The clinical performance of dental composites has been significantly improved over the past decade through modificationsin formulation that include: using more stable polymerization promoters for greater color stability; incorporatinghigh concentrations of finely ground fillers to produce adequate strength and excellent wear resistance while retaining translucency;adding radiopacifying agents for improved diagnostics; and utilizing dentin adhesives. However, there are problemswhich limit the use of composites, especially in posterior teeth. The materials remain very technique-sensitive, due to theextensive contraction which accompanies polymerization and negatively influences marginal sealing. In addition, the materialsare generally considered to have inadequate mechanical properties and wear resistance in contact areas to serve as totalreplacements for amalgams. Current efforts are focusing on several areas, including the development of non- or minimallyshrinkingdental composites containing spiro-orthocarbonates as additives to dimethacrylates or epoxy-base resins, and theproduction of alternative filler materials for ideal wear resistance and esthetics. This paper reviews the composition and characteristicsof current dental composites, as well as recent areas of study.
18
http://cro.sagepub.com/ Critical Reviews in Oral Biology & Medicine http://cro.sagepub.com/content/6/4/302 The online version of this article can be found at: DOI: 10.1177/10454411950060040301 1995 6: 302 CROBM J.L. Ferracane Current Trends in Dental Composites Published by: http://www.sagepublications.com On behalf of: International and American Associations for Dental Research can be found at: Critical Reviews in Oral Biology & Medicine Additional services and information for http://cro.sagepub.com/cgi/alerts Email Alerts: http://cro.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Jan 1, 1995 Version of Record >> at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission. cro.sagepub.com Downloaded from at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission. cro.sagepub.com Downloaded from
Transcript
http://cro.sagepub.com/Critical Reviews in Oral Biology & Medicine
http://cro.sagepub.com/content/6/4/302The online version of this article can be found at:
DOI: 10.1177/10454411950060040301
1995 6: 302CROBMJ.L. Ferracane
Current Trends in Dental Composites
Published by:
http://www.sagepublications.com
On behalf of:
International and American Associations for Dental Research
can be found at:Critical Reviews in Oral Biology & MedicineAdditional services and information for
at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
J.L FerracaneDepartment of Biomaterials and Biomechanics, Oregon Health Sciences University, 611 S.W. Campus Drive, Portland, Oregon 97201-3097
ABSTRACT: The clinical performance of dental composites has been significantly improved over the past decade through mod-ifications in formulation that include: using more stable polymerization promoters for greater color stability; incorporatinghigh concentrations of finely ground fillers to produce adequate strength and excellent wear resistance while retaining translu-cency; adding radiopacifying agents for improved diagnostics; and utilizing dentin adhesives. However, there are problemswhich limit the use of composites, especially in posterior teeth. The materials remain very technique-sensitive, due to theextensive contraction which accompanies polymerization and negatively influences marginal sealing. In addition, the materi-als are generally considered to have inadequate mechanical properties and wear resistance in contact areas to serve as totalreplacements for amalgams. Current efforts are focusing on several areas, including the development of non- or minimally-shrinking dental composites containing spiro-orthocarbonates as additives to dimethacrylates or epoxy-base resins, and theproduction of alternative filler materials for ideal wear resistance and esthetics. This paper reviews the composition and char-acteristics of current dental composites, as well as recent areas of study.
"Composite" refers to a mixture. In materials science, acomposite is a mixture produced from at least two of thedifferent classes of materials, i.e., metals, ceramics, andpolymers. Dental composites are complex, tooth-coloredfilling materials composed of synthetic polymers, partic-ulate ceramic reinforcing fillers, molecules which pro-mote or modify the polymerization reaction that pro-duces the cross-linked polymer matrix from thedimethacrylate resin monomers, and silane couplingagents which bond the reinforcing fillers to the polymermatrix. Each component of the composite is critical tothe success of the final dental restoration. However, themost significant developments in the evolution of com-mercial composites to date have been a direct result ofmodifications to the filler component.
Dental composites have been considered acceptablerestorative materials for anterior applications for manyyears. Their tooth-matching ability and lack of metallicmercury have caused them to be promoted as an adjunctto or substitute for dental amalgam in the restoration ofthe posterior dentition. Though not universally acceptedby the profession, the continued "fine tuning" of com-posite formulations by dental manufacturers has pro-duced acceptable materials for more expanded use inthe posterior dentition. These alterations have mainlyinvolved the use of radiopaque glass fillers that are capa-
ble of being ground or formed into very fine particlesizes, thus enhancing the polishability and intra-oralabrasion resistance of the resultant composite.Favorable results from long-term clinical trials demon-strate that when placed correctly, composites can pro-duce esthetic posterior restorations with excellentlongevity (el-Mowafy et ai, 1994; Taylor et al, 1994).However, there remain significant problems that limitthe usefulness of these materials in the routine practiceof dentistry. Although one of the concerns relates to whatis perceived as a limited durability when the material isplaced in occlusal contact, the most significant problemsrelate to the excessive contraction accompanying intra-oral polymerization of composite. It is likely that thedevelopment of a new matrix polymer that undergoeszero or negligible curing contraction would be a majorstep toward solving the majority of the difficultiesinvolved in the use of dental composite.
This paper will present a summary of the composi-tion and characteristics of current dental composites.Each component of the composite will be discussed sep-arately, first by describing the state-of-the-art of presentmaterials as presented in the literature, and subsequent-ly by discussing recent and future areas of study. Themanner in which each component influences the use ofthe material and the outcome of the final restoration willbe discussed. Recent clinical and laboratory findingsidentifying the successes as well as the current problems
302 Crit Rev Oral Biol Med 6(4):302-318(1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
with composites will be highlighted and used to suggestfuture directions for research and development.
(II) FillersFillers are often used in the plastics industry to reducethe cost of a component, because the polymers are usu-ally the most expensive material in the part. Fillers arealso added to provide reinforcement, e.g., fiberglass.Fillers are used in dental composites to providestrengthening (Ferracane et ai, 1987; Chung and Greener,1990), increased stiffness (Braem et ai, 1989; Kim et ai,1994), reduced dimensional change when heated andcooled (Soderholm, 1984; Yamaguchi et ai, 1989),reduced setting contraction (Munksgaard et ai, 1987; Igaetai, 1991), radiopacity (van Dijkenetfl!., 1989), enhancedesthetics, and improved handling. In general, the physi-cal and mechanical properties of the composite areimproved in direct relation to the amount of filler added.A variety of ceramic filler materials has been utilized, butthe selection is limited by several factors.
One of the most important considerations in theselection of a filler is the optical characteristics of thecomposite. The monomer resins used in dental compos-ites have a refractive index of approximately 1.55. Fillerswith refractive indices which differ greatly from this valuewill cause the composite to appear optically opaque, cre-ating an esthetic and curing problem. Because glassescan have refractive indices ranging from 1.4 to 1.9, theselection of an appropriate filler for dental compositesmust be guided by a consideration of this importantvariable.
(A) PRESENT MATERIALS
Initially, fused or crystalline quartz and various borosili-cate or lithium aluminosilicate glasses were used asfillers for dental composites. The glass or quartz wasground or milled into particles of various sizes, rangingfrom approximately 0.1 |nm to 100 |xm (Phillips, 1991).These particles were added to resin monomer at approx-imately 70-80 wt% (55-65 vol%) to make a paste thatcould be hardened into a dental restorative material withstrength and stiffness far surpassing those of the unfilledpolymer itself. The major advantage to using quartz wasthat it is readily available and has an excellent opticalmatch to the polymer resin. However, quartz has draw-backs in that it is not radiopaque and can be very abra-sive to enamel. Another drawback to the original quartzand glass fillers were that the particles were large andvery hard in relation to the surrounding polymer matrix.These characteristics ensured that as the surface of thecomposite was abraded, the polymer would wear awaymore quickly than the fillers, leaving them raised andexposed from the surface. This made the surface of therestoration rough and less enamel-like, due to apprecia-ble scattering of incident light Thus, polishability and
esthetics were compromised.Microfills, containing amorphous silica, were devel-
oped to address the polishing requirements of anteriorrestorations. These silicon dioxide particles are sub-microscopic, averaging approximately 0.04 (urn in diame-ter, though the size varies among materials. The amor-phous silica is incorporated alone and as pre-polymer-ized resin fillers and agglomerates. The latter are neces-sary to increase the volume of filler particles in the com-posite. The small particles have a large surface-area-to-volume ratio, thus requiring considerable amount ofmonomer to wet their surface in order to produce ahomogeneous, non-sticky composite paste. This charac-teristic limits the filler concentration to approximately 35wt%, which in turn limits the strength and stiffness of thematerial. In order to circumvent these limitations par-tially and enhance filler reinforcement, a manufacturingtechnique was developed to produce heavily filled poly-mer resin blocks that can be milled into particles approx-imately 25 |im in size. When these pre-polymerized resinfillers are added to the resin with additional amorphoussilica, pastes with filler levels of 50-60 wt% (35-45 vol%)are possible. The small size of the particles allowed thesecomposites to be polished without preferential abrasion,thus producing smooth surfaces and excellent esthetics.However, these fillers, like quartz, are not radiopaque.Recently, radiopacity has been achieved in microfills bythe addition of small concentrations of other fillers, suchas Ytterbium trifluoride (Heliomolar RO, Ivoclar). The netresult for the microfills is excellent esthetics and pol-ishability, but strength and stiffness lower than those ofquartz-filled or glass-filled composites that contain larg-er particles. The poorer mechanical properties are attrib-uted to the use of a lower concentration of fillers in themicrofills.
Most current composites are filled with radiopaquesilicate particles based on oxides of barium, strontium,zinc, aluminum, or zirconium (Hosoda et ai, 1990; Khanet ai, 1992). The glasses are milled by special processesto produce particulates of very small size. Many currentmaterials include few particles which equal or exceed 3-5 Jim in size, and most have average particle sizes ofapproximately 0.6-1.0 |um. Some of the composites havea very uniform distribution of small filler sizes, while oth-ers utilize a broader distribution of particles. These com-posites also contain a small amount of amorphous silicamicrofiller to improve handling characteristics andreduce stickiness.
There has not been a definitive study to prove thesuperiority of any specific filler. Several studies haveidentified and evaluated the elements leached from den-tal composites aged in vitro and have verified that theradiopaque glasses containing zinc, barium, and stron-tium are more soluble than quartz or silica in aqueoussolutions (Soderholm et ai, 1984; 0ysaed and Ruyter,
6(41:302-318(1995) Crit Rev Oral Bio! Med 303 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 1. Scanning electron micrograph of the polished surfaceofa microfill composite, Heliomolar RO, showing a very smoothsurface and the presence of the pre-polymerized resin fillers.
Figure 2. Scanning electron micrograph of the polished surfaceor a mini-filled composite, Herculite XRV, showing a relativelysmooth surface dominated by irregularly shaped particles of lessthan 1.0-|im size and few particles greater than 2 ^m.
1986; Soderholm, 1990). The quantities of elementsleached are very low (ppm levels), and the main concernhas been related to the possibility that the filler/matrixinterface may become hydrolytically unstable due to thesolubility of the fillers, leading to a more rapid erosion ofthe composite. No clinical evidence exists to supportthis concern. However, a composite has been developedin Japan specifically with this thought in mind. Graft LCII (GC Corp.) contains glass filler particles treated with amonomer to graft methacrylate groups covalently to thefiller surface, thus enhancing the filler/matrix interfacialstrength and its hydrophobicity (G-C product literature;Tani, 1993).
As previously stated, the most significant changes incommercial composites have been made through alter-ing the filler component. These changes have promptedthe periodic development of classification systems fordental composites based upon filler size and volumefraction. In 1983, Lutzand Phillips published a system forcharacterizing dental composites based on particle size.Their system included traditional composites (avg. parti-cle size = 1-15 urn), hybrids containing a mixture ofground glass and microfill particles (avg. particle sizes =5 nm and 0.04 |j.m, respectively), and microfills (avg. par-ticle size = 0.04-0.1 um). The microfills were divided intosubclasses which included a characterization of the typeof pre-polymerized resin fillers incorporated, i.e., splin-tered, agglomerated, or spherical.
Recently, Willems et al. (1992) published a similarclassification system. The basic difference between thetwo reflects the fact that the most popular non-microfillcomposites have smaller mean particle sizes and fewerlarge particles than composites of a decade ago. The
term "hybrid" is no longer used, since nearly all dentalcomposites are now "hybrids" of two size ranges, becausethey contain some amorphous silica to improve handlingby reducing stickiness. Instead, composites are classifiedas midway-filled (< 60 vol%) and compact-filled (> 60vol%), with classifications of ultrafine (avg. size < 3 urn)and fine (avg. size > 3 |im) within each category. The cat-egories of microfill composites remain virtuallyunchanged, though new materials are included which arepredominantly filled with amorphous silica but also con-tain some macroscopic reinforcing fillers or radiopaci-fiers. Also, fiber-reinforced materials are classified in thenew system.
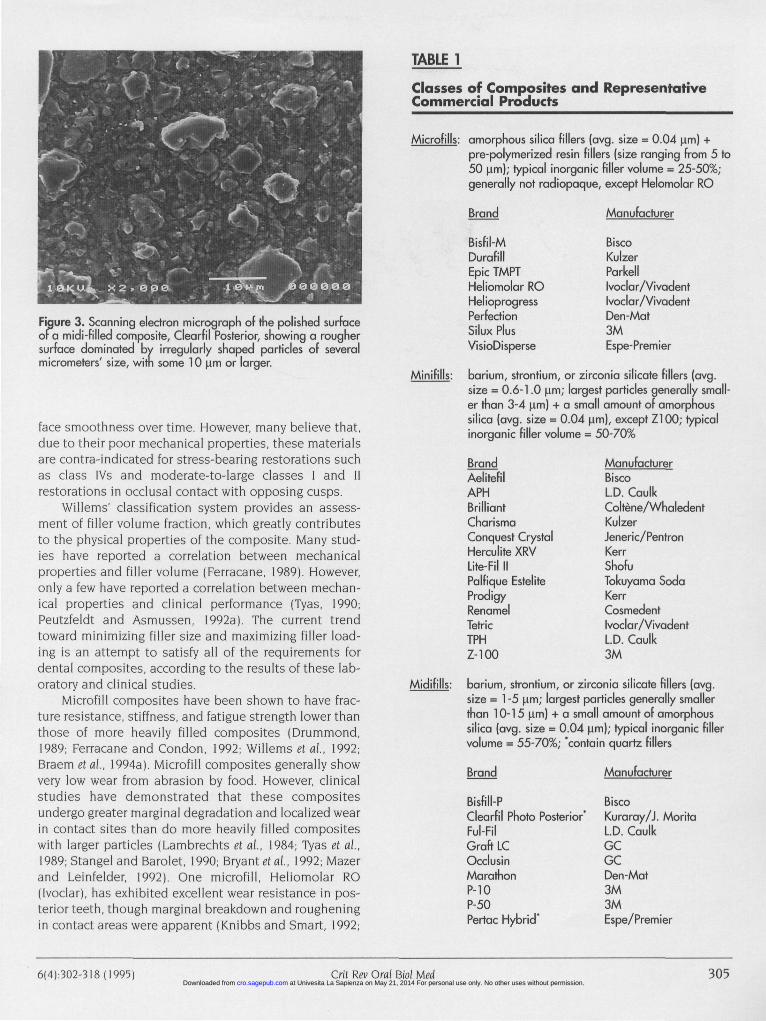
A simpler classification system has been describedby Bayne et al. (1994). In this system, the three populartypes of composites are described by the size of theirlargest fillers as microfills (average particle size = 0.01-0.1 \im), minifills (average particle size = 0.1-1.0 urn), andmidifills (average particle size = 1.0-10.0 urn). Scanningelectron micrographs of the polished surfaces of repre-sentative composites in each class demonstrate the dif-ferences in particle size and surface smoothness (Figs. 1-3). This classification system is less inclusive than previ-ous ones, but provides necessary information about thelargest added particles which significantly affect polisha-bility. Therefore, the two most important filler considera-tions at present are the amount and size of the particles.A listing of commercial products from the three differentclasses of composites is presented in Table 1.
The generally accepted view is that microfill com-posites have the most ideal esthetic qualities, due totheir excellent polishability and capacity to retain sur-
304 Crit Rev Oral Bid Med 6(4):302-3I8 (1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 3. Scanning electron micrograph of the polished surfaceofa midi-filled composite, Clearfil Posterior, showing a roughersurface dominated by irregularly shaped particles of severalmicrometers' size, witn some 10 u,m or larger.
face smoothness over time. However, many believe that,due to their poor mechanical properties, these materialsare contra-indicated for stress-bearing restorations suchas class lVs and moderate-to-large classes I and lirestorations in occlusal contact with opposing cusps.
Willems' classification system provides an assess-ment of filler volume fraction, which greatly contributesto the physical properties of the composite. Many stud-ies have reported a correlation between mechanicalproperties and filler volume (Ferracane, 1989). However,only a few have reported a correlation between mechan-ical properties and clinical performance (Tyas, 1990;Peutzfeldt and Asmussen, 1992a). The current trendtoward minimizing filler size and maximizing filler load-ing is an attempt to satisfy all of the requirements fordental composites, according to the results of these lab-oratory and clinical studies.
Microfill composites have been shown to have frac-ture resistance, stiffness, and fatigue strength lower thanthose of more heavily filled composites (Drummond,1989; Ferracane and Condon, 1992; Willems et al, 1992;Braem et al, 1994a). Microfill composites generally showvery low wear from abrasion by food. However, clinicalstudies have demonstrated that these compositesundergo greater marginal degradation and localized wearin contact sites than do more heavily filled compositeswith larger particles (Lambrechts et al., 1984; Tyas et al.,1989; Stangel and Barolet, 1990; Bryant etai, 1992; Mazerand Leinfelder, 1992). One microfill, Heliomolar RO(Ivoclar), has exhibited excellent wear resistance in pos-terior teeth, though marginal breakdown and rougheningin contact areas were apparent (Knibbs and Smart, 1992;
TABLE 1
Classes of Composites and RepresentativeCommercial Products
barium, strontium, or zirconia silicate fillers (avg.size = 0.6-1.0 u.m; largest particles generally small-er than 3-4 u.m) + a small amount of amorphoussilica (avg. size = 0.04 (am), except Z100; typicalinorganic filler volume = 50-70%
6(4):302-318 (1995) Crit Rev Oral Bio! Med 305 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 4. Scanning electron micrograph of the fracture surfaces of two microfill composites: (a) Silux Plus, showing a rough texture withmany debonded and plucked pre-polymerized resin fillers; and (b) Epic TMPT, showing a smoother texture with cleaved pre-polymerizedresin fillers due to the enhanced bonding with the matrix.
Mazer and Leinfelder, 1992). Another microfill, Silux (3MDental Products), has also shown excellent abrasionresistance after five years, but experienced an incidenceof fracture higher than that of more heavily filled materi-als (Tyas and Wassenaar, 1991). A current hypothesis isthat inadequate fatigue resistance is responsible for theaccelerated occlusal contact wear and marginal degrada-tion observed in composites with filler particles thataverage less than 1.0 u.m in size (Mazer et al, 1992; Braemetai, 1994b).
A factor contributing to the degradation of themicrofill composites is the fact that the pre-polymerizedresin fillers are not bonded well to the polymer matrix.The resin fillers are heat-cured and do not form covalentchemical bonds with the polymerizing matrix, due to thelack of available methacrylate groups on their surfaces.Therefore, they become debonded and dislodged underhigh stresses. A relatively new microfill composite wasdeveloped to minimize this problem by enhancing thebond between the matrix and the organic fillers. EpicTMPT (Sun Medical, Japan, and Parkell, USA) uses a typ-ical urethane dimethacrylate in conjunction with a newmonomer, trimethylol propane trimethacrylate (TMPT),to make the organic fillers. As will be discussed shortly,the greater availability of reactive species on the organicfiller due to the TMPT theoretically enhances the chemi-cal reaction between the matrix polymer and the filler.The resultant material is reported to be a highly wear-resistant microfill which is also resistant to marginaldegradation when tested in vitro (Suzuki and Leinfelder,1994). A comparison of scanning electron micrographs ofthe fracture surfaces of a conventional microfill (Silux,3M) and Epic TMPT reveals a difference in bonding, asdepicted by the high proportion of pre-polymerized resin
fillers debonded or protruding from the surface of theconventional microfill (Figs. 4a-b).
The wear of composites in the oral environment isprimarily related to filler particle size and interparticlespacing (Bayne et al, 1992). Because the matrix is softerand less wear-resistant than the inorganic filler, it is pref-erentially abraded by food, toothpaste, etc. As the poly-mer matrix wears down, it exposes the filler particles,allowing them to be plucked from the surrounding matrixduring the next abrasion cycle. The use of smaller parti-cles minimizes the space between particles and theextent of filler plucking and surface degradation duringchewing, thus reducing the rate of abrasive wear. Clinicalstudies of reasonable duration, i.e., five years or more,have confirmed the success of many composites in smallto moderate posterior occlusal cavities, showing wearrates in contact-free areas of 10-20 urn or less per yearwhen the average particle size is less than 1.0 urn (Bayneetai, 1991; Wilson etai, 1991; Mazer and Leinfelder, 1992;Wendt and Leinfelder, 1994; Leinfelder, 1995). Theseresults have fueled the further development of very heav-ily filled small-particle composites, and several new sys-tems have emerged.
One such material is Z100 (3M Dental Products),which uses zirconia silica fillers produced by a syntheticsol-gel process instead of particles made from minedminerals or melted glasses (Fig. 5). The sol-gel process isone in which a metal carboxylate and a metal oxide solare mixed and form a gel by dehydration. The gel is heat-treated and then ground to produce the fillers. A similartechnology is utilized to make Palfique Estelite(Tokuyama Soda), which contains spherical silica zirco-nia fillers with a particle size of 0.2-0.3 Jim (Tani, 1993).This composite is the improved version of Palfique intro-
306 Crit Rev Oral Bid Med 6(4):302-318 (1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 5. Scanning electron micrograph of the polished surfaceofZlOO showing a relatively smooth surface dominated byspherically shaped fillers with an average size of less than 1.0mm and few particles larger than 3-4 mm.
duced in 1983 (Tani, 1983). Though a similar filler wasused in its predecessor, P-50 (developed in 1988), thefillers in Z100 are ground differently to produce roundedparticles in a wide distribution of very small sizes (aver-age = 0.5-0.7 u,m; largest particles = 4 u,m). This obviatesthe need to add amorphous silica to improve handling.The composite is very dense (65-70 vol% fillers) and hasgood strength, handling, and abrasion resistance. Thegood abrasion resistance and polishability are believedto be due in part to the spherical nature of the fillers. Atleast one other composite developed in japan, Progress(Kanebo), also consists of a very high concentration (75vol%) of spherical fillers which are graded at two sizes(1.5 u,m and 0.1-0.5 urn). The high filler loading can beachieved only by having a non-uniform distribution ofparticles.
Another relatively recent addition to the compositemarket is Tetric (lvoclar). The novelty of this composite isthat it contains four different types of fillers. Bariumglass is used to achieve radiopacity and is combined withspheroidal silica particles, amorphous silica forimproved handling, and ytterbium trifluoride for itspotential therapeutic effects. Studies have confirmedthat fluoride is released from one fluoride-containingcomposite, Heliomolar RO (Arends and Ruben, 1988),but that the amount is two orders of magnitude lowerthan that leaching from glass-ionomer restoratives(Takahashi et al, 1993). Thus, the potential therapeuticeffects of the fluoride released from these compositesare questionable. The maximum particle size of Tetric isapproximately 3 u.m. The properties of this material arecomparable with those of Z100 and other ultrafine com-
posites, such as Brilliant D.I. (Coltene/Whaledent),Charisma (Kulzer), Herculite XRV (Kerr), and Prisma TPH(L.D. Caulk). The average particle size for most of thesecomposites is 0.6-0.8 \im. Recent studies suggest thatthese composites are all very wear-resistant, averagingapproximately 10-20 u.m/year due to abrasion(Leinfelder, 1995). In addition, all can be used as heat-treated inlays to enhance marginal sealing.
Perhaps the most wear-resistant compositedesigned for posterior applications is ClearfilPhotoposterior (Kuraray, Japan) (Wendt and Leinfelder,1992). This composite contains a high level (71 vol%) ofquartz fillers of approximately 3 u.m average size (Fig. 3).It also contains some particles which equal and exceed10 u,m. The material has excellent mechanical properties(Willems et al, 1992), though it is difficult to polish assmoothly as other small-particle composites due to thelarge fillers. In addition, because quartz is a very abrasivematerial, this composite has the potential to wearopposing dentition at a more rapid rate than other soft-er glasses. It is possible that the low abrasion wear forthis material is slightly misleading, in that it may bewearing the opposing teeth at the same time, thus mini-mizing its own loss.
This review of current composites emphasizes thatthe best mechanical properties are achieved by theincorporation of high concentrations of filler particles ofvarious sizes into the resin. The packing of particles isimproved by the use of a non-uniform size distribution(i.e., Clearfil and Z100), and this results in greater fillerdensity and maximum reinforcement. Though thesematerials, many of which are characterized as midifills,are acceptable for posterior use, they are less appropri-ate for anterior restorations, where esthetics and pol-ishability are of the utmost importance. The microfillshave the most ideal esthetics, and should be used inanterior restorations where stresses are low. Theminifills, which are also highly polishable, can be used inanterior teeth when greater strength is required due tomoderate occlusal loading. Thus, there is no ideal com-posite restorative, though the minifills may come theclosest to reaching this goal.
(B) RECENT AREAS OF STUDY
With the possible exception of the microfills, virtuallyany dental composite may prove to be abrasive to enam-el. The development of fillers that are softer than currentglasses would be clinically beneficial because theyshould be less abrasive to opposing teeth. This is espe-cially important when multiple restorations are placed inan arch. Calcium metaphosphate (CMP) ceramics offerone potential filler material that meets this criterion. Themajor advantage to the use of the CMPs is a softer sur-face texture as a result of their less brittle nature. Manycalcium phosphate ceramics have been tried as fillers for
6(4):302-318 (1995) Crit Rev Oral Biol Med 307 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
composites, but their use has been seriously limited bya high refractive index. Recently, Antonucci et al. (1991)prepared calcium metaphosphates with improved refrac-tive indices. These minerals exist in vitreous as well ascrystalline form. Composites made from the ground vit-reous CMP in Bis-GMA absorbed substantial amounts ofwater and were very weak. The crystalline form of themineral produced better composites, but they were stillconsiderably weaker than commercial materials, possi-bly due to the difficulty in coupling the CMP to the resinmatrix with silane-coupling agents.
As will be described, polymerization contraction andits accompanying stresses are among the biggest prob-lems facing the expanded use of composites. Becausethe polymerization of the resin monomers causes thecontraction, it is obvious that maximizing the quantity ofthe inert filler and thus minimizing the quantity of theresin results in less shrinkage during curing (Iga et al,1991). This provides a driving force for maximizing fillerlevels in composites. However, modifications of the fillermay also affect the amount of contraction and itsaccompanying stress. In a recent study, polymerizationcontraction stress in composites was reduced throughthe addition of 1 wt% of small (1 (im) hollow plasticspheres which provide sites for stress relief during curing(Li et al, 1993). Contraction stress could be reduced tonear zero with only a minimal reduction (i.e., 10%) inmechanical properties. There has apparently been nocommercial application of this idea to date. Also, it islikely that the hollow spheres would have a negativeeffect on the optical characteristics of the composite.
An alternative to conventional composites has beendeveloped (Bowen et al, 1991). "Megafilled" compositerestorations are produced by filling the bulk of the cavitypreparation with beta-quartz glass inserts (LeePharmaceuticals). The inserts are surrounded by light-cured composite, which bonds to the insert via a silane-coupling agent. The inserts are produced in a variety ofshapes and sizes to fit most cavity preps. When fittedinto the cavity, they minimize the volume of shrinkingcomposite and reduce curing contraction (George andRichards, 1993). One recent in vitro study showed thewear of a beta-quartz restoration to be similar to that ofP-50 or Herculite XR (Kawai and Leinfelder, 1993).
Other recent studies have utilized glass fibers asreinforcing fillers for composites, showing improvementsin fracture toughness and wear resistance (Li et al, 1993).At least one commercial composite (Restolux SP4, LeePharmaceuticals) makes use of fiber reinforcement,though polishability and abrasion resistance wouldseem to be less than ideal for such materials.
The future in filler technology probably lies in theexpanded use of sol-gel processing of particles for com-posites with excellent radiopacity (Suzuki et al, 1991) andabrasion resistance (Seghietal, 1993). The ability to pro-
duce particles of even smaller than current sizes wouldbe a great advantage, because it would allow manufac-turers to produce higher levels of filler loading throughmore efficient packing. One consideration is the use ofnanofillers, particles anywhere from 1 to 100 nm in size(Dagani, 1992; Bayne et al, 1994). It is likely that newcomposites will be formulated with some proportion offillers below 50 nm in size, though there are technical dif-ficulties in producing such materials with appropriatehandling characteristics.
It is also reasonable to assume that a greateremphasis will be placed on the use of fluoride-contain-ing inorganic materials as fillers. As mentioned, ytter-bium fluoride is used in several products (i.e., HeliomolarRO, Helioprogress, and Tetric from Ivoclar), and substan-tial fluoride has been shown to be released from thesematerials for up to five years (Arends and Ruben, 1988).A recent study examining in situ demineralization and flu-oride release from these composites demonstrated thatenamel demineralization decreased as fluoride releaseincreased (Dijkman et al, 1993). By extrapolation of thedata, the authors predicted that a composite thatreleased 200-300 |iig/cm2 fluoride over a one-month peri-od would completely inhibit secondary caries underplaque conditions. This amount is approximately 40-50times as much as that released by Heliomolar RO.Therefore, despite the fact that these fluoridated com-posites release significant amounts of fluoride, their pre-sent ability to prevent secondary caries is questionable,and improvements in technology will be required toincrease the level of fluoride release. Dijkman et al. (1993)showed that a composite with a fluoro-aluminum silicatefiller released an order of magnitude more fluoride thanHeliomolar, and that the fluoride release rate increasedin a linear manner with time. This was hypothesized tobe due to the greater water solubility of the silicate fillerin comparison with ytterbium fluoride. Though this mayenhance fluoride release, a filler with dramaticallyincreased water solubility may eventually compromisethe properties of the composite in the oral environment.
(Ill) Resin MonomersThe hardening of a dental composite is the result of achemical reaction between dimethacylate resinmonomers that produces a rigid and heavily cross-linkedpolymer network surrounding the inert filler particles.The extent of this reaction, often called the degree ofcure, is very important in that it dictates many of thephysical and mechanical properties of the compositerestoration. The degree of cure is influenced by many fac-tors, including the addition of polymerization promotersand inhibitors (Yoshida and Greener, 1994), the chemicalstructure of the monomers (Ferracane and Greener, 1986;Beatty et al, 1993), the chemical or light energy impartedto activate the reaction (Rueggeberg and Jordan, 1993),
308 Crit Rev Oral Biol Med 6(4):302-318(1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
the filler composition of the material(Kawaguchi et al, 1994), and the shade ofthe composite.
Accompanying the polymerizationreaction is a dimensional change thatresults in shrinkage. Shrinkage is causedby the monomers becoming covalentlybonded by the polymerization reaction,thus exchanging van der Waals' distancesfor covalent bond distances. The magni-tude of the shrinkage is dictated by thenumber of covalent bonds that form, i.e.,the extent of the reaction, as well as by thesizes of the monomers. Therefore, the goalof achieving maximum curing reaction toenhance the properties of the polymermatrix is at odds with the desire to mini-mize dimensional change, the latter beingnecessary for achieving good marginal integrity of therestoration. One method to counteract this problem is touse monomers of very large molecular weight, thus min-imizing the contraction per given volume of material.
The monomer originally developed for dental com-posites approximately 25 years ago, Bis-GMA, is stillused in most products today. Though new resins havebeen developed which claim to be less hydrophilic,tougher, or have less dimensional change than Bis-GMA,there is little evidence that the clinical performance ofcomposites has been dramatically affected by differencesin resin composition. Because the polymerization con-traction is the most significant problem with currentdental composite, it is highly desirable to develop a newor modified resin system that does not result in a netshrinkage during curing. This is currently an area ofintense research.
(A) PRESENT MATERIALS
As has been true for the past 30 years, 80-90% of com-mercial dental composites utilize the Bis-GMA (2.2-b i s ( 4 - ( 2 - h y d r o x y - 3 - m e t h a c r y l o y l o x y -propoxy)phenyl]propane) monomer developed by Dr.Rafael Bowen as their matrix-forming resin (Ruyter andOysaed, 1987). Other base monomers used in presentcommercial composites include: urethane dimethacry-lates (UDMA), with or without Bis-GMA (used in Ivoclarproducts like Helionnolar, Helioprogress, andTetric); ure-thane tetramethacrylate (UTMA) (used in Kuraray prod-ucts like Clearfil Photoposterior); bis(methacryloyloxy-methyl)tricyclodecane (used in ESPE-Premier productslike Pertac Hybrid); ethoxylated bisphenol-A-dimethacry-late (BisEMA); and a linear polyurethane made from Bis-GMA and hexamethylenediisocyanate (used in L.D.Caulk products like Prisma APH and TPH) (Ruyter, 1988;Tani, 1993). The chemical structure of many of thesemonomers is shown in Table 2. Due to their lower vis-
TABLE 2
Chemical Structure of Monomers Used in Dental Composites
cosity, UDMA-based composites may cure more exten-sively than Bis-GMA-based composites (Ferracane et al,1992). However, a recent study showed depth of cure tobe less in certain UDMA-composites, due to a greatermismatch in the refractive index between monomer andfiller (SoderholmeU/., 1993).
Bis-GMA has a very high viscosity because of thehydrogen bonding interactions that occur between thehydroxy groups on the monomer molecules. Thus, Bis-GMA must be diluted with a more fluid resin in order tobe useful for dental composites. TEGDMA (triethyleneg-lycoldimethacrylate) has excellent viscosity and copoly-merization characteristics, and it is most often used asthe diluent monomer for UDMA or the more viscous Bis-GMA. Optimal properties are produced when TEGDMA isused in a 1:1 ratio with Bis-GMA (Stannard et al, 1993).Other diluents include ethylene- and hexamethylene-gly-coldimethacrylate and benzyl methacrylate, a monofunc-tional monomer added to enhance polymer chain elon-gation and degree of cure (Ruyter and Nilsen, 1993).
The drawbacks to existing resins for compositesinclude: excessive polymerization shrinkage, incompleteconversion and cross-linking, and undesirable watersorption. Composite monomers cure by a free radicalpolymerization reaction to form glassy, cross-linkedpolymer networks that are relatively insoluble and some-what brittle, but reasonably strong. Resin strength isdependent upon monomer composition, being greatestwhen stiff Bis-GMA molecules are used and the degree ofconversion (DC) of the methacrylate groups is maximized(Ferracane, 1989). The minimal flexibility of the Bis-GMAmolecule enhances the rigidity of the polymer backbone.Increased cure results in enhanced cross-links betweenpolymer chains, thus enhancing the stiffness of the poly-mer network. In addition, the further conversion ofmonomer to polymer limits the number of unreactedmonomers that may serve as plasticizers in the polymer
6 ( 4 ) 3 0 2 - 3 1 8 ( 1 9 9 5 ) Crit Rev Oral Biol Med 309 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 6. Schematic representation of the polymerization of dimethacrylate monomersto form the cross-linked polymer network of dental composites containing smallamounts of unreacted monomers and many pendant methacrylate groups (C=C).
matrix (Fig. 6). In present commercial composites, it hasbeen verified by infrared spectrophotometry that 25-55%of the methacrylate groups remain unreacted after poly-merization (Ferracane and Condon, 1992; Ferracane,1994). An analysis of data on the extraction of unreactedspecies from the polymerized material suggests that lessthan 1 in 10 of the unreacted molecules is free and capa-ble of being released (Ferracane, 1994). The result is thatnearly 90% of the unreacted methacrylate groups are pre-sent on pendant molecules which have reacted at oneend by linking with the polymer chain (Fig. 6). These mol-ecules are therefore capable of serving as internal plasti-cizers for the composite.
Though DC is maximized by the inclusion of a highpercentage (40-50%) of diluents in the resin, the cure isaccompanied by a significant polymerization shrinkage(1.5-3 vol%) for most commercial materials (De Gee et al,1993). The stress associated with the curing contractionis one of the most significant problems for current mate-rials, because it adversely affects the seal at the cavosur-face margin. This is of paramount importance, becausethe predominant reason for replacement of compositesis secondary caries (Qvist et al, 1990; Maclnnis et al,1991). Recently, an experimental composite containingsmall concentrations of an antibacterial monomer hasbeen evaluated and shown to have adequate physicalproperties (Imazato and McCabe, 1994). This approachseems worthy of further study in light of the current dif-ficulty in producing excellent margins with composite
restorations.Shrinkage stresses can be reduced,
but not eliminated, by increasing fillerloading. Water sorption by the polymernetwork also contributes to a reductionin the stress (Feilzer et al, 1990). Thoughthe shrinkage and build-up of internalstress are very rapid and take place with-in minutes in a composite restoration(Davidson and De Gee, 1984), wateruptake by resin composite takes place ata much slower rate, requiring hours ordays to reach saturation (Ferracane andCondon, 1990). Thus, the delayed natureof the water sorption minimizes its effecton stress reduction. In addition, watersorption may cause erosion of thefiller/matrix interface and a softening ofthe polymer network, which can con-tribute to reductions in strength, stiff-ness, and wear resistance (Kawaguchi etal, 1988; Soderholm and Roberts, 1990;Ferracane et al, 1993). Water sorptioncan be reduced by the use of morehydrophobic monomers, such as theethoxylated version of Bis-GMA (Bis-
EMA), which do not contain unreacted hydroxyl groupson the main polymer chain (Ruyter and Nilsen, 1993).
(B) RECENT AREAS OF STUDY
Recent studies have investigated the effects of incorpo-rating different monomers as well as developing entirelynew monomers for dental composites. The ultimate goalhas been to develop materials with enhanced cure andenhanced properties, or minimal polymerization shrink-age.
Peutzfeldt and Asmussen (1991, 1992b) hypothe-sized that cyclic acid anhydrides could serve as cross-linking agents for Bis-GMA or UDMA composites toenhance their strength and abrasion resistance. Theyshowed that the tensile strength of composites could beincreased by a mean of 20% when a 1:1 molar ratio ofmaleic anhydride and methacrylamide was added to thebase resin. Though only a few of the formulationsshowed an increase (up to 10%) in flexural strength, andmost showed a reduction in elastic modulus, modulus ofresilience was increased for many. In general, theimprovement in properties was greater for the UDMA-based resin than for the Bis-GMA-based resin, especiallywhen the composites were heat-treated for one hour at125-150°C after being light-cured, as is commonly donefor composite inlays. The properties were tested afterbeing aged for only one week in water, however, and arecent study suggested that the properties of certainheat-treated composites may decline with time due to
310 Crit Rev Oral Biol Med 6(4):302-318(1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
water sorption (Ferracane et al, 1993).In similar studies, Peutzfeldt and Asmussen
(1992c,d) showed that adding 20% of bifunctionalketones, such as diacetylacetone, to UDMA and Bis-GMAcomposites caused a significant increase in diametraltensile strength, flexural strength, and modulus of rup-ture, presumably by increasing cross-linking. Similarresults were obtained when aldehydes, such as propanal,were added to these resins (Peutzfeldt and Asmussen,1992e). Subsequent studies verified that the degree ofcure was increased for these resin systems, though it wasnot possible to state whether the improvement in prop-erties was a result of enhanced polymerization or greatercross-linking (Peutzfeldt, 1994a,b). Likewise, Antonucci etal (1992) reported some improvement in the flexuralstrength of experimental composites by adding ben-zaldehyde to increase DC by chain-transfer reactions.
Other attempts to increase DC have had the addi-tional aim of reducing polymerization shrinkage.Stansbury (1990) reported on the synthesis of a series ofcyclopolymerizable monomers described as "oxy bis-methacrylates". These dimethacrylate monomers couldbe reacted to a DC of 90%, suggesting that they undergocyclopolymerization with a 40% reduction in curing con-traction compared with TEGDMA resins with similar DC.When mixed with Bis-GMA and an appropriate filler,composites with tensile strength comparable with that ofconventional composites were produced. A series ofdifunctional oxybismethacrylates, such as the oligomerof ethoxylated bis-phenol A diacrylate (OEPBA)(Stansbury, 1992a), has been synthesized and used toproduce light-cured composites with properties similarto those of ethoxylated Bis-GMA composites. The bene-fit of these new resin composite systems is that theyshow enhanced toughness and less curing shrinkagethan conventional Bis-GMA-based composites. However,the differences are probably too small to be reflected ina clinical improvement.
Stansbury and Antonucci (1992) have also synthe-sized methylene-butyrolactone (MBL), the cyclic analogof methyl methacrylate, in order to increase the DC andimprove the stability of composites. Because MBL ismore reactive than MMA, the addition of 10 wt% to a Bis-GMA/TEGDMA resin produced composites with slightlyimproved strength and a significant increase in DC.Furthermore, IR spectroscopy showed that the MBL wasalmost completely reacted in the polymerizationprocess. These results warrant the study of other multi-functional lactones.
In another study, 50-100% increases in elastic modu-lus were produced in unfilled resins made from copoly-mers of Bis-GMA and tetrahydrofurfuryl methacrylate(Davy and Braden, 1991). The authors hypothesized thatthe increase in stiffness could be attributed to the small-er diluent molecules occupying free volume spaces with-
in the main polymer network, thus enhancing the molec-ular interactions within the polymer.
Other studies have addressed the water sorptionconcerns of composites. Fluorinated monomers andoligomers which are more hydrophobic than existingbase monomers have been synthesized (Antonucci et al,1993). Composites made from fluorinated monomershave been shown to have greater strength than conven-tional Bis-GMA-based materials after storage in water,due to the hydrophobic nature of the fluoride additive(Kawaguchi et al, 1989). These resins and composites arenot as heavily plasticized by water as a result of thereduced water sorption. A recently synthesized fluorinat-ed monomer has also been shown to produce compos-ites with improved creep resistance, presumably a resultof its reduced water uptake (Culbertson et al, 1993).
In the past few years, another monomer system hasbeen developed and commercialized for dental compos-ites. The material, Conquest Crystal (leneric/Pentron), isbased on what is described as a methacrylic ester of anoligocarbonate polymer that produces a semi-crystallinepolymer matrix (Waknine, 1991). The supposed benefitsof this material are an enhanced toughness and lowerpolymerization shrinkage compared with those of Bis-GMA-based or UDMA-based composites. The effect ofthis different composition has not been clinically deter-mined to date.
Because the mechanical properties and clinical suc-cess of current materials appear to be dictated more bythe filler component than by the resin matrix, it is ques-tionable whether the monomers developed in thesestudies will have a dramatic effect on the clinical perfor-mance of dental composites. More than likely, the great-est advances in resin technology will be made in the areaof minimizing polymerization shrinkage and its accom-panying stress. Earlier efforts were not successful, butseveral recent studies have been more encouraging.
Stansbury (1992b) has synthesized spiro-orthocar-bonate monomers (SOCs) which expand during polymer-ization through a double-ring-opening process. Thesemonomers contain methylene groups capable of freeradical polymerization, making them useful as additivesto dimethacrylates (Fig. 7). The task is to cause sufficientdouble-ring-opening to produce enough expansion tocounter the free radical polymerization shrinkage of thedimethacrylates, all within a reasonable time frame forclinical application. This has not occurred to date.Recently, Stansbury (1992c) reported that spiro orthocar-bonate-substituted methacrylates showed nearly com-plete ring-opening of the SOC when polymerized indilute solutions. Less ring-opening was obtained whenthe resin was cured in bulk and the composites hadabout 1% shrinkage. Miyazaki et al (1994) reported on thesynthesis of acrylates and methacrylates containingspiro ortho esters that were capable of being polymer-
6(4) :302-3 l8 (1995) Crit Rev Oral Bid Ued 31 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 7. Chemical structure of two of the SOC monomers understudy for non-shrinking dental composites.
ized by heat, ionic and free radical initiators. Though allcommon methods of curing were possible, the resultantpolymers were weak, and the reduction in polymerizationshrinkage was not enough to be clinically significant.Other ring-opening monomers based on vinyl cyclicacetals have been co-polymerized with Bis-EMA to givecomposites with good strength, but shrinkage has notbeen reported (Reed et ai, 1992).
Because the reaction of vinyl functional groups (con-taining C=C) ensures polymerization contraction, othershave taken a different approach with SOCs. Byerley et al.(1992) and Eicket ai (1992) recently reported on the syn-thesis of new SOCs polymerized with epoxy resins viacationic UV photo-initiation. These alicyclic SOCs con-tain four rings attached to a central spiro carbon, andexpansion is again achieved by a double-ring-openingmechanism (Fig. 7). The cationic initiator used is (4-octy-loxyphenyl)phenyliodonium hexafluoroantimonate, withchlorothioxanthone as a sensitizer. The mixing of 5% ofthe SOC in an epoxy base produced a resin with sub-stantial tensile strength and modulus, acceptable watersorption and solubility, and a slight expansion. Increasedconcentrations of the SOC produced greater expansionand slightly stronger polymers, but water sorption andsolubility were high due to incomplete reaction of theSOC. However, the results of these studies are encourag-ing, and work is continuing.
The development of a dental composite with zeronet dimensional change would be the single most signif-
icant advancement in these materials since their devel-opment. Though composites do not have ideal strength,wear resistance, or durability, significant improvementsin their formulation have produced materials capable ofbeing used in a wide variety of dental applications.However, the difficulty encountered in placing the mate-rials, most of which is a direct result of the curing con-traction, severely limits their use in many dental prac-tices. The clinician must continually rely on an adhesivematerial as an intermediate between the composite andtooth structure to provide a durable marginal seal.Though materials have been developed which exhibitexcellent adhesive strength to both enamel and dentin,the ability for this adhesion to be achieved routinely inthe moist oral cavity is questionable and highly doubtful,due to the significant stress imposed on thetooth/restoration bond by the contracting composite fill-ing material. The development of a non-shrinking com-posite would obviate the need for a very strong adhesive,one that is capable of resisting the substantial force ofpolymerization contraction. For this reason, it is wellworth the effort expended in the development of thisnew material. However, it is realistic to expect that themarketing of commercial dental composites with ade-quate strength and abrasion resistance and zero shrink-age through the use of expanding monomers remainsseveral years away.
(IV) Polymerization Promoters and ModifiersThe polymerization of the monomers in a dental com-posite paste can be accomplished in several ways.Appropriate chemical species are added to the compos-ite paste to facilitate this process. The reaction must beactivated, however, by an external stimulus. In self-curedor auto-cured materials, this stimulus is the mixing oftwo pastes, one of which contains a chemical activatorand the other of which contains a chemical initiator. Forheat-cured materials, temperatures of 100°C or moreprovide the stimulus which activates the initiator. Forlight-cured systems, the visible-light energy provides thestimulus to activate the special initiator in the paste.Each of these mechanisms is efficient in producing ahigh degree of cure under the appropriate conditions.However, several factors directly related to the polymer-ization promoters affect the rate and extent of the poly-merization.
(A) PRESENT MATERIALS
Self- or auto-curing composites were the first typesdeveloped. The chemistry was based on traditionalacrylic systems. Curing is initiated by mixing two pastes,which brings together the initiator, benzoyl peroxide, andthe activator, an amine such as dihydroxyethyl-p-tolui-dine (DHEPT), in order to start the polymerization reac-tion. Self-cure composites lessened in popularity when
312 Crit Rev Oral Biol Med 6(4):302-318(1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
light-curing was developed. Light-curing offered a con-trolled working time and the elimination of the mixingprocedure that took time and incorporated porosity intothe material. In addition, clinical studies have shownthat self-cure composites undergo more darkening thanlight-cured composites overtime (Tyas, 1992). However,self-cure composites may be experiencing a re-emer-gence.
A technique that was introduced years ago in Japanhas recently been described where the proximal box of aclass II restoration is filled with a self-cured compositeand the occlusal portion is filled with a light-cured com-posite (Bertolotti, 1991). The rationale is that certaindentin adhesives may initiate the cure of the self-curecomposite at the interface, causing the polymerizationcontraction to occur toward instead of away from thewarm tooth surface. The use of the light-cured compos-ite on the surface provides the benefits of maximumworking time and fewer bubbles in the surface material.No controlled clinical studies have been presented tosupport this procedure to date, but at least one dentalmanufacturer has produced a self-curing version of theircomposite for this purpose (Bis-fil II, Bisco, Inc).
Self-curing polymerization is also used in dual-curecomposites used as cements for composite and ceramicinlays. The rationale behind these materials is that anyportion not exposed to the light source will self-cure onits own. However, the self-cure reaction does not pro-duce as high a DC as the light activation (Caughman andRueggeberg, 1992). This may be because the cure of themonomers is significantly inhibited by the use of low lev-els of amine/peroxide or high levels of inhibitor (such asbutylated hydroxytoluene) that are incorporated to max-imize working time. The clinical significance of this dif-ference in cure is not yet known.
The most popular mode of causing the curing of den-tal composites is light activation. The initiator in light-activated dental composites is camphoroquinone (CQ),which is sensitive to blue light in the 470-nm region ofthe electromagnetic spectrum. The reactivity of CQ isenhanced by the addition of an amine-reducing agent,such as dimethylamino ethylmethacrylate (DMAEM),ethyl-4-dimethylaminobenzoate (EDMAB), or N,N-cya-noethyl-methylaniline (CEMA). CQ and amine concen-trations vary in commercial composites from 0.2-1.2 wt%(Taira et al, 1988). Recently, Yoshida and Greener (1994)systematically varied the ratios of CQ and DMAEM inunfilled resins and found that maximum cure was pro-duced when the two were used in a 1:1 ratio, as long asCQ was present at 1.0 mol% or more. However, the incor-poration of small fillers of a size that is equivalent to thewavelength of the curing light (approximately 0.5 jim)produces composites with poorer light transmission(Kawaguchi et al, 1994). This has prompted proprietarymodifications in the types and amounts of additives
used to enhance overall curing depth. At the same time,these alterations in composition have produced com-posites which are more sensitive to the operatory anddental unit lights. The clinician must be careful to mini-mize exposure to light until he or she is ready to cure thematerial; otherwise, premature polymerization willbegin, and the working time will be reduced to an unac-ceptable level.
Another common method for curing compositesextra-orally is through the application of heat, eitheralone or in conjunction with light-curing. This procedureis commonly used to cure composite inlays and onlays,either in the laboratory or at chairside. Many compositesused for direct placement can also be cured with lightand heat or in light-curing ovens to produce theserestorations. Concept (Ivoclar) is a microfilled compositespecifically designed as an inlay/onlay material. It iscured by being heated to 120°C in water under approxi-mately 80 psi of pressure. The pressure produces a densematerial, and the heat activates the benzoyl peroxide cat-alyst present in the paste. Heat-curing or a post-light-cure heat treatment improves the properties of compos-ites by enhancing cure and/or cross-linking of the poly-mer (Wendt, 1989; Ferracane and Condon, 1992). Clinicalevaluations have shown improvement in wear resistance(Leinfelder and Broome, 1994) and resistance to margin-al degradation (Wendt and Leinfelder, 1990) as a result ofthe heat treatment.
(B) RECENT AREAS OF STUDY
Though current activity in this area appears to be mini-mal, the development of new monomer systems will cer-tainly stimulate work to produce agents for maximumcuring efficiency. One such area of study involves thedevelopment of non-shrinking polymers which are poly-merized via cationic initiation (Byerley et al, 1992). Thequestion that arises deals with the compatibility of boththe resins cured via cationic polymerization and thoseused in dental adhesives which polymerize via free-radi-cal mechanisms. A recent study by Stansbury et al. (1993)showed that a monomer with ring-opening potentialcould be co-polymerized with Bis-EMA by a free radicalmechanism or a combination of a free radical and cation-ic mechanism, but did not co-polymerize well undercationic conditions alone. Extensive studies of the bio-compatibility of the cationic initiators will also berequired to prove their safety.
Another emerging area involves the use of lasers tocure dental composites to a greater extent and to agreater depth of cure using shorter illumination times.Theoretically, shorter curing times, even at higher inten-sity, will also produce less heat build-up in teeth, thoughthis has never been proven to be a significant clinicalproblem. Generally, studies show that composites curedwith an argon laser have slightly greater surface hardness
6 ( 4 ) 3 0 2 - 3 1 8 ( 1 9 9 5 ) Crit Rev Oral Biol Med 313 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Figure 8. Simplified schematic representation of silane bonding between the fillersand the polymer matrix in dental composites.
and depth of cure than composites cured with a visible-light source (Blankenau et al, 1991). However, these dif-ferences have been less apparent when adequate curingtimes of 40-60 seconds are used with efficient visible-light-curing units (Kurokawa, 1990).
In addition, though peak temperatures can bereduced with low-power laser curing, considerable heatis generated when lasers are used at the higher powers,where they are most efficient for curing (Burtscher, 1991).Therefore, though some minimal improvements may beobtained by the use of an argon laser, the results to datedo not demonstrate a rationale for the use of this expen-sive device for routine curing of composites. In addition,another factor which sheds doubt on the usefulness ofthis rapid-curing technique is the stress produced on theadhesive bond. It has been suggested that compositesthat undergo a slow cure may have enhanced marginalintegrity, because strong bonds to tooth structure can besecured by the adhesive before the forces of polymeriza-tion contraction from the composite reach significantlevels (Unoand Asmussen, 1991). Faster curing producesa more rapid elevation in stress within the composite aswell as at the interface, which may disrupt the bonds asthey are forming, thus compromising marginal sealing(LoscheeUL, 1994).
(V) Filler/Matrix-coupling AgentsDuring the initial development of dental composites, itwas shown that the acquisition of good properties in thematerial was dependent upon the formation of a strongbond between the inorganic filler particles and the
organic polymer matrix (Bowen, 1963).The linking of these two phases isbrought about by coating the fillerswith a coupling agent that has charac-teristics of both the filler and thematrix. The usual coupling agent fordental composites is a molecule whichhas silanol (Si-OH) groups on one endand methacrylate groups (containingC=C) on the other end. These mole-cules are capable of forming covalentbonds to both the silicon-oxygengroups in the silica-based fillers andthe methacrylate groups in the resinmatrix (Fig. 8). Studies have verified theimportance of this coupling in dictatingthe mechanical properties of the resul-tant composite (Nishiyama et al, 1991;Mohsen and Craig, 1995a,b).
(A) PRESENT MATERIALS
Most commercial composites containsilica-based fillers, and therefore usesilanes with functional methacrylate
groups as filler/matrix-coupling agents. The most com-mon silane is 3-methacryloxypropyl trimethoxysilane(MPS). Other agents have been experimented with, suchas other silanes, 4-META, and various titanates and zir-conates, but none has been as successful as MPS. Forexample, MPS was recently compared with APS (3-acry-loxypropyltrimethoxysilane) and shown to producestronger and more stable composites with quartz or zir-conia silicate (Mohsen and Craig, 1995a,b).
(B) RECENT AREAS OF STUDY
Craig and Dootz (1993) reported that a mixture of silanesmay be used to improve the properties of composites.They added a fluoro-alkyl silane to MPS (1:3) for Zr-sili-cate fillers. The resultant composites had 20% greatertensile strength and 60% less water sorption than com-posites with MPS alone. Recently, Mohsen and Craig(1995b) demonstrated that silanation at three times theamount necessary to provide uniform coverage of a zir-conia-silica filler gave the best properties.
Further developments in fillers for composites maynecessitate the continued development of couplingagents. However, based on the tremendous history of theuse of silanes in industrial composites and their reason-ably successful use in dental composites to date, it seemslikely that future studies will involve only further refine-ments of existing silanes in terms of optimal amountsand modes of coverage (Soderholm and Shang, 1993).
(VI) SummaryIt is apparent that current composites have significantly
314 Crit Rev Oral Biol Ued 6(4):302-318 (1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
improved clinical performance compared with their pre-decessors, especially in posterior teeth and in stress-bearing areas on anterior teeth. However, it is also appar-ent that current formulations remain less than ideal interms of dimensional change during curing and long-term fatigue and fracture resistance.
Future research efforts will remain committed to thedevelopment of non-shrinking polymer systems whichcan be mixed with appropriate curing modifiers andfillers to produce restorative materials with excellentqualities. Considerable effort will be expended in thelaboratory and clinic to ensure that the new materialshandle and perform at and above the level of existingmaterials. Weaknesses will be identified, and furtherrefinements in formulations will then take place to max-imize performance. The extent of these tests will dependupon the nature of the candidate monomers, because ifmethacrylate systems are used as base monomers withfree-radical catalysts, the efforts will necessarily be lessextensive than if cationic polymerization composites areproduced from non-methacrylate base resins. A full com-plement of biocompatibility testing of all of the compo-nents in the new materials will be required. In the inter-im, further changes in dental composite formulation willbe minor, probably in the areas of new fillers and grind-ing processes which produce the necessary sizes of par-ticles in high yields. These particles will ideally be veryfracture-resistant and only minimally abrasive to dentinand enamel. In addition, their refractive index will beaccurately matched to existing as well as newly devel-oped polymers. Finally, continued development of fillersand polymers containing therapeutic agents, such as flu-oride, is likely to produce composites which may havecariostatic properties like glass ionomers.
AcknowledgmentsThe author thanks Mr. }ohn Condon for his efforts in producing thescanning electron micrographs. A portion of this work was presented atthe Second International Congress on Dental Materials, held inHonolulu, Hawaii, on November 1-4, 1993. The Congress was jointlysponsored by the Academy of Dental Materials and The JapaneseSociety for Dental Materials and Devices.
REFERENCES
Antonucci ]M, Fowler BO, Venz S (1991). Filler systemsbased on calcium metaphosphates. Dent Mater 7:124-129.
Antonucci JM, Stansbury JW, Keeny SM, Matsukawa S(1992). Effect of aldehydes on the mechanicalstrength of dental composites (abstract). I Dent Res72:598.
Antonucci )M, Liu D-W, Stansbury JW (1993). Synthesis ofhydrophobic oligomeric monomers for dental appli-
cations (abstract). I Dent Res 72(Spec Iss):369.Arends J, Ruben J (1988). Fluoride release from a com-
CM (1991). Clinical longevity of ten posterior com-posite materials based on wear (abstract). ) Dent Res70:344.
Bayne SC, Taylor DF, Heymann HO (1992). Protectionhypothesis for composite wear. Dent Mater 8:305-309.
Bayne SC, Heymann HO, Swift El (1994). Update on den-tal composite restorations. I Am Dent Assoc 125:687-701.
Beatty MW, Swartz ML, Moore BK, Phillips RW, RobertsTA (1993). Effect of crosslinking agent content,monomer functionality, and repeat unit chemistry onproperties of unfilled resins. 1 Biorned Mater Res 27:403-413.
Bertolotti R (1991). Posterior composite technique utiliz-ing directed polymerization shrinkage and a novelmatrix. Pract Perio Aesth Dent 3:53-58.
Blankenau RJ, Kelsey WP, Powell GL, Shearer GO,BarkmeierWW, Cavel WT (1991). Degree of compositeresin polymerization with visible light and argonlaser. Aust Dent J 4:40-42.
Bowen R (1963). Properties of silica reinforced polymerfor dental restoration. 1 Am Dent Assoc 66:57-64.
Bowen RL, Eichmiller FC, Marjenhoff WA (1991). Glass-ceramic inserts anticipated for "megafilled" compos-ite restorations. ) Am Dent Assoc 122:71-75.
Braem M, Ringer W, Van Doren VE, Lambrechts P,Vanherle G (1989). Mechanical properties and fillerfraction of dental composites. Dent Mater 5:346-349.
Braem MJA, Davidson CL, Lambrechts P, Vanherle G(1994a). \n vitro flexural fatigue limits of dental com-posites. I Biomed Mater Res 28:1397-1402.
Braem M, Lambrechts P, Vanherle G (1994b). Clinical rel-evance of laboratory fatigue studies. I Dent 22:97-102.
Bryant RW, Marzbani N, Hodge KV (1992). Occlusal mar-gin defects around different types of composite resinrestorations in posterior teeth. OperDent 17:215-221.
Burtscher P (1991). Curing of composites with an argonlaser (abstract). ] Dent Res 70(Spec lss):526.
Byerley T), Eick ID, Chen GP, Chappelow CC, Millich F(1992). Synthesis and polymerization of new expand-ing dental monomers. Dent Mater 8:345-350.
Caughman W, Rueggeberg F (1992). Monomer conversionin dual cure resin adhesives (abstract). I Dent Res71 (Spec Iss): 160.
Chung K, Greener EH (1990). Correlation between degreeof conversion, filler concentration and mechanicalproperties of posterior composite resins. I Oral Rehabil17:487-494.
Craig RG, Dootz ER (1993). Effect of mixed silanes onstrength and sorption of composites (abstract). I DentRes 72(Spec Iss):383.
6(4):302-318 (1995) Crit Rev Oral Biol Med 315 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Culbertson BM, Sang J, Brantley WAr Lo SK (1993). Newdental resins with improved creep resistance(abstract). ] Dent Res 72(Spec Iss):178.
Dagani R (1992). Nanostructured materials promise toadvance range of technologies. Chem Eng News 70:18-24.
Davidson CL, De Gee AJ (1984). Relaxation of polymer-ization contraction stresses by flow in dental com-posites. J Dent Res 63:146-148.
Davy KW, Braden M (1991). Study of polymeric systemsbased on 2,2-bis-4(2-hydroxy-3-methacryloyl-oxypropoxy)phenylpropane. Biomater 12:406-410.
De Gee AJ, Feilzer AJ, Davidson CL (1993). True linearpolymerization shrinkage of unfilled resins and com-posites determined with a linometer. Dent Mater 9:11-14.
Dijkman GEHM, de Vries J, Lodding A, Arends J (1993).Long-term fluoride release of visible light-activatedcomposites in vitro: a correlation with in situ deminer-alization data. Caries Res 27:117-123.
Eick JD, Byerley TJ, Chappell RP, Chen GP, Bowles CQ,Chappelow CC (1992). Properties of expandingSOC/epoxy copolymers for dental use in dental com-posites. Dent Mater 9:123-127.
el-Mowafy OM, Lewis DWF Benmergui C, Levinton C(1994). Meta-analysis on long-term clinical perfor-mance of posterior composite restorations. J Dent22:33-43.
Feilzer AJ, deGee AJ, Davidson CL (1990). Relaxation ofpolymerization contraction shear stress by hygro-scopic expansion. J Dent Res 69:36-39.
Ferracane JL (1989). In vitro evaluation of compositeresins. Structure-property relationships.Development of assessment criteria. Trans head DentMater 2:6-35.
Ferracane JL, Antonio RC, Matsumoto H (1987). Variablesaffecting the fracture toughness of dental compos-ites. J Dent Res 66:1140-1145.
Ferracane JL, Condon JR (1990). Rate of elution of leach-able components from composite. Dent Mater 6:282-287.
Ferracane JL, Condon JR (1992). Post-cure heat treat-ments for composites: properties and fractography.Dent Mater 8:290-295.
Ferracane JL, Greener EH (1986). The effect of resin for-mulation on the degree of conversion and mechanicalproperties of dental restorative resins. J Biomed MaterRes 20:121-131.
Ferracane JL, Condon JR, Suh B (1992). Effect of filler ondegree of conversion (DC) of resins (abstract). J DentRes 72(Spec Iss):598.
Ferracane JL, Hopkin JK, Condon JR (1993). The proper-ties of heat-treated composites after aging (abstract).I Dent Res 72(Spec lss):135.
George LA, Richards ND (1993). Polymerization shrink-age in a composite restoration involving a glass-ceramic insert (abstract). J Dent Res 72(Spec Iss).-351.
Hosoda H, Yamada T, Inokoshi S (1990). SEM and ele-mental analysis of composite resins. J Prosthet Dent64:669-676.
Iga M, Takeshige F, Ui T, Torii M, Tsuchitani Y (1991). Therelationship between polymerization shrinkage mea-sured by a modified dilatometer and the inorganicfiller content of light-cured composites. Dent Mater ]10:38-45.
Imazato S, McCabe JF (1994). Influence of incorporationof antibacterial monomer on curing behavior of adental composite. I Dent Res 73:1641-1645.
Kawaguchi M, Fukushima T, Horibe T (1988). Effect ofmonomer structure on the mechanical properties oflight-cured unfilled resin. Dent Mater] 7:174-181.
Kawaguchi M, Fukushima T, Horibe T (1989). Effect ofmonomer structure on the mechanical properties oflight-cured composite resins. Dent Mater] 8:40-45.
Kawaguchi M, Fukushima T, Miyazaki K (1994). The rela-tionship between cure depth and transmission coeffi-cient of visible-light-activated resin composites. JDent Res 73:516-521.
Kawai K, Leinfelder KF (1993). Effect of glass inserts onwear of composite resins (abstract). J Dent Res 72(SpecIss):114.
Khan AM, Suzuki H, Normura Y, Taira M, Wakasa K,Shintani H, et al (1992). Characterization of inorganicfillers in visible-light-cured dental composite resins. IOralRehabil 19:361-370.
Kim KH, Park JH, Imai Y, Kishi T (1994). Microfracturemechanisms of dental resin composites containingspherically-shaped filler particles. J Dent Res 73:499-504.
Knibbs PJ, Smart ER (1992). The clinical performance of aposterior composite resin restorative material,Heliomolar R.O.: 3-year report. J Oral Rehabil 19:231-237.
Kurokawa M (1990). Study on light-cured compositeresins: consideration of the polymerization character-istics of composites cured by argon ion laser. J NihonUniv Sch Dent 32:48.
Lambrechts P, Vanherle G, Vuylsteke M, Davidson CL(1984). Quantitative evaluation of the wear resistanceof posterior dental restorations: a new three-dimen-sional measuring technique. J Dent 12:252-267.
Leinfelder KF (1995). Posterior composite resins: thematerials and their clinical performance. J Am DentAssoc 126:663-676.
Leinfelder KF, Broome JC (1994). ]n vitro and in vivo evalu-ation of a new universal composite resin. J Esthet Dent
316 Crit Rev Oral Biol Ued 6(4):302-318 (1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
Munksgaard EC, Hansen EK, Kato H (1987). Wall-to-wallpolymerization contraction of composite resins versusfiller content. Scand ] Dent Res 95:526-531.
Nishiyama N, Ishizaki T, Horie K, Tomari M, Someya M(1991). Novel polyfunctional silanes for improvedhydrolytic stability at the polymer-silica interface. JBiomed Mater Y<es 25:213-221.
0ysaed H, Ruyter IE (1986). Water sorption and fillercharacteristics of composites for use in posteriorteeth. J Dent Res 65:1315-1318.
Peutzfeldt A (1994a). Quantity of remaining doublebonds of diacetyl-containing resins. I Dent Res 73:511-515.
Peutzfeldt A (1994b). Quantity of remaining doublebonds of propanal-containing resins. I Dent Res73:1657-1662.
Peutzfeldt A, Asmussen E (1991). Influence of carboxylicanhydrides on selected mechanical properties ofheat-cured resin composites. I Dent Res 70:1537-1541.
Peutzfeldt A, Asmussen E (1992a). Modulus of resilienceas predictor for clinical wear of restorative resins. DentMater 8:146-148.
Peutzfeldt A, Asmussen E (1992b). Effect of temperatureand duration of post-cure on selected mechanicalproperties of resin composites containing carboxylicanhydrides. Scand I Dent Res 100:296-298.
Peutzfeldt A, Asmussen E (1992c). Influence of ketones
on selected mechanical properties of resin compos-ites. I Dent Res 71:1847-1850.
Peutzfeldt A, Asmussen E (1992d). Ketones in resin com-posites. Effect of ketone content and monomer com-position on selected mechanical properties. ActaOdontol Scand 50:253-258.
Peutzfeldt A, Asmussen E (1992e). Influence of aldehydeson selected mechanical properties of resin compos-ites. I Dent Res 71:1522-1524.
Phillips RW, Editor (1991). Skinner's science of dentalmaterials. 9th ed. Philadelphia, PA: W.B. SaundersCo., pp. 215-248.
Qvist V, Qvist I, Mjor IA (1990). Placement and longevityof tooth-colored restorations in Denmark. Acta OdontolScand 48:305-311.
Reed B, Stansbury J, Antonucci I (1992). Ring-openingdental resin systems based on cyclic acetals(abstract). ) Dent Res 71 (Spec Iss):276.
Rueggeberg FA, Jordan DM (1993). Effect of light-tip dis-tance on polymerization of resin composite. \nt JProsthodont 6:364-370.
Ruyter IE, Nilsen J (1993). Chemical characterization ofsix posterior composites (abstract). 1 Dent Res 72(SpecIss):177.
Ruyter IE, 0ysaed H (1987). Composites for use in poste-rior teeth: Composition and conversion. J Biomed MaterRes 21:11-23.
Seghi RR, Sang J, Hayes D, Culbertson BM (1993).Relative abrasion rates of sol-gel derived dual matrixcomposites. ] Dent Res 72(Spec Iss): 113, Abstr. No. 80.
Soderholm K-JM (1984). Influence of silant treatment andfiller fraction on thermal expansion of compositeresins. J Dent Res 63:1321-1326.
Soderholm K-JM (1990). Filler teachability during waterstorage of six composite materials. Scand ) Dent Res98:82-88.
Soderholm K-JM, Achanta S, Olsson S (1993). Variablesaffecting the depth of cure of composites (abstract). JDent Res 72(Spec Iss): 138.
Soderholm KM, Roberts MJ (1990). Influence of waterexposure on the tensile strength of composites. J DentRes 69:1812-1816.
Soderholm K-JM, Shang S-W (1993). Molecular orienta-tion of silane at the surface of colloidal silica. J DentRes 72:1050-1054.
Soderholm K-JM, Zigan M, Ragan M, Fischlschweiger W,Bergman M (1984). Hydrolytic degradation of dentalcomposites. I Dent Res 63:1248-1254.
Stangel I, Barolet RY (1990). Clinical evaluation of twoposterior composite resins: two-year results. J OralRehabil 17:257-268.
Stannard JG, Sornkul E, Collier R (1993). Mechanical
6(41:302-318(1995) Crit Rev Oral Biol Med 317 at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
properties of composite resin co-polymers (abstract).) Dent Res 72(SpecIss):135.
Stansbury JW (1990). Cyclopolymerizable monomers foruse in dental resin composites. I Dent Res 69:84-848.
Stansbury JW (1992a). Synthesis and evaluation of novelmultifunctional oligomers for dentistry. J Dent Res71:434-437.
Stansbury JW (1992b). Spiro orthocarbonate-substitutedmethacrylates: New monomers for ring-opening poly-merization (abstract). I Dent Res 71:239.
Stansbury JW (1992c). Synthesis and evaluation of newoxaspiro monomers for double ring-opening poly-merization. J Dent Res 71:1408-1412.
Stansbury JW, Antonucci JM (1992). Evaluation of meth-ylene lactone monomers in dental resins. Dent Mater8:270-273.
Stansbury JWr Antonucci JM, Reed BB (1993). Initiatoreffects on the tensile strength of novel dental com-posites (abstract). J Dent Res 72(Spec Iss):385.
Suzuki H, Taira M, Wakasa K, Yamaki M (1991).Refractive-index-adjustable fillers for visible-light-cured dental resin composites: preparation of TiO2-SiO2 glass powder by the sol-gel process. J Dent Res70:883-888.
Suzuki S, Leinfelder KF (1994). An in vitro evaluation of acopolymerizable type of microfilled composite resin.Quintessence \nt 25:59-64.
Taira M, Urabe H, Hirose T, Wakasa K, Yamaki M (1988).Analysis of photo-initiators in visible-light-cured den-tal composite resins. J Dent Res 67:24-28.
Takahashi K, Emilson CG, Birkhed D (1993). Fluoriderelease in vitro from various glass ionomer cementsand resin composites after exposure to NaF solu-tions. Dent Mater 9:350-354.
Tani Y (1983). A new composite resin "Palfique"—charac-teristics and clinical use. Dent Outlook 62:887-896.
Tani Y (1993). New technology of composite resins devel-oped in Japan. Trans Second \nt Cong Dent Mater, pp. 54-61.
Taylor DF, Bayne SC, Leinfelder KF, Davis S, Koch GG(1994). Pooling of long term clinical wear data forposterior composites. Am J Dent 7.167-174.
Tyas MJ (1990). Correlation between fracture properties
and clinical performance of composite resins in classIV cavities, hustr Dent J 35:46-49.
Tyas JM, Wassenaar P (1991). Clinical evaluation of fourcomposite resins in posterior teeth. Five-year results.hustr Vent] 36:369-373.
Tyas MJ, Truong VT, Goldman M, Beech DR (1989).Clinical evaluation of six composite resins in posteri-or teeth, hustr Dent J 34:147-153.
Uno S, Asmussen E (1991). Marginal adaptation of arestorative resin polymerized at reduced rate. Scand JDent Res 99:440-444.
van Dijken JWV, Wing KR, Ruyter IE (1989). An evaluationof the radiopacity of composite restorative materialsused in class I and class II cavities, hcta Odontol Scand47:401-407.
Waknine S (1991). Conquest DFC: a novel universal den-tal composite restorative system. Esthet Dent Update2:70-72.
Wendt SL (1989). Time as a factor in the heat curing ofcomposite resins. Quintessence \nt 20:259-263.
Wendt SL, Leinfelder KF (1990). The clinical evaluation ofheat-treated composite resin inlays. J Am Dent hssoc120:177-181.
Wendt SL, Leinfelder KF (1992). Clinical evaluation ofClearfil photoposterior and bonding system: 3-yearresults. Am J Dent 5:121-125.
Wendt SL, Leinfelder KF (1994). Clinical evaluation of aposterior resin composite: 3-year results. Am J Dent7:207-211.
Willems G, Lambrechts P, Braem M, Celis JP, Vanherle G(1992). A classification of dental composites accord-ing to their morphological and mechanical character-istics. Dent Mater 8:310-319.
Wilson NHF, Wilson MA, Wastel DG, Smith GA (1991).Performance of Occlusin in butt-joint and bevel-edgedpreparations: five-year results. Dent Mater 7:92-98.
Yoshida K, Greener EH (1994). Effect of photoinitiator ondegree of conversion of unfilled light-cured resin. J
318 Crit Rev Oral Biol Ued 6(4):302-318(1995) at Univesita La Sapienza on May 21, 2014 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from