treat him with a trial of erythropoietic stimulants (EPO, Darbopoietin)? (high stimulants (EPO, Darbopoietin)? (high predicted response)predicted response)
4)4) Try something else?Try something else?
Initial therapyInitial therapy
Erythropoietin 30,000u once per week Erythropoietin 30,000u once per week
x 6wksx 6wks Erythropoietin 30,000u once per week Erythropoietin 30,000u once per week
+ G-CSF 105ug three times per week+ G-CSF 105ug three times per week
x 6 weeksx 6 weeks Erythropoetin 60,000u +G-CSF 2 weeksErythropoetin 60,000u +G-CSF 2 weeks No response-steady deteriorationNo response-steady deterioration
March 2009March 2009
Wheelchair- boundWheelchair- bound Angina at rest despite maximum Angina at rest despite maximum
medical therapymedical therapy Hb 5.7g/dlHb 5.7g/dl Repeat bone marrow:Repeat bone marrow:
Gross dysplasia, no increase in blastsGross dysplasia, no increase in blasts Karyotype 46XY onlyKaryotype 46XY only IPSS intermediate-1IPSS intermediate-1
Case 1 Question 3Case 1 Question 3What would you opt for?What would you opt for?
1). Palliative care with no further 1). Palliative care with no further therapy?therapy?
2). Trial of azacitidine if approved?2). Trial of azacitidine if approved?
3). Trial of lenalidomide if approved?3). Trial of lenalidomide if approved?
4).4). Trial of anti-thymocyte globulin Trial of anti-thymocyte globulin (ATG)?(ATG)?
Case 1 Answer 3Case 1 Answer 3What would you opt for?What would you opt for?
1). Palliative care with no further 1). Palliative care with no further therapy?therapy?
2). Trial of azacitidine if approved?2). Trial of azacitidine if approved?
3). 3). Trial of lenalidomide if approved?Trial of lenalidomide if approved?
4).4). Trial of anti-thymocyte globulin Trial of anti-thymocyte globulin (ATG)?(ATG)?
Exceptional Circumstances GroupExceptional Circumstances Group
Approved trial of lenalidomide based on Approved trial of lenalidomide based on fulfilling local criteria for fulfilling local criteria for exceptionality:exceptionality:
‘‘Because of his religious beliefs he is Because of his religious beliefs he is unable to receive the standard unable to receive the standard therapy-blood transfusion’therapy-blood transfusion’
Case 1 continuedCase 1 continued
22/04/09 started first cycle 22/04/09 started first cycle lenalidomidelenalidomide 10mg od for 21 days out of 28 days10mg od for 21 days out of 28 days
12/05/09 GP phoned:12/05/09 GP phoned: Bedridden, home oxygen, not coming to Bedridden, home oxygen, not coming to
hospital again, no further treatmenthospital again, no further treatment Most recent Hb 4.3g/dlMost recent Hb 4.3g/dl
Here is the really Here is the really exceptional bit!exceptional bit!
22/09/09 FBC from GP!!!22/09/09 FBC from GP!!!
Hb 13.5 g/dlHb 13.5 g/dl WCC 6.6 x 10WCC 6.6 x 1099/l/l Neuts 3.8 x 10Neuts 3.8 x 1099/l/l Platelets 166 x 10Platelets 166 x 1099/l/l
Contacted GP-It is him and repeat FBC same!Contacted GP-It is him and repeat FBC same!
Continued on lenalidomide for two years with Continued on lenalidomide for two years with normal blood counts and no symptoms of anaemianormal blood counts and no symptoms of anaemia
Case 1 Case 1 What should you display in your What should you display in your
MDS clinic?MDS clinic?
Therapeutic OptionsTherapeutic Options
High Risk MDS – Main problems are bone High Risk MDS – Main problems are bone marrow marrow failure & leukaemiafailure & leukaemia
Supportive careSupportive care AzacitidineAzacitidine ChemotherapyChemotherapy Stem cell transplantationStem cell transplantation
AzacitidineAzacitidine
It has been suggested that It has been suggested that azacitidine may switch on important azacitidine may switch on important anti-cancer genesanti-cancer genes
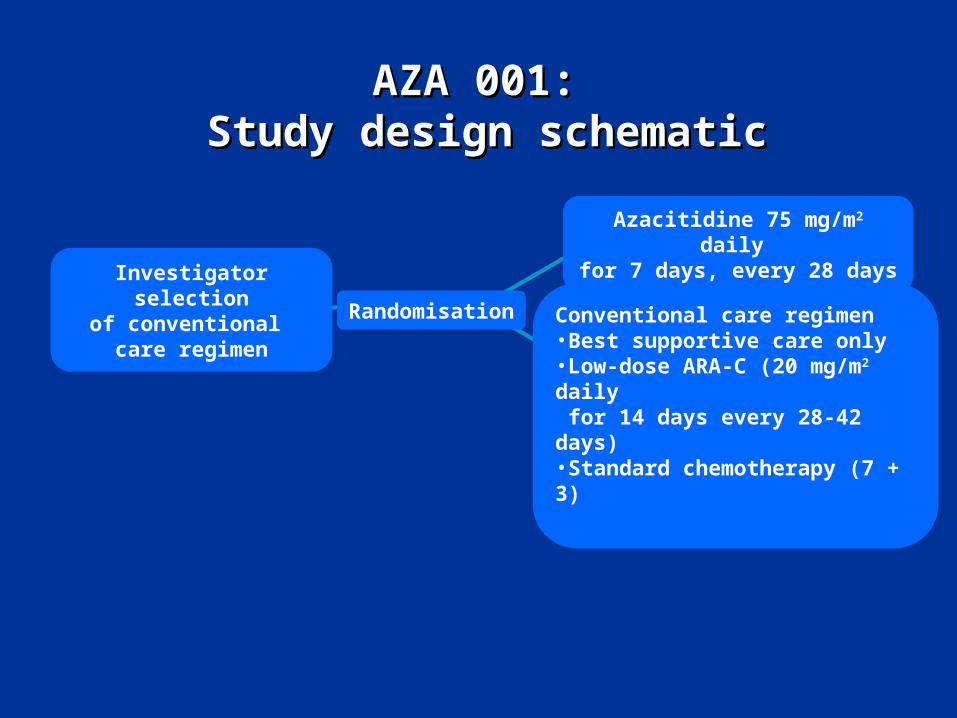
AZA 001:AZA 001: Study design schematicStudy design schematic
RandomisationInvestigator selection
of conventional care regimen
Azacitidine 75 mg/m2 daily for 7 days, every 28 days
Conventional care regimen•Best supportive care only•Low-dose ARA-C (20 mg/m2 daily for 14 days every 28-42 days)•Standard chemotherapy (7 + 3)
AZA-001: AZA-001: Vidaza is the only licensed drug that Vidaza is the only licensed drug that
has demonstrated a survival advantage has demonstrated a survival advantage in Int-2 and High-risk MDSin Int-2 and High-risk MDS
Vidaza – increases the median survival to 24.5 months (compared to 15 Vidaza – increases the median survival to 24.5 months (compared to 15 months with CCR) providing a months with CCR) providing a 9.4 month benefit9.4 month benefit
In a post hoc analysis Vidaza In a post hoc analysis Vidaza doubled 2-yeardoubled 2-year survivalsurvival rate compared with rate compared with CCR (p<0.001)CCR (p<0.001)
1. Fenaux P, et al. The Lancet Oncology 2009; 10: 200-01
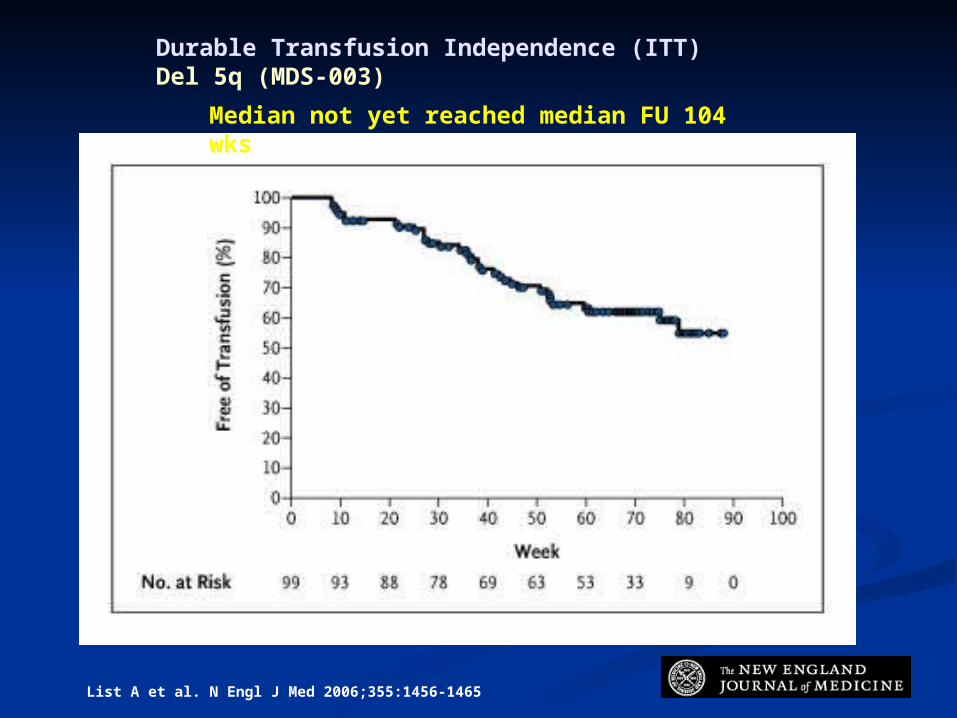
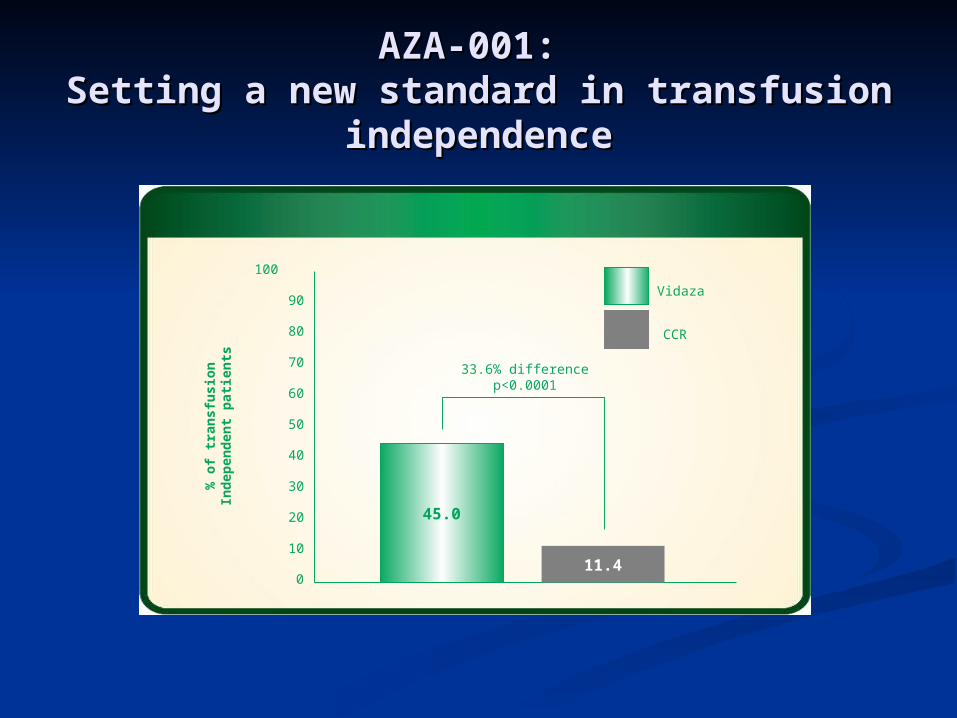
AZA-001: AZA-001: Setting a new standard in transfusion Setting a new standard in transfusion
independenceindependence
1. Santini V. J Clin Oncol 2008 2. Fenaux P, et al. The Lancet Oncology 2009; 10: 200-013. Vidaza SmPC December 2008.
100
80
60
40
20
0
% o
f tr
ansf
usi
on
Ind
epen
den
t p
atie
nts
90
70
50
30
10
45.0
11.4
33.6% differencep<0.0001
Vidaza
CCR
Azacitidine (Vidaza)Azacitidine (Vidaza)
Standard of care for high risk MDS Standard of care for high risk MDS patients who are not candidates for patients who are not candidates for transplantationtransplantation
Approved by NICE ( Approved by NICE ( great help of great help of UKMDS Patient Forum) UKMDS Patient Forum)
Not approved by SMCNot approved by SMC
The Scottish PerspectiveThe Scottish Perspective
The Scottish Medicines ConsortiumThe Scottish Medicines Consortium
Statutory body which is part of: Statutory body which is part of: Quality Improvement Scotland (QIS)Quality Improvement Scotland (QIS)
To advice the NHS in Scotland as to To advice the NHS in Scotland as to the cost effectiveness of new the cost effectiveness of new treatmentstreatments
SMC vs. NICESMC vs. NICE
SMC decisions only apply in ScotlandSMC decisions only apply in Scotland
NICE NICE single drugsingle drug decisions only apply decisions only apply in England, Wales and Northern in England, Wales and Northern IrelandIreland
NICE NICE multiple treatmentmultiple treatment assessments assessments apply in Scotland and replace any apply in Scotland and replace any existing SMC guidanceexisting SMC guidance
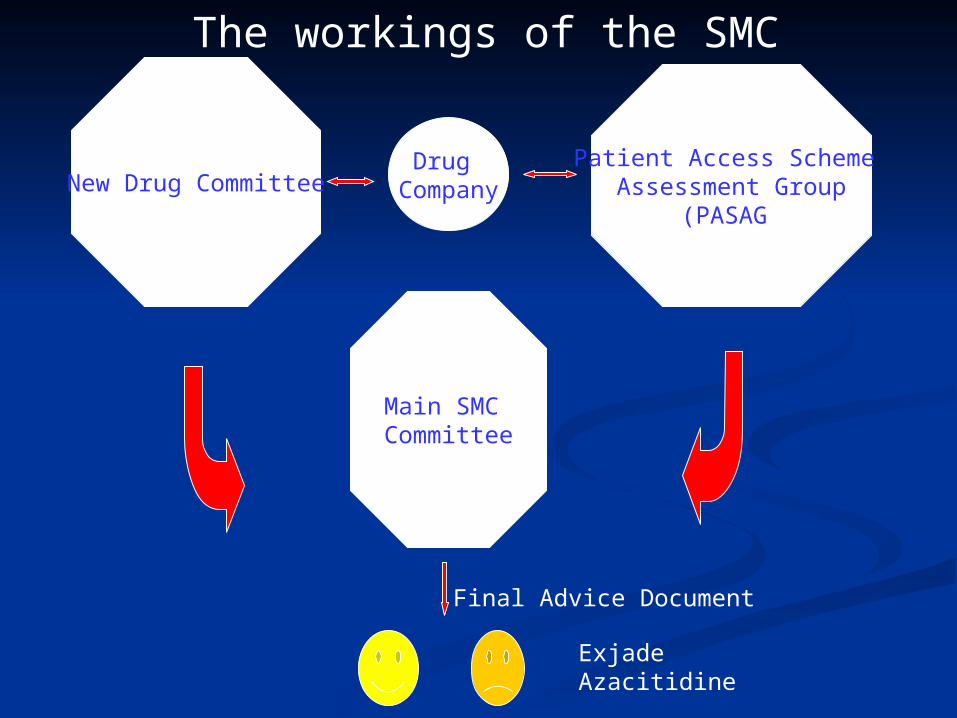
New Drug CommitteePatient Access Scheme
Assessment Group(PASAG)
Main SMC Committee
Final Advice Document
The workings of the SMC
ExjadeAzacitidine
Drug Company
What about stem What about stem cell cell
transplantation?transplantation?
Current transplant activity Current transplant activity in MDSin MDS
EBMT EBMT
2008:2008: 1147 allografts for MDS ~ 10% of total 1147 allografts for MDS ~ 10% of total
Bone MarrowBone Marrow Hypercellular-confirmed on trephineHypercellular-confirmed on trephine Trilineage dysplasiaTrilineage dysplasia Blasts 1%Blasts 1%