62
10/6/2016 1 Current Trends in MIH What’s Working? What We’re Gonna Do… • MIH and EMS Economic Models • Medical Oversight • Training & Continuing Education • Tech to Support MIH Programs
10/6/2016
1
Current Trends in MIHWhat’s Working?
What We’re Gonna Do…
• MIH and EMS Economic Models
• Medical Oversight
• Training & Continuing Education
• Tech to Support MIH Programs
10/6/2016
2
MIH Economics:What’s Working?
Matt Zavadsky, MS‐HSA, EMTChief Strategic Integration OfficerMedStar Mobile Healthcare
© 2016 MedStar Mobile Healthcare
Healthcare Finance 3.0
• FFS OUTCOMES• Readmission & VBP penalties• MSPB calculations = 2015
– Medicare Spending Per Beneficiary
• Bundled payments– CCJR– Cardiac
• Push to Managed Medicare/Medicaid• Merger and Acquisition activity
Healthcare Finance 3.0
• ACOs• 838 as of April 2016
– 28.3 million covered lives
http://healthaffairs.org/blog/2016/04/21/accountable‐care‐organizations‐in‐2016‐private‐and‐public‐sector‐growth‐and‐dispersion/
10/6/2016
3
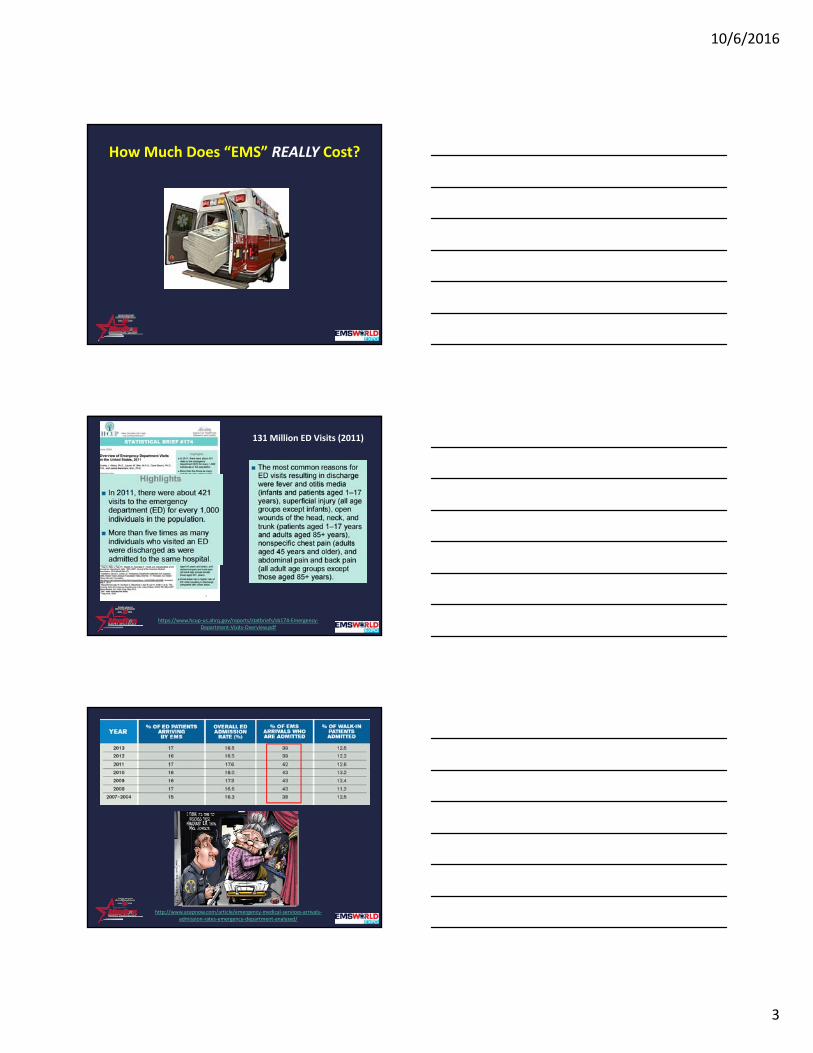
How Much Does “EMS” REALLY Cost?
131 Million ED Visits (2011)
https://www.hcup‐us.ahrq.gov/reports/statbriefs/sb174‐Emergency‐Department‐Visits‐Overview.pdf
http://www.acepnow.com/article/emergency‐medical‐services‐arrivals‐admission‐rates‐emergency‐department‐analyzed/
10/6/2016
4
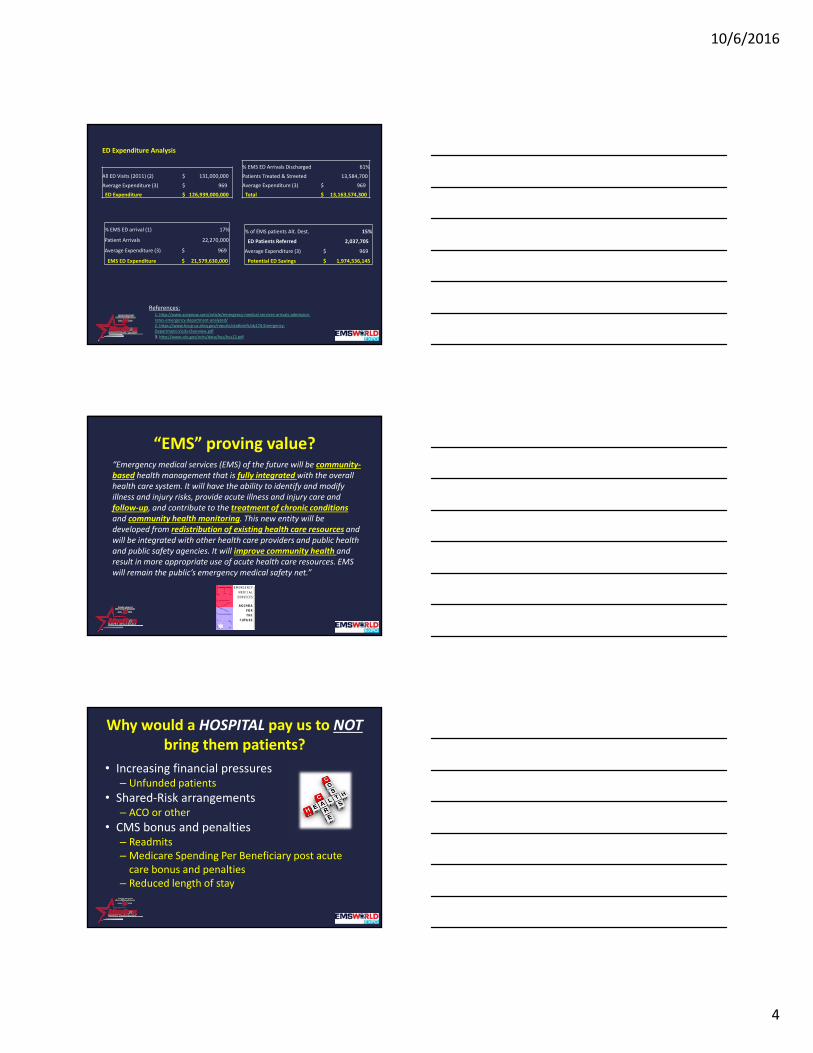
ED Expenditure Analysis
All ED Visits (2011) (2) $ 131,000,000
Average Expenditure (3) $ 969
ED Expenditure $ 126,939,000,000
% EMS ED arrival (1) 17%
Patient Arrivals 22,270,000
Average Expenditure (3) $ 969
EMS ED Expenditure $ 21,579,630,000
% EMS ED Arrivals Discharged 61%
Patients Treated & Streeted 13,584,700
Average Expenditure (3) $ 969
Total $ 13,163,574,300
References:1. http://www.acepnow.com/article/emergency‐medical‐services‐arrivals‐admission‐rates‐emergency‐department‐analyzed/ 2. https://www.hcup‐us.ahrq.gov/reports/statbriefs/sb174‐Emergency‐Department‐Visits‐Overview.pdf
3. http://www.cdc.gov/nchs/data/hus/hus12.pdf
% of EMS patients Alt. Dest. 15%
ED Patients Referred 2,037,705
Average Expenditure (3) $ 969
Potential ED Savings $ 1,974,536,145
“EMS” proving value?“Emergency medical services (EMS) of the future will be community‐based health management that is fully integrated with the overall health care system. It will have the ability to identify and modify illness and injury risks, provide acute illness and injury care and follow‐up, and contribute to the treatment of chronic conditions and community health monitoring. This new entity will be developed from redistribution of existing health care resources and will be integrated with other health care providers and public health and public safety agencies. It will improve community health and result in more appropriate use of acute health care resources. EMS will remain the public’s emergency medical safety net.”
Why would a HOSPITAL pay us to NOTbring them patients?
• Increasing financial pressures– Unfunded patients
• Shared‐Risk arrangements– ACO or other
• CMS bonus and penalties– Readmits– Medicare Spending Per Beneficiary post acute care bonus and penalties
– Reduced length of stay
10/6/2016
5
Hospitals Are Paying For…
• 9‐1‐1 Nurse Triage
– Reduce preventable ED visits
– Improve HCAHPS scores
• High Utilizer Group (HUG) patients
– Reduce preventable ED visits
– Improve HCAHPS scores
– 1115a Waiver projects
• Delivery System Reform Incentive Payments (DSRIP)
Hospitals Are Paying For…
• Readmission prevention programs– Reduce preventable readmits
– Reduce penalties• Or keep up with reductions
– Improve HCAHPS scores• Transition home
• Transitional response units (medic w/NP)– Reduce preventable ED visits
– Reduce preventable admissions/readmissions
Hospitals Are Paying For…
• BPCI//CCJR
– Hospitals//Ortho bundled payment for knee surgery
– Desire to < preventable ED visits/Admissions
– Use MedStar CCPs to:
• Reduce cancelations pre‐procedure
• Express rehab if possible based on home environment
• Reduce length of stay for the procedure
• Intervene in 911 response 90 days post‐procedure
10/6/2016
6
Why would a Physician IPA pay usto NOT transport patients?
• Reduce spend
– In a shared risk contract with 3rd party payer
• Improve patient experience
– NCQA Accreditation standards
• Improve outcomes
– Fewer hospitalizations
– Fewer Hospital Acquired Conditions (HAC)
IPA is Paying For…
• High Utilizer Group (HUG) patients– Reduce preventable ED visits
– Improve HCAHPS scores
• Admission/Readmssion prevention programs– Reduce preventable admissions
• Pre and beyond 30‐days
• Care about the SPEND
– Improve Physician HCAHPS scores• Transition home
IPA is Paying For…
• Observational admission avoidance– Reduce spend
• Shared risk contract
• Palliative Care project– Meet patient goals– Transition to Hospice– Reduce spend
10/6/2016
7
Why would Hospice pay us NOTtransport patients?
• Voluntary disenrollment– Patient wishes not met– High cost / lost revenue– CMS penalty?
• Involuntary revocation– Patient wishes not met– High cost / lost revenue– CMS penalty?
Hospice is Paying For…
• Notification of response– Start the hospice nurse enroute to scene
• Back‐up episodic intervention– While awaiting Hospice nurse
• 9‐1‐1 redirection– Respond/assess/consult– Care at home or direct admit to inpatient hospice
Why would HOME HEALTH pay us to see their patients
(and notify them if a patient calls 9‐1‐1)?
• Reduce spend– After hours RN home visits– Avoid sending RN to patient not at home
• Improve outcomes– Fewer re‐hospitalizations
• Increased referrals from referring agencies?
• Improve patient/customer satisfaction– Referring agency referral source– NCQA Accreditation standards
10/6/2016
8
Home Health is Paying For
• Register patients on their service in our CAD
– Notify them if we respond to the residence
– On‐scene care coordination
• < transport rate
• Provide after hours home visits
– Intervene to prevent HH visit & ED transport
Why would a 3rd Party Payer Pay for us to NOT transport a Patient?
• Reduce spend for unnecessary ambulance transports
• Reduce spend for unnecessary ED visits
• Reduce spend for preventable admissions
• Improve patient experience of care
– HEDIS measures/NCQA
3rd Party Payers are Paying for…
• High utilizer programs– UPMC Community Connect
• Highmark and UPMC Health
– Minnesota Community Paramedics• Medicaid
– Maine Community Paramedics• Medicaid
– Idaho Community Paramedics• Medicaid & SIM CMMI
– Albuquerque Community Paramedics• Patient Education
10/6/2016
9
How 3rd Party Payers are Paying…
• Patient contact fee (Medicaid)
• Capitated rate
– PMPM for population
• All or members “at risk”
Post‐Acute Care Providers
• Contracts for post‐acute care
– Post Acute Analytics
– TrustedCare
– WellMed
– Kindred
How Medicare is Paying…
10/6/2016
10
Economic Models…
• Follow the $$
– Who’s at risk for the cost/spend
• Don’t talk to mid‐level managers
– Perceive this a ‘work’ without reward
– CFO buy in key
Economic Models…
• Direct funding
• Patient contact fees
• Enrollment fees
• Pseudo capitated
• Population based
• Shared savings/risk
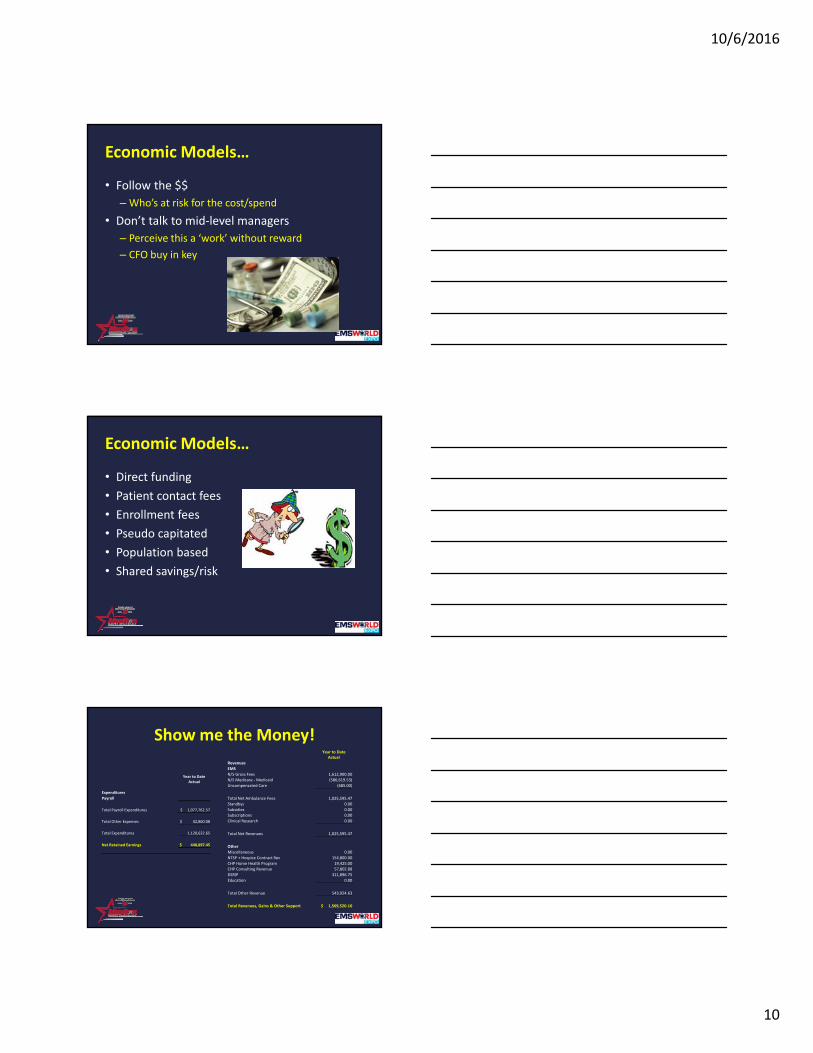
Show me the Money!Year to Date
ActualRevenues
EMS
N/S Gross Fees 1,612,900.00N/S Medicare ‐Medicaid (586,619.53)
Uncompensated Care (685.00)
Total Net Ambulance Fees 1,025,595.47
Standbys 0.00
Subsidies 0.00Subscriptions 0.00
Clinical Research 0.00
Total Net Revenues 1,025,595.47
Other
Miscellaneous 0.00
NTSP + Hospice Contract Rev 154,800.00
CHP Home Health Program 19,425.00CHP Consulting Revenue 57,802.88
DSRIP 311,896.75
Education 0.00
Total Other Revenue 543,924.63
Total Revenues, Gains & Other Support $ 1,569,520.10
Year to DateActual
Expenditures
Payroll
Total Payroll Expenditures $ 1,077,762.57
Total Other Expenses $ 42,860.08
Total Expenditures 1,120,622.65
Net Retained Earnings $ 448,897.45
10/6/2016
11
Customer Messages…
• Hospitals– How can we help improve your readmission rate?
– How can we help improve your HCAHPS scores?
– How can we help with your MSPB?• Especially in pre and post‐acute admissions metric
• As well as length of stay
• Shared‐Risk providers– How can we help reduce your spend on admissions?
– How can we help reduce your spend on Obs admits?
– How can we help improve your HCAHPS scores?
Customer Messages…
• Home Health
– How can we help increase your referral base?
– How can we help reduce your spend for after hours services?
– How can we help prevent you from arriving and no one is home?
Customer Messages…
• Hospice
– How can we help assure the patient’s wishes are met?
– How can we help reduce your spend for ambulance and ED services?
– How can we help prevent voluntary disenrollment's and revocations?
10/6/2016
12
Future of EMS Economic Model
• Supplier to Provider status• Part of a bundled payment• Shift to outcome‐based payments
– Like the rest of healthcare
• Shared risk contracting– Payers, other providers– Part of an ACO (for real)– Capitated fees (happening now)
• Pay for performance– Adherence to clinical bundles– Proven to make a ‘clinical’ difference
• STEMI, Stroke, Trauma, COPD clinical bundles
10: Congress, in consultation with the U.S. Department of Health and Human Services, should identify, evaluate, and implement mechanisms that ensure the inclusion of pre‐hospital care (e.g., emergency medical services) as a seamless component of health care delivery rather than merely a transport mechanism.
http://www.nap.edu/read/23511/chapter/1
Possible mechanisms that might be considered in this process include, but are not limited to:
• Amendment of the Social Security Act such that emergency medical services is identified as a provider type, enabling the establishment of conditions of participation and health and safety standards.
• Modification of CMS’s ambulance fee schedule to better link the quality of pre‐hospital care to reimbursement and health care delivery reform efforts.
• Establishing responsibility, authority, and resources within HHS to ensure that pre‐hospital care is an integral component of health care delivery, not merely a provider of patient transport. The existing Emergency Care Coordination Center could be leveraged as a locus of responsibility and authority (see Recommendation 4) but would need to be appropriately resourced and better positioned within an operational division of HHS to ensure alignment of trauma and emergency care with health delivery improvement and reform efforts.
10/6/2016
13
Medical Direction for MIH‐CP Who’s in charge? Neal J. Richmond, M.D., FACEP
10/6/2016
14
EMS systems transition
Mobile Integrated Healthcare – Community Paramedicine• Faced with some of the same challenges
• Characterized the development of traditional service delivery models
Evolution of our discipline
Focus on operational metrics & performance measures• NFPA 1710 response time standards
• 8‐minutes for ALS (4‐minutes for BLS)
• 2 medics & 2 EMTs on the scene of every ALS level cal
• 60‐seconds to dispatch
• Sophisticated/high performance systems• Dynamic deployment and system status management
• Unit‐hour‐utilization rates (UHUs), total time‐on‐task or drop times
• Extraordinary emphasis on process• How fast do we get there?
• How many does it take to get the job done?
• How many& what kinds of things are on the rig?
The unfortunate reality
Standards upon which performance measures are based• Are on unstable scientific footing
• 8‐minute ALS vs. 4‐minute BLS response time
• Were never realistically validated• Can anybody meet them?
• With what resources and at what costs?
• Most systems are unable to meet them• Take a look at the web
• Yet we continue to chase them• At great operational, political, and financial cost
• Sometimes to the near exclusion of focusing on quality• Ensuring delivery of high quality patient care
10/6/2016
15
Historical perspective
Emergency Medical Service System Act – 1973• Provided funding for a regional approach to prehospital care
• Focus on trauma
• Defined 15 essential elements of an EMS system• Communications, Training, Manpower, Mutual Aid, Transportation,
Accessibility, Facilities, Critical care units, Transfer of care, Consumer participation, Public education, Public safety agencies, Standard medical records, Independent review and evaluation, and Disaster Linkage
• Remarkably, didn’t include Medical Direction and Oversight
excuse me
Limited consensus
Evidence‐based clinical quality measures• Little guidance, authority, political will, interest or resources
• To collect & analyze meaningful data
• Ensure high quality medical care and patient outcome
Excuse me
While we pause for a brief message from the soapbox
10/6/2016
16
For example
How many of us can figure out• Whether an airway is really in place?
• Or what it took to get it there?
• Current unrecognized esophageal intubation rate = 25%
• How many ‘successful’ tubes have prolonged periods of• Hypotension/bradycardia
• Desaturation/hypoventilation
• Aspiration/airway trauma
What happened?
After we got to the cardiac arrest?• Not just how long it took to get there.
• Did we spend 80‐90% of the time on the chest
• Or where there multiple pauses greater than 10‐seconds?
• And did we keep the CPR compression rate in the sweet spot?
And not to belabor the point, but…
For those of us who use mechanical CPR devices• How long does it take to put one of these on?
• Even 1‐pause > 15‐seconds
• Decreases chance of walking out of the hospital alive by 50%
10/6/2016
17
The new frontier of MIH‐CP
Translate EMS from its more traditional role• Public Safety Public Health
• Emergency Medical Transportation Emergency Medical Navigation• Not everyone needs an ambulance
• Not everyone needs an ER
• Can we keep patients out of the revolving door?• Hospital admissions and readmissions
• Decrease unnecessary utilization of 911 and ER resources?
• Decrease costs of healthcare utilization?
Up until now
MIH‐CP measurement & QA also focused on process measures• Admission/readmission avoidance
• Cost reduction• Medicare/ Medicaid
• 3rd‐party payers: Blue Cross/ Blue Shield, Cigna, Humana. Aetna
• Improved 911 and ED resource utilization
• All critically important elements
We have a great opportunity
To get it right from the start this time• And not get stuck going down the rabbit‐hole of process once again
• Operational/financial/administrative metrics & measures
• Critically important• Efficient, effective and sustainable health of our systems
• Something that many systems often, in fact, overlook or ignore
•
10/6/2016
18
But we may miss the boat (again)
If we lose sight of the mission• And forget to keep the patient front and center
• Decreasing costs
• improving 911 resource, ER & hospital utilization
• Decreasing admissions/readmissions
• But we should also directly focus on the patient care itself
May be surrogate measures for quality of patient care
A few questions
Medical Direction and oversight of MIH‐CP programs
? ?
Is there any evidence?
That we benefit our patients• Keeping them out of the hospital (& out of our ambulances)
• Managing their CHF at home• Avoiding readmission within 30‐days
• And not just saving the hospital the readmission penalty from CMS
• Navigating low priority 911 callers with a nurse triage line• Alternate sources of transport or care
• Does their course of disease, quality of life of, or survival outcome actually improve?
10/6/2016
19
Is there a critical role?
EMS Medical Director in MIH‐CIP• Or can we just rely on our partners?
• Primary care/other specialties
• To provide the necessary Medical Direction and Oversight
• Do outside docs have the time, interest or understanding?• To participate in meaningful Quality Assurance
At what point?
Does an MIH client become a 911 patient?• Are our providers appropriately credentialed and trained & QA’d?
• Not just to manage the MIH client
• But to manage clients who cross the abstract & artificial boundary
• From primary or chronic MIH to acute/emergency 911 patient
• Who credentials them?• EMS Medical Director or outside cardiologist or orthopedist
Do contracts and directives suffice?
Between EMS‐MIH systems and primary & specialty care providers
Or should there be protocols for everything we do? • Especially with regard to our providers & patients who may straddle the sometimes blurred or gray border between MIH and 911
10/6/2016
20
How do we navigate the inherent tension?
Between Medical Directors and 911/MIH system Directors• System Directors (Executive Directors, Ops bosses or Chiefs)
• Priority is to sustain & grow the business (not just ensure the quality of care)
• Integrate external physicians into the organization• Who may have their own agendas, business interests & desires to steer patients
• Medical Directors• May have limited training, experience or interest in population health
• Who may not want to have non‐EMS docs involved• Medical Control
• Protocol Development
Dammit, Jim!
And finally
MIH‐CP“Are those same elements that have inhibited the focus on quality in in favor of process in traditional 911 Emergency Medical Services about to have the same effect on MIH that they have had on the growth, development and approach to innovation throughout our discipline so far?”
…Audience says
10/6/2016
21
So, what are the challenges?It’s not rocket science• Chasing ‘holy grail’ of clinical quality & performance measurement
• For as long as we’ve been chasing response times, both not too successfully
• For almost two decades (since 2001)• Alphabet soup of national agencies: NASEMSO, NHTSA and HRSA MCHB • Working to develop a national database• National EMS Information System (NEMSIS)
• Latest evolution is the EMS COMPASS Initiative
• Problem is not so much about creating the perfect dataset
• Than most of us still measure not much of anything• Limited tools, resources or interest
• And so we don’t really know how we’re doing
We can do this
By bringing the same grass roots approach• To Medical Direction, QA, and clinical performance measurement
• That we used to develop these MIH‐Programs from the ground‐up
• We didn’t start with the Triple Aim • And then abstractly theorize 80‐ways to accomplish it
• We identified a need (things that were staring us in the face)• Figured out how to deal with them, largely by trial and error.
• We don’t need the perfect, all encompassing list of things to QA
• Including stuff we may never have the ability to measure• Let alone whether any of this tells us how our patients are doing
A quick story
Defending proposed budget to the Board of Directors• Why devote 1‐2 FTEs to QA’ing cardiac arrests & airways?
• Comprise maybe 1‐2% of entire 911 EMS call volume
• Most of our patients aren’t typically straddling the border of life and death when we find them
• And it’s hard to measure whether or not are interventions are clearly beneficial
• But if we can reduce the rate of unrecognized misplaced tubes
• Decrease the incidence of unrecognized and untreated V‐fib• Ensure we are compressing the chest > 90% of the time
• Then we’ve accomplished a lot First do no harm
10/6/2016
22
Simply stated
Quality is a difficult thing to measure in Medicine• It’s not that easy to figure out that we’ve made someone better
• Clearly, we are going to have to figure out some metrics• If we’re going to get reimbursed by CMS (that’s being worked on)
• Boots on the ground level
• Figure out how to mitigate or at least reduce harm
• If you’re not too sure how to do it
• You don’t have to do everything, • Just start with something
• Another thought from William Osler
…and know that by practice
alone, you can become
expert
Protocols for Mobile Integrated Healthcare
Do we need them and, if so, who should write them?
• Is the whole concept outdated and inapplicable to MIH
•Shouldn’t a well‐trained MIH provider be able to function independently?
MIH program ‘protocols’
Often a hodgepodge of contracts, directives, procedures & training programs• High Utilizer Group (HUG)
• Non‐Adherent HUG (system abuser)
• 911 Nurse Triage
• Congestive Heart Failure readmission avoidance
• Hospice
• Observation admission avoidance
• Home Health Partnerships
10/6/2016
23
Protocols may be beneficial
Not just to manage the MIH patient at home• But also to guide the interaction between the MIH provider and
• The primary care professional or extensivist and
• On‐Line Medical Control
• Manage the interface between MIH and 911• When the client suddenly becomes a patient
• Ensure • Clarity, consistency and quality of care• Accountability of providers• Integrity of the program
Congestive Heart Failure (CHF)
Diuresis and potassium (K+) repletion• Management based on i‐STAT potassium/creatinine, EKG & weight
• Specific indications for treating high and low K+ and 911 transport
Diabetes
Insulin, IV fluids• Management based on i‐STAT glucose, bicarbonate & anion gap
• Including indications for 911 transport
10/6/2016
24
High Utilizer Group (HUG)
Defines • Referral criteria, initial home visit/patient assessment, development of an individualized care plan, scheduled & unscheduled home visits, and what happens when the patient calls p11
Non‐adherent HUGDefines
• Evaluation and designation of Non‐adherent HUG status, what happens with calls to 911, MIH response, management anddisposition, documentation and QA
Protocols are only so good
911 or MIH: they are only the ‘point’ or ‘tip’ of the spear• On the back end
• There’s a sentient human being (MIH or EMS provider) who can use them
• As the foundation for critical thinking and clinical decision making
• But if you think that’s it, you’re gonna miss the boat (again)• Also a need for robust QA
Matt ‘tip of the spear’ Zavadskythrowing the triple aim
patient experience
population health
cost
10/6/2016
25
And the judges say…
4.9Let Jabba have
him
Doug HootenExecutive Director
MedStar
Rob LawrenceExecutive Director
Richmond Ambulance Authority
Brent MyersExecutive DirectorEnvision Death Star
But all is not lost…
10.2
Justin BieberExecutive Director of
All 12‐year old girls on the planet Earth
Alas, I digress
A few MIH case studies
O
Only the pictures have been changed
to protect the innocent
10/6/2016
26
Case #1
68 y/o male with Congestive Heart Failure (CHF) • Past Medical History
• HTN, DM, COPD and CHF 2° to MI
• Several readmissions for CHF in the past year, with two in the last month
Case #1
68 y/o male with Congestive Heart Failure (CHF) • History of present illness
• Last admission presented with complaints of progressive dyspnea on exertion
• Chest‐x‐ray showed signs of significant volume overload
• Echocardiogram reveals an ejection fraction less than half normal EF‐ 27%
• Discharged from the hospital 1‐week ago
• Referred to the CHF readmission avoidance program on discharge
Case #1
68 y/o male with Congestive Heart Failure (CHF) • First MIH visit (1‐week after enrollment)
• Mild increased work of breathing
• Vital signs: BP‐150/90; HR‐96; RR‐20; O2 sat 94%;• Weight ‐ 200 lb (196 @ discharge); lungs clear; 2+ edema;;
• 12‐lead EKG unchanged
• Send to the ER or manage at home?
10/6/2016
27
Case # 1
On‐scene management• Electrolytes & renal function checked with i‐STAT
• Potassium ‐ 2.9 (low)
• Creatinine ‐ 1.6 (mildly elevated)
• Management & disposition• 4 lb wt. gain
• Doubled Lasix dose according to protocol from from 40 mg bid ‐ 80 mg bid
• Increased the potassium by 50% from 40mEq ‐ 60mEq/day
• Discussed with primary care physician and scheduled for follow‐up in 48‐hours
Case # 1
Follow‐up• Doing well at time of next visits
• MIH (24‐hours)
• Primary care provider (48‐hours)
• Hospital readmission avoided• No in‐hospital complications pneumonia, UTI)
• Estimated cost reduction to Medicare $10k for admission
• No hospital readmission penalty
• MIH program reimbursed under Medicaid waiver program
Case #2
54 y/o male with one 911 call and ED visit each month• Past Medical History
• HTN, IDDM, chronic pancreatitis, chronic diarrhea, anorexia,
• Psychiatric illness: depression/schizoaffective disorder• Medications: Antidepressant (Elavil) and Atypical antipsychotic (Clozaril)
• Non‐compliant with all scheduled hospital clinic appointments for 2‐years
10/6/2016
28
Case #2
1st MIH enrollment visit 2‐days after discharge• Patient assessment
• Not taking medications prescribed upon discharge from the hospital
• Still not eating well and has chronic diarrhea
Case #2
On‐scene management• Electrolytes and renal function checked with i‐STAT
• Potassium ‐ 2.8 (low)
• Renal function – creatinine also low
• Management & disposition• Patient is provided bus pass and clinic appointment for the next day
Case #2
What happens next• Call to 911 two‐days later
• Ambulance and MIH unit show up on‐scene
• Patient never followed‐up with clinic as scheduled
• MIH provider unable to perform repeat chemistry i‐STAT
• No 12‐lead EKG done
• Transport refused
• Patient signed out of high utilizer program
• Repeat call to 911 three‐days later• Patient found by EMS in cardiac arrest
• Resuscitative efforts unsuccessful
10/6/2016
29
Case #2
Sentinel event/QA review• Point‐of‐care testing with i‐STAT not formally protocolized
• High utilizers
• Within MIH scope of practice• CHF and diabetes protocols for readmission avoidance• Potassium not below threshold for transport in CHF protocol (K < 2.5)
• Ongoing reason for further K+ depletion• Chronic diarrhea• Low caloric intake (possible magnesium deficiency ‐malnutrition)
• Also demonstrated by low renal function
• No clear protocol, but requires understanding• Differential diagnosis of what causes low potassium• Clinical manifestations of hypokalemia
• Cardiotoxic effects (dysrhythmias)• Muscle weakness (respiratory failure cardiac arrest)
• Bottom line • Nice to have numbers, but you still have to do something about them• Illustrates need for consistent QA
Case #3
50 y/o female with Congestive heart Failure• Past Medical History
• HTN, breast CA, and CHF 2° to MI
Case #3
50 y/o female with Congestive Heart Failure
•History of present illness• Hospitalized 1‐week ago with severe CHF exacerbation• Patient admits to no current cocaine use
• 4+ pitting edema to both legs and anasarca to both thighs/lower abdomen
• 12‐leak EKG reveals no new or acute MI
• Chest x‐ray showed significant pulmonary congestion
• Discharged home 3‐days later after aggressive diuresis regimen
• Referred to MIH CHF readmission avoidance program
10/6/2016
30
Case #3
50 y/o female with Congestive Heart Failure• 1st MIH enrollment visit one‐week later
• Patient appears noticeably dypneic after getting up to answer the door• States she called 1°‐care physician last night
• Told her to increase her Lasix from bid to tid, but she’s not sure which pill is Lasix
• Last night she had mac & cheese for dinner
• Gained 4 lbs. over the past 4‐days• Also notes trouble sleeping since getting home from the hospital
• ‘Feels like she’s going to suffocate’ at night (though still uses same # pillows)
• States she was getting ready to call 911• Vital signs notable for RR‐24, but O2 sat = 98%
Case #3
On‐scene management• Electrolytes and renal function checked with i‐STAT
• Potassium ‐ 3.5 (low normal);
• Creatinine ‐ normal
• Management & disposition• Followed protocol and discussed with 1° care physician
• Doubled up Lasix for 2‐days
• Went over medications and need for dietary compliance
• Arranged out‐patient follow‐up in 48‐hours
Case #3
What happens next• Call to 911 morning of scheduled out‐patient follow‐up visit
• Patient found in bed by EMS in cardiac arrest
• Resuscitative efforts unsuccessful
10/6/2016
31
Case #3
Sentinel event/QA review• Exact cause of arrest undetermined
• Significance of complaints of severe orthopnea/pnd• Very early findings for CHF decompensation
• As peripheral volume redistributed centrally
• What would an ER doc have done with this patient?
• Bottom line• it’s not just about the numbers
A few lessons learned
Is there any evidence?
That we benefit our patients• Keeping them out of the hospital (& out of our ambulances)
• Does their course of disease, quality of life of, or survival outcome actually improve?
• The jury is out, but it is our responsibility to collect this data
• While clinical quality is a difficult thing to measure
• We can least initially focus on avoiding harm
• We don’t need to wait for the perfect, all‐inclusive list of measures
• Just pick a couple of things
10/6/2016
32
Is there a critical role?
EMS Medical Director in MIH‐CIP• Or can we just rely on our partners?• There is a critical need for developing robust partnerships
• With primary and specialty care providers
• These will likely lead to • Innovative programs and protocols • Opportunities for enhanced patient care• Meaningful sustainability for our systems
• But most of these colleagues in other disciplines have full‐time jobs• May not have the time or resources to focus on MIH QA
• The EMS‐MIH Medical Director plays a central role• Coordinating and Integrating these diverse disciplines
Do protocols serve a purpose?
Do contracts and directive suffice?• At any point, an MIH client may become a 911 patient
• Protocols ensure clarity, consistency and accountability
• They also provide the basis for appropriate credentialing/ training
• Functions that may be effectively designed or coordinated by the EMS Medical Director
How do we navigate the inherent tension?
Between Medical Directors and 911/MIH system Directors• Medical Direction and Oversight should be at the table
• Operational, financial and political decision making
• Ensures appropriate prioritization and mission critical focus
10/6/2016
33
Welcome!
Anne Montera & John Clark
Credentialing and Education
October 5, 2016
© 2016 The Paramedic Foundation. All Rights Reserved.
National Certification Exam
• History
• Process
• Collaboration
• Statistics
10/6/2016
34
© 2016 The Paramedic Foundation. All Rights Reserved.
National Certification Exam
Detailed Content Outline
1. Community Based Needs
2. Interdisciplinary Collaboration
3. Patient Centric Care
4. Preventative Care and Education
© 2016 The Paramedic Foundation. All Rights Reserved.
National Curriculum
• History
• 4.0 Framework
• Statistics
© 2016 The Paramedic Foundation. All Rights Reserved.
New Framework
1. Introduction to CP
2. Systems of Care
3. Social Determinates of Health
4. CP Operations
5. CP Interventions
6. Developing Cultural Competence
7. Personal Safety and Wellness
8. Chronic Disease Management
9. Mental Health
10. Documentation
11. Outreach and Education
12. Older Adult
10/6/2016
35
© 2016 The Paramedic Foundation. All Rights Reserved.
Continuing Education & Accreditation
• State by State
• Core Competencies
• Opportunities
Questions?
Anne [email protected]
970‐471‐3501
John [email protected]‐368‐4970
105Copyright © 2015. Infor. All Rights Reserved. www.infor.comCopyright © 2015. Infor. All Rights Reserved. www.infor.com 105
Introducing Infor Healthcare
September 27, 2016
10/6/2016
36
106Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Discussion topics
Your organization’s 3-5 year strategy and objectives
Infor: Who we are
How Infor helps drive transformation in healthcare
Next steps
107Copyright © 2015. Infor. All Rights Reserved. www.infor.com
3rd largestprivate tech company
14,000employees
9,000engineers
$2.8brevenue
$800mfree cash flow
12quarters of double digit license growth
$2.5b invested capital
1,700new employees
$400m In R&D
108Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Our strategySpecialized, deep industry suite
Architected for speed, change & choice
Science-driven, real-time analytical insights
We think about industries differently than anyone else.”
CHARLES PHILLIPS, CEO, INFOR
10/6/2016
37
109Copyright © 2015. Infor. All Rights Reserved. www.infor.com
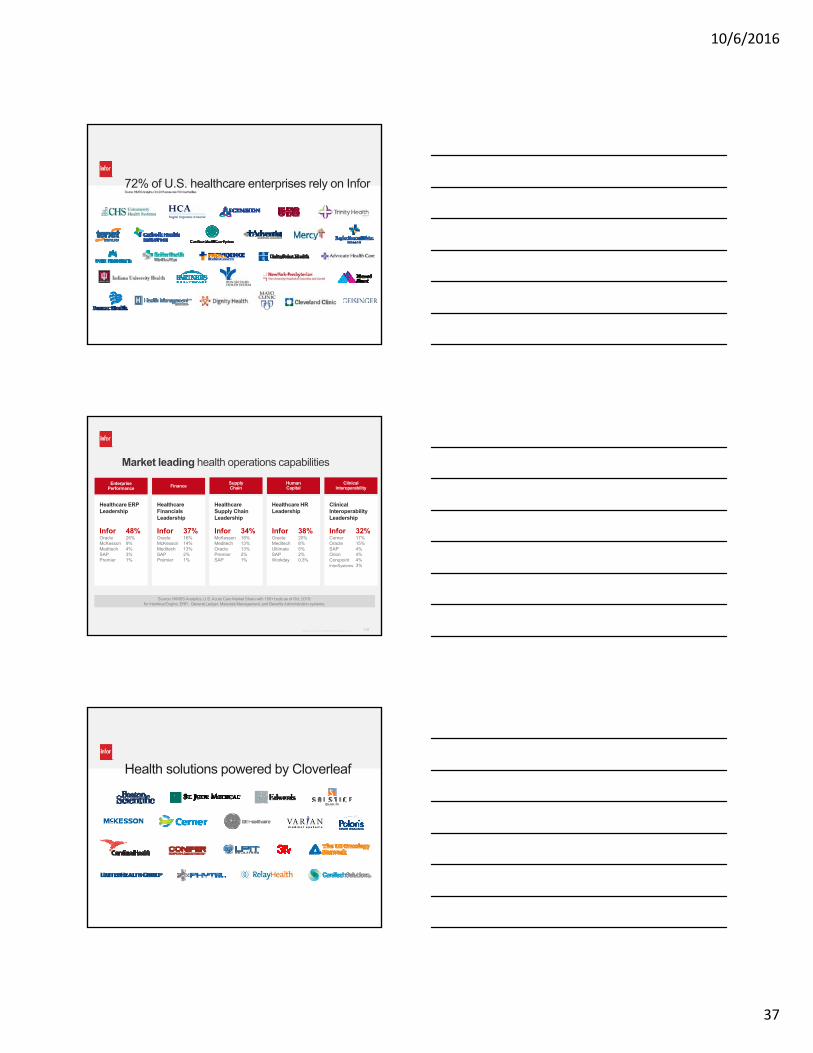
72% of U.S. healthcare enterprises rely on InforSource: HIMSS Analytics, Oct. 2015 acute-care 150+ bed facilities
110Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Market leading health operations capabilities
Enterprise Performance
Healthcare ERP Leadership
Infor 48%Oracle 26%McKesson 9%Meditech 4%SAP 3%Premier 1%
Healthcare ERP Leadership
Infor 48%Oracle 26%McKesson 9%Meditech 4%SAP 3%Premier 1%
Finance
Healthcare Financials Leadership
Infor 37%Oracle 16%McKesson 14%Meditech 13%SAP 2%Premier 1%
Healthcare Financials Leadership
Infor 37%Oracle 16%McKesson 14%Meditech 13%SAP 2%Premier 1%
SupplyChain
Healthcare Supply Chain Leadership
Infor 34%McKesson 18%Meditech 13%Oracle 13%Premier 2%SAP 1%
Healthcare Supply Chain Leadership
Infor 34%McKesson 18%Meditech 13%Oracle 13%Premier 2%SAP 1%
Human Capital
Healthcare HR Leadership
Infor 38%Oracle 20%Meditech 8%Ultimate 5%SAP 2%Workday 0.3%
Healthcare HR Leadership
Infor 38%Oracle 20%Meditech 8%Ultimate 5%SAP 2%Workday 0.3%
Clinical Interoperability
Clinical Interoperability Leadership
Infor 32%Cerner 17%Oracle 15%SAP 4%Orion 4%Corepoint 4%InterSystems 3%
Clinical Interoperability Leadership
Infor 32%Cerner 17%Oracle 15%SAP 4%Orion 4%Corepoint 4%InterSystems 3%
Source: HIMSS Analytics, U.S. Acute Care Market Share with 150+ beds as of Oct. 2015: for Interface Engine, ERP, General Ledger, Materials Management, and Benefits Administration systems.
111Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Health solutions powered by Cloverleaf
10/6/2016
38
112Copyright © 2015. Infor. All Rights Reserved. www.infor.com
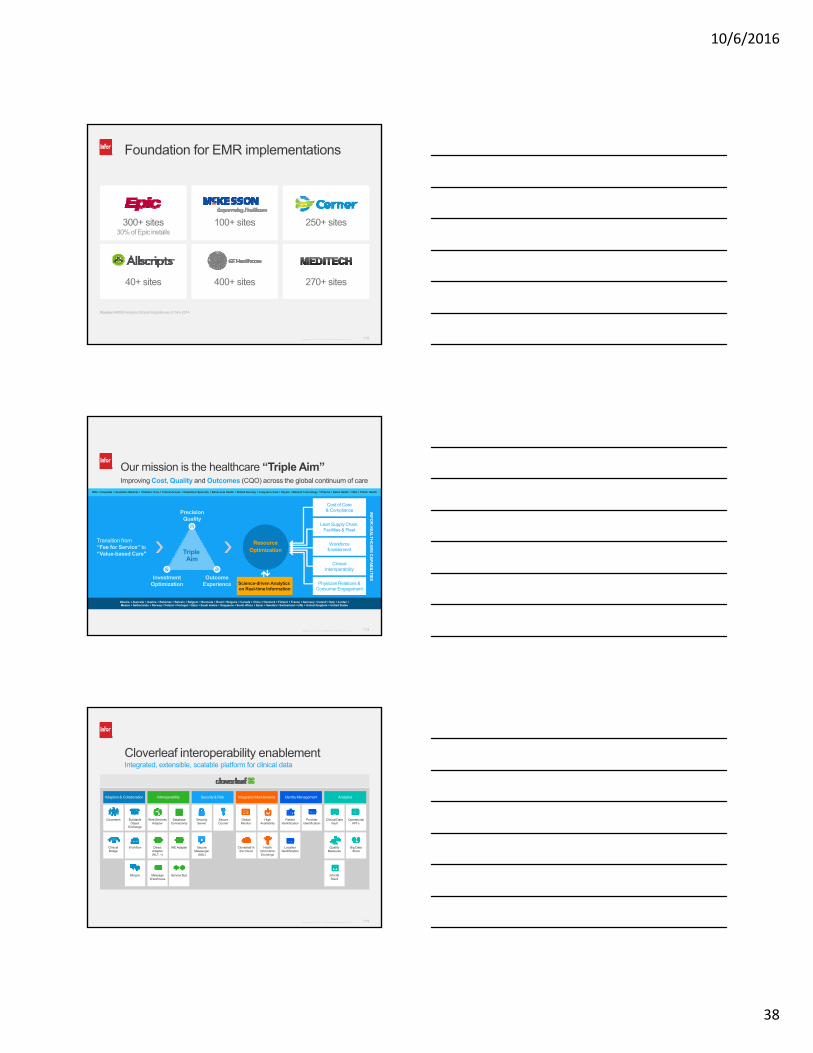
Foundation for EMR implementations
300+ sites30% of Epic installs
250+ sites
270+ sites400+ sites40+ sites
Source: HIMSS Analytics Clinical Integration as of Nov 2014
100+ sites
113Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Improving Cost, Quality and Outcomes (CQO) across the global continuum of care
Our mission is the healthcare “Triple Aim”
Transition from “Fee for Service” to “Value-based Care" Triple
Aim
PrecisionQuality
OutcomeExperience
InvestmentOptimization
ResourceOptimization
Science-driven Analytics on Real-time Information
Cost of Care& Compliance
Lean Supply Chain,Facilities & Fleet
WorkforceEnablement
ClinicalInteroperability
Physician Relations & Consumer Engagement
INF
OR
HE
AL
TH
CA
RE
CA
PA
BIL
ITIE
S
IDNs Hospitals Academic Medical Pediatric Care Critical Access Outpatient Specialty Behavioral Health Skilled Nursing Long-term Care Payers Medical Technology Pharma Retail Health HIEs Public Health
Albania Australia Austria Bahamas Bahrain Belgium Bermuda Brazil Bulgaria Canada China Denmark Finland France Germany Ireland Italy Jordan Mexico Netherlands Norway Poland Portugal Qatar Saudi Arabia Singapore South Africa Spain Sweden Switzerland UAE United Kingdom United States
114Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Cloverleaf interoperability enablement
Adaptors & Collaboration Interoperability Security & Risk Integration Maintenance Identity Management Analytics
Integrated, extensible, scalable platform for clinical data
ClinicalBridge
Workflow
Clovertech BuildableObject
Exchange
Ming.le
DirectAdapter(HL7, +)
IHE Adapter
MessageWarehouse
Web ServicesAdapter
DatabaseConnectivity
Service Bus
SecureMessenger
(SSL)
Security Server
SecureCourier
Cloverleaf in the Cloud
HealthInformationExchange
GlobalMonitor
High Availability
LocationIdentification
PatientIdentification
ProviderIdentification
Clinical Data Vault
OperationalKPI’s
QualityMeasures
Big DataStore
Infor BIStack

10/6/2016
39
115Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Leverage the Health Information Exchange
EmployedPCP’s
Patient Identity Management Tool
HIESemantic Clinic Data/Tags Providers, Populations
Clinical Messaging - Exports Criteria Specific Content
Care ManagementPatient Engagement Platform
Long-term Integrated Technology Topology
DischargeManagement
CallCenter
Care ModelsPatientPortal
ClinicalDisease
Repository
CommunityMedical Group
Payer ClaimsData
Labs eRx HospitalsSpecialtyClinics
Mobile Integrated Healthcare
ACO
116Copyright © 2015. Infor. All Rights Reserved. www.infor.com
Hook & LoopUser-centered design process
Design with mobile in mind
Standardization
Accessible & inclusive
User groups
Digital transformation services
Dynamic Science LabsLarge value proposition
Big Data challenges
Requirements gathering
Value measurement
Self-learning
Endless test/control
Infor LabsDevOps
Reference architecture
Cloud operations
Information security office
Performance benchmark center
Global demo environment
Infor capabilities go beyond software
117Copyright © 2015. Infor. All Rights Reserved. www.infor.com
+
+
+
+
Today
Complexity & inconsistency
Misalignment
Information silos
Tomorrow
Data-drivenbest practices
Collaboration & accountability
Unrivalled integration & engagement
People and systems working together in support of cost effective, quality outcomes
Transforming how healthcare is delivered
QualityCost
Outcomes
10/6/2016
40
118Copyright © 2015. Infor. All Rights Reserved. www.infor.com
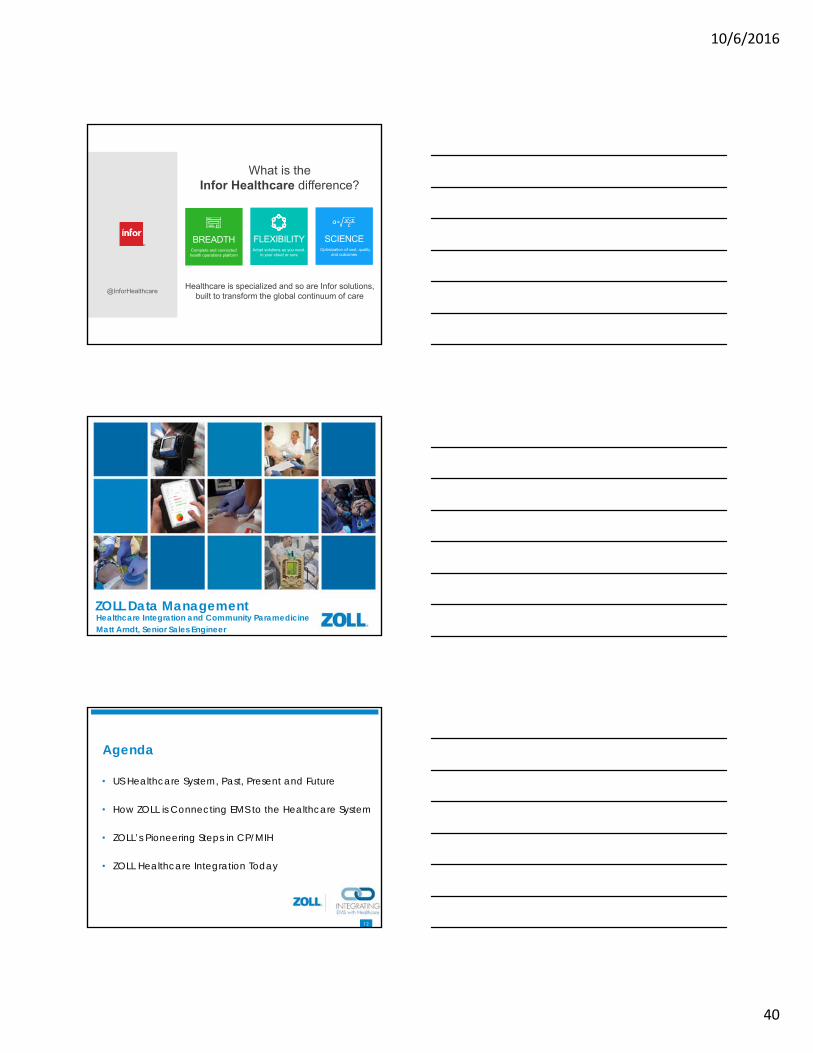
SCIENCEOptimization of cost, quality
and outcomes
FLEXIBILITY Adopt solutions as you need,
in your cloud or ours
BREADTH Complete and connected health operations platform
@InforHealthcare
What is the Infor Healthcare difference?
Healthcare is specialized and so are Infor solutions, built to transform the global continuum of care
119ZOLL Medical 11
ZOLL Data ManagementHealthcare Integration and Community ParamedicineMatt Arndt, Senior Sales Engineer
120ZOLL Medical 12
Agenda
• US Healthcare System, Past, Present and Future
• How ZOLL is Connecting EMS to the Healthcare System
• ZOLL’s Pioneering Steps in CP/MIH
• ZOLL Healthcare Integration Today
10/6/2016
41
121ZOLL Medical 12
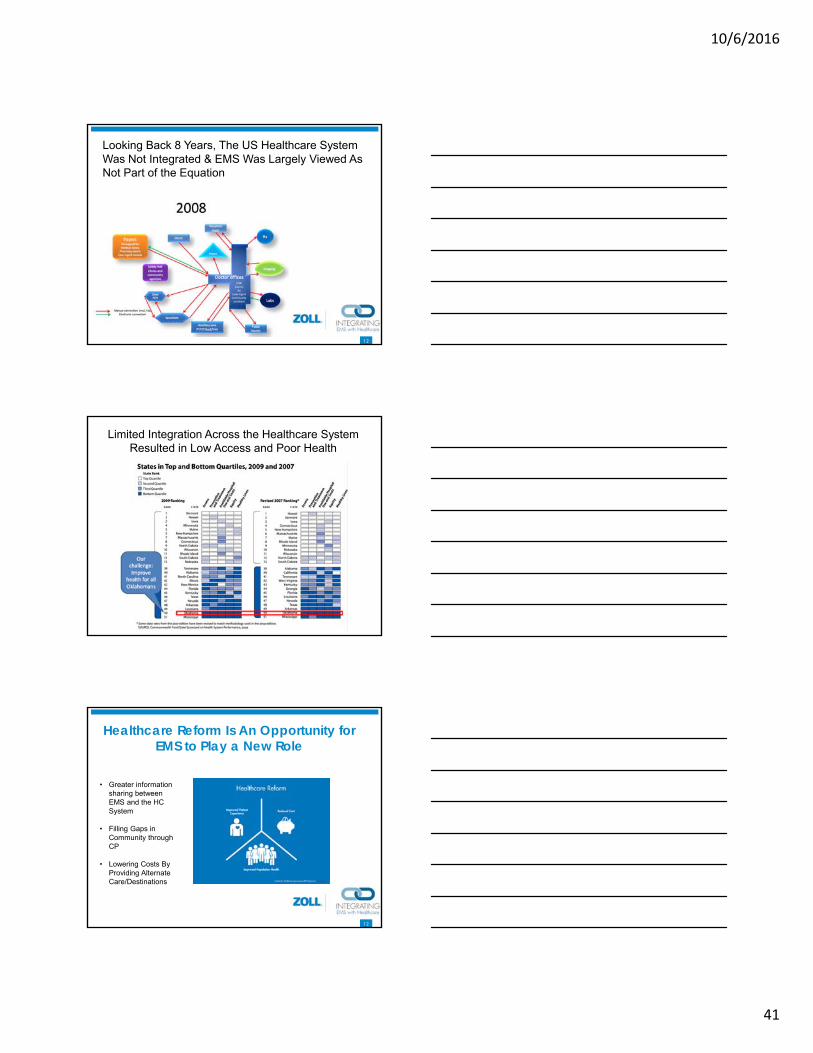
Looking Back 8 Years, The US Healthcare System Was Not Integrated & EMS Was Largely Viewed As Not Part of the Equation
Limited Integration Across the Healthcare System Resulted in Low Access and Poor Health
123ZOLL Medical 12
Healthcare ReformHealthcare Reform Is An Opportunity for EMS to Play a New Role
• Greater information sharing between EMS and the HC System
• Filling Gaps in Community through CP
• Lowering Costs By Providing Alternate Care/Destinations
10/6/2016
42
124ZOLL Medical 124
Key Terms for Healthcare Integration• HL7 means Health Level 7
• International standards body for healthcare data and data exchange
• NEMSIS V3 is now HL7 “approved”• Translated: We Speak The Language
Now• EMS more advanced than healthcare
in general because of NEMSIS• HIE – Health(care) Information Exchange
• Mobilization of healthcare information electronically across organizations within a region or community
125ZOLL Medical 12
Goals of an HIE?
Facilitate access and retrieval of health dataWhich helps to provide ________ care
• Faster• Safer• Efficient
• Savings in the Millions locally• Patient centered
U.S. Healthcare System Today, EMS is Still On the Outside, But That is Changing
10/6/2016
43
Healthcare ReformZOLL Healthcare Exchange Solution
• Break through the brick wall and connect your EMS operation with the greater healthcare system
• Connect with either your local HIE or Hospital partners or both!
• Share patient data from ZOLL RescueNet ePCR with your partners
Healthcare ReformMultiple Customers are Already Connected
• Hospital & HIE Connections Are Live today
• Connect with either your local HIE or Hospital partners or both!
129ZOLL Medical 12
Patient Versus Incident
• Most of healthcare is patient centric• EMS tends to be incident centric
• We don’t identify patients first, the rest of healthcare tends to do that
• Increased likelihood of duplicates• Not a showstopper, but needs to be understood
and managed
10/6/2016
44
130ZOLL Medical 130
Why Field EMS Should Care?
• Reminder of the HIE goals
• Times when you don’t know anything about the patient
• When you want to know more about the patient
Integrated EMS Service Example
• Oklahoma City and Tulsa OK• 170,000 responses, 100+ ambulances, 500
providers
• Real Benefit of Integration
132ZOLL Medical 13
HC Reform Is Only Making Integration More Essential
• As the payment landscape changes, integrations like this will become more important.• Physicians – will be graded on the health of their
population of patients• Hospitals – 90 day re-admits and other value
based payment models• ACOs – they HAVE to have integrated data in
order to provide the info that will be required of them to get their reimbursement
10/6/2016
45
133ZOLL Medical 133
To Learn More about EMSA’s EMS Integration Experience
Frank GreshCIOEMSA(405) [email protected]
134ZOLL Medical 13
ZOLL Has A Solution for Integrating EMS with the Healthcare System
To Learn More Go To https://www.zolldata.com/HL7-for-ems/
ZOLL EMS Mobile Health For Your CP / MIH ProgramZOLL EMS Mobile Health For Your CP / MIH Program
10/6/2016
46
136ZOLL Medical 136
EMS Mobile HealthDIFFERENTIATOR
EMS Mobile Health focuses on patient care over time instead of an event-based approach to patient care.
• Many Visits, One Record—A Community Paramedicine First
• A Guided Path to Better Health Outcomes
• Spend More Time with Patients and Less On Documentation
A Guided Path to Better Health Outcomes
137ZOLL Medical 13
Configure the system to meet the specific needs of your CP/MIH program
EMS Mobile Health
A Guided Path to Better Health Outcomes
ADMINISTRATION
138ZOLL Medical 13
Fully document each patient visit and all relevant issues such as medications, vitals, labs etc.
EMS Mobile Health
A Guided Path to Better Health Outcomes
DOCUMENT A VISIT
10/6/2016
47
139ZOLL Medical 13
Quickly conduct a medication inventory to help catch errors and ensure the patient is taking what they should be
EMS Mobile Health
A Guided Path to Better Health Outcomes
MEDICATION INVENTORY
140ZOLL Medical 14
• ZOLL’s EMS Mobile Health will fit into the broader healthcare environment• We’re following medical record standards – not
just ePCR standards• Integrating to other healthcare systems via HL7• We’re building healthcare standards into the
product from the beginning (ICD-10, RxNorm, SNOMED, etc.)
EMS Mobile Health
A Guided Path to Better Health Outcomes
DESIGNED FOR INTEGRATION WITH HEALTHCARE
141ZOLL Medical 14
• Easily activated• Product resides in a SaaS environment
• No expensive servers to purchase• No IT staff to support it
• Integration• Product will be integrated with scheduling, billing, ePCR,
CAD, monitors, HIEs, analytics, etc.• Supports a wide range of devices
• Works on laptops, tablets, phones, etc.• Just needs an Internet connection
EMS Mobile Health
A Guided Path to Better Health Outcomes
EASY UTILIZATION
10/6/2016
48
142ZOLL Medical 14
• ZOLL understands CP/MIH is an entirely new business model• Our solution is specifically designed to support CP• The system is patient-based – not incident-based• Rather than forcing CP/MIH into our existing
ePCR product, we built it from the ground up in partnership with key thought leaders
EMS Mobile Health
A Guided Path to Better Health Outcomes
ZOLL’S CP/MIH VISION
143ZOLL Medical 14
REMSA• Elaine Messerli BSN RN• Clinical Operations
Manager• Community Health Program• 450 Edison Way• Reno NV 89502• Direct: 775-353-0755
Before we started using EMS Mobile Health, our community paramedicswere seeing about 6 patients a day and then taking a lot of informationback to the office and struggling to get the charts done by the end of theshift.
With EMS Mobile Health, we can add up to 2 to 4 patient visits aday because we can chart at the bedside. A paramedic can now see asmany as 8 to 10 patients per day.”
Jake Beck, Community Paramedic Clinical Coordinator,REMSA, Nevada
144ZOLL Medical 14
Golder Ranch Fire District, Tucson, AZ• Live since March 1st, 2015• Program Type: Community Paramedicine• Key Quote: Joshua Hurguy “Our initial plan was to use ZOLL’s
ePCR product to support our CP/MIH program. However, we quickly learned that using an incident based product was not sustainable and appropriate for CP/MIH. I highly recommend ZOLL’s patient based EMS Mobile Health product to anybody looking to launch this level of service in their community.”
• Reference Contact: Joshua Hurguy, Battalion Chief - EMS
Golder Ranch Fire District
3885 East Golder Ranch Drive
Tucson, Arizona 85739
(520) 825-5920 Office
10/6/2016
49
145ZOLL Medical 14
Medstar, Clinton Township, MI• Program Type: Mobile Integrated Health – Hospital
Readmission Reduction• Key Quote: Kolby Miller, Within the course of the pilot, we will be
able to provide an analysis of the impact of our Mobile Health Paramedics on patient’s health status and frequency of emergency department utilization and subsequent readmissions, Miller said. “Along the way, we expect to provide very valuable services, with a healthy dose of individualized care and compassion for all of the patients in the program.”
• Reference Contact: Kolby Miller
Chief Executive Officer
Medstar, Inc.
380 North Gratiot, Clinton Township, MI 48036
586-468-6510
146ZOLL Medical 14
Complete EMS Enterprise Resource Planning One Stop Integration with the Healthcare System
Communications Center
Patient Care
HR & Finance
Fleet & Safety
ImageTrend Community Health™
Integrated documentation Patient‐centric Records Data Analysis
10/6/2016
50
Community Assessment using Impact™ Scores
ImageTrend Program Management
ImageTrend’s Patient Centric Record
10/6/2016
51
ImageTrend’s Patient Centric Timeline
ImageTrend Worksheets
ImageTrend Health Information Hub™
10/6/2016
52
Value of i-STAT® Systemin EMS
Nicole Bodine, Product Manager
047161 Rev A. 09/2016
Purpose
• Benefits of Point of Care Testing (POCT)
• i-STAT Introduction• How i-STAT fits into EMS
Space
Value of Point of Care Testing (POCT)
Enhance patient assessment in the out-of-hospital setting
• Allows the provider to gain objective information at a patient’s side rather than waiting for blood to be sent to a hospital’s lab for results
• Potential to speed emergency department decision-making
• Can change pre-hospital care based on data from point of care test
• Early disease recognition
Improve patient outcomes by ensuring the right patient receives the right care at the right time and in the right setting.
10/6/2016
53
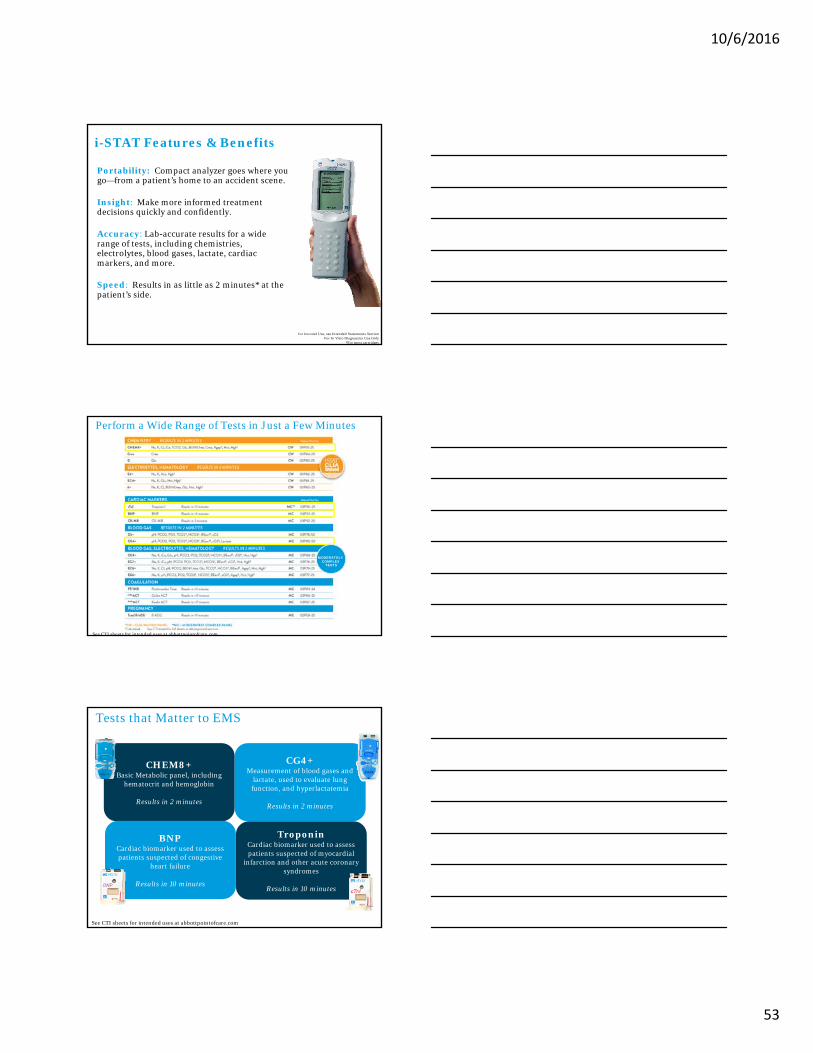
i-STAT Features & Benefits
Portability: Compact analyzer goes where you go—from a patient’s home to an accident scene.
Insight: Make more informed treatment decisions quickly and confidently.
Accuracy: Lab-accurate results for a wide range of tests, including chemistries, electrolytes, blood gases, lactate, cardiac markers, and more.
Speed: Results in as little as 2 minutes* at the patient’s side.
For Intended Use, see Intended Statements SectionFor In Vitro Diagnostics Use Only
*For most cartridges
Perform a Wide Range of Tests in Just a Few Minutes
See CTI sheets for intended uses at abbottpointofcare.com
MODERATELYCOMPLEX
TESTS
Tests that Matter to EMS
For Intended Use, see Intended Statements SectionFor In Vitro Diagnostics Use Only
Menu
CHEM8+Basic Metabolic panel, including
hematocrit and hemoglobin
Results in 2 minutes
CG4+Measurement of blood gases and
lactate, used to evaluate lung function, and hyperlactatemia
Results in 2 minutes
TroponinCardiac biomarker used to assess patients suspected of myocardial
infarction and other acute coronary syndromes
Results in 10 minutes
BNPCardiac biomarker used to assess patients suspected of congestive
heart failure
Results in 10 minutes
See CTI sheets for intended uses at abbottpointofcare.com
10/6/2016
54
Lab-Quality Results in 3 Easy Steps
STEP 1Fill cartridge with 2-3 drops of fresh whole
blood
STEP 2Insert cartridge into
i-STAT
STEP 3View the results in
minutes on the i-STAT screen
Current i-STAT Uses in EMS
Emergency Medical Care
Mobile Integrated Healthcare-Community Paramedicine(MIH-CP)
Remote Care & Telehealth
i-STAT Across Healthcare
Emergency Department
Urgent Care
Long Term Care
Ambulatory Surgery Centers
Dermatology
EMS
Oncology
NICU
Critical Care/ICU
Primary Care
Government/Military
Radiology Cardiology
10/6/2016
55
Stop by Booth 1252
RESPONSIVE INNOVATIONEMS World Expo 2016
MIH-CP Technology Panel
10/6/2016
56
Hello
Communications
“The single biggest problem in communication is the illusion that it has taken place.”
- George Bernard Shaw
Responsive Innovation:
Mobile Telemedicine
Disruptive TechnologyResponsive Innovation
10/6/2016
57
Responsive Innovation in EMS
VERSION UPDATE: Healthcare 3.0 ~ EMS 3.0
The Revolution in EMS Care
Promoting Innovation in Emergency Medical Services
Core Purpose:To improve the health and well being of the public at large, by providing Responsive Innovation for public safety responders and care providers.
10/6/2016
58
Mobile Telemedicine
HIPAA-Secure multi-media messaging and live streaming video
The future of connected care is already in your hands.
Enhanced Decision Support
• Stroke • Trauma • Burns• 12-Leads
Document
• CQI
• Training
• Legal
• Refusals
Real-time situational awareness
• MCI Triage
• Disaster Coordination
• Group Messaging
• Document Geo tag
10/6/2016
59
Telemedicine Consults
• Mobile Integrated Healthcare
• Community Paramedicine
NEW!
“I can do a more thorough evaluation, make a better diagnosis, provide better care, and better answer the question, ‘What do we need to do for this patient?’”
-Dr Dan Godbee, Medical Dir. E-BR EMS
10/6/2016
60
Takeaways:• Change is all around us
• Communicate in new and better ways
• Embrace Responsive Innovation
Curt Bashford201.313.7075 [email protected]
ResponsiveInnovation.com
Get connected.get the Whitepaper• Learn more
• Share ideas • See a demo• Get a free trial
Visit Booth 1339
T H E F U T U R E O F H E A L T H C A R E C O N N E C T I V I T Y
Healthcare Connected
Improve Community Health Through the Power of Data
10/6/2016
61
A few questions…
Healthcare 2017 and beyond…
What we do know…

10/6/2016
62
A vision for success

















