NHS Improving Quality Improving the Physical health care of people with mental ill health: Cardiovascular health of people with serious mental illness National Learning Network Event Wednesday 29 th April 2015
Transcript
NHS Improving Quality
Improving the Physical health care of people with mental ill health:
Cardiovascular health of people with serious mental illness
National Learning Network Event
Wednesday 29th April 2015
Welcome and Introduction
Steve Fairman
Managing Director (Interim)
NHS Improving Quality
Housekeeping
• There will be no fire alarm test today. If the fire alarm does sound, please make your way to the front of the building where hotel staff will direct you.
• Toilets are located near the registration desk
• Please remember to turn off your mobile phone
• Follow us on Twitter @nhsiq#CVDSMI
Improvement Programmes
• Domain 1 – Living Longer Lives
• Domain 2 – Long Term Conditions
• Domain 3 – 7 Day services & Acute
• Domain 4 – Patient Experience
• Domain 5 – Patient Safety
Living Longer LivesHilary Walker
• ‘Practically universal’ use of IPC sleeves in stroke units across England
• 97% of CCGs using the GRASP suite of audit tools or alternative (2 new tools COPD and HF) launched in-year
• 8 pilot sites preventing heart problems in patients with diabetic foot ulcers
• Successful breathlessness symposium and 3 pilot sites supported to test new models of care
• Four pilot sites improving the physical health of people with serious mental illness; 200 people attending learning event
CVD SMI Pilot Project
CVD Matters: Setting the Scene
Huon Gray
National Clinical Director
Cardiac
“CVD matters: setting the scene”
Huon GrayNational Clinical Director (Cardiac), NHS England
Consultant Cardiologist, University Hospital of Southampton
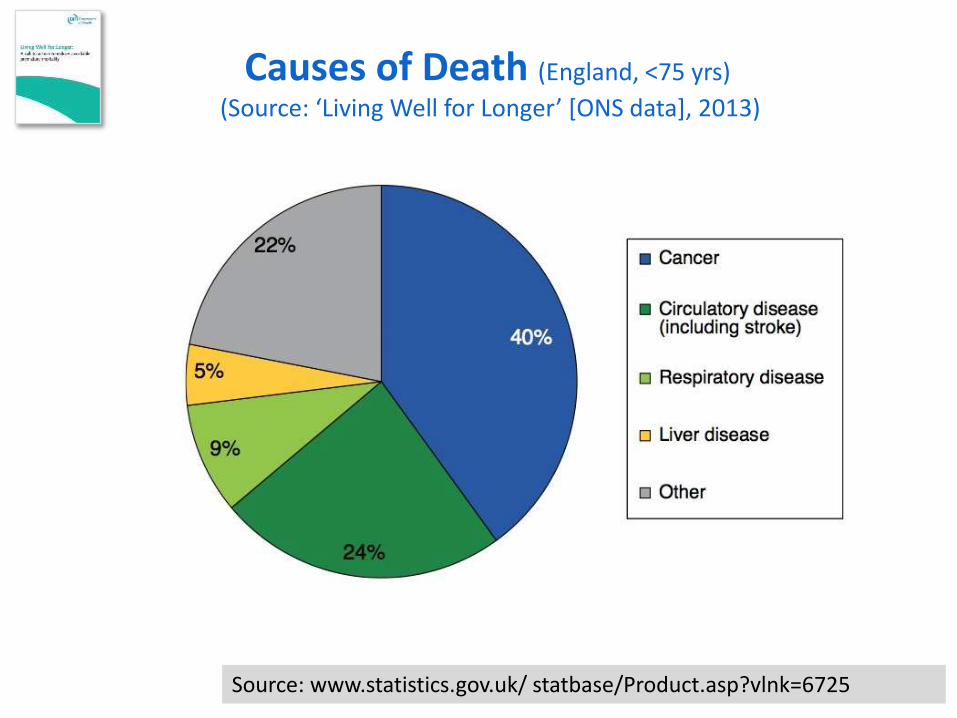
(Source: ‘Living Well for Longer’ [ONS data], 2013)
CVD………..
• 200k deaths pa (1:3 of all)
• 4.9m adults have CVD (11.7% of population)
• 1.4m hospital admissions in 2010/11• 65% were patients under 75 yrs
• >50% were emergencies
• CVD costs NHS & UK economy £30bn pa.
• Prevalence increases with deprivation - Inequalities
“Services for the prevention of CV Disease”
NICE Commissioning Guide 45. March 2012
Deaths by Disease & Deprivation (England <75 yrs)
Global Burden of Disease Study. Lancet 2013;381:997-1020
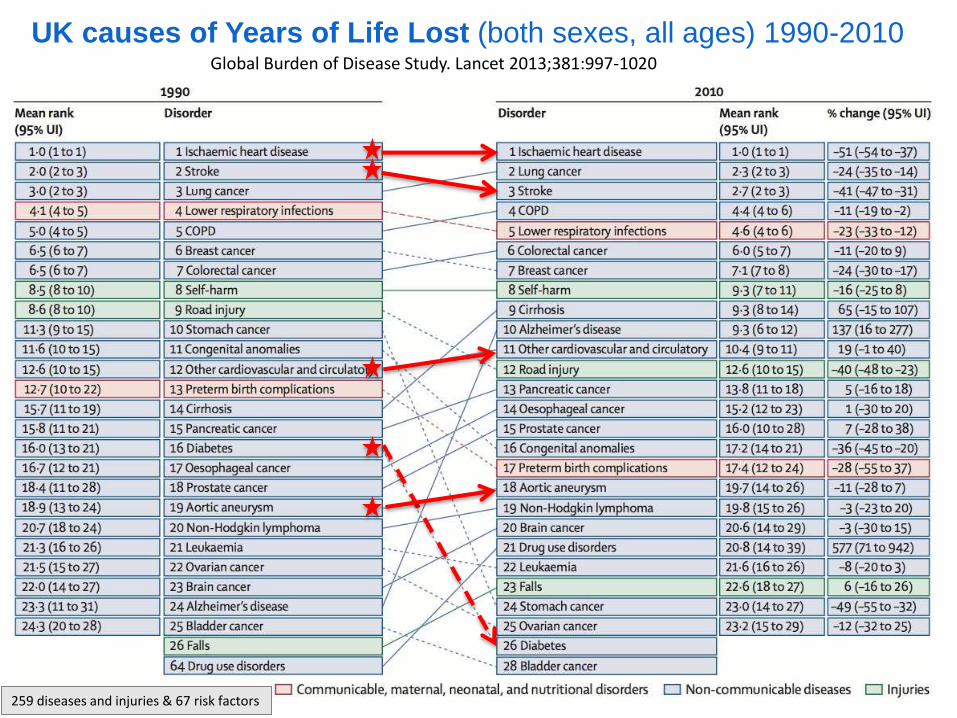
UK causes of Years of Life Lost (both sexes, all ages) 1990-2010
Global Burden of Disease Study. Lancet 2013;381:997-1020
UK causes of Years of Life Lost (both sexes, all ages) 1990-2010
259 diseases and injuries & 67 risk factors
Global Burden of Disease Study. Lancet 2013;381:997-1020
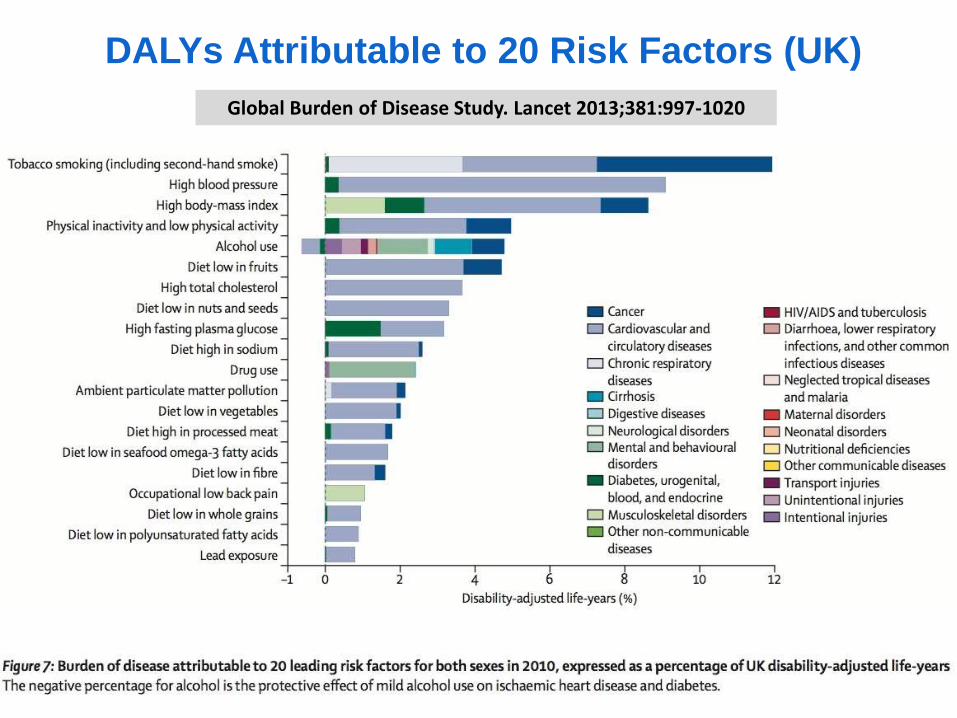
DALYs Attributable to 20 Risk Factors (UK)
“The performance of the UK in terms of premature mortality….is below the mean of the EU15+…….further progress will require improved public health, prevention, early intervention and treatment activities……and deserves an integrated and strategic response”
Outline
• Why is CVD important?
• Relationship between CVD & Mental Health
• CVD Outcomes Strategy
• 5 Year Forward View
• Health Checks and CVD Risk
• Conclusions
INTERHEART: Risk of AMI with
Multiple Risk Factors (52 countries, n≈30,000)
Yusuf et al. Lancet 2004;364:937-52
Yusuf et al. Lancet 2004;364:937-52
INTERHEART: Risk of AMI with
Multiple Risk Factors (52 countries, n≈30,000)
Yusuf et al. Lancet 2004;364:937-52
INTERHEART: Risk of AMI with
Multiple Risk Factors (52 countries, n≈30,000)
JAMA Psychiatry 2014; October 8th
…”people having a first schizophrenia spectrum episode were significantly
more likely to show a host of cardiovascular and endocrinologic risk
factors than the general population of a similar age.”
…”among relatively young patients enrolled (mean age 24) – half were
overweight or obese, nearly 60% had abnormal lipid levels, half have had
raised BP, and 13% had metabolic syndrome”
…”some of these findings likely related to antipsychotic Rx, but the illness
itself and associated unhealthy lifestyles also played major roles”
JAMA Psychiatry 2014; October 8th
Pyschosocial Factors & CVD
• Promotion of atherosclerosis [Circulation. 1999;99(16):2192]
– Direct effects (endothelium, platelets)
– Indirect via usual risk factors
• Depression and anger increase risk of angina & MI [Normative Aging Study 1998-2000]
• Depression in 20-40% of people having CABG, and poorer outcomes [Circulation. 2005;111(3):271]
• AHA (2004) recommends depression screening for those with CHD [Circulation. 2008;118(17):1768]
Pyschosocial Factors & CVD
• EPIC-Norfolk UK Prospective cohort study[Am J Psychiatry 2008;165(4):515]
– 19,000 people with major depressive disorder in year before enrolment
– initially free of CHD
– Median F/U 8.5 years
• Those with depression 2.7 more likely to die from IHD even after adjustment for traditional & other socio-demographic risk factors
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England,
who do not have an existing vascular disease, and who are not currently being treated for certain risk factors. It is aimed at
preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and
includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE
recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the
programme is clinically and cost effective.
Each year NHS Health Check can on
average:
• prevent 1,600 heart attacks and
save 650 lives
• prevent 4,000 people from
developing diabetes
• detect at least 20,000 cases of
diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a
percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the
protective effect of mild alcohol use on
ischaemic heart disease and diabetes.*
[Ref 4]
[Ref 5]
Top seven causes of preventable
mortality: high blood pressure, smoking,
cholesterol, obesity, poor diet, physical
inactivity and alcohol consumption.
[Ref 1]
NHS Health Checks
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England,
who do not have an existing vascular disease, and who are not currently being treated for certain risk factors. It is aimed at
preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and
includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE
recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the
programme is clinically and cost effective.
Each year NHS Health Check can on
average:
• prevent 1,600 heart attacks and
save 650 lives
• prevent 4,000 people from
developing diabetes
• detect at least 20,000 cases of
diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a
percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the
protective effect of mild alcohol use on
ischaemic heart disease and diabetes.*
[Ref 4]
[Ref 5]
Top seven causes of preventable
mortality: high blood pressure, smoking,
cholesterol, obesity, poor diet, physical
inactivity and alcohol consumption.
[Ref 1]
NHS Health Checks
NHS Health Check: explainedThe NHS Health Check programme is a national risk assessment
and management programme for those aged 40-74 years
NHS Health Check is a national risk assessment and management programme for those aged 40 to 74 living in England,
who do not have an existing vascular disease, and who are not currently being treated for certain risk factors. It is aimed at
preventing heart disease, stroke, diabetes and kidney disease and raising awareness of dementia for those aged 65-74 and
includes an alcohol risk assessment. An NHS Health Check should be offered every five years.
The programme systematically targets the top seven causes of premature mortality. It incorporates current NICE
recommended public health guidance, ensuring it has a robust evidence base. Economic modelling suggests the
programme is clinically and cost effective.
Each year NHS Health Check can on
average:
• prevent 1,600 heart attacks and
save 650 lives
• prevent 4,000 people from
developing diabetes
• detect at least 20,000 cases of
diabetes or kidney disease earlier
Burden of disease attributable to 20 leading risk factors for both sexes in 2010, expressed as a
percentage of UK disability-adjusted life-years
*The negative percentage for alcohol is the
protective effect of mild alcohol use on
ischaemic heart disease and diabetes.*
[Ref 4]
[Ref 5]
Top seven causes of preventable
mortality: high blood pressure, smoking,
cholesterol, obesity, poor diet, physical
inactivity and alcohol consumption.
[Ref 1]
http://www.jbs3risk.com
Heart 2014;100:ii1-ii67
http://www.jbs3risk.com
Heart 2014;100:ii1-ii67
Example 1Young female with significant risk factorsEffect of intensive risk factor modification
• 35-year-old female smoker
• Systolic BP of 160mmHg
• TC of 7.0mmol/L, HDL of 1.4mmol/L (non-HDL of 5.6mmol/L)
• Family history of premature CVD
Estimated average
survival without a
CV event
Estimated average
survival without a
CV event
Effect of intensive risk factor modification
Effect of intensive risk factor modification
Conclusions
• CVD still important cause of premature mortality
• CVD increases risk of mental illness
• CVD is common in those with mental illness
• In SMI, CVD Risk factors are similar to those of people without SMI, but are more prevalent
• CVDOS highlights what can be done
• Five year Forward View emphasises the importance of prevention and parity of esteem.
Improving the physical health of those
with severe mental health problems
– a patient perspective
Graham Morgan MBE
Updates from NHS IQ Pilot Sites and
the Royal College of Psychiatrists
2gether
Mersey Care
Northumberland, Tyne and Wear
Tees, Esk and Wear Valley
NHS Foundation Trusts
and
Royal College of Psychiatrists
Introduction
Emma Stark
Project Delivery Manager
Living Longer Lives team
Living Longer Lives Cardiovascular Disease/Serious Mental Illness Team
Clare BeardSenior Improvement Manager
Emma StarkProject Delivery Manager
Eleanor Kent-DysonProject Delivery Support Officer
Steve HodgesProgramme Delivery Manager
CVD Outcomes Strategy
“Action 1: NHS IQ will work with all relevant interests to develop and evaluate service models to manage CVD as a family of diseases, in the community and in hospital.
As part of this, NHS IQ will develop and test a standardised template that can be used in hospitals and in the community, and incorporated into service specifications, to assess fully patients with cardiovascular problems.”
SMI CVD Project
Presented by:
John Trevains – Deputy Director of Nursing
Helen Eddy – Physical Health Facilitator
55
What we are doing?
• Designing and implementing a simple and sustainable
process for monitoring CVD risk factors and delivering
targeted interventions
• Using health intelligence data to enhance practice
• Expanding our inpatients programme to a wider cohort
and incorporate the community teams across Trust
• Improving the communication of physical healthcare
information between secondary and primary care
Current Position
• A dedicated nurse to champion and lead this project
• An established health data intelligence system
• Improved communication with staff
o Training provided to all wards
o Clear point of contact
o Intranet
• LESTER tool care plan embedded into our clinical systems to
further support intervention
Next steps?
• Embed training into established training packages
• Establish key relationships with external providers
• Liaison with Primary Care team to work with GP’s and
offer training
• Open RiO – simplifying recording
NHS IQ Project: Improving cardiovascular health for people with SMI
Dr Simon Tavernor- Associate Medical Director
Joanne Scoltock- Modern Matron (Physical Health)
Mersey Care Project Aims
• Embedding the Lester tool as a trust-wide standard of care, initially in a 24-bedded acute male inpatient ward by:
• Identifying staff training needs- medical/ nursing
• Developing specialist service pathways where needed
• Working with service users
• Raising awareness of the importance of physical healthcare management.
What We Have Done
• Audit
• Made links with primary care
• Engaged with Service Users
• Made changes to Clinical Information System
• Staff Training
• Revised the Trust Physical Health Policy
• Placed NHS IQ project within a broader trust strategy for physical health
Current Position
Future Priorities
• Implementation of changes to clinical information system
• Focus on piloting on inpatient ward
• Re audit
• Look at equality issues against data
• Engagement with stakeholders
• Development of care pathways- cardiac in primary and secondary care
Project Summary
• Train and support 96 physical health link
workers across our trust to lead the
implementation of the Lester tool (2014).
• Develop sustainable, effective and clinically
appropriate pathways to deliver the interventions
arising from the implementation of the Lester
tool (2014).
Progress so far…
• Identified 96 link workers (inpatient and community)
• 88 of those have completed foundation PH training
• PH passport being rolled out to all nursing staff
• Regular link worker meetings established across NTW
• Project manager appointed!
• High-level project plan drafted
Next steps
• Develop a detailed project plan
• Promote and ensure continued good take up of
clinical skills training
• Increase link worker confidence in their application
of clinical skills
• Improve quality of information recording on the RiO
core physical health documentation
Tees, Esk & Wear Valleys NHS
Foundation Trust
Karen Conlon, Project Lead (Physical Health/SMI)
Robert Redfern, Project Nurse (Physical Health/SMI)
Jonathan Allen, Project Facilitator (NHS IQ Project)
Mike Leonard, Clinical Pharmacist
WHAT WE ARE DOING
Project Summary:
Implementing an electronic physical health monitoring
tool incorporating the Lester Tool.
Educating clinical staff to ensure that physical health
expertise is accessible in one acute ward and one
rehabilitation unit and aligned community teams.
Improving the inpatient/community/primary care
interfaces.
CURRENT POSITION
Working group established.
Clinical staff, service users and carers engaged in the
process.
Baseline audit of current position submitted.
Staff training needs identified, training commenced and
staff knowledge survey disseminated.
Electronic tool ready to go.
NEXT STEPS
Implement electronic recording tool.
Continue staff training.
Audit of service users.
Evaluation of the implementation of Lester 2014
Alan Quirk and Sonya Chee
CVD SMI Pilot Project National Learning Network Event
Wednesday 27th April 2015
Aims
To evaluate:
1. The impact of pilot initiatives on levels of physical health screening and interventions for inpatients
2. How the pilot sites achieved their objectives (or not) and the factors associated with this
Design & Methods
Design
• Realistic evaluation of pilot sites’ work
• Combines collection and analysis of data from 2 main work packages (WPs)
WP1: Impact of initiatives on levels of screening and intervention
• Case note audit before and after pilot initiatives
• Analysis of screening and interventions data
WP2: Case studies of Lester implementation
• Site visits – interviews and observation
• How, why, at what rate does the new technology spread?; What do people do to make the Lester workable?
Progress
• Baseline data received from sites
• Preliminary analysis of screening data
• Introductory visits to all pilot sites
• Observation of networking meeting for pilot sites
• Patient focus group at Mersey Care
• Drafting of patient questionnaire
Baseline sampleKey demographic characteristics (N=328) n (%)
% of patients who were still inpatients at the
time of data collection 91 (28%)
Average length of
stay
Mean number of days 121
Range (min – max):
days3–2969
Average age
Median age: years 43
Range (min – max):
years19-98
GenderMales 252 (77%)
Females 76 (23%)
EthnicityWhite British/Irish or
any other White
background
288 (88%)
• Smoking
• Weight
• Blood pressure
• Glucose
• Cholesterol
Screening and intervention
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTW TEWV 2gether Mersey Care Total
Patient was
pregnant/gavebirth within thelast 6 weeks
Documented
evidence ofrefusal
Not documented
Yes, recorded
Blood glucose screening during inpatient stay
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTW TEWV 2gether Mersey Care Total
Documentedevidence ofrefusal
Notdocumented
Yes, recorded
Cholesterol screening during inpatient stay
Best case scenario for Lester implementation?
• Long patient stays
• Staff with ‘holistic’ philosophy of care
• Teams/specialist staff in place with skills in physical health
• Technological skill/flexibility of IT systems
• Established links between services
Key question for case studies: how are good outcomes
achieved in different contexts – what is feasible?
Next steps
• Full analysis of baseline data (WP1)
• Site visits to pilot sites (WP2)
• Stakeholder consultation (WP3)
Questions?
Breakout sessions – Round 1Session 1: Using the patient voice to improve physical health care for people with Serious Mental Illness – Somerville room
Session 2: Improving cardiovascular care for people with severe mental illness - Delivering effective physical health checks in practice – Main room
Session 3: Physical health interventions - the patient journey from a physical health perspective from admission to discharge – Trinity room
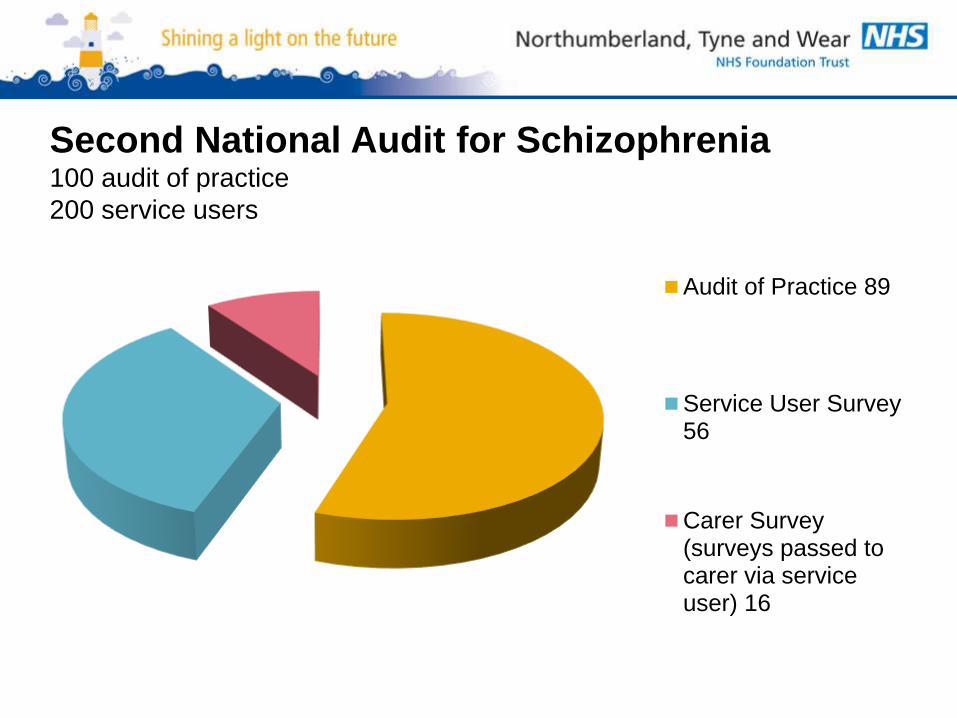
Session 4: Reasons for TEWVs success in the National Audit of Schizophrenia and how we are building on this – Merton room
Breakout sessions – Round 2Session 5: Physical health and wellbeing is everybody’s business: embedding the Lester tool through a comprehensive programme of training and support – Main room
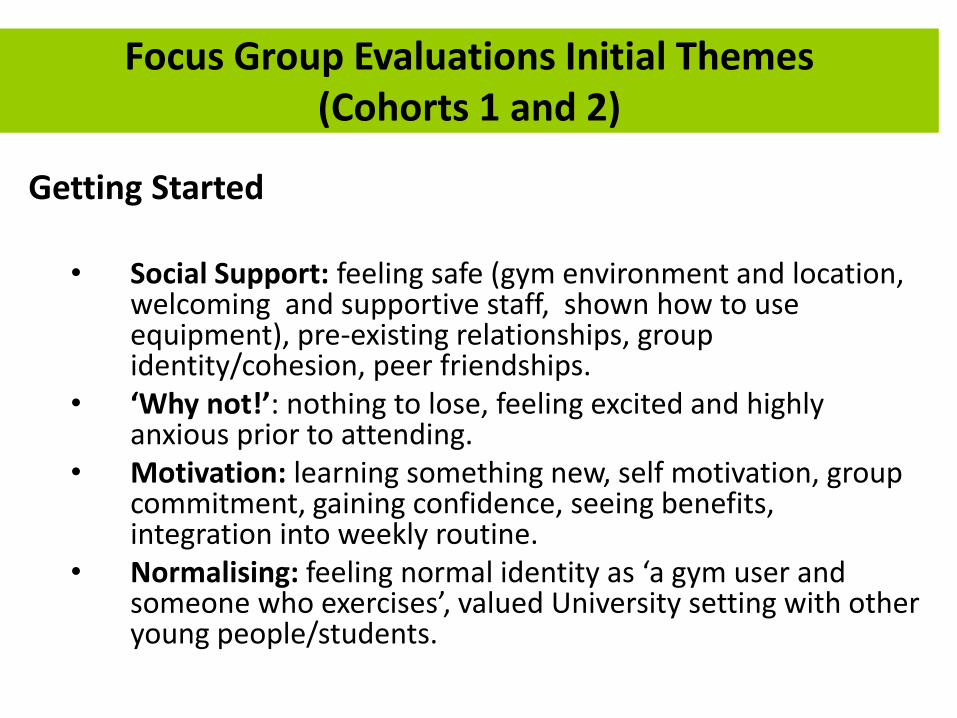
Session 6: SHAPE Programme – Early Physical Health Interventions for young people with psychosis and bipolar disorder - Somerville room
Session 7: Screening for cardiometabolic risk factors in people prescribed antipsychotic medication – Trinity room
Session 8: Sharing experience and expectations for physical health care in an acute setting – Merton room
Moving beyond CVD to improve
physical health & build collaboration
between primary and specialist care -
using technology at scale across a
whole city (Bradford)
Kate Dale and Angela Moulson
Improving the Quality of
Physical Health Checks
Kate Dale, Mental/Physical Health Project Lead BDCT
• Dr Angela Moulson
• Clinical Specialist Lead Adult Mental Health & LD Bradford
NB all material copyright BDCT and BAPCT
Research
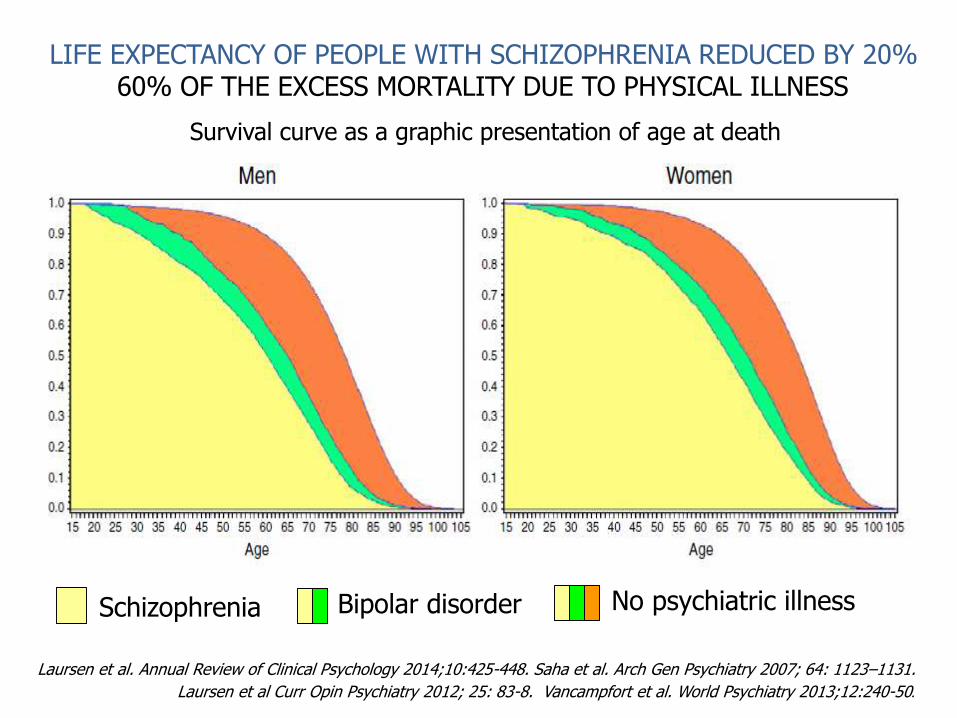
• Patients with Severe Mental Illness (SMI) experience health inequalities.
• The most notable is a shorter lifespan, reduced by around 20 years compared to the general population
• There is considerable evidence that one of the main causes of early death in people with SMI is cardiovascular disease
• Other physical causes include cancer
The Quality and
Outcomes Framework (QOF)
• Recommends:
• A physical health check within the last 12
months
Past QOF
Recommendations
• Recording Alcohol consumption
• BMI
• BP
• Cholesterol/HDL
• Blood Glucose
• Cytology Recordings
• However it does not specify
interventions
Present QOF
• BP
• Alcohol
• Cervical Screening
• Lithium
Mental/Physical Health
QoF Indicators
• The practice has a (SMI) register.
• Physical health to be reviewed at 12 monthly intervals.
• The review includes a check on accuracy of any prescribed medication
• Side effect monitoring
Review of physical health
Review of co-ordination arrangements with secondary care
• Lithium monitoring
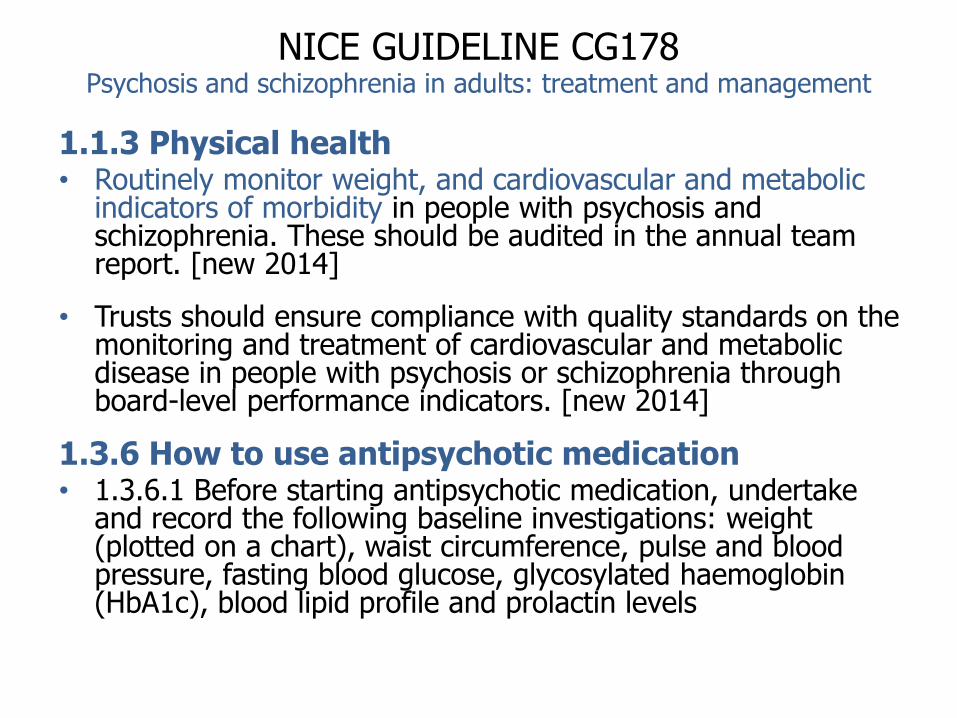
National Institute for Clinical
Excellence (NICE)
• Offers guidance for:
• bipolar disorder(CG38)
• Schizophrenia (CG82)
The Bipolar Guide
Recommends:
• Thyroid Function
• Blood Glucose
• Lipid profile in the over 40s
• Blood Pressure
• Weight/BMI
• Smoking status
• It also recommends prolactin, liver function tests, renal
function tests, full blood count and serum drug levels to
monitor certain drugs
Proposal to address health
inequalities in the SMI population in
Bradford
• A more specific standardised data entry
template based on existing mental health QOF
indicator
• Specific to areas of physical health risks
prevalent to those with SMI
• More specific tests e.g. blood tests for diabetes,
cholesterol, ECG and other appropriate tests.
• Auditable across the whole city using the
SystmOne primary care information system
First round of audits June/July
2009
• The audit tool used was based on our
proposed best practice template
• To support a proposal for (mandatory)
template locally
Audit Outcome
• 12 practices audited
• Using QOF SMI registers
• 20% of each register
• Random sample
• Total of 104 patients included
• Anonymous
• 42% female 58% male
Audit Findings77% Had BMI Recorded 79% smoking status recorded
52% eligible patients offered weight loss
advice
87% of smokers had been given cessation
advice
70% of eligible women had a cervical
smear test
55% alcohol status recorded
39% had a cholesterol test and 38% had a
triglyceride test
78% of heavy alcohol users were offered
advice
45% had a blood glucose recorded
3% waist circumference measured
38% had a thyroid function recorded 74% Had blood pressure recorded
Audit Findings
No patients had been given a
cardiovascular risk calculation
This would be a good way to identify high risk people for prevention
No patients had a blood test for
prolactin levels
(elevated prolactin is a significant and common adverse effect of antipsychotic treatment)
Discussion
• The quality of the health checks is in part
very good, but could be improved.
• Priority should be given to calculating
cardiovascular risk.
The SystmOne Physical
Health Check Template
Screenshots
Physical Health Check
Template
• The template is simply added to the GP system
• It supports a high quality check
• It helps predict risk
• It offers advice on what to do with abnormal
findings
• It is linked to a series of audit reports
• It supports QoF reporting
Copyright BDCT & BAPCT
2011
Copyright BDCT & BAPCT
2011
RIO Version
Now Live in Secondary Care
New Physical Health/Wellbeing
Clinics in 5 CMHTs Across BDCT
Second round of audits
• Using the new template in our first
practice
• 75 people were on the SMI register
• Data are available for the first 27 people
checked using new template
Body Mass Index (BMI)
27/27 BMI’s recorded (100%)
4 out of 27 patients had a Normal BMI
23 out of 27 patients had an Abnormal BMI
ALL 23 patients where offered weight loss advice
4 BMI<25
Normal
10 BMI 25–30
Overweight
8 BMI 30-35
Obese
5 BMI >35
V. Obese
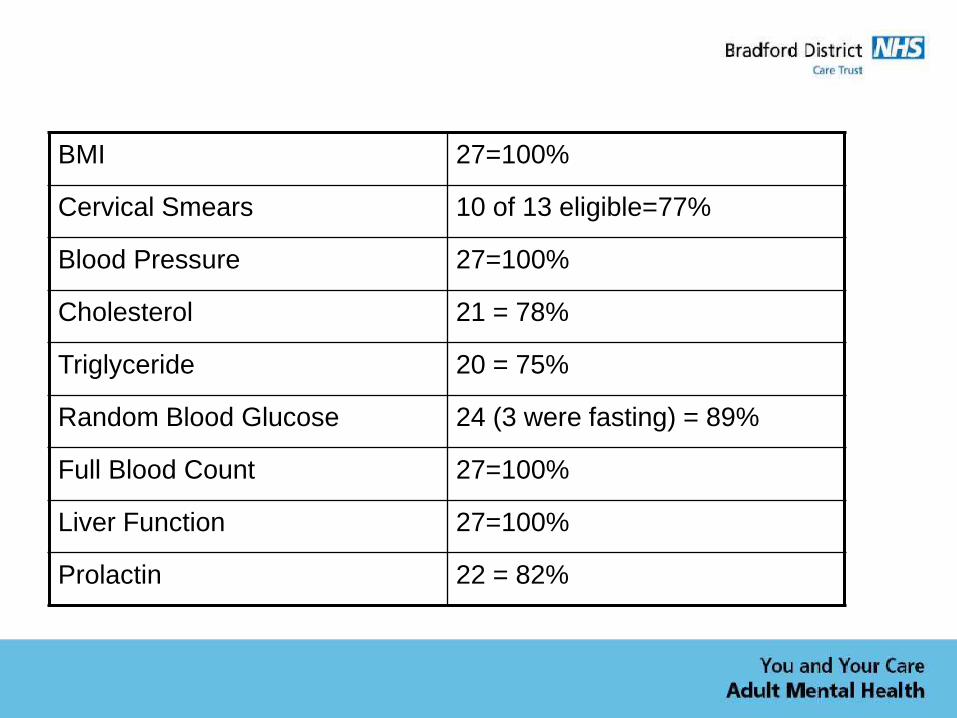
BMI 27=100%
Cervical Smears 10 of 13 eligible=77%
Blood Pressure 27=100%
Cholesterol 21 = 78%
Triglyceride 20 = 75%
Random Blood Glucose 24 (3 were fasting) = 89%
Full Blood Count 27=100%
Liver Function 27=100%
Prolactin 22 = 82%
Thyroid Function 24 = 89%
Smoking Status 27= 100% (18 smokers, 3 ex, 6 non)
Smoking Advice 18 = 100%
Weekly alcohol intake 27 = 100%
Current drug misuse 27 recorded = 100% 0 current users
On Lithium 2
ECG 23 Requested
Q Risk 13 Recorded = 48%
Quarterly Reports
April 2011
Baseline
Total SMI
Population:4,608
on CPA 811
July 2011
Quarter 1
Total SMI
Population:4,657 on
CPA 824
September 2011
Quarter 2
Total SMI
Population 4,719
on CPA 836
Further Roll out of the physical
health check template across
6 GP practices
Use of Physical Health Check Template for the annual
Review
Practice MH
Register
Annual
Review
Baseline
Annual
Review
Q1
Annual
Review
Q2
A 117 5 (4%) 14 20 (17%)
B 128 0 3 18 (14%)
C 142 0 4 13 (9%)
D 71 18 (25%) 20 22 (31%)
E 38 0 4 6 (16%)
F 60 9 (15%) 7 14 (23%)
Average 7% 18%
Blood Pressure Recordings in last 12
months
Practice MH Register Baseline Q1 Q2
A 117 84 82 86 (74%)
B 128 102 101 107 (84%)
C 142 83 87 93 (65%)
D 71 54 54 59 (83%)
E 38 24 24 25 (66%)
F 60 45 42 47 (78%)
Average (75%)
Opportunities
• Reduce health inequalities
• Reduce preventable deaths
• Improve quality of life, health and wellbeing for
patients and families
• Improve experience of health services for
patients and families
• Tailor interventions to high risk groups (age,
ethnicity, substance users)
4318
325
MH Register, NoProlactin Level
MH Register,Prolactin Level inL12m
Prevalence of prolactin
measurement is low
Prolactin elevation occurs in up to 95% of people on antipsychotic medication,
depending on medication type, and has risks for sexual dysfunction, osteoporosis
and breast cancer
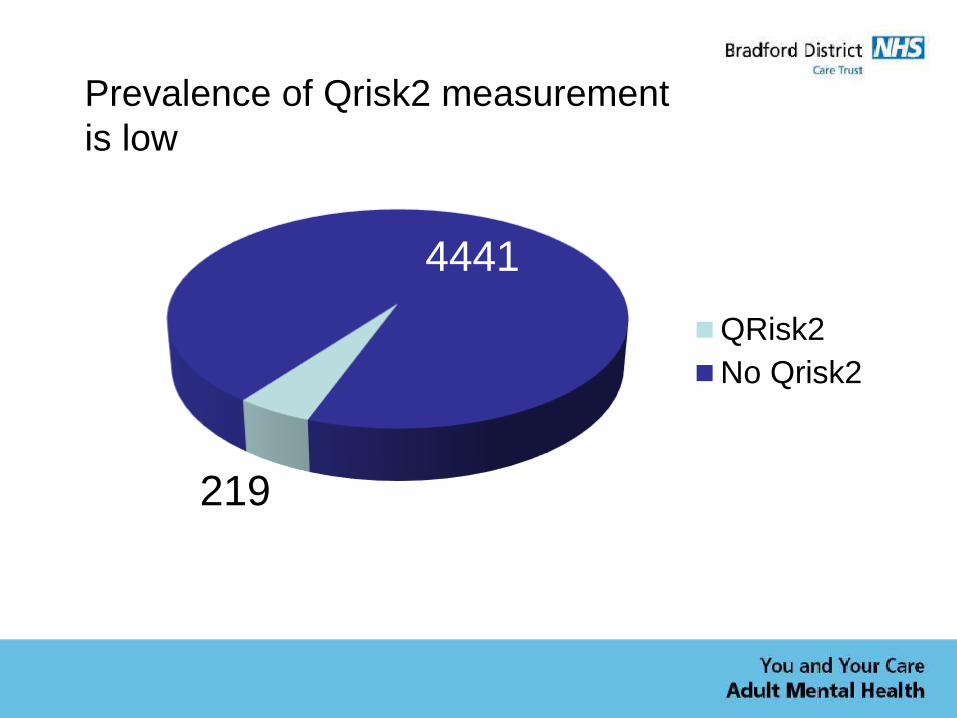
219
4441
QRisk2
No Qrisk2
Prevalence of Qrisk2 measurement
is low
72%
28% 0-20%
Highrisk
QRisk2 shows high risk in
SMI population
The prevalence of high risk for cardiovascular death is over twice that in
the general population
The End
NB all material copyright BDCT
Mental health 2015/2016 priorities
& achieving parity of physical
health care
Geraldine Strathdee
National Clinical Director
Mental Health
NHS | Presentation to [XXXX Company] | [Type Date]127
Parity of esteem : Improving the
CVD of people with SMI health
Dr. Geraldine Strathdee, National Clinical Director for Mental
Health……..@DrG_NHS
April 2015
This talk : Mental health’s time has come!
• Join the social movement of 250,000 leaders for action on mental health
• Update on the national public & political support for mental health
• The 5 year Forward View :what it means for mental health & recovery
• Update on the major commitment to parity of physical healthcare in MH
Thanking you front line leaders
• We need to to give 15 minutes of your time:
• Mind and Rethink Mental Illness are running an online survey to gather views that can be inputted to the mental health Taskforce.
– The link is here: http://www.surveymonkey.com/s/mh2020
International Human Rights movement Access to proven effective treatment delivered, in a society that provides care and not contempt for
people experiencing an episode of mental illness, has become an international Human Rights movement
129
3 new intelligence results coming soon
• Primary care QOF: – Heart UK data
– The Atlas of Variation
• Community sample – The National audit of Schizophrenia, 2014 community
population and now on My NHS
• All inpatients in every bed type in England – The CQUIN inpatient
130
131
The Mental Health Taskforce of England 5 Year Forward view Lifespan mental health
Being Born well Best early years Living and working wellGrowing older
wellDying well
Building Positive mental
health in individuals and communities
through raising political & public awareness and reduced stigma
Prevention of mental ill
health
through addressing the fundamental
causes
Improving access to
timely, effective services for the 16
mental health care pathways maximizing the potential of the
digital revolution
Transformation
of services to deliver
value, better outcomes, quality & personalized Right
Care
Building a sustainable
future
Of
Leaders, intelligence & and improvement
programmes
Access to evidence based care 7 Right Care NICE/SCIE effective care interventions
1. Right information that empowers & enables choice & self
management
2. Right Physical health care in primary care & specialist MH providers
3. Right Medication education, monitoring, support for adherence
4. Right Psychological therapies
5. Right Rehabilitation/ training/ employment
6. Right Care plan for housing, healthy lifestyles, self management
7. Right crisis relapse prevention care plan
In the Right least restrictive setting by the Right trained & supervised team
132
This applies to wider primary care, inpatient & community care
specialist mental health and social care providers
CQUIN: The top 8 key implementation tips
Board to floor
commitment
• Clinical leadership by top clinical leaders
• Proper sophisticated programme management
• Co design and constant fed back of progress in a dashboard to each clinical team so they can own the need to improve
• Commission and employ GPs & practice nurses to come on to wards to do immediate action, but also to train and supervise MH staff
• Use templates for both primary and secondary care : like any QOF activity
• Work force training , preferably practice nurses and ward nurses and MDTs together
• Use the creativity of your staff to co run healthy lifestyle groups
The provision of healthcare is now very challengingsmart thinking, all hands on deck, resilience needed
There is no option but to do High impact actions
• 40-60%: Tele triage ( skilled) reduces need for face to face by 40% & gets the right care quicker
• 10% account for 40% resource: Stratification of the top 100 repeating crises, avoidable repeat detentions, repeat admissions
• Think like a patient, behave like a taxpayer: Variation is a stupid waste of money we have to share & learn from the best
• Early intervention means better outcomes & less demand in medium term
• Hope and optimism by MH professionals as good as the Afgistan vets
• Mobilizing service users, their supporters & communities in their care plans & Personal health budgets
• Streamlining pathways :help identify the issues NO duplication
• Using digital to half paperwork to free up time to care……
• Staff and SUs: getting active, having fun, shared creativity
134
What are our 5 aims for lifespan mental health?
1. Building resilient individuals and communities: To continue to build public and political
support for mental health reform through increasing awareness of the individual and societal benefits of positive mental health & awareness of the types & causes of mental illness, in order to transform attitudes to mental health & reduce stigma. The power of social media & digital enablers are key
2. Preventing mental ill-health : To understand and maximize the opportunities for prevention of
mental ill heath, and the promotion of mentally healthy and resilient individuals and communities:
3. Introducing access standards to timely, effective care with outcome measurement When a person develops mental illnesses, they have timely access to personalized ,
integrated, holistic, effective, high quality treatments, that optimizes the health & functional outcomes & quality of life for individuals, their families, and, as the norm, takes place in the community or in the persons home, &reduces unnecessary use of healthcare resources.
4. Transformation of services : When a person’s illness is complex and severe, and requires specialist
interventions, that the care provided, is personalized, culturally appropriate, delivered in the least restrictive settings and 24/7 personalized home care services by trained and supported staff
5. Building a sustainable future :To develop & deliver the transformation needed, though creation of
an expert ‘state of the art’ leadership development, implementation & improvement programme and promotion of a Learning Organisation model throughout all our commissioned healthcare organizations
Empowering patients
• Information- Access to information will be improved. Within 5 years all citizens will be able to access their medical care records & share them with carers or others they choose
• Provide support to people to manage their own health- There will be investment in evidence-based approaches e.g. group-based education for people with specific conditions & self-management educational courses
• Increase patients direct control over the care provided to them-Ensure that patients have choice over where and how they receive care
• Integrated Personal Commissioning (IPC)- A voluntary approach to blending health and social care funding for individuals with complex need
• Supporting Carers- New ways will be found to support carers, by working with voluntary organisations and GP practices to identify them and provide better support
• Encouraging community volunteering- Develop new roles for volunteers which could include family and carer liaison workers, educating people in the management of long-term conditions and helping with vaccination programmes
• Stronger partnerships with charitable and voluntary sector organisations- The NHS will try to reduce the time and complexity associated with securing local NHS funding by developing a short national alternative to the standard NHS Contract where grant funding may be more appropriate and encourage funders to commit to multiyear funding wherever possible
• The NHS as a local employer- The NHS is committed to ensuring that boards and the leadership of NHS organisations better reflect the diversity of local communities they serve. As an employer to ensure all staff have support and opportunities to progress and create supported job opportunities to ‘experts by experience’ e.g. people with learning disabilities who can help drive changes in culture and services
Engaging communities
Transforming Mental health care in England 2020to achieve parity of access, effective care, quality & value across the Lifespan: 5YFV
Communities:
• Building informed, collaborative resilient communities Training every leader in intelligence
• Maximizing prevention
Introduction of access & integrated, effective care standards & measured outcomes for
• the 16 mental health conditions /pathways from primary care to specialized commissioned provision
• Starting with early intervention psychosis, perinatal mental health , eating disorders, liaison and CYP
Integration of clinical practice and pathways through transformation of
• Acute care: Liaison services to Acute care: A/E &
• Integrated care pathways in LTC clinics in acute trusts & community provider services
• Vanguards, and new models of commissioning & payments
Crisis Care transformation: Inverting the triangle & achieving fidelity models
• No more CYP in police cells, stratification
Transforming specialist mental health services through transformation of
• Psychosis care: 60% spend & needs: improving access, Right Care, reducing major efficiency variation, stratification
• Maximizing use of current resources to community based, multidisciplinary, multi agency teams and recovery
Enablers: Leadership, Workforce, Networks, digital, scientific revolution, payment systems
Care planning : 21st century Recovery style
– Identifying the social & friends & family support & knowledge network
– Coproduced formulation, agreeing the issues, offering Choices
– Shared decision making in care planning ( Newcastle)
– Personalization, including Personal Health Budgets
– ‘I” first person singular coproduced care plans
– NICE/SCIE evidence based integrated care to deliver Outcomes
– Using technology to reduce bureaucracy & free up time to care
– Service users, their networks & staff: coaching model & having fun
138
Baseline: What was the starting problem with mental health crisis services in England in 2014
If I have a physical health crisis I ring 999 or 111 and
get expert help
If I am in mental health crisis , I don’t know what number to ring or where I should go
to get help
If I have a physical health crisis and I go to my GP or
A/E, staff are trained to manage my acute care
If I go to my GP surgery in a mental health crisis, I have a
1: 3 chance of being assessed and treated in line with NICE
basic standards
I may end up in any of 14 different places to get help in
crisis including police cells, transport police, duty
systems in mental health and acute care, A/E, home care.
I may be brought to a police cell for a mental health
assessment rather than a hospital
If I go to A/E I have only a 45% chance or being
assessed by staff trained to do mental health
assessments
I am more likely to keep having to come back to A/E in crisis when I don’t get a trained response and am
more likely to go on to commit suicide
I have just a 45% chance of being seen by a trained
mental health liaison team in A/E so I am more likely to be
admitted to a bed in a hospital or care home
If I am seen by a crisis home treatment team they are so busy that they can give me and my family less support
than I need
If I need admission to a mental health bed in a crisis,
I may have to travel hundreds of miles
If I am from a BAME community my crisis is likely to be responded to by police,
not healthcare
The MH crisis concordat / UEA care model
8. Adequate beds when needed
7. Alternatives to Hospital beds e.g. day treatments and crisis houses
6. 24/7 Liaison mental health teams in A/E & acute trusts all ages
5. 24/7 Crisis Home Treatment Teams
4. Places of safety for S 135/136
3. Trained tele triage & tele health
2. Single number access ? 111
1. CCGs & HWWBs tackle causes
1. Identify Causes & Prevent by all agencies :• Identify the causes of MH crises & prevent• Public health, Health & Wellbeing Boards, CCGs, transport systems,
police, housing, social care, primary care
2. Single coordinated access number & system• single access number to ring ? 111• all agency response, GPs, social care, NHS
3. Tele triage and tele health well trained staff• Reduce suicide & face to face need by 40% • Respond to police & other referrers
4. S 136 places of safety/ street triage
5. Crisis Home treatment teams with fidelity• reduce admissions and LOS by 50%• ? Could coordinate street triage etc
6. Liaison mental health teams• in A/E & acute trusts reduce admissions to acute beds and
care homes by 50% & reduced LOS
7. Crisis houses & day care for as alternatives 8. Adequate acute beds when needed
CCG/ LA area local characteristics City/urban/rural/deprivation descileHot spots for crisis events, e.g suicides, transport hub, mobile populations
Governance
Do u have in place:
Crisis Concordat multi agency programme board establishedSystem resilience Board: MH lead on it Urgent care networks: MH lead?
Concordat action plan developed Access standards agreed
Have you agreed local standards Have you waiting times in line with national standards What has each agency committed to in the Action plan
Directory of Services Have you got a DOS with the key Local Govt, 3rd sector, NHS & other CQC registered services: helplines, psychological therapies, bereavement, relationship in and out of
hours Benchmarked in & out of hours the reasons for crisis calls
111 / Single point of access Yes/ No
Tele triage & tele healthService with trained workforce
Yes/No: Does your single point of access include :GP in & out of hours MH crisis responseSocial care, Housing , Carer crisis response Street triage police and / or Transport hub triage services Ambulance hub triage Liaison & diversion triage for custody Alcohol and drug services
Crisis Home treatment team Is the team commissioned in line with local need Does the team operate to the ‘Fidelity’ criteria
Liaison to acute trust/ primary care Is the team Core, Core Plus, enhanced, comprehensive Was the person a 4 hour breach What is the team’s RCPsych peer accreditation PLAN network standard
Crisis houses / day treatment Yes/NO
Beds when needed of the right type Beds of all types
Best practice & UEA Cquin needed
• Identify and code the common causes of crisis• JSNA: is a good crisis section in your local JSNA • Directory of services and NHS Choices: what’s in your area • Clinical team dashboard for continuous feedback to teams• Caseload zoning including NICE Clinical care• Where are the highest performing teams • What competencies are needed to work in CHTT
Please add to Crisis Concordat best practice http://www.crisiscareconcordat.org.uk/inspiration/
• The new UEA CQUIN :Help your frequent users and trust http://www.england.nhs.uk/wp-content/uploads/2015/03/9-cquin-guid-2015-16.pdf
Elective care system in mental health 2015-2020: we are building personalized, recovery
orientated, high quality care, home based 24/7 care & reduction of suicide at every level
High secure beds
Medium secure beds
Low secure beds
Intensive rehabilitation closed unit
for complex dual diagnosis
Open rehabilitation units
Locally authority Residential rehabilitation
Supported accommodation with care package
Own tenancy plus personalized budget
24/7 Assertive outreach/ community forensic team multi agency teams
24/7 Assertive outreach /rehabilitation & recovery, multiagency teams
24/7 Assertive outreach /rehabilitation & recovery multi agency teams
Rehabilitation / recovery team: multi agency
Rehabilitation / recovery team
CMHT/ Enhanced primary care SMI with 3rd sector outreach
CMHT/ Enhanced primary care SMI with 3rd sector outreach
Design Principle :It is vital to understand that in mental health our ‘technology’ and ‘care model design principle’ is that in order to provide safe, NICE concordant , efficient services, we need proven effective care teams to link with bedsIn mental health we are expert at using case managers to triage all admissions & work early on the discharge plans
The beds The teams
Will you Wo (Man) up for mental health We have 250,000 mental health leaders
who Speak up & Move to Action for mental health
Will you join that social movement ?
On social media, & from the Crisis concordat and networks we have experts by experience, families, mothers, teachers, carers, 3rd sector skilled activists, WeNurses, We Docs, WeMH commissioners, CCG MH leads, BPS, MIND, Rethink, AHSNs, SCNs, Clarhs, maternal mental health alliance, the leading active communication savvy mental health trusts, HFMA, We AMHPs, pharmacists, Royal colleges, and other professional bodies, PMs. DPMs, cabinet office, MPs, DWP etc etc and FTN, NHD Confed, Kings fund, Nuffield foundation, artists, poets, musicians, and many many more in England
We get the leading edge new data, research findings, front running innovations alerts
We share state of the art quality improvement top tips, we share best practice
We now are linked to a growing international mental health social movement aiming to build Collaborative , compassionate resilience individuals and communities….@DrG_NHS
144
The 15/16 Access & Waiting Time Standards
145
New access standards
• Access to psychological therapies: 75% of people referred to the ImprovedAccess to Psychological Therapies programme will be treated within 6weeks of referral, and 95% will be treated within 18 weeks of referral.
• Access to early intervention for psychosis: More than 50% of peopleexperiencing a first episode of psychosis will be treated with a NICEapproved care package within two weeks of referral.
• Access to eating disorder services for CYP
• Access to perinatal care
• £30m targeted investment on effective models of liaison psychiatry in agreater number of acute hospitals. Availability of liaison psychiatry willinform CQC inspection and therefore contribute to ratings.
Next steps : What are the enablers
• The voice of the people & communities & government
• Evaluation of Service Improvement in Mental Health – Tuesday 19th May, 12.30 -13.30
• Demand and Capacity in Mental Health Services –Friday 26th June, 12.30 – 13.30
• 3 Dimensions of Care for Diabetes (3DFD): Integrating psychological, social and diabetes care for patients with poor diabetes control -Thursday 18th June, 12.30 – 13.30
NHS IQ Website
Further information on NHS Improving Quality’s work
programmes can be found at http://www.nhsiq.nhs.uk/
An email containing a link to an evaluation survey of today’s event will be sent to all delegates.
Please do take the time to complete the survey as it will help us design the next event.
Thank you!
www.nhsiq.nhs.uk‘
Putting Patients FirstThe NHS England Business Plan 2013/14-2015/16
‘Patients, professionals and citizens need far better information on local services and need to be able to take control of their health when they want to. They need to be able to offer feedback on local services and know that those comments will be acted upon.’
Experience of Care
‘The involvement of patients, carers and the public in shaping and improving the way in which services are designed, delivered and improved is crucial.’
NHS Constitution
‘Foster a common culture shared by all in the service of putting the patient first’ and ‘… patients must be the first priority in all of what the NHS does.’
Robert Francis QC
EDNAEntirely
Demanding of
Nothing
At all
DORADemanding
Of
Regular
Attention
Next?
• High expectations
• Have never known a time before the NHS
• Very assertive
• Can research things on the internet
• May film or record their experiences
• User of social media
• Not afraid to challenge authority
• Care and treatment seen as a right and an entitlement when
and where they choose
• May approach the local/national media
What are the benefits?
• Improve healthcare
• Inform and educate
• Build confidence with the public
• Make better use of resources
• Improve how services are evaluated
Think of all the ways we ask patients, carers and
members of the public for feedback
How is the NHS currently using feedback?- asking the right questions before engagement
• Seven day services• End of life care• Cancer patient experience survey• Friends and Family test• Complaints• Working with individual trusts• Mental Health Services (parity of esteem)• Cardio-vascular projects
Improving cardiovascular care for people with severe mental illness: delivering effective physical health checks in practice
Dr Sheila HardySenior Research Fellow, Northamptonshire Healthcare NHS Foundation Trust; Postgraduate Nurse Educator for the Charlie Waller Memorial Trust; Honorary Senior Lecturer, UCL; Visiting Fellow, University of Northampton
Overview
• Ensuring everyone with severe mental illness receives screening and lifestyle advice
• How we have implemented physical health checks and the results we have seen
• Monitoring improvement in practice
Ensuring everyone with severe mental illness receives screening and lifestyle advice
Why?
• More likely to:
oDie early
oHave a number of modifiable risk factors for cardiovascular disease
oHave a comorbid physical condition
• Less likely to have:
oMonitoring of their physical health
oPhysical examination
oPrompt diagnosis for a physical problem
oIntervention to help change unhealthy behaviour (e.g. smoking)
oScreening for cancer (e.g. mammography)
oSurgical intervention (e.g. following an MI)
Ensuring everyone with severe mental illness receives screening and lifestyle advice
How?
• Provide financial incentives
• Prepare clinicians, support workers, carers
• Provide appropriate guidance and tools
Payment incentives – primary care
2014/15 QOF ID Indicator wording Changes
MH001The contractor establishes and maintains a register of patients with schizophrenia, bipolar affective disorder and other
psychoses and other patients on lithium therapy -
MH002
The percentage of patients with schizophrenia, bipolar affective disorder and other psychoses who have a comprehensive
care plan documented in the record, (in the preceding 12 months) agreed between individuals, their family and/or carers as
appropriate -
MH003The percentage of patients with schizophrenia, bipolar affective disorder and other psychoses who have a record of blood
pressure in the preceding 12 months -
MH004
The percentage of patients aged 40 or over with schizophrenia, bipolar affective disorder and other psychoses who have a
record of total cholesterol:hdl ratio in the preceding 12 months Retired
MH005
The percentage of patients aged 40 or over with schizophrenia, bipolar affective disorder and other psychoses who have a
record of blood glucose or HbA1c in the preceding 12 months Retired
MH006The percentage of patients with schizophrenia, bipolar affective disorder and other psychoses who have a record of BMI in
the preceding 12 months Retired
MH007The percentage of patients with schizophrenia, bipolar affective disorder and other psychoses who have a record of alcohol
consumption in the preceding 12 months -
MH008
The percentage of women aged 25 or over and who have not attained the age of 65 with schizophrenia, bipolar affective
disorder and other psychoses whose notes record that a cervical screening test has been performed in the preceding 5
years-
MH009The percentage of patients on lithium therapy with a record of serum creatinine and TSH in the preceding 9 months
-
MH010The percentage of patients on lithium therapy with a record of lithium levels in the therapeutic range in the preceding 4
months -
Monitoring - primary care (pre specific payment incentive for SMI)
Cholesterol 2,378,115 98.4% 218,539 71.7% Chi² = 262020 p <.001
HBA1c or glucose 2,363,485 94.9% 197,494 64.8% Chi² = 495257 p <.001
Monitoring - primary care (post specific payment incentive for SMI)
Mitchell and Hardy. (2013) Psychiatric Services.
Locally Enhanced Service (LES)
Enhanced services plug a gap in essential services or deliver higher than specified standards, with the aim of helping PCTs (now CCGs) reduce demand on secondary care. Enhanced services expand the range of services to meet local need, improve convenience and extend choice (DH 2010).
Payment Incentives
Inpatients – Physical Health CQUIN 2014/15
INDICATORS
Indicator 1: 65 per cent of funding for demonstrating, through a national audit process similar to the National Audit of Schizophrenia, full implementation of appropriate processes for assessing, documenting and acting on cardio metabolic risk factors in patients with psychoses, including schizophrenia.
Indicator 2: 35 per cent of funding for completion of a programme of local audit of communication with patients’ GPs, focusing on patients on the CPA, demonstrating by Quarter 4 that, for 90 per cent of patients, an up-to-date care plan has been shared with the GP, including the holistic components set out in the CPA guidance.
Payment incentives
Primary Care
38% of practice nurses would like training to carry out physical health checks for people with SMI (Hardy 2014). 23% currently doing it without having had training (Hardy 2014).
Secondary care
Over 80% of mental health nurses reported they would like training for the management of diabetes, cardiovascular health, and nutrition. Sixty-nine percent would like education about smoking and 67% reproductive health (Robson et al 2012). A survey carried out on behalf of UCLPartners (March 2015) found 92% of mental health nurses wanted training in how to deliver a health check and 83% in how to monitor cardiovascular risk.
Prepare staff
Prepare staff
(Hardy 2014)
Prepare staff – primary care
Hardy and Huber (2014)
Prepare staff – primary care
175
HENCEL and UCLPartners: Practice nurse masterclasses
Ten modules:
Compulsory
Module 1 – Mental health awareness (classroom)
Optional
Module 2 – Behaviour change (classroom)
Module 3 – Physical health of people with mental illness (classroom)
Module 4 – Wellbeing (classroom)
Module 5 - Co-morbidities: using a psychological approach (classroom)
Module 6 - Alcohol and drug awareness (e-learning)
Module 7 - Medications used in mental illness (e-learning)
Module 8 - Your patient’s journey (e-learning)
Module 9 - Care planning (e-learning)
Module 10 - Specific conditions (e-learning)
Prepare staff – primary care
Prepare staff – primary care
Practice nurse training
• The Charlie Waller Memorial Trust have been granted
permission by Health Education England to use these
materials.
• Training can be provided free of charge to identified
healthcare trainers from individual organisations.
Training for mental health clinicians in preparation
Prepare staff – secondary care
Appropriate guidance and tools
Guidance for all
Appropriate guidance and tools
Tools for all
http://physicalsmi.webeden.co.uk/
Appropriate guidance and tools
Guidance and tools for practice nurses
Appropriate guidance and tools
Guidance and tools for mental health nurses
The HIP
Results from implementation
Monitoring - primary care (post training)
Hardy et al. (2014) International Journal of Social Psychiatry.
Results from implementation
Offering lifestyle advice – following training
Hardy et al. (2014) International Journal of Social Psychiatry.
• ~[Title/Initial/Surname]
• ~[Patient Address Block]
• ~[Post Code]
• Dear ~[Title] ~[Surname]
• You are invited to …………..Medical Centre, on…………….at………….for a health
• check.
• The purpose of the appointment is to check that you are physically well and review
• the medications that you are taking. You will be offered a blood test and may be
• offered an ECG (examination of your heart). You can refuse any of the
examinations
• offered to you if you so wish. Please bring a specimen of urine.
• If you have any medical problems these can be dealt with during this appointment.
• If you have any questions or concerns, please contact the surgery by
ringing…………
• Yours sincerely
• Name of Practitioner
Results from implementation
Results from implementation
Present
• Evaluation of training sessions have shown improvements in clinician’s knowledge and attitudes (Hardy and Kingsnorth 2015, Hardy and Huber 2014).
• Audits (QoF, NAS can show increase in activity but not quality)
Need for research including qualitative elements to find out impact on patients (Hardy et al 2013)
Monitoring improvement in practice
Department of Health. (2010) Enhanced Services. http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Healthcare/Primarycare/Primarycarecontracting/DH_4126088
Hardy S. (2014) Mental health and wellbeing survey: A snapshot of practice nurses’ views regarding responsibility and training. http://uclpstorneuuat.blob.core.windows.net/cmsassets/Mental%20health%20and%20wellbeing%20survey%2020%20Jan%202014.pdf
Hardy S, Deane K and Gray R. (2013) The Northampton Physical Health and Wellbeing Project: The views of patients with severe mental illness regarding their physical health check. Mental Health in Family Medicine. 9 (4) 233-240.
Hardy S and Gray R. (2012) Is the use of an invitation letter effective in prompting patients with severe mental illness to attend a primary care physical health check? Primary Health Care Research & Development. 13 (4) 347-352.
Hardy S, Hinks P and Gray R. (2013) Screening for cardiovascular risk in patients with severe mental illness in primary care: a comparison with patients with diabetes. Journal of Mental Health. 22 (1) 42-50.
Hardy S, Hinks P and Gray R. (2014) Does training practice nurses to carry out physical health checks for people with severe mental illness increase the level of screening for cardiovascular risk? International Journal of Social Psychiatry. 60 (3) 236-242.
Hardy S and Huber J. (2014) Training practice nurses to care for people with severe mental illness. Primary Healthcare. 24 (3) 18-23.
Hardy and Kingsnorth. (2015) Mental health nurses can increase capability and capacity in primary care by educating practice nurses. Journal of Psychiatric and Mental Health Nursing. (in press).
Harvey S, Newton A and Moye G. (2005) Physical health monitoring in schizophrenia: the use of an invitational letter in a primary care setting. Primary Care & Community Psychiatry. 10 (2) 71-4.
Mitchell A and Hardy S. (2013) Surveillance for metabolic risk factors in patients with severe mental illness vs diabetes: National Comparison of Screening Practices. Psychiatric Services. 64 (10) 1060-1063.
Norman P and Conner M. (1993) The role of social cognition models in predicting attendance at health checks. Psychology & Health 8 (6) 447 – 462.
• PRIMROSE Trial- Prediction and management of cardiovascular risk for people with severe mental illnesses. A research programme and trial in primary carecarried out by UCL.
• ERIC-D - a feasibility study of a cardiovascular risk reduction programme in an at risk population with mental health problems which developed a training programme for mental health professions in primary care.
• Access to detailed baseline data. Certain CCGs within the UCLPartners geography have completed a ‘deep dive’ into their data surrounding CVD and SMI through the UCLPartners Mental Health Informatics Platform. This platform gives access to the spectrum of mental health illness and data surrounding CVD risk. It also has the capability to obtain health economics data.
191
UCLPartners CVD/SMI Projects
• UCLP hosts the CCG Mental Health Leadership Network with the SCN. This represents an opportunity for engagement in Primary Care.
• The QMUL Clinical Effectiveness Group has produced an SMI Template and SMI in primary care guide that highlights the codes and approach to screening used within 3 East London CCGs who use EMIS.
192
Proposed UCLPartners Project
• AIM- to increase the uptake of screening for CVD risk in those with SMI and ensure that where risk is identified, an intervention is offered.
• HOW?
• Learn from best practice in CVD and SMI within the UCLPartners geography and from national work that has taken place.
• Use the available data to scrutinise for the true impact of mental health on mortality rates and current CVD risk. Although we have StandardisedMortality Ratios for SMI available at borough level as a hard outcome, there is a lack of info on coverage or outcomes of interventions. We would aim to improve coverage/ outcomes of interventions we know work to address causes of premature mortality in this group.
193
Proposed UCLPartners project
• Ensure that where appropriate there is patient engagement in the process to co-create pathways and interventions, as required.
• Implement a full screening tool for CVD risk (such as the Bradford tool, with adaptation/testing where required) into primary care within an interested CCG.
• Ensure that all high impact interventions for exercise, diet, smoking cessation and alcohol support are embedded in the tool (based on the Lester model.)
• Support GP practices to deliver the required interventions perhaps utilisingservices in secondary care depending on what the gap analysis of service provision is.
• Utilise capability across the system to deliver interventions through the collection of data from primary and secondary care.
194
Proposed UCLPartners Project
• Link with UCL research that has informed the development of QoF and NICE guidance.
• Ensure a whole pathway approach to sharing key information between relevant stakeholders.
• WHERE?
• In order to deliver this potential project, UCLPartners would gather expressions of interest for involvement from CCGs (and MHTs where appropriate.)
• We will select a pilot site with the intention to roll out learning to other interested areas
• WHEN?
• Awaiting the outcome of a business case approval
• Lloyd Andrews (Exercise and Health Practitioner).
• Sophie Lucas (Exercise and Health Practitioner).
• Karen Dawe (Lead Physiotherapist for the Trust).
• Damon Coombs (Ward Manager).
Wotton Lawn Hospital
• 80 bed unit plus a 12 bed low secure unit for working age
adult patients.
• Approximately 630 acute admissions over the 2014-2015
period.
PHYSICAL HEALTH in SMI
• Association between physical co-morbidity and mental ill-health haslong been established. In his 1897 text, The Pathology of Mind, SirHenry Maudsley noted: ‘Diabetes often shows itself in families inwhich insanity prevails’.
• People with severe and enduring mental health conditions (SMI)experience worse physical health.
• Reduced life expectancy compared to the general population.
• There is an excess of over 40,000 deaths among SMI patients whichcould be reduced if SMI patients received the same healthcareinterventions as the general population.
Physical Health at Wotton Lawn Hospital (WLH)
• Staff recognise increase in co morbidities.
LESTER tool Red zone ‘high risk’Smoker 58%Alcohol misuse 22%Substance Misuse 31%BMI ^25 67%High BP 27%Abnormal Glucose 13%Abnormal Lipids 18%
Physiotherapy and the Exercise and Health Team
• 3.0 WTE Exercise and Health Practitioners (Band 5 and
Band 6).
• 3.0 WTE Physiotherapists (Band 5).
• 1.0 WTE Physiotherapy Assistants (Band 4).
Offering a seven day service 8am-8pm
Physiotherapy intervention as part of the initial patient journey
• Falls assessment, which may include additional assessment
e.g. Berg Balance.
• VTE assessment
• Further specific assessment. For example; neurological,
musculo-skeletal, respiratory.
• Development of specific treatment and intervention
programmes.
Exercise and Health intervention as part of the initial patient journey
• MUST assessment (Malnutrition Universal Screening
Tool)
• LESTER tool
• Prioritisation analysis
• PAR-Q
• Development of specific treatment and intervention
programmes/care plans.
• Physical health enquiries within MDT setting – working
in-line with EoC and NEWS scores
Ward based interventions
• Essence of Care screening on admission and minimum
of every 28 days thereafter
• Physical examination by admitting Doctor
• ECG on admission and as indicated
• National Early Warning Score (NEWS) completed for all
service once a week and as clinically indicated.
• Physical health discussed at the MDT meeting each
week for all service users
• Activities coordinator and activities programme
LESTER tool • The Lester Tool helps to identify mental health patients
at risk of Cardiometabolic conditions and allows for early
intervention. Smoking
Poor lifestyles
BMI over 25
Hypertension
Raised blood sugars
Raised blood Lipids
Substance misuse
Alcohol use
How we prevent/reduce the risk factors• Offer a gym within the hospital, swimming and walking groups, hydrotherapy, 1:1 running session,
circuits, Pilates, dance, box fit.
• Healthy living sessions
• Smoking cessation nurses within the physiotherapy/exercise and health department – commencing NRT
• 1:1 health education
• Leaflets
• Liaison and joint working with OT’s, nursing staff, dietician’s, doctors, kitchen staff, turning point, external
government led organisations e.g. change4life
• Offer healthy meal options and food diaries
• Physical health monitoring including weight, BP, pulse, BM’s.
• Address motivation and mental health
• Physical health leads/champions
• Activity coordinators
• Healthy social activities
• Inclusion for all
Case studyMs B –
54 years old, diagnosed with bipolar disorder as a teenager.
Never married and lived with brother who suffered with alcoholabuse and unfortunately passed away last year.
Ms B has one friend who she goes on holiday with yearly and willmeet for coffee once a week. Other than this, Ms B leads asecluded life
Ms B used to be admitted to Wotton Lawn approximately 3 timesper year.
On this admission, Ms B had presented with low mood and lowlevels of motivation which resulted in her spending prolongedperiods of time in bed and self neglect.
Assessments completed:- Problems identified:-
• MUST assessment
• LESTER tool completed
• Falls and VTE completed
• PAR-Q
• Waterlow
• Risk assessments for use of profiling bed and
mattress
• Poor knowledge regarding healthy diet and
wellbeing
• Poor sleep hygiene
• Poor house hygiene
• Believed that she had no money
• Required carers for initiation of tasks so to prevent
self-neglect
• On lithium medication
• Obese
• Not meeting the 150 minutes of exercise per week
• Lonely
• Raised blood sugars
• HTN
• Previous breast cancer
• Oedema in lower limbs
• Poor mobility
• Pressure areas of concern
Actions taken:-• Turning rota and provision of specialist equipment
• VTE monitoring
• Circulatory exercise
• Mobility work and Extend sessions
• Timetabled physical activity to provide structure
• Gym x3 per week (as willing)
• Swimming once per week
• Daily walking for 30 minutes
• Healthy eating advice/food shopping
• Well being advice – sleep hygiene, breast cancer awareness
• Weekly weighing
• Food diaries
• Dr medication review for HTN and diabetes
• Offered support when going to follow up appointments at the breast clinic
• OT intervention for daily living tasks
• Outpatient walk4life every Wednesday morning
Results • Has not been admitted to Wotton Lawn Hospital for over 1 year and half
• Weight loss of 5kg during 2 month admission
• Continues to attend community walking group every Wednesday and carers also
help with maintaining a healthy diet
• Continues to lose weight in the community and has more structure to her week
• Able to identify signs or concerns regarding breast care
• Regular visits to GP for diabetes and HTN control
• Also seen by recovery team in the community and has asked that she goes for
walks with the team rather than going for coffee
Thank you
Any Questions?
References
1. Lester H, Shiers D, Rafi I et al (2012). Positive cardiometabolic health resource: an intervention framework for patients with psychosis on antipsychotic medication. Royal College of Psychiatrists, London.
2. Holt R (2012). Cardiovascular disease and diabetes in people with severe mental illness: causes, consequences and pragmatic management. PCCJ Practice Review E-publication ahead of print; doi:10.3132/pccj.2011.085.
3. NICE. Preventing Type 2 diabetes (recommendation 19) http://guidance.nice. co.uk/PH38.
Dr Sally Wise
Consultant Psychosis Team
Clinical Director
A 7 year Journey!
Resistance to change
Lithium deaths
QTc sudden deaths
Silos of excellence
• Lithium register
• HDAT
• Both run and monitored by Pharmacy
• Quick, simple, cost neutral solution
Only Applies to Specific Groups
Lean thinking
• Applied to specific patient groups only
• Standard work
• Continuous process
• Visual control
• Monitored through POMH audits
• Clozapine clinics
Now for all patients!
Now for all patients!
• Specialisation of teams – significant enabler
Vehicle of change and willing to change
• Transparency of problems and obstacles
• Psychosis pathway regulated specific interventions at
Young People with Psychosis are on a path to obesity, type 2 diabetes, cardiovascular disease and premature death
Start
HERE
NOW! STOPnaturalhistory
Established psychosisRCT
First episode of psychosis
12 kg
Antipsychotic-Induced Weight Gain
Alvarez-Jimenez et al (2008)
The same life expectancy and expectations of life as peers without psychosis
SHAPE Programme: Aims
• To support young people experiencing a First Early Psychosis to make treatment and lifestyle choices informed by an understanding of their greater risk for future obesity, CVD and diabetes
• To provide access to healthcare in a positive and socially inclusive environment which embraces the importance of ‘ordinary lives’
• Offered as part of holistic care package to youngpeople accessing the Worcestershire EIP Service:
• 12-20 individuals per 12 week SHAPE programme
• Rolling programme running 5x over the year
• 60 young people with psychosis will have access to the SHAPEprogramme during the 12 month piloting and evaluationphase
SHAPE programme
• A physical health and wellbeing intervention programme developed with an EI service user group
• Structured intensive bespoke physical health group intervention:• Delivered over 12 weeks with a
years free gym membership • Nutritionists, exercise
physiologists, sports therapists and health trainers expertise
• Utilising student (EAYL) and peer group support
• Located in a youth focused, socially inclusive University gym setting
• Monitoring and evaluation at pre-intervention, baseline week 1, week 12 and 12 months post intervention.
SHAPE Programme Objectives
• Engage young people with psychosis in relation to their physical health needs through a structured health and wellbeing programme – Improve cost efficiency of physical health
monitoring and intervention via a ‘one stop shop’– Improve access to health advice– Reduce tobacco smoking, substance use and
improve diet and healthy lifestyle behaviours
• Enhance quality of care plans addressing physical health concerns– Review medication and side effects regularly to
minimise the development of complications – Complete a documented physical health
assessment within 6 weeks of initiating anti-psychotic medication
• Maintain pre-illness weight levels or support weight loss to within 7% of pre-illness weight levels over 12 months
• Maintain/reduce BMI, blood glucose, lipid profile and blood pressure within the normal range
SHAPE Programme Elements
• Physical health ‘MOT ‘ assessment at baseline, 12 weeks and 12 months
• Health educational programme on healthy eating, smoking cessation, substance misuse, dental care, sexual health care and stress management.
• Group cardiovascular exercise and use of exercise suite gym sessions
• Personalised nutritional advice.
• Smoking cessation advice.
• Mindfulness and relaxation training.
• Motivational goal setting to review goals and maintain focus
• SHAPE workbook summarising content and practical tasks for each week to allow the participants to keep a progress record and use as a learning resource
• Carers evening to engage support from family members
• Collaboration with primary care practitioners to reduce physical health risks
• Referral for specialist assessment and treatment where required.
Group Exercise Component
• Evidence based: literature review to inform content/ duration of the group exercise/gym session components.
• Exercise prescription based on ‘Physical Activity and Mental Health National Consensus’ (Biddle et al. 2000):
– exercise 2-4 days per week for a duration of 20-30 minutes.
– at a moderate intensity and engaging in a wide range of exercises
– total exercise duration (incl. warm-up and cool-down) approx. 45-60 mins.
• Group cardiovascular exercise and exercise suite gym sessions include aerobic exercise (badminton, basketball, walking), gym circuits and resistance training (gym induction/equipment introduction, individualised programmes in open gym sessions) and other low impact exercise activities (Tai Chi, Pilates).
• Level 3 exercise referral fitness coach leading exercise sessions to gauge participants exercise intensity/duration to ensure within correct exercise prescription for the programme, monitor and adapt programme in response to any exercise related health concerns and for patients with known medical conditions such as hypertension.
Nutritional Support: Background
• Healthy eating advice offered as part of the integrated 12 week programme
• Enable participants to make healthier food & drink choices
• Help off-set weight gain often associated with medication
• Try to give practical advice & offer access to one to one support
Week 3: Introduction to Healthy Eating
• Introduction to Healthy Eating
• Review food groups
• What makes a balanced diet
• Talk about fruits & vegetables– 5 a day (80g is a portion,
potatoes don’t count)
• Review resources:– Eatwell plate
– Harvard food plate
• Portion sizes for meats, cheese, saturated fat
Week 7: Menu Planning & Shopping Lists
• Review list of healthy store cupboard items that can make it easier to eat healthier at home
– Long life
– Convenience
– Economical
• Tips for health menu planning over a week
• Tips for healthy eating if buying food out
Week 11: Healthy Snack tasting
• Session after the gym session
• Tasting session focusing on snacks– Combination of sweet & savoury snacks to
try
– Gives participants the opportunity to try new things without spending money in case they don’t like them
– Hopefully this will help change behaviours
– Review food labels & cost
– Look at calorie content, sugar, salt & saturated fat content
– Opportunity to talk to peers and nutrition lecturers, ask questions and get input on menu planning ideas
Other Resources and 1:1 nutritional support
• Participants offered a range of leaflets including some with menu planning tips & shopping lists & advice re. portion sizes– NHS Change for Life– British Heart Foundation
• Free cookbook• After the 12 weeks participants
can also access a 1:1 nutritional consultation in the McClelland centre – 1 hr 15 min session– Tailored programme can be
developed
SHAPE Location
• McClelland Centre for Health and Wellbeing, University of Worcester City Centre Campus
• In Worcester City, 5 minutes away from main bus and rail stations
• Exercise suite with gym equipment and weights room
• Group meeting room for educational sessions
• Clinic room to carry out health MOT’s, weight and fitness assessments
• Individual consultation rooms for smoking cessation, sexual health and nutritional therapy individual appointments
2
1
9
4
3
2
1
2
SHAPE Attendance by Locality (cohorts 1 and 2)
Monitoring and Evaluation (baseline (within 6 wks medication initiation), week 1, week 12 and 12 months follow up)
•Key physical health risk markers including BMI, waist circumference, resting blood pressure, blood glucose and total serum cholesterol•Weight, fitness levels, readiness to exercise •Self-reported lifestyle behaviours and healthy coping strategies in relation to target health behaviours. •Patient related experience engagement with and acceptability of/satisfaction with the programme and challenges/barriers to programme adherence. •Engagement (enrolment, utilisation, adherence) and dropout rates •Clinical outcomes in terms of recovery, changes in functioning and symptom improvements •Cost-efficiency: service usage data, staff time, use of personal budgets
Table 1. Baseline characteristics of SHAPE participants. Data are presented as mean and standard
Table 2. Baseline characteristics of SHAPE participants.
Variable N % of SHAPE Participants
Smoking* 47 45%
Alcohol 45 40%
Drug use 44 16%
Sedentary 46 37%
Healthy Eating* 46 30.4%
Medications
Aripiprazole 44 18%
Clozapine 44 23%
Olanzapine 44 27%
Paliperidone 44 2.3%
Quetiapine 44 23%
Risperidone 44 7%
Cohort 1: Outcomes (June-Sept 2014)
Baseline Physical Measures (n=12 enrolled)• 6 participants with a BMI>30.0 (Obese)• 5 participants with a BMI 25.0 – 29.9
(Overweight)12 week Physical Measures (n=7 completed programme):• No statistically significant change in
weight, BMI or waist circumference• 5 participants maintained weight
– 1 had a 6cm decrease in waist circumference
• 2 participants increased weight by 4kg
Cohort 2 Outcomes
Baseline Physical Measures
• 4 participants with a BMI>30.0 (Obese)
• 4 participants with a BMI 25.0 – 29.9 (Overweight)
12 week Physical Measures (n=7):
• No statistically significant change in weight, BMI or waist circumference
• 3 participants maintained weight (+/- 1kg)
• 4 participants lost weight (-2 to -8.4kg)
• 3 participants increased weight (+2.4 to +9.6kg)
Mean within-group change (95% CI) Paired T-
test
UK SHAPE (n=17)
SHAPE
Paired T-test
from Pre-post
Bondi KBIM (n=16)
Bondi Standard
Care (n=12)
Weight (kg) 0.4 (2.6 to -1.9)
t = -0.342, p = 0.737
1.8 (-0.4 to 2.8)
7.8 (4.8 to 10.7)*
t = -1.121, p = 0.31
BMI (kg/m2) -0.01 (0.7 to -0.7)
t = 0.045 p = 0.965
0.4 (-0.1 to 0.9)
2.6 (1.6 to 3.6)*
t = -0.543. p = 0.61
Waist
circumference
(cm)
1.0 (4.6 to -2.7)
t = -0.562 p = 0.582
0.1 (-2.1 to 2.2)
7.1 (4.8 to 9.4)*
t = 0.733, p = 0.51
SHAPE 12 week Outcome Data: Cohorts 1 and 2 (Combined) (results compared with Bondi ‘Keeping Body in Mind’ (KBIM) Programme data)
Focus Group Evaluations Initial Themes (Cohorts 1 and 2)
Getting Started
• Social Support: feeling safe (gym environment and location, welcoming and supportive staff, shown how to use equipment), pre-existing relationships, group identity/cohesion, peer friendships.
• ‘Why not!’: nothing to lose, feeling excited and highly anxious prior to attending.
• Motivation: learning something new, self motivation, group commitment, gaining confidence, seeing benefits, integration into weekly routine.
• Normalising: feeling normal identity as ‘a gym user and someone who exercises’, valued University setting with other young people/students.
Focus Group comments: Getting Started
• Social support:
“…when people started to talk to me, and I started to talk back to them, it was easier because I felt like I’d made a friend, and then more friends, and it was easier than just being on your own, because you felt like you were going with somebody.”(Focus Group 1)
• Why not!:
“I was suffering from really bad anxiety and panic attacks, and I really didn’t want to go. I really had to force myself to go, but I survived the first time, which made me persevere.”(Focus Group 1)
• Motivation
“Yes. Sometimes I wake up and I don’t feel like doing anything, but
because I’m committed to coming I force myself to go”(Focus Group 1)
• Normalising
“I think it’s quite good because there’s other people that come at the same time, so you don’t feel like you’re here for a specific activity, and there’s other people working out as well, so you feel like you’re in a normal environment.” (Focus Group 2)
“Because it’s a Uni- it’s got that extra edge to it. All the students walking around, learning, smart.”(Focus Group 2)
Focus Group Evaluations Initial Themes (Cohorts 1 and 2)
Maintaining New Behaviours
Structured Activities: workbook guidance (mixed feedback), variation in programme activities, new knowledge from education sessions
Gaining Confidence: self identity as ‘active’ and ‘someone who does exercise’, benefits in terms of fitness levels, new possibilities in relation to exercise and activities
Applying new knowledge: lifestyle changes, new friendships, personal goal setting
Focus Group comments: Maintaining new behaviours
• Structured activities
“Every week was different, I’ll give it that. It wasn’t the same old thing, it was very varied.” (Focus Group 2)
“I like the talking and nutrition parts. I also liked learning about drugs, I found it interesting.”(Focus Group 1)
• Gaining confidence
“The sessions have been worthwhile and I have gotten more fit and
I have lost weight” (Focus group 1)
“Easier to move around without getting out of breath” Focus Group 1)
• Applying new knowledge
“It has made me change my routine on other days as well. Before I wouldn’t want to go out or do anything, like walk my dog. Or I would do it, but because it was so late in the day that I’d have no choice but to do it, whereas I’ve started doing it in the morning, then setting up my day with it, just to get that level of activity and to make me feel just a little bit better. So it has helped me to know how to exercise.”
(Focus Group 1)
• Family support
“Dad noticed I had lost weight” .”(Focus Group 1)
“my husband helped – we changed our diet together” .”(Focus Group 1)
SHAPE Funding and Support
• Health Foundation 2014 SHINE award• Funded from June 2014 to September 2015• Ongoing access funded from personal budgets• Drinks bottles and step counters sponsored by Postcode
Anywhere• Logo and design work gifted by Concept Advertising and
Comparison of 15 antipsychotic drugsLeucht S et al. Lancet. Online June 2103
WEIGHT GAIN WITH ANTIPSYCHOTICSM
ea
n w
eig
ht
ch
an
ge
(k
g)
Bushe et al. J Psychopharmacol 2013;27:358-365
3-year observational data from the Worldwide Schizophrenia Outpatient Health Outcomes Database
Mean weight change from baseline for patients receiving monotherapy (completer analysis)
METABOLIC RISKS ASSOCIATED WITH ANTIPSYCHOTIC DRUGS
De Hert M et al. Nat Rev Endocrinol 2011:8:114-26
SCHIZOPHRENIA AND THE METABOLIC SYNDROME
• MS: cardiometabolic risk factors highly predictive of type 2 diabetes and CV disease
• Indicated by presence of ≥3 specific factors
• hypertension, dyslipidaemia, central obesity, raised fasting glucose
• Reported point prevalence ranges from 5.7% to 63% De Hert et al. World Psychiatry 2009;8:15–22; Malhotra et al. J Aff Disorders 2013; Suttajit S et al 2013
• Meta-analyses of 126 studies, 77 publications (n= 25,692)
• Overall prevalence of metabolic syndrome is 32.5%
• Strongest influence: illness duration (p<.0001)
• Highest rates in those prescribed clozapine (51.9%) and lowest in those unmedicated (20.2%) Mitchell AJ et al. Schizophr Bull 2013;39:306-18
• Patients with schizophrenia should receive regular monitoring and adequate treatment of cardio-metabolic risk factors
NICE GUIDELINE CG178Psychosis and schizophrenia in adults: treatment and management
1.1.3 Physical health• Routinely monitor weight, and cardiovascular and metabolic
indicators of morbidity in people with psychosis and schizophrenia. These should be audited in the annual team report. [new 2014]
• Trusts should ensure compliance with quality standards on the monitoring and treatment of cardiovascular and metabolic disease in people with psychosis or schizophrenia through board-level performance indicators. [new 2014]
1.3.6 How to use antipsychotic medication• 1.3.6.1 Before starting antipsychotic medication, undertake
and record the following baseline investigations: weight (plotted on a chart), waist circumference, pulse and blood pressure, fasting blood glucose, glycosylated haemoglobin (HbA1c), blood lipid profile and prolactin levels
1.3.6 How to use antipsychotic medication• 1.3.6.4 Monitor and record the following regularly and systematically
throughout treatment, but especially during titration:• weight, weekly for the first 6 weeks, then at 12 weeks, at 1 year and
then annually (plotted on a chart)• waist circumference annually (plotted on a chart)• pulse and blood pressure at 12 weeks, at 1 year and then annually• fasting blood glucose, HbA1c & blood lipid levels at 12 weeks, 1 year
and then annually [new 2014]
• 1.3.6.5 The secondary care team should maintain responsibility for monitoring service users' physical health and the effects of antipsychotic medication…• for at least the first 12 months or• until the person's condition has stabilised..whichever is longer. Thereafter, the responsibility for this monitoring may be transferred to primary care under shared care arrangements. [new 2014]
NICE GUIDELINE CG178Psychosis and schizophrenia in adults: treatment and management
PRESCRIBING OBSERVATORY FOR MENTAL HEALTH (POMH-UK): WHAT DO WE DO?
• Funded solely by subscriptions from member organisations: NHS and private/charitable health providers in the UK
• Run national quality improvement programmes (QIPs) in discrete areas of prescribing practice
• Convene QIP steering group: clinicians from relevant speciality
• Set evidence-based, clinical practice standards:
• Recognised by clinicians as realistic/reflecting best practice
• Provide customised data collection tools and data analysis
• Provide ‘benchmarked’ feedback to services
• Develop and offer bespoke change interventions
• Re-audit 18 months later and provide ‘benchmarked’ feedback on changes from baseline
• Subsequent supplementary audits with benchmarked feedback
DATA FOR QUALITY IMPROVEMENT
Benchmarked performance against clinical standards• Benchmarking against other clinical services is anonymous• Most potent element: reflection by clinical teams on their
benchmarked performance • Prompts local action plans to address areas where
performance falls short of the audit standards
Other audit data• Demographic/diagnostic/clinical information collected• Context for interpretation/understanding of practice• Informs local strategies/systems to achieve improvement
Ownership of data• Ownership of local data retained by healthcare services• Data collected suitable for QI purposes but not for
objective ranking/judgement of healthcare organisations Getting the Measures of Quality, Kings Fund 2010
1Prescribing high dose and combined antipsychotics
2Screening of metabolic side
effects of antipsychotic drugs
3Prescribing high-dose/combined
antipsychotics: forensic services
4 Prescribing anti-dementia drugs
6Assessment of side effects of
depot antipsychotic medication
7 Lithium monitoring
8 Medicines reconciliation
9 Use of antipsychotics in LD
10Use of antipsychotic medication
in CAMHS
11Prescribing antipsychotics for
people with dementia
12Prescribing for people with
personality disorder
13 Prescribing for ADHD
14Substance misuse: alcohol
detoxification
15 Valproate for bipolar disorder
16 Rapid tranquillisation
POMH-UK QUALITY IMPROVEMENT PROGRAMMEScreening for the metabolic side effects of
antipsychotic drugs
Practice standard• All patients prescribed continuing antipsychotic medication should
have their blood pressure, body mass index (or other measure of obesity), blood glucose (or HbA1C) and lipids measured at least once a year.
• Annual screening is the minimum acceptable practice:• Most guidelines recommend more frequent screening of some
or all of these measures depending on the drug prescribed or a patient’s demographic or clinical characteristics
Participating services• Conducted in Assertive Outreach Teams
% PATIENTS SCREENED FOR EACH OF THE 4 ASPECTS OF METABOLIC SYNDROME IN THE PAST YEAR
NATIONAL SAMPLE AT BASELINE 2005 (21 Trusts participated, N=1,966)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Blood pressure Obesity Glycaemic control Lipid profile
55828%
23312%
117560%
51726%
27214%
117760%
34117%
31516%
131067%
42822%
19910%
133968%
Test result/measurement recorded in casenotes
Some reference to screening in casenotes, but no result recorded
No evidence of screening in casenotes
For every case of diabetes identified, 1 missed For every case of hypertension identified, 4 missedFor every case of dyslipidaemia identified, 7 missed
CLINICAL BARRIERS
Questionnaire to clinical teams:
• About a third uncertain as to whether such physical health screening was the responsibility of the psychiatric team rather than, for example, a primary care clinician.
• Less that half were confident about interpretation of abnormal results
• Limited access to basic equipment such as a tape measure and weighing scales
Barnes et al. Schiz Bull 2007;33:1397-1401
TARGETED INTERVENTION
Baseline2006
Re-audit 2007
2c suppl.2008
2d suppl.2009
2e suppl.2010
2f suppl.2012
Number of Trusts and patients
21 TrustsN=1,966
21 TrustsN=1,516
13 TrustsN=1,035
21 TrustsN= 2,522
29 TrustsN=3,058
32 Trusts1,591
No evidence of screening 46% 25% 31% 28% 28% 14%
Some reference to screening
43% 52% 50% 50% 49% 52%
Test/result measure for all 4 aspects
11% 23% 18% 22% 24% 34%
SCREENING FOR METABOLIC SYNDROME IN AOTsAT EACH AUDIT SINCE BASELINE
% OF PATIENTS SCREENED FOR ALL 4 CARDIOMETABOLIC RISK FACTPOTRS IN ASSERTIVE OUTREACH SUBSAMPLE, 2012 (N=1,569)
ICD-10 DIAGNOSTIC CATEGORIESSCREENING IN THE PAST YEAR FOR CARDIO-METABOLIC RISK FACTORS IN
PATIENTS ON ANTIPSYCHOTIC DRUG TREATMENTAOT, adult recovery, and forensic services, 2012, n=6078
1,646
170
286
2,198
387
395
692
179124
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
F20-29 F30-39 All other
Perc
enta
ge o
f p
atie
nts
no evidence ofscreening
some referenceto screening
All four aspectsrecorded
SCREENING FOR CARDIO-METABOLIC RISK FACTORS IN PATIENTS ON ANTIPSYCHOTIC DRUG TREATMENT
Adult services (affective disorder) past 1 year: 2012 CAMHS (bipolar disorder) past 6 months: 2014
17013
387
24
179
3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Adult services 2012 CAMHS services 2014
Perc
enta
ge o
f p
atie
nts
no evidence ofscreening
some referenceto screening
all four aspecstrecorded
SUMMARY• The findings suggest that audit-based QIPs can help improve
clinical practice in relation to physical healthcare screening• Success may be partly attributed to:
• Use of a practice standard widely accepted as best practice• Bespoke change interventions
• Change interventions addressed barriers to screening identified by participating clinical teams
• Analysis of the data revealed factors predicting targeting of patients for screening:• More likely to be screened: Known diagnosis of hyperlipidaemia or
diabetes, prescribed clozapine• Less likely to be screened: prescribed a depot/long-acting
antipsychotic preparation as only antipsychotic treatment
• Only a minority of community psychiatric patients prescribed antipsychotic medication is screened for the metabolic syndrome in accordance with best practice recommendations
SUMMARY• Analysis of the data revealed factors predicting targeting of
patients for screening
More likely to be screened• Known diagnosis of hyperlipidaemia• Known diagnosis of diabetes• Prescribed clozapine
Less likely to be screened• Prescribed a depot/long-acting antipsychotic preparation
as only antipsychotic treatment • ? proxy for variables not collected in the audit:
• Level of engagement with clinical services• Frequency of medication review• Perception by clinicians that at least some of the antipsychotic drugs
commonly prescribed as depot/long-acting preparations have a lower liability for metabolic side effects