36
Cystic Fibrosis Module C Chapter 41
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | cody-conley |
| View: | 214 times |
| Download: | 0 times |

Cystic Fibrosis
Module C
Chapter 41

Objectives
• State the clinical definition for Cystic Fibrosis. Describe the anatomic alterations of the lungs in Cystic Fibrosis.
• Describe the etiology of Cystic Fibrosis. • List the clinical manifestations seen in Cystic
Fibrosis. • Describe the management of Cystic Fibrosis. • Indicate the lab test used to evaluate a patient
for cystic fibrosis and give normal values and values used to identify cystic fibrosis.

Definition
• Formerly known as MucoviscidosisMucoviscidosis.
• An inherited disease of the exocrine glands, primarily affecting the GI and respiratory systems, and usually characterized by COPD, exocrine pancreatic insufficiency, and abnormally high sweat electrolytes.

Exocrine Glands
• Exocrine glands are glands whose secretions pass into a system of ducts that lead ultimately to the exterior of the body.• Sweat Glands• Pancreatic ducts• Intestinal ducts• Liver & bile ducts • Reproductive glands• Lungs (bronchial glands)

Incidence
• Most common life-shortening disease genetic disease in US• Affects about 30,000 children and adults in
US.• 1 in 3,500 live births.
• Greater incidence in white births.
• 10,000,000 symptomless carriers (1 in 25).• 80% diagnosed by age three; ~10% at age 18
or older.

Etiology
• Various mutations of a single gene located on chromosome 7.
• Gene cells normally produce a protein called Cystic Fibrosis Transmembrane Regulator (CFTR).
• A mutation known as F508 results in deletion of the amino acid phenylalanine at position 508 of the CFTR protein. (70% of all cases)
• This results in a defect in chloride transport by epithelial cells (also Na and K).

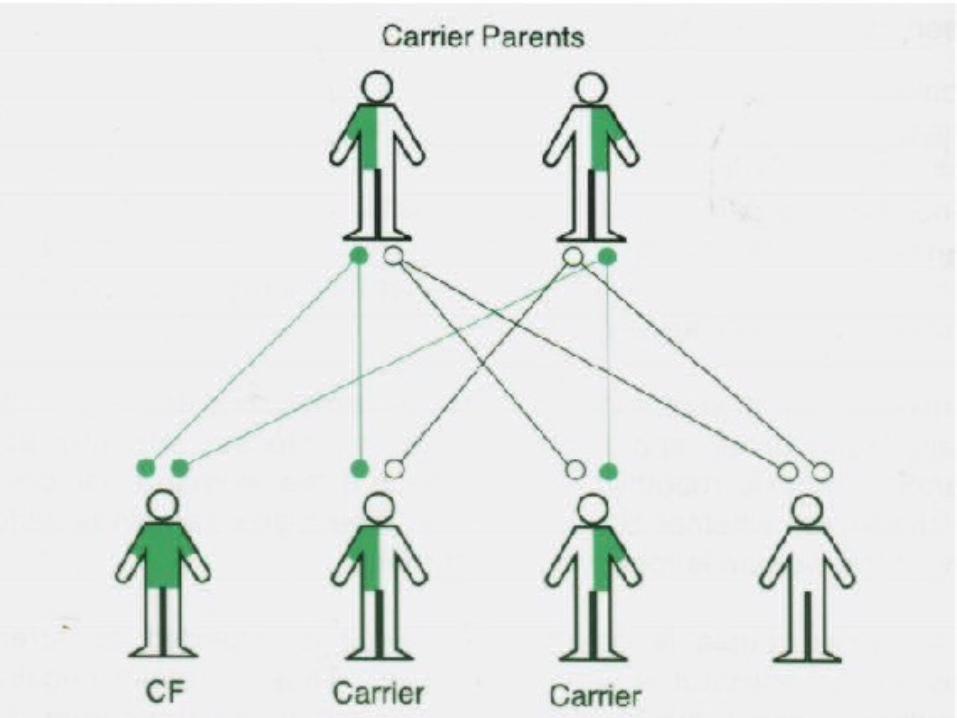
Etiology• Carriers of a single defective gene have no
clinical disease.• If both parents are carriers, children who
inherit one abnormal gene from each parent will be homozygoushomozygous and develop CF.
• Regardless of sex, the children of two carrier parents will have:• a 25% chance of having CF,• a 50% chance of being carriers, • a 25% of being normal (non-carrier).

Pathology
• Nearly all exocrine glands are affected in varying degree of severity.
• Three types of defects:• Glands become obstructed by viscid material
(pancreas, intestines, bile ducts, gallbladder).• Increased secretion of abnormal mucus (bronchial
glands)• Histologically normal cells, but increased secretion of
Sodium and Chloride (sweat glands).
• The lungs may appear normal at birth but abnormal structural changes occur rapidly.

Pathophysiology - Pulmonary• Bronchial glands hypertrophyhypertrophy and there is metaplasiametaplasia of
goblet cells.• Impairment of mucociliary clearance.• Mucous plugging leads to hyperinflation and atelectasis.• Retained secretions lead to frequent infections
(pneumonia).• Staphylococcus aureus• Haemophilus Influenza• Pseudomonas Aeruginosa (mucoid variant)
• Smooth muscle constriction.• Chronic bronchitis, bronchiectasis and lung abscess.• AIRWAYS – NOT GAS EXCHANGE UNITS.

Pathophysiology - Intestinal Tract• Meconium Ileus: Obstruction of
the small intestine of the newborn caused by impaction of thick, dry tenacious meconiummeconium, usually at or near the ileocecal valve.• Deficiency of pancreatic enzymes• Earliest manifestation of CF
• Newborns have abdominal distention and fail to pass stool within 12 hours after birth
• Intestinal Obstruction occurs in older children and adults
Pathophysiology - Pancreas
• Pancreatic ducts become plugged with mucous which leads to fibrotic changes.
• Cannot digest fats, proteins and cannot break down nutrients.• Deficiency of vitamins A, D, E, K.
• Vitamin K deficiency leads to easy bruising and bleeding.
• Patients have difficulty gaining weight.• Cachectic
• Vitamin D deficiency leads to absorption of Calcium and Phosphorus.
• Diabetes

Pathophysiology – Sweat Glands
• Glands secrete up to 4 times the normal amount of Na and Cl.• The actual volume of sweat does not change.
• Sweat Chloride concentration can be used as a diagnostic indicator.• “Kiss a baby”• Greater than 60 mEq/L is diagnostic in
children.• In adults, a concentration of greater than 80
mEq/L is usually required for a diagnosis.
Pathophysiology – Other
• Nasal Polyps and Sinusitis• 20% of patients.• Polyps are multiple and may cause nasal
obstruction and distortion of normal facial features.
• Sterility• 99% of men and many women are sterile. • Women not likely to carry fetus to term.• Infant will have cystic fibrosis or will be a
carrier.

Signs & Symptoms
• Vital Signs:• Tachypnea• Tachycardia• Hypertension• May have increased temperature if infection present.
• Inspection:• Use of accessory muscles during I & E.• Increased A-P diameter of the chest.• Pursed lip breathing.• Clubbing• Cyanosis

Signs & Symptoms
• Palpation:• Decreased tactile and vocal fremitus.
• Percussion• Hyperresonant percussion note.
• Auscultation• Diminished breath sounds.• Crackles, rhonchi, wheezing.
Cor Pulmonale
• Chronic hypoxemia • Polycythemia• Pulmonary hypertension.• Distended neck veins.• Enlarged and tender liver.• Peripheral edema.• Pitting edema.
Spontaneous Pneumothorax
• 20% greater incidence.• 50% recurrence rate.
• Symptoms include:• Pleuritic pain• Shoulder pain• Sudden dyspnea
• Can be precipitated by • Excessive exertion• High altitude• Positive pressure breathing
Pulmonary Function
• Obstructive Picture:• Decreased FVC• Decreased flowrates• Increased RV, TLC, FRC• Flow Volume Loop
• Scooped out

Arterial Blood Gases
• Mild to Moderate CF• Acute alveolar hyperventilation with
hypoxemia.
• Severe CF• Chronic ventilatory failure with hypoxemia.• Increased shunting.• Watch out for “acute on chronic” condition
during exacerbations of disease.
Chest X-ray
• Translucent (dark)
• Depressed or flattened diaphragms
• Right ventricular enlargement
• Areas of atelectasis and fibrosis
• Pneumothorax
• Abscess formation

Treatment• Oxygen Therapy
• Treat hypoxemia ( / , shunt)
• Nutritional Support• Pancreatic Enzymes to aid food digestion• Increase of calories by 50 – 100%• Multivitamins and minerals• Salt
• Mobilization of Bronchial Secretions• Bronchial Hygiene Protocol• Hyperinflation Protocol• Aerosolized Medication Protocol
Bronchial Hygiene
• Hydration
• Cough Techniques• Active Cycle Breathing, Autogenic Drainage,
• Deep Breathing• IS, Flutter, PEP therapy
• Chest Physical Therapy• Percussion & Vibration• Postural Drainage
• Mucolytic Therapy
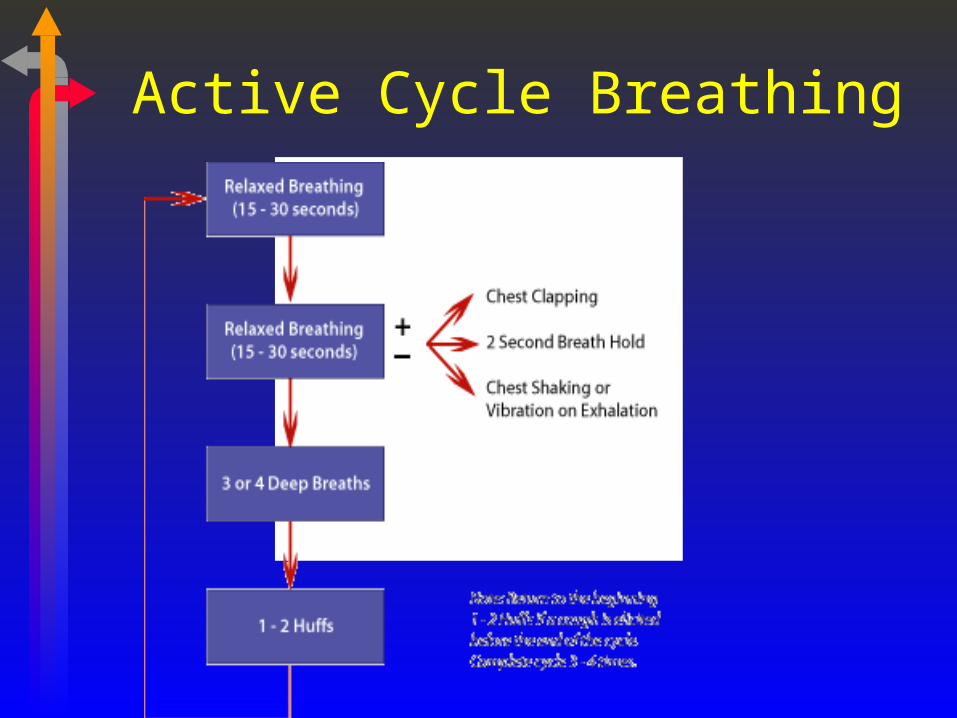
Active Cycle Breathing

Autogenic Drainage

PEP Therapy
• Used in the management of airway secretions and atelectasis.
• Patient is instructed to inhale a volume of air larger than Vt through a one way valve.
• Exhale actively through a fixed orifice to a normal level.
• Fixed orifice is chosen to achieve a PEP of 10 to 20 cm H2O during exhalation.
• Perform 10-20 breaths followed by coughs.

PEP Therapy


Postural Drainage & Percussion
High Frequency Chest Wall Compression
• ThAIRapy Vest• Inflatable, personally
fitted jacket attached to a large pump that generates variable high frequency oscillations and applies that directly to the chest wall.
• Pulse frequency is set for 5-25 Hertz (300 to 1500 cycles/min).
Aerosolized Medications
• Mucolytics - Pulmozyme
• Sympathomimetics
• Parasympatholytics
• Xanthines
• Antibiotics - tobramycin, colisitin

Mechanical Ventilation
• Treat increased PaCO2 (and low pH)• Use caution with increasing tidal volume.
• Increased RV leads to overdistension.• Extend expiratory time.
• Auto PEEP
• Shorten inspiratory time (increase inspiratory flow rate).
• Use respiratory rate to control PaCO2.• Control patient (?) pharmacologically.• Permissive hypercapnia and acidosis.
• Treat reduced PaO2
• Usually a result of hypoventilation and / imbalance.
• Responds well to increase in FIO2.

Home Care
• Patient, family education
• Home oxygen
• Aerosol therapy
• CPT/PD

Future Therapies
• denufosol tetrasodium• denufosol is designed to enhance the lung's
innate mucosal hydration and mucociliary clearance through stimulation of the P2Y2 receptor.
• HUH?

Prognosis
• Diagnostic testing for the abnormal gene is now available.
• Life expectancy is 37 years of age (CF Foundation) with some patients living past 40 years. Death is usually due to pulmonary complications• Respiratory failure• Heart failure










