CYRIAX Transverse Friction Massage Effects Deep transverse friction has three main effects : * Traumatic hyperaemia, which helps to evacuate pain triggering metabolites. * Movement of the affected structure, which prevents or destroys adhesions and helps optimize the quality of the scar tissue. * Stimulation of mechanoreceptors, which produces a quantity of afferent impulses that stimulate a temporary analgesia. This also helps the patient to perform movement exercise. Indications-contraindications of friction massage Indications : muscular, tendinous and ligamentous lesions. Contraindications : * Calcification * Rheumatoid tendinous lesions * Local sepsis * Skin diseases Technical details • Exact localization It is imperative that deep friction is given at the site of the lesion ; after all, it is there where we need to influence the scar formation. • No movement between finger and skin We need to friction the structure and not the overlying skin. Do not glide over the skin, otherwise you might damage the skin, making deep friction impossible for the next session(s). If the patient used a creamy body lotion then cleansing the skin with alcohol or use a thin layer of cotton-wool between the finger and skin. • Transverse Deep friction is given transverse to the fiber direction. • Sufficient amplitude Make sure we make a big movement and move over-up-and again over the structure in order to have a good contact. Therefore it is necessary to take a reserve of skin : first we move the skin superficially in the opposite direction and then we apply pressure and perform the active phase of the deep friction. 1
Transcript
CYRIAX
Transverse Friction Massage Effects
Deep transverse friction has three main effects : * Traumatic hyperaemia, which helps to evacuate pain triggering metabolites. * Movement of the affected structure, which prevents or destroys adhesions and helps optimize the quality of the scar tissue. * Stimulation of mechanoreceptors, which produces a quantity of afferent impulses that stimulate a temporary analgesia. This also helps the patient to perform movement exercise.
• Exact localization It is imperative that deep friction is given at the site of the lesion ; after all, it is there where we need to influence the scar formation.
• No movement between finger and skin We need to friction the structure and not the overlying skin. Do not glide over the skin, otherwise you might damage the skin, making deep friction impossible for the next session(s). If the patient used a creamy body lotion then cleansing the skin with alcohol or use a thin layer of cotton-wool between the finger and skin.
• Transverse Deep friction is given transverse to the fiber direction.
• Sufficient amplitude Make sure we make a big movement and move over-up-and again over the structure in order to have a good contact. Therefore it is necessary to take a reserve of skin : first we move the skin superficially in the opposite direction and then we apply pressure and perform the active phase of the deep friction.
1
• Sufficient depth How deep must the deep friction be ? Sufficient to reach the structure ; so, it depends on the location of the structure.
• Starting position Make sure the friction massage is comfortable for you as well for the patient. Position the patient in a way where you can easily reach the structure you want to friction. Make sure your position is comfortable also in order to save energy. Make the lesion accessible to the finger. Tendons with a tendon sheath are generally frictioned in a stretched position, just like ligaments (better contact). Muscle bellies are always frictioned in a shortened position (easier to move the fibers in relation to each other).
• Various grips are used, according to the nature and the position of the lesion.
• Economy of effort : concentrate on performing an arm movement instead of a small finger movement since this is much more comfortable to the patient and to the therapist. Make sure you make a two-phase movement : active phase with more pressure (movement of the structure) and relaxation phase, without pressure. Always try to keep your own finger joints slightly flexed (if you friction too much with your interphalangeal joints in hyperextension, you might provoke a traumatic arthritis in those joints).
Duration and frequency
* For most lesions, 3 times/week is sufficient frequency : usually 15' per session ; we start the first session with 10'. In some chronic lesions the duration of treatment will reach 20'. If more than one spot has to be treated (e.g. achilles tendinitis), it will be 10' per localization. * There are two exceptions where a different strategy is used : the medial collateral ligament of the knee and the lateral ankle ligaments. Here, the deep friction is given in a progressive way. The details will be discussed in the appropriate sections. * If the structure is too tender on palpation, the interval between the sessions is prolonged ; the duration and the intensity of the deep friction do not change. * The treatment can be ended when the patient is symptomfree and the functional examination has become negative ; remaining local tenderness on palpation can be ignored. Exception : quadriceps and hamstrings muscle bellies ; To avoid recurrences, the treatment has to be continued for another week after full clinical recovery.
Normal execution
When describing the techniques in detail, the "normal execution of the deep friction" will often be mentioned. What we mean by that is : one or more fingers are put onto the lesion, reinforced by one or more fingers. A reserve of skin is taken in the opposite direction, pressure is applied and the active phase of the DF is then a movement towards ourselves. In most cases, this is a large arm movement and not a small finger movement, with all our finger joints slightly flexed. The relaxation
2
phase then follows into the opposite direction. Remark : sometimes all fingers are used next to each other for DF, i.e. when treating muscle belly lesions in large muscles. This is necessary to prevent the formation of adhesions. When the DF is given tenoperiostally, there should always be a contact with both tendon and bone.
3
Shoulder techniques
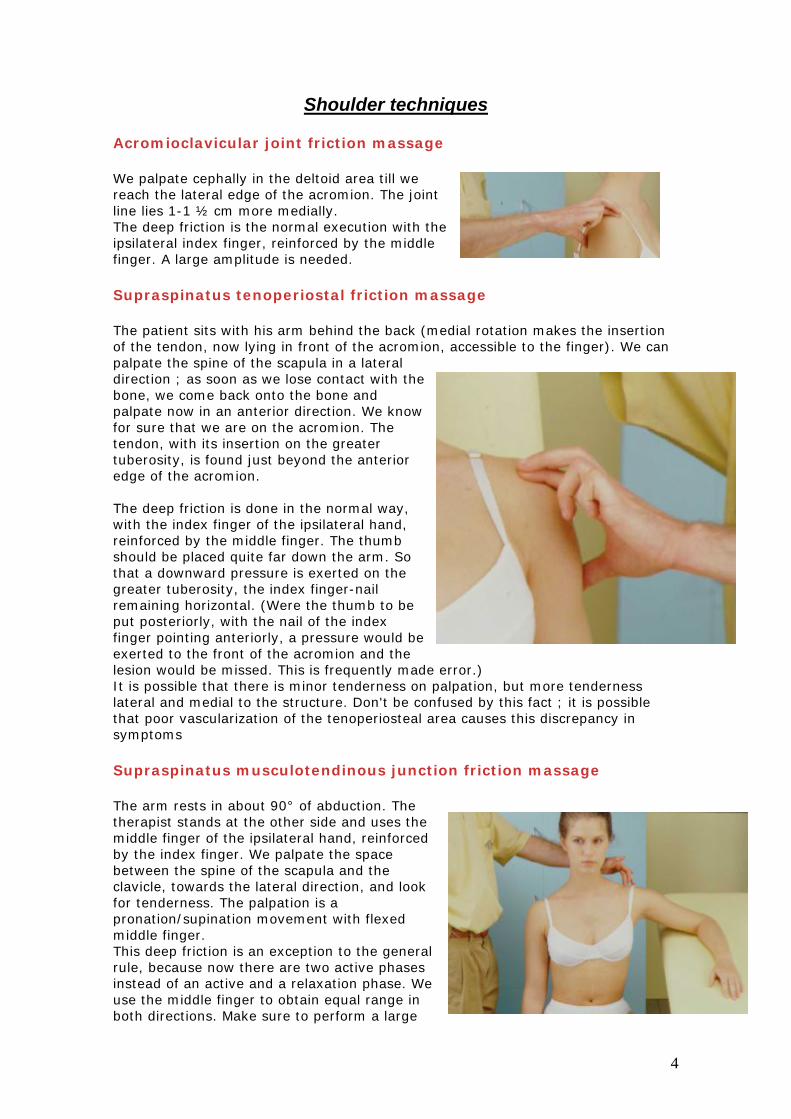
Acromioclavicular joint friction massage
We palpate cephally in the deltoid area till we reach the lateral edge of the acromion. The joint line lies 1-1 ½ cm more medially. The deep friction is the normal execution with the ipsilateral index finger, reinforced by the middle finger. A large amplitude is needed.
Supraspinatus tenoperiostal friction massage
The patient sits with his arm behind the back (medial rotation makes the insertion of the tendon, now lying in front of the acromion, accessible to the finger). We can palpate the spine of the scapula in a lateral direction ; as soon as we lose contact with the bone, we come back onto the bone and palpate now in an anterior direction. We know for sure that we are on the acromion. The tendon, with its insertion on the greater tuberosity, is found just beyond the anterior edge of the acromion. The deep friction is done in the normal way, with the index finger of the ipsilateral hand, reinforced by the middle finger. The thumb should be placed quite far down the arm. So that a downward pressure is exerted on the greater tuberosity, the index finger-nail remaining horizontal. (Were the thumb to be put posteriorly, with the nail of the index finger pointing anteriorly, a pressure would be exerted to the front of the acromion and the lesion would be missed. This is frequently made error.) It is possible that there is minor tenderness on palpation, but more tenderness lateral and medial to the structure. Don't be confused by this fact ; it is possible that poor vascularization of the tenoperiosteal area causes this discrepancy in symptoms
The arm rests in about 90° of abduction. The therapist stands at the other side and uses the middle finger of the ipsilateral hand, reinforced by the index finger. We palpate the space between the spine of the scapula and the clavicle, towards the lateral direction, and look for tenderness. The palpation is a pronation/supination movement with flexed middle finger. This deep friction is an exception to the general rule, because now there are two active phases instead of an active and a relaxation phase. We use the middle finger to obtain equal range in both directions. Make sure to perform a large
4
movement and avoid extending the distal interphalangeal joint (otherwise you will loose good contact and also damage your own interphalangeal joint) .
Infraspinatus tenoperiostal friction massage
The patient lies in the sphinx position (prone on elbows) : 90° of elbow flexion, with the shoulder in slight lateral rotation and adduction. This is the best, but not always the most comfortable position (e.g. elderly patients or some back patients). For that reason there exists an alternative in side-lying, where the same components as in the sphinx position can be built in. Technique : the palpation, in view of finding the precise localization, is a supination movement with flexed thumb. In this way, when palpating under the spine of the scapula, in a lateral direction, the difference between muscle belly (soft), tendinous body (cable), insertion (cable and bone) and beyond the insertion (bone without cable) can clearly be felt. The deep friction itself is taking a reserve of skin in a pronation direction first, then applying pressure and performing the active phase of the movement, which is a supination. Since the skin in this area is so vulnerable, a thin layer of cotton-wool is used between the patient's skin and our thumb. It is best to perform this technique with both hands, whereby one thumb reinforces the other. Make sure the frictioning thumb stays flexed, otherwise you loose good contact.
Subscapularis tenoperiostal friction massage
Palpation : for a right subscapularis, we palpate with the left thumb under the clavicle in a lateral direction ; we reach the coracoid process. We move caudal and laterally again till we feel the lesser tuberosity (check : lateral to this bone we find the bicipital groove). Back to the lesser tuberosity, thumb in a 45° direction pointing to the nipple, make a large movement of the thumb forwards (taking the skin with us) aback to the lesser tuberosity with the thumwell flexed. The purpose is to keep a deltoid border behind our finger, so that we can reach the structure in a more optimal and direct way. While performing this backward movement we feel one or two tendoslip under our thumb (short head of biceps and coracobrachialis) and, if we keep our thumb flexed, we do not lose the anterior edge of the deltoid muscle. Now we bring our thumb back in a longitudinal direction for the deep friction. This will be a large rolling movement of the arm cephally, with the thumb as flat as
nd b
ns
5
possible , for the patient's comfort. However, a slight degree of flexion is permanently needed, in order to keep the edge of the deltoid behind our thumb during the entire friction. So we cannot release the pressure completely on the way back as in a normal deep friction.
Biceps, caput longum friction massage
Palpation : see technique for the subscapular tendon. With the patient's arm in lateral rotation, the contralateral thumb is put longitudinally into the groove and pressure is exerted sideways. The active phase of the deep friction is a medial rotation with the other arm, while the thumb exerts pressure. Remark : the groove can easily be felt, but the tendon is not always felt (depends probably on theight of the bony edges of the groove).
he
6
Elbow techniques
Biceps muscle belly friction massage
The muscle is in a relaxed position. The precise site of the lesion is found on palpation. The deep friction is a pinching technique ; the fingers are applied anteriorly to the muscle and a reserve of skin is taken in a posterior direction. Then pressure is applied (the pinch is closed as it were) and the active phase is a straight forward movement. We feel the fibres of the biceps slide under our fingers. Avoid making a circular movement and flexing too much the interfalangeal joints
Biceps insertion friction massage
We palpate the joint line between humerus and radius. Two cm more distally, the flexed thumb is applied quite medially, with the patient's arm in supination. The thumb is set in sharply and deeply. The active phase of the deep friction is bringing the patient's arm in pronation while exerting pressure with the thumb. At around ¾ of pronation, the biceps insertion slips under our thumb. The pressure is released on the way back. Some discomfort during this friction is normal
Triceps friction massage
The starting position is 90° flexion and supination. The deep friction is the normal execution with 1-3 fingers, according to the size of the lesion, and with the thumb as a fulcrum anteriorly.
7
Supinator friction massage
The starting position is ¾ extension and pronation. We find the precise spot by palpation : we palpate in the zone between radius and ulna. For a right elbow, the flexed left thumb is used, between radius and ulna. (Avoid putting the thumb cranial to the radius, in the extensor muscles.) A reserve of skin is taken in an oblique cranial direction. The deep friction is an active movement in an oblique downward direction. It is a smooth arm movement, rather than a pure thumb movement. Notice that there is not much space. Remark : make sure you have space to perform an arm movement during the friction.
Pronator teres friction massage
During palpation, we ask for a slight contraction towards pronation to make sure that we find the correct structure. The deep friction is the normal execution.
Tennis elbow type 1 friction massage
The starting position is 90° elbow flexion and supination. We palpate the lateral aspect of the lateral epicondyle, we put our thumb a little bit higher until we reach the sharp edge just above the lateral epicondyle. We flex the thumb 90°, so that the thumb-nail now faces forwards. A reserve of skin is given upwards and pressure is applied on the anterior aspect of humerus. The active phase of the deep friction is an arm movement downwards with pressure in a posterior direction, followed, as always, by a phase of relaxation.
8
Tennis elbow type 2 friction massage
The starting position is 90° flexion and supination. The therapist's thumb is 90° flexed, with the tip of the thumb lateral to the lateral epicondyle. The deep friction has to be given at the front of the epicondyle, therefore he brings his thumb now onto the anterior aspect of the bone. The correct spot is reached when only a very small range of movement is possible (a translation movement in a medial direction) and when the movement stops with a hardend-feel. The other fingers act as a fulcrum at the medial side of the elbow. The active phase of the deep friction is a translation movement at the front of the lateral epicondyle, with pressure applied in a medial/downward direction. To avoid losing contact with the lesion, the patient should not abduct his arm, nor should our thumb be put too high or too flat. Using a layer of cotton wool between finger and skin could be used to prevent damage to the skin (short finger nails are an advantage).
er
Tennis elbow type 3 friction massage
The starting position is ¾ of extension and pronation. First look for the precise localization : the tendon level with the joint line or with the radial head. The thumb is put as flat as possible on the lesion, a reserve of skin is taken in a medial direction, pressure is applied and the active phase of the deep friction is a movement in a lateral direction.
Tennis elbow type 4 palpation
The starting position is 90° flexion and supination. Level with the neck of the radius, a pinching grip with all fingers is used ; the muscle belly is lifted upwards as it were. This results automatically in a visible wrist extension.
9
Golfer elbow friction massage
Complete elbow extension. We find the medial epicondyle and proceed to the front of it. Deep friction as normally executed. Remark : - at the tenoperiosteal junction deep friction is a straight line movement and the feel is rather hard ; - at the musculotendinous junction the deep friction is a more ample round movement, and the feel is softer.
10
Wrist and hand techniques
Dorsal carpal ligament friction massage, proximal or distal row
The wrist is held flexed ; the therapist sits at the patient's ulnar side, close to the treatment table, the patient's arm slightly outside the couch. For a right wrist, the deep friction (lateral-medial) is the normal execution with the right index finger, reinforced by the middle finger.
The wrist is held flexed ; the therapist faces the patient. The deep friction (cephal-caudal) is the normal execution with the tip of the thumb.
Extensor carpi radialis longus or brevis friction massage
The therapist sits at the patient's ulnar side close to the treatment table, the patient's arm slightly outside the couch ; the wrist is held in flexion. Deep friction is normally executed with the index finger reinforced by the middle finger. The longus inserts radially on the base of the second metacarpal bone ; the brevis radially on that of the third metacarpal bone.
Extensor carpi ulnaris friction massage
The wrist is held in radial deviation. The deep friction is executed normally with the index finger, reinforced by the middle finger.
Flexor carpi radialis friction massage
The wrist is held in extension ; the deep friction is executed normally with the thumb.
11
Flexor digitorum friction massage
The wrist and the fingers are held in extension. The deep friction is executed normally with four fingers, the thumb acting as a fulcrum.
CMC 1 joint friction massage anterior part
Palpation of the joint can be done as follows. During passive ab- and adduction, or flexion and extension movements, we palpate the first metacarpal bone in a proximal direction ; first we feel only bone, then we reach the joint line and, consequently, we feel movement. For a left hand (palm facing upwards) the right thumb is put at the front of the jand the thenar muscle is pushed aside.The capsule is slightly stretched by an extension-backward movement of the patient's thumb. The active phase of the deep friction is a supination movement of the forearm. Make sure the patient's hand is outside the couch, so that there is enough space for the therapist's arm to perform the movement.
oint
is
CMC 1 joint friction massage lateral part
Changing from the anterior to the lateral part of the joint is as follows : the patient's hand is brought in a vertical position, we change thumbs (to allow our thumb to relax 5'), move laterally and stretch the capsule by bending the patient's thumb. The deep friction is executed normally.
Tenosynovitis tunnel 1 and 3 friction massage
The patient's wrist and thumb are flexed. Our thumb is put longitudinally onto the lesion, a large reserve of skin is given towards pronation, after which the deep friction is a supination movement with the ipsilateral hand.
Interosseus muscle belly friction massage
The patient's hand lies flat on the couch with the fingers slightly spread. This deep friction is an exception to the two phases rule (active phase followed by a relaxation phase). The deep friction, with a slightly bent middle finger, is a pro-supination movement, in which the pressure not released, i.e. both movements are active
phases.
Interosseus tendon friction massage
12
In order to reach the fairly palmarly situated tendon, we have to create some room for our thumb. Our middle finger pushes a knuckle up, our thumb pushes the other knuckle down. The deep friction is a supination movement with the tip of the thumb.
Starting position : slight abduction and lateral rotation. The deep friction is a pinching technique with thumb and fingers, with the heel of the hand as a fulcrum. A large reserve of skin is taken in a lateral direction, then pressure is applied and the active phase of the deep friction is a horizontal movement in a medial direction.
Adductor longus tenoperiostal friction massage
Starting position : slight abduction and lateral rotation. For a right adductor longus we palpate in the cranial direction with the left middle finger until we feel the inferior edge of the pubic bone : the finger is then turned 45° medially and now feels bone and tendon at the same time. It is reinforced by the other middle finger. The deep friction is executed normally.
Psoas muscle belly friction massage
The patient adopts the half-lying position. Site of the lesion : below the inguinal ligament and medial to the sartorius muscle. For a right psoas muscle, we use the right index and middle fingers, reinforced by the left middle and ring fingers. Make sure that during the DF you keep a deep contact. Remark : for the patient's comfort, it is essential to keep the fingers horizontal and to increase the pressure gradually.
Rectus femoris tendon friction massage
The patient sits with 90° hip flexion. We find the tendon just lateral to the sartorius muscle. For a right rectus femoris, the flexed fingers of the left hand, reinforced by the fingers of the other hand, grasp the tendon. The deep friction is the normal execution with an active phase towards the therapist.
13
Iliotibial band friction massage
The patient lies on his side with a cushion between his knees. The therapist takes a reserve of skin towards himself, then puts the thumb onto the lesion and reinforces it with the heel of the other hand ; both arms are extended. The deep friction is the normal execution, in which the active phase is a forward movement of the entire trunk. The patient's pelvis is stabilized by the therapist's thigh and fingers.
Hamstrings muscle belly friction massage
The muscle is in a fully relaxed position (prone lying, knees 90° flexed). The deep friction is the normal execution with all fingers, covering a large area in order to limit the risk of adhesion formation.
Hamstrings origin friction massage
The patient lies on his side with the hips and the knees in 90° flexion. The deep friction is executed normally with two or three fingers ; they feel the ischium and the tendons at the same time. Remark : it is easier to work in close contact with the patient on a higher treatment table.
14
Knee techniques
Medial collateral ligament friction massage
The friction is given in as much extension and flexion as possible. The knee is supported by a cushion. For a left knee, we use the left middle or index finger ; we find the joint line and we palpate in a posterior direction until, beyond the midline, the ligament is found (a large flat structure). The deep friction is the normally executed. For the deep friction in flexion, we find the lesion in extension first, keep our finger on it, and bend the knee. The deep friction, again, is the normal execution. Notice that the direction in which the ligament now lies has changed, and so has the direction of our friction.
Lateral collateral ligament friction massage
The knee is extended ; we palpate the joint line in a posterior direction. We feel, successively, bone, then a thin flat structure (iliotibial tract), bone again and then a tendon-like structure, the LCL. Even more laterally, the biceps tendon can be found. The DF is the normal execution.
Medial coronary ligament friction massage
The starting position is 90° flexion and lateral rotation. For the left knee, we place the left index finger onto the tibial plateau. The finger nail faces upwards ; in this way, pressure can be applied in a downward direction. The thumb should be put far down, in order to maintain this pressure. The deep friction is normally executed. For a lateral coronary ligament, the knee is in medial rotation.
Quadriceps muscle belly friction massage
The muscle is in a shortened position, i.e. with the patient sitting, without a cushion under the knee. Large contact with both hands ; the deep friction is the normal execution with all fingers. The active phase of the DF is reinforced by a backward movement of the trunk ; the relaxation phase is the forward movement.
Suprapatellar : the distal half of the patella is pushed in a posterior direction, so as to make the proximal part tilt forwards, which makes it easier to reach the lesion. The deep friction is the normal execution with the ring finger, reinforced by the middle finger, using the thumb more distally as a fulcrum. The pressure is applied towards the toes. Since the lesion lies tenoperiosteally, there is contact with the contractile structure and the bone at the same time. Infrapatellar : now, the upper half of the patella is pushed posteriorly. The deep friction is the same as above.
Quadriceps parapatellar medial friction massage
For a left knee, the right thumb pushes the patella in a medial direction. The left hand is in supination ; the ring finger, reinforced by the middle finger, exerts an anterior pressure on the back of the patella. The deep friction is the normal execution, i.e. a reserve of skin in a cranial direction, then pressure is applied, the active phase is a caudal movement with pressure in an anterior direction. It is an arm not a finger movement. The forearm remains parallel to the patient's leg. For practical reasons, the deep friction is done in a caudal direction.
Biceps femoris tendon friction massage
The patient lies prone with his foot beyond the edge of the couch. He actively holds his foot up for a moment, to enable us to find the tendon more easily. The deep friction is the normal execution with 1, 2 or 3 fingers, according to tsize of the lesion.
he
16
Pes anserinus friction massage
We palpate the soft structures from distal to proximal until we find the bony edge of the tibia, then we move 1 cm distally again. The fingers are applied in a 45° medial-downward direction. The deep friction is the normal execution with four finger tips, reinforced by the other hand.
Popliteus muscle belly friction massage
The patient lies prone with his knee slightly bent. We first palpate the head of the fibula, then 1 ½ cm cephally up the joint line, and another 1 ½ cm cephally lies the insertion on the lateral femoral condyle. From here, we imagine a 45° line caudally and the muscle belly lies fanwise around this line. We look for the most tender spot, pull the skin towards us (= reserve of skin) and apply the flat thumb on the lesion. It is reinforced by the heel of the hand ; the therapist's arms are straight. The deep friction consists of an active phase medially-upwards, followed by a relaxation phase. It is more a trunk movement than an arm movement. In order to work comfortably, the pressure is only gradually increased.
Popliteus origo friction massage
Starting position : 90° knee flexion. About 1 cm from the edge of the femoral condyle, we find a vertical sulcus, containing the popliteal tendon. The deep friction is performed by the left or the right thumb of choice. The tip of the thumb is put vertically into the sulcus ; the active phase of the deep friction is a transverse movement towards the left or the right. The sulcus can always be felt, but the tendon may not be felt.
17
Foot and ankle techniques
ndment
Gastrocnemius muscle belly friction massage
Starting position : plantarflexion and slight knee flexion. The DF is the normal execution, carried out with all fingers, regardless of the size of the lesion. In such a way the risk of adhesions is significantly smaller. Make sure to take enough reserve of skin, so that the range can be big enough. The DF-movement can be guided by a body-movement.
The therapist can either stand or sit. The thigh immobilizes the foot in dorsiflexion in order to bring some tension in the tendon. The DF is a pinching technique with thumb and index finger, reinforced by the middle finger. A large reserve of skin is given in an anterior direction, then pressure is applied athe active phase of the DF is a straight movebackwards. For the patient's comfort it is important that the therapist's DIP-joints are not flexed too much. To avoid damage to the skin it is necessary to use a thin layer of cotton wool between fingers and skin. This technique is best performed with both hands simultaneously. After having pushed the skin forwards, the therapist's arms are almost extended.
In plantiflexion the tendon is pushed medially by the therapist's thumb ; in this way the necessary space can be created. The contact with the thumb is not sharp, but flat. The DF is performed with the ring finger reinforced by the middle finger. First, a reserve of skin is taken in pronation, then pressure is applied ; the active phase of the DF is a supination movement. It is very important that the therapist's forearm remains parallel to the patient's leg. Therefore the couch is put in a rather high position to enhance the therapist's comfort.
18
Achilles tendon insertion friction massage
The starting position is once more plantiflexion. The DF is the normal execution with both index fingers. Fingers athumbs form a circle, pressure is applied towards the toes. The finger feels tendon and bone at the same time.
nd
Peronei proximal aspect friction massage
The therapist stands next to the patient. The tendons are brought on the stretch by some plantiflexion and adduction. The DF consists of the normal execution with one or more fingers (depending on the size of the lesion).
Peronei distal aspect friction massage
The starting position is the same. The DF is the normal execution with the index finger reinforced by the middle finger.
Peronei aspect behind the malleolus friction massage
Again, the tendons are in a stretched position. The therapist, however, now stands in front of the patient. This part of the tendon is treated with a supination technique with the ring finger, reinforced by the middle finger. All finger joints are slightly flexed. A reserve of skin is given in pronation ; the active phase of the DF is a supination movement.
The therapist's thigh keeps the foot in dorsiflexion. The entire ring finger is put on the lesion and a reserve of skin is taken in pronation ; pressure is applied and the active phase of the DF is a supination movement. Reinforcing the ring finger with the fingers of the other hand makes the active phase even more effective and certainly more practical.
19
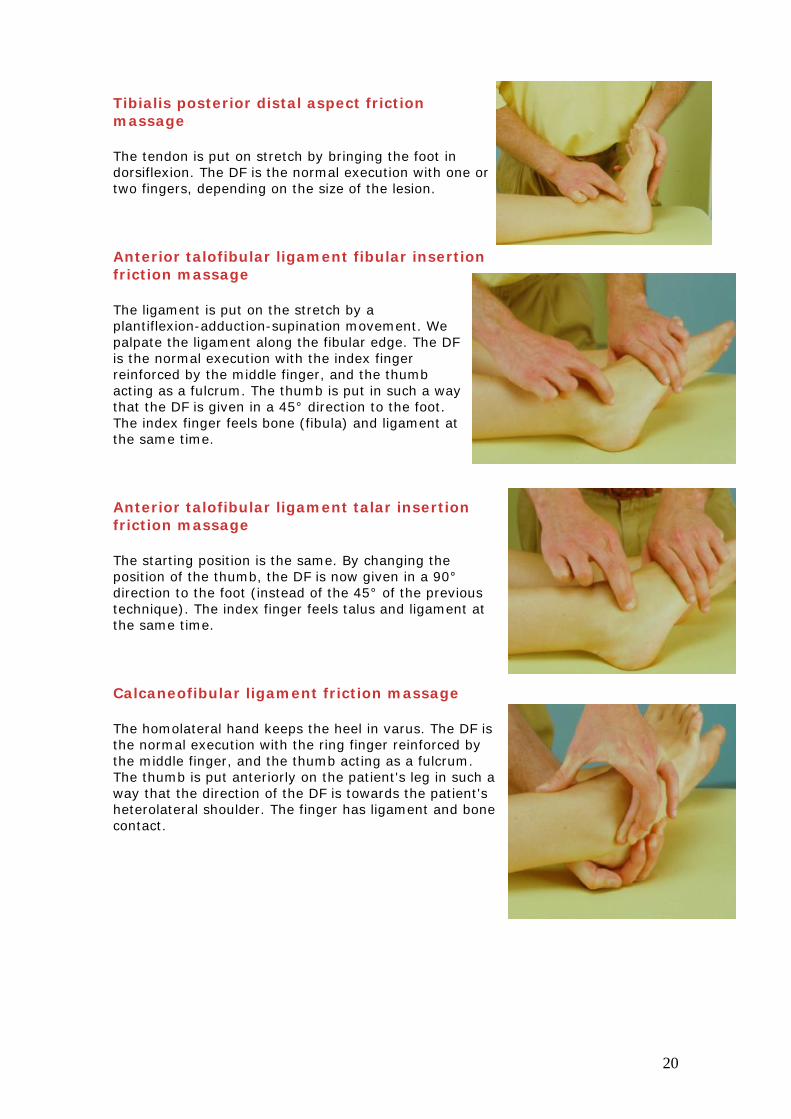
Tibialis posterior distal aspect friction massage
The tendon is put on stretch by bringing the foot in dorsiflexion. The DF is the normal execution with one or two fingers, depending on the size of the lesion.
The ligament is put on the stretch by a plantiflexion-adduction-supination movement. We palpate the ligament along the fibular edge. The DF is the normal execution with the index finger reinforced by the middle finger, and the thumb acting as a fulcrum. The thumb is put in such a way that the DF is given in a 45° direction to the foot. The index finger feels bone (fibula) and ligament at the same time.
The starting position is the same. By changing the position of the thumb, the DF is now given in a 90° direction to the foot (instead of the 45° of the previous technique). The index finger feels talus and ligament at the same time.
Calcaneofibular ligament friction massage
The homolateral hand keeps the heel in varus. The DF is the normal execution with the ring finger reinforced by the middle finger, and the thumb acting as a fulcrum. The thumb is put anteriorly on the patient's leg in such a way that the direction of the DF is towards the patient's heterolateral shoulder. The finger has ligament and bone contact.
20
Calcaneocuboid ligament friction massage
The foot is kept in some mid-tarsal adduction. Palpation : we stand medially to the patient's foot. We place our heterolateral thumb first on the head of the fifth metatarsal bone, then next to it (proximal) ; now the joint line between cuboid and calcaneus lies just proximal to our thumb. Our ifinger palpates along the joint line from the sole tothe dorsum of the foot : first a peroneal tendon ifelt, then bone and eventually a flat soft structure, which is the calcaneocuboid ligament. The DF is the normal execution with the index finger reinforced by the middle finger, and the thumb acting as a fulcrum.