Cytomegalovirus Granulomatous Hepatitis ]OHN CLARKE, M.D. ROBERT M. CRAIG, M.D. RICHARD SAFFRO. M.D. PATRICK MURPHY, M.D. HlDI]IRO YOKOO. M.D. Chicugo, Jllinois From the Infectious Diseases and Gastroenter- ology Sections, Department of Medicine, and from the Pathology Department, Northwestern University Medical School and the Veterans Administration Lakeside Hospital, Chicago, II- linois. Requests for reprints should be addressed to Dr. John Clarke, Department of Medicine, Northwestern Memorial Hospital, 251 East Su- perior Avenue, Chicago, Illinois 68611. Manu- script accepted July 5.1978. Three patients with granulomatous hepatitis due to cytomegalovirus are described. They are compared to the three previously described patients with this disease, and their clinical and serologic charac- teristics are discussed. Similarities and differences between infec- tious mononucleosis (Epstein-Barr virus) and cytomegalovirus in- fections are adduced. That cytom&galovirus may he a cause of granulomatous hepatitis in the adult is stressed. Cytomegalovirus (CMV) is an unusual cause of granulomatous hepa- titis. We have recently seen three patients who presented with pro- longed, unexplained fever, and who were found to have granuloma- tous hepatitis and CMV infection. Two of these patients are consid- erably older than those previously described and point out the need for awareness of this entity in older adults. These three patients are described and compared to three previously described patients with CMV granulomatous hepatitis. CASE REPORTS Case 1. A 55 year old school teacher was admitted to Northwestern Memorial Hospital in October 1976 with a two week history of chills, fever, night sweats, myalgias and mild photophobia. One month prior to admission, transient di- arrhea occurred following a trip to California. She had never worked with beryllium but had received a I U blood transfusion in 1949. On admission, her temperature was 39.2’C, pulse rate Wmin, respirations 18/min and blood pressure 110/60 mm Hg. She was not icteric. her neck was supple, and her chest was clear. No murmurs were present. There was no hepatosplenomegaly or lymphadenopathy. and the ncurologic examination was within normal limits. She was mildly anemic and had a marked lymphocytosis. The chest roent- genogram revealed atelectasis in the lower lobe of the left lung and minimal blunting of the left costophrenic angle. Liver scan, electrocardiogram, upper gastrointestinal tract and gallbladder roentgenograms were within normal limits. Stool examinations for ova, parasites and fecal leukocytes were negative, and stool cultures did not reveal enteric pathogens. Hcterophil tests and tox- oplasma serologies were negative. Nonspecific cold agglutinins and agglutinins to anti-1 activity were present at 1:8 and 1:64 dilutions, respectively. Comple- ment fixing antibody titers against CMV rose from less than 1:lO to 1:320. Urine culture on the ninth hospital day was negative, but urine cultures one week later and two months after discharge were positive for CMV. Corresponding complement fixation titers were <l:lO, 1:40 and 1:80. Five months after dis- charge, urine culture for CMV was negative. The patient’s liver test results and hematologic values are outlined in Table I. A bone marrow aspirate revealed small areas of histiocytic aggregation as well as slight lymphocytosis and plasmacytosis. The liver biopsy specimen revealed some areas of focal liver 264 February 1979 The American Journal of Medicine Volume 66
Transcript
Cytomegalovirus Granulomatous Hepatitis
]OHN CLARKE, M.D.
ROBERT M. CRAIG, M.D.
RICHARD SAFFRO. M.D.
PATRICK MURPHY, M.D.
HlDI]IRO YOKOO. M.D.
Chicugo, Jllinois
From the Infectious Diseases and Gastroenter- ology Sections, Department of Medicine, and from the Pathology Department, Northwestern University Medical School and the Veterans Administration Lakeside Hospital, Chicago, II- linois. Requests for reprints should be addressed to Dr. John Clarke, Department of Medicine, Northwestern Memorial Hospital, 251 East Su- perior Avenue, Chicago, Illinois 68611. Manu- script accepted July 5.1978.
Three patients with granulomatous hepatitis due to cytomegalovirus are described. They are compared to the three previously described patients with this disease, and their clinical and serologic charac- teristics are discussed. Similarities and differences between infec- tious mononucleosis (Epstein-Barr virus) and cytomegalovirus in- fections are adduced. That cytom&galovirus may he a cause of granulomatous hepatitis in the adult is stressed.
Cytomegalovirus (CMV) is an unusual cause of granulomatous hepa- titis. We have recently seen three patients who presented with pro- longed, unexplained fever, and who were found to have granuloma- tous hepatitis and CMV infection. Two of these patients are consid- erably older than those previously described and point out the need for awareness of this entity in older adults. These three patients are described and compared to three previously described patients with CMV granulomatous hepatitis.
CASE REPORTS
Case 1. A 55 year old school teacher was admitted to Northwestern Memorial Hospital in October 1976 with a two week history of chills, fever, night sweats, myalgias and mild photophobia. One month prior to admission, transient di- arrhea occurred following a trip to California. She had never worked with beryllium but had received a I U blood transfusion in 1949.
On admission, her temperature was 39.2’C, pulse rate Wmin, respirations 18/min and blood pressure 110/60 mm Hg. She was not icteric. her neck was supple, and her chest was clear. No murmurs were present. There was no hepatosplenomegaly or lymphadenopathy. and the ncurologic examination was within normal limits.
She was mildly anemic and had a marked lymphocytosis. The chest roent- genogram revealed atelectasis in the lower lobe of the left lung and minimal blunting of the left costophrenic angle. Liver scan, electrocardiogram, upper gastrointestinal tract and gallbladder roentgenograms were within normal limits. Stool examinations for ova, parasites and fecal leukocytes were negative, and stool cultures did not reveal enteric pathogens. Hcterophil tests and tox- oplasma serologies were negative. Nonspecific cold agglutinins and agglutinins to anti-1 activity were present at 1:8 and 1:64 dilutions, respectively. Comple- ment fixing antibody titers against CMV rose from less than 1:lO to 1:320. Urine culture on the ninth hospital day was negative, but urine cultures one week later and two months after discharge were positive for CMV. Corresponding complement fixation titers were <l:lO, 1:40 and 1:80. Five months after dis- charge, urine culture for CMV was negative. The patient’s liver test results and hematologic values are outlined in Table I. A bone marrow aspirate revealed small areas of histiocytic aggregation as well as slight lymphocytosis and plasmacytosis. The liver biopsy specimen revealed some areas of focal liver
264 February 1979 The American Journal of Medicine Volume 66
CYTOMEGALOVIRUS GRANULOMATOUS HEPATITIS-CLARKE ET AL.
NOTE: Values in parentheses under column headings represent normal values. LDH = lactic dehydrogenase; SGOT = serum glutamic ox- aloacetic transaminase; ND = not determined ‘ Per 100 white blood cells + January 25, 1977.
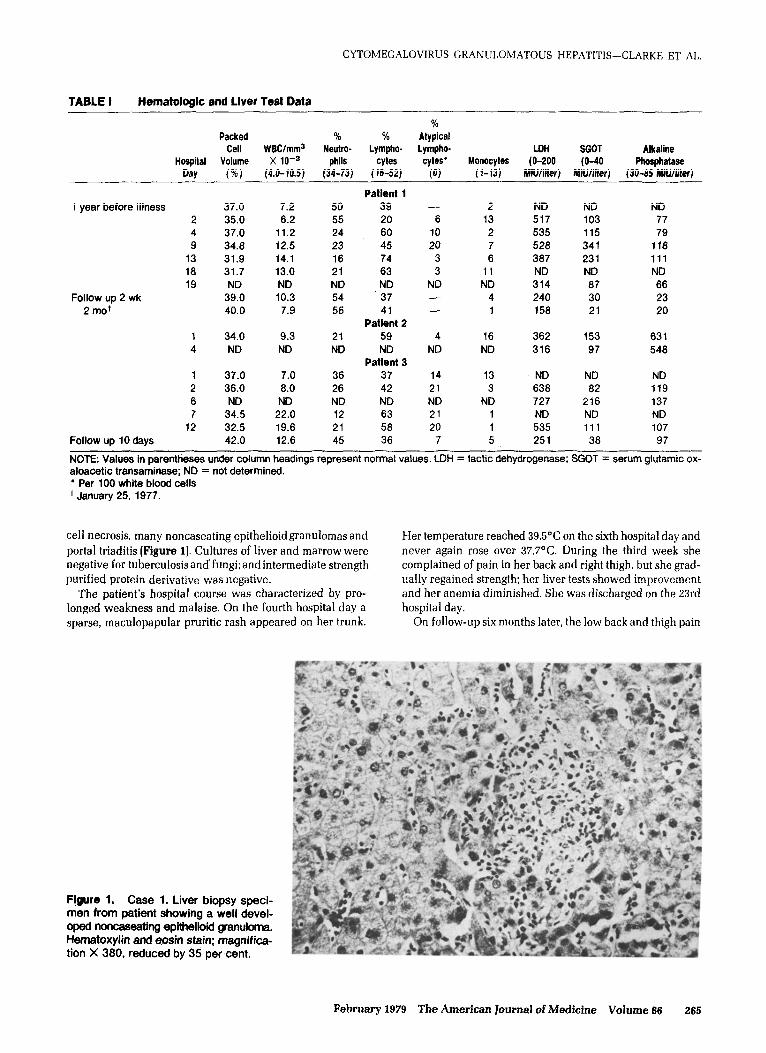
cell necrosis. many noncaseating epithelioidgranulomas and portal triaditis (Figure 1). Cultures of liver and marrow were negative for tuberculosisand’fungi;andintermediate strength purified protein derivative was negative.
The patient’s hospital course was characterized by pro- longed weakness and malaise. On the fourth hospital day a sparse, maculopapular pruritic rash appeared on her trunk.
Her temperature reached 39.5”C on the sixth hospital day and never again rose over 37.V’C. During the third week she complained of pain in her back and right thigh, but she grad- ually regained strength, her liver tests showed improvement and her anemia diminished. She was discharged on the 23rd hospital day.
On follow-up six months later, the low back and thigh pain
Figure 1. Case 1. Liver biopsy speci- men from patient showing a well devel- oped noncaseating epithelioid gfanufotna. Hematoxylin and eosin stain: magnifica- tion X 380, reduced by 35 per cent.
February 1876 The American Journal of Medicine Volume 66 265
CYTOMEGALOVIRUS GRANULOMATOUS HEPATITIS-CLARKE ET AL.
had resolved. The liver and spleen were not palpable, and the The temperature was 38%. respirations Wmin, pulse rate patient appeared dramatically improved. Repeat purified 65/min and blood pressure llQ/55 mm Hg. There was no ic- protein derivative was negative, and a Varidasee skin test was terus, hepatosplenomegaly, adenopathy or evidence of positive. bleeding.
Case 2. A 60 year old white housewife was well until the last week of October 1976 when generalized malaise developed. Two weeks later, she noted aching in her legs, fever and oc- casional drenching sweats. She had never received a trans- fusion. She was admitted to another hospital in late October with a temperature of 38.6%. She was icteric. A liver-spleen scan revealed spotty hepatic uptake and increased splenic uptake. A liver biopsy was unsuccessful, and she was trans- ferred to Northwestern Memorial Hospital on November 11, 1976.
Hematologic values, liver tests and sero!ogic data are shown in Table I. The patient was mildly anemic. A marked lym- phocytosis with 14 per cent atypical forms was noted at the first hospital. Titers against Proteus 0X-19, OXK and Proteus 0 were 1:320,1:40 and l:20, respectively. Antinuclear antibody (ANA) was present at 1:lO dilutions with a homogeneous pat- tern, and rheumatoid factor was positive at a titer of 1640. The chest roentgenogram revealed a modest right pneumothorax. The electrocardiogram was within normal limits.
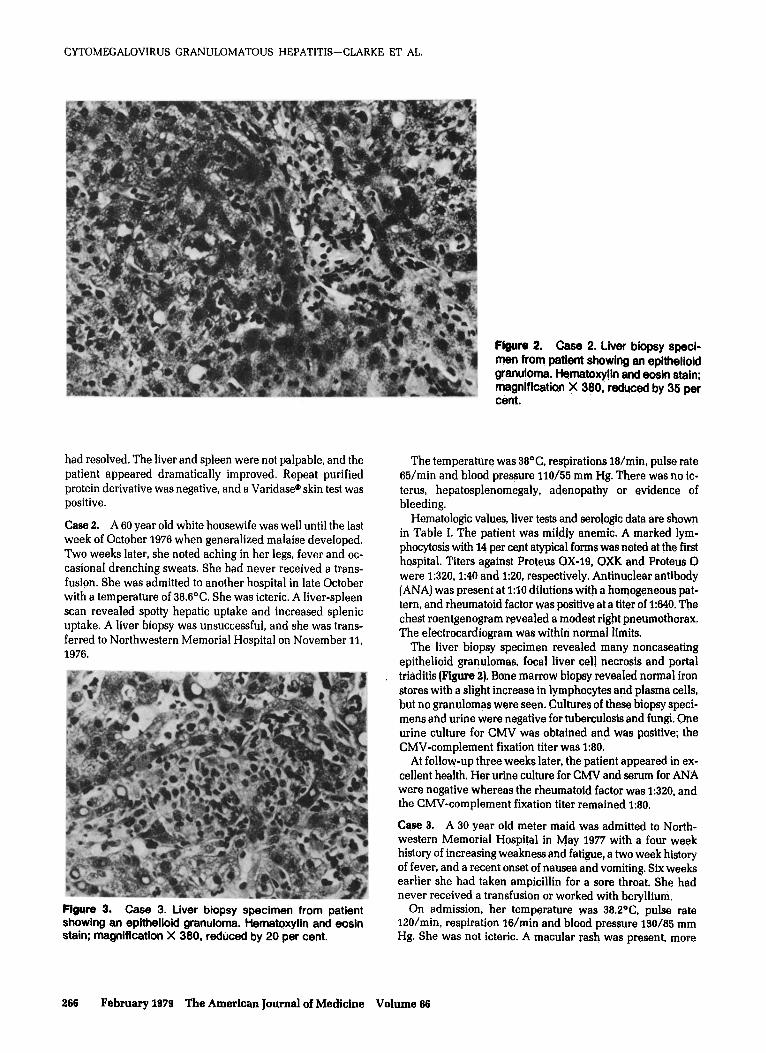
The liver biopsy specimen revealed many noncaseating epithelioid granulomas, focal liver cell necrosis and portal triaditis (Figure 2). Bone marrow biopsy revealed normal iron stores with a slight increase in lymphocytes and plasma cells, but no granulomas were seen. Cultures of these biopsy speci- mens and urine were negative for tuberculosis and fungi. One urine culture for CMV was obtained and was positive: the CMV-complement fixation titer was 1:80.
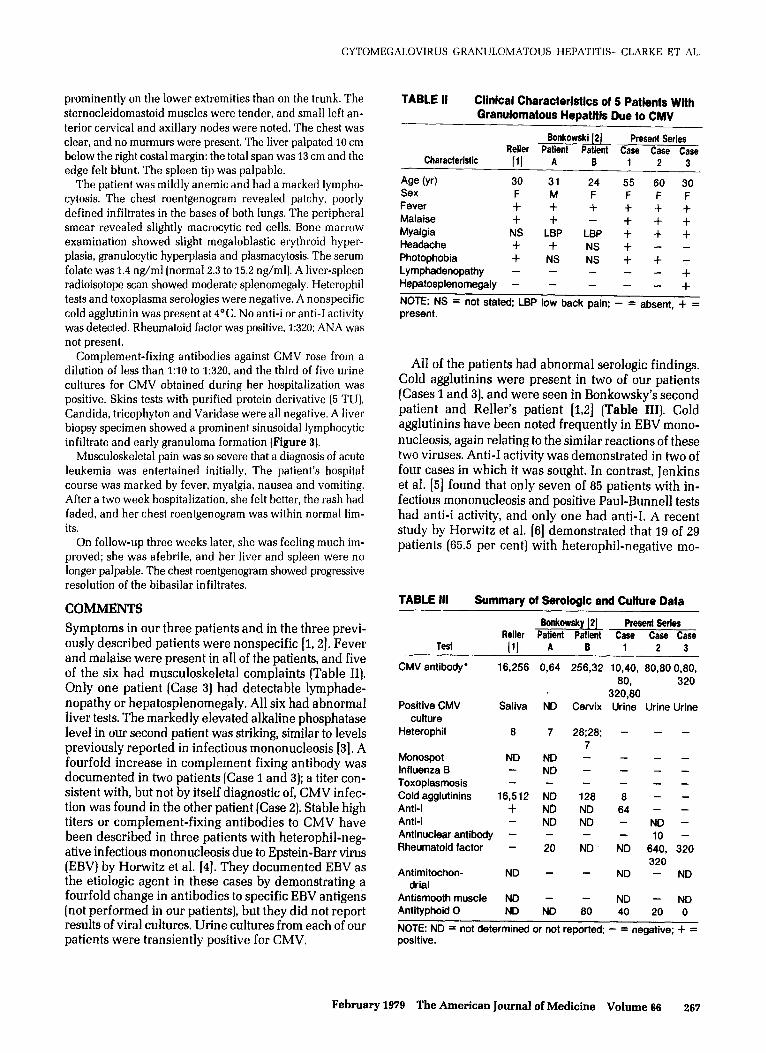
Figure 3. Case 3. Liver b _r_, _r__ .._ _.. _._... r-_.-_._ showing an epithelioid granuloma. Hematoxylin and eosin stain; magnification X 380, reduced by 20 per cent.
Figure 2. Case 2. Liver biopsy speci- men from patient showing an epithelioid granuloma. Hematoxy!in and eogin stein; magnification X 380, reduced by 35 per cent.
At follow-up three weeks later, the patient appeared in ex- cellent health. Her urine culture for CMV and serum for ANA were negative whereas the rheumatoid factor was 1:320, and the CMV-complement fixation titer remained 1:80.
Case 3. A 30 year old meter maid was admitted to North- western Memorial Hospital in May 1977 with a four week history of increasing weakness and fatigue, a two week history of fever, and a recent onset of nausea and vomiting. Six weeks earlier she had taken ampicillin for a sore throat. She had never received a transfusion or worked with beryllium,
On admission, her temperature was 38.2%, pulse rate 12O/min, respiration lG/min and blood pressure 130/85 mm Hg. She was not icteric. A macular rash was present, more
266 February 1979 The American Journal of Medicine Volume 66
prominently on the lower extremities than on the trunk. The sternocleidomastoid muscles were tender, and small left an- terior cervical and axillary nodes were noted. The chest was clear, and no murmurs were present. The liver palpated 10 cm below the right costal margin: the total span was 13 cm and the edge felt blunt. The spleen tip was palpable.
The patient was mildly anemic and had a marked lympho- cytosis. The chest roentgenogram revealed patchy, poorly defined infiltrates in the bases of both lungs. The peripheral smear revealed slightly macrocytic red cells. Bone marrow examination showed slight megaloblastic erythroid hyper- plasia, granulocytic hyperplasia and plasmacytosis. The serum folate was 1.4 ng/ml [normal 2.3 to 15.2 ng/ml). A liver-spleen radioisotope scan showed moderate splenomegaly. Heterophil tests and toxoplasma serologies were negative. A nonspecific cold agglutinin was present at 4°C. No anti-i or anti-1 activity was detected. Rheumatoid factor was positive, 1:320; ANA was not present.
Complement-fixing antibodies against CMV rose from a dilution of less than 1:lO to 1:320. and the third of five urine cultures for CMV obtained during her hospitalization was positive. Skins tests with purified protein derivative (5 TU), Candida, tricophyton and Varidase were all negative. A liver biopsy specimen showed a prominent sinusoidal lymphocytic infiltrate and early granuloma formation [Figure 3).
Musculoskeletal pain was so severe that a diagnosis of acute leukemia was entertained initially. The patient’s hospital course was marked by fever, myalgia, nausea and vomiting. After a two week hospitalization, she felt better, the rash had faded, and her chest roentgenogram was within normal lim- its.
On follow-up three weeks later, she was feeling much im- proved; she was afebrile. and her liver and spleen were no longer palpable. The chest roentgenogram showed progressive resolution of the bibasilar infiltrates.
COMMENTS
Symptoms in our three patients and in the three previ- ously described patients were nonspecific [1,2]. Fever and malaise were present in all of the patients, and five of the six had musculoskeletal complaints (Table II). Only one patient (Case 3) had detectable lymphade- nopathy or hepatosplenomegaly. All six had abnormal liver tests. The markedly elevated alkaline phosphatase level in our second patient was striking, similar to levels previously reported in infectious mononucleosis [3]. A fourfold increase in complement fixing antibody was documented in two patients (Case 1 and 3); a titer con- sistent with, but not by itself diagnostic of, CMV infec- tion was found in the other patient (Case 2). Stable high titers or complement-fixing antibodies to CMV have been described in three patients with heterophil-neg- ative infectious mononucleosis due to Epstein-Barr virus (EBV) by Horwitz et al. [a]. They documented EBV as the etiologic agent in these cases by demonstrating a fourfold change in antibodies to specific EBV antigens (not performed in our patients], but they did not report results of viral cultures. Urine cultures from each of our patients were transiently positive for CMV.
CYTOMEGALOVIRUS GRANULOMATOUS HEPATITIS-CLARKE ET AL.
TABLE II Clinical Characteristics of 5 Patients With Granulomatous Hepatitis Due to CMV
Bonkowski 121 Present Series Reller Patient Patient Case Case Case
All of the patients had abnormal serologic findings. Cold agglutinins were present in two of our patients (Cases 1 and 31, and were seen in Bonkowsky’s second patient and Reller’s patient [1,2] (Table III). Cold agglutinins have been noted frequently in EBV mono- nucleosis, again relating to the similar reactions of these two viruses. Anti-I activity was demonstrated in two of four cases in which it was sought. In contrast, Jenkins et al. [5] found that only seven of 85 patients with in- fectious mononucleosis and positive Paul-Bunnell tests had anti-i activity, and only one had anti-I. A recent study by Horwitz et al. [6] demonstrated that 19 of 29 patients (65.5 per cent) with heterophil-negative mo-
TABLE ill Summary of Serologic and Culture Data
6onkowsky [2] Present Series Reller Patient Patient Csse Case Case
NOTE: ND = not determined or not reported; - = negative; + = positive.
February 1979 The American Journal of Medicine Volume 99 267
CYTOMEGALOVIRUS GRANULOMATOUS HEPATITIS-CLARKE ET AL.
nonucleosis due to CMV had anti-I, IO (34.5 per cent] had unclassified cold agglutinins and none had anti-i. In marked contrast, of 150 patients with heterophil- positive mononucleosis due to EBV, 30 (20 per cent) had anti-i, 62 (41.3 per cent) had unclassified cold agglutin- ins, 33 (22 per cent) had anti-1 and 25 (16.7 per cent] had no cold agglutinins. Anti-i antibodies have previously been documented in CMV infections [7] and in EBV infections associated with hemolytic anemia [5]. Finally, one of our patients had ANA and two had a high rheu- matoid factor. Bonkowsky’s first patient had rheumatoid factor activity at a I:20 dilution. His second patient and one of our patients (Case 1) had antibodies to typhoid 0 at I:80 and 1:40 dilutions, respectively. No positive se- rologic test for syphilis, antimitochondrial antibody or smooth muscle antibody was noted.
illness clinically indistinguishable from classic infec- tious mononucleosis caused by EBV [13,14]. CMV has also been well documented as a cause of the postper- fusion syndrome [15,16], post-transfusion mononucle- osis [17] and hepatitis [18]. Recent reports have de- scribed serious infections in the compromised host [19,20].
As suggested, illnesses caused by CMV and EBV have many clinical similarities. Prolonged shedding of these agents occurs in asymptomatic subjects, each virus may be transmitted by transfusion, neurologic manifestations have been well described with both infectious agents and, finally, a characteristic rash typically follows am- picillin administration to patients with the mononu- cleosis syndrome.
The significance of these nonspecific antibodies is not known, but the diverse antibody response parallels that seen in EBV mononucleosis. It has been postulated that under normal conditions some T cells may have a role in suppressing B cell-mediated antibody synthesis [8]. Failure in this function, as may occur in CMV or EBV infection, could lead to the abnormal circulating anti- bodies observed.
Another immunologic abnormality, transient anergy, was noted in Reller’s patient [I] and in one of ours. This phenomenon has been well described in EBV mono- nucleosis by Haider et al. [9]. Howard and Najarian [lo] have demonstrated marked depression of cell-mediated immunity in a murine model of CMV infection and hypothesized that synthesis of viral particles may compete with normal immune function. Mangi et al. [Ill have proposed that depression of cell-mediated im- munity in EBV mononucleosis may be due to antigenic competition.
It is clear that a granulomatous response in general, and granulomatous hepatitis in particular, represent host responses to a broad spectrum of infectious and toxic agents. The pathophysiology of the granulomatous re- sponse has recently been reviewed [21], but the role of viral agents remains to be well defined. Several reviews have emphasized that sarcoidosis, tuberculosis and histoplasmosis are major etiologies of granulomatous hepatitis [22,23]. However, granulomas have not been mentioned in numerous series of EBV hepatitis, indi- cating that granulomatous hepatitis due to EBV is probably rare.
From the clinical standpoint, CMV is associated with several distinct syndromes in man [12]. In the neonatal period, it may cause a devastating illness: in childhood, CMV infection may be clinically unrecognized. The incidence of antibody positivity increases into adult life, indicating that exposure throughout life continues. The patient with CMV infection may also present with an
REFERENCES
Our patients had well documented CMV infection. Each had prolonged fever and two (Cases 1 and 3) ful- filled all of Jordan’s 1141 criteria for CMV mononucle- osis. Further, CMV was cultured from urine in each case, and the serologic titers were consistent with CMV infection. Of interest was the age of two of our patients, above the usual age reported for this infection. CMV should, therefore, be considered in the differential di- agnosis of granulomatous hepatitis, even in older pa- tients.
ACKNOWLEDGMENT
We are grateful for the encouragement and editorial criticism provided by Dr. John Phair.
3. Schuster F,lOgnibene AS: Dissociation of serum bilirubin and alkaline phosphatase in infectious mononucleosis. JAMA 209: 267,1969.
4. Horwitz CA, et al.: Heterophil-negative infectious mono- nucleosis and mononucleosis-like illnesses. Laboratorv confirmation of 43 cases. Am J Med 63: 947,1977. ’
5. Jenkins WJ, Koster HG. Marsh WL, et al.: Infectious mono- nucleosis. An unsuspected source of anti-i. Br J Hematol 2: 480. 1965.
6. Horwitz CA, et al.: Cold agglutinins in infectious mononu-
cleosis and heterophil-antibody-negative mononucleo- sis-like syndromes. Blood 66 195.1977.
7. Berlin BS, Chandler R, Green D: Anti “i” antibody and he- molytic anemia associated with spontaneous cytomegalo- virus mononucleosis. Am J Clin Path01 67: 459.1977.
8. Denman AM, Allison AC, Barnes RD: Cooperating and controlling functions of thymus-derived lymphocytes in relation to autoimmunity. Lancet 2: 1351971.
9. Haider S, Coutinho M de L, Emond RTD: Tuberculin anergy and infectious mononucleosis. Lancet 2: 74.1973.