42
Type 1 DM, 2015- No Longer a Disease of Youth Dace Trence, MD April, 2015 Type I Diabetes (Trence), NWGEC Spring 2015 1
Type 1 DM, 2015-
No Longer a Disease of Youth
Dace Trence, MD
April, 2015
Type I Diabetes (Trence), NWGEC Spring 2015 1
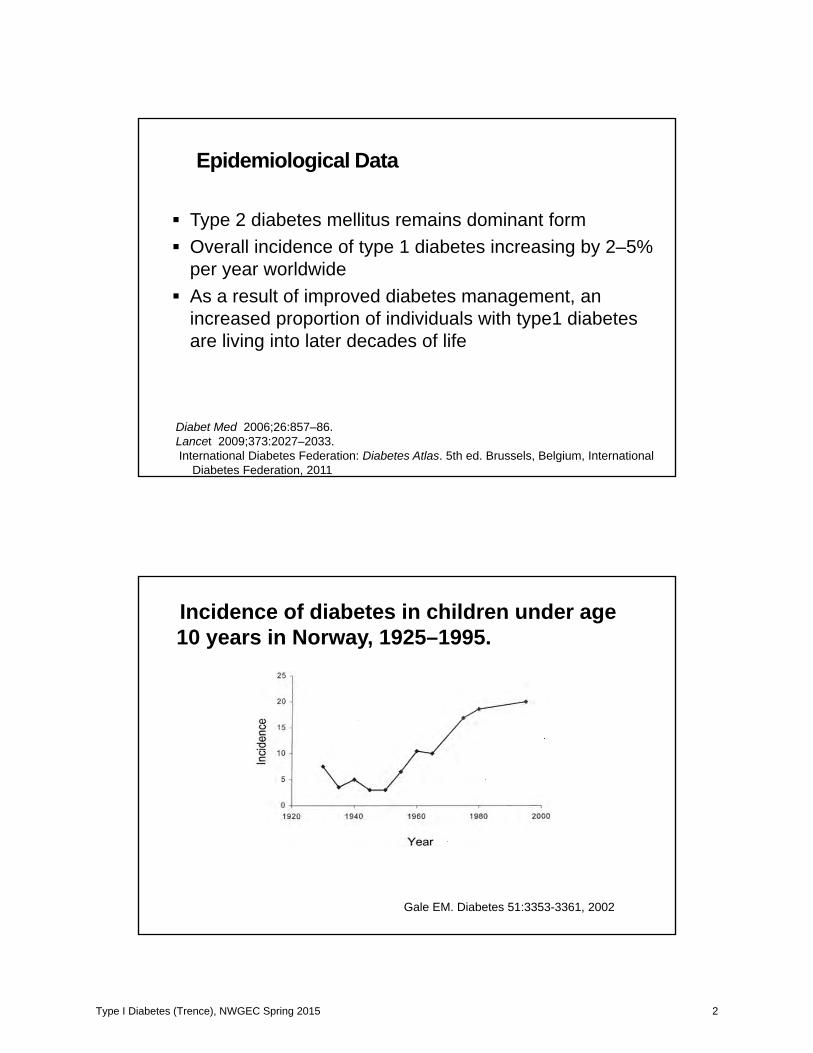
Epidemiological Data
Type 2 diabetes mellitus remains dominant formOverall incidence of type 1 diabetes increasing by 2–5% per year worldwide As a result of improved diabetes management, an increased proportion of individuals with type1 diabetes are living into later decades of life
Diabet Med 2006;26:857–86.Lancet 2009;373:2027–2033.International Diabetes Federation: Diabetes Atlas. 5th ed. Brussels, Belgium, International
Diabetes Federation, 2011
Incidence of diabetes in children under age 10 years in Norway, 1925–1995.
Gale EM. Diabetes 51:3353-3361, 2002
Type I Diabetes (Trence), NWGEC Spring 2015 2
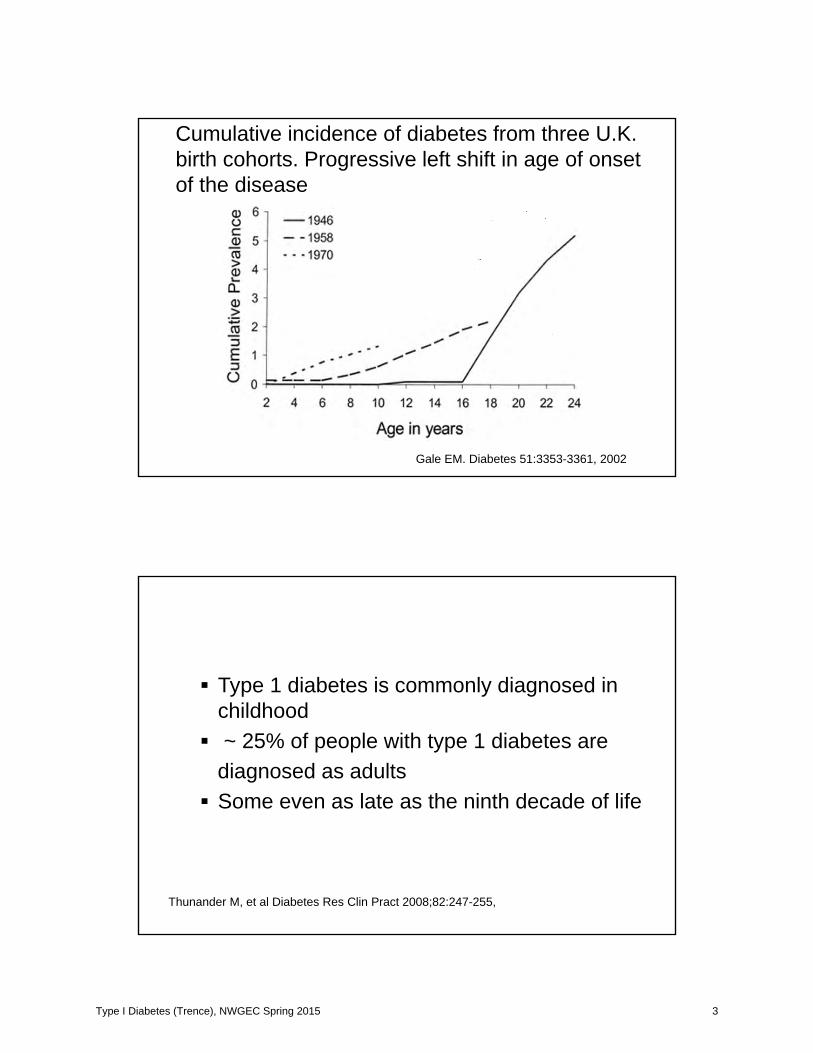
Cumulative incidence of diabetes from three U.K. birth cohorts. Progressive left shift in age of onset of the disease
Gale EM. Diabetes 51:3353-3361, 2002
Type 1 diabetes is commonly diagnosed in childhood~ 25% of people with type 1 diabetes are
diagnosed as adults Some even as late as the ninth decade of life
Thunander M, et al Diabetes Res Clin Pract 2008;82:247-255,
Type I Diabetes (Trence), NWGEC Spring 2015 3
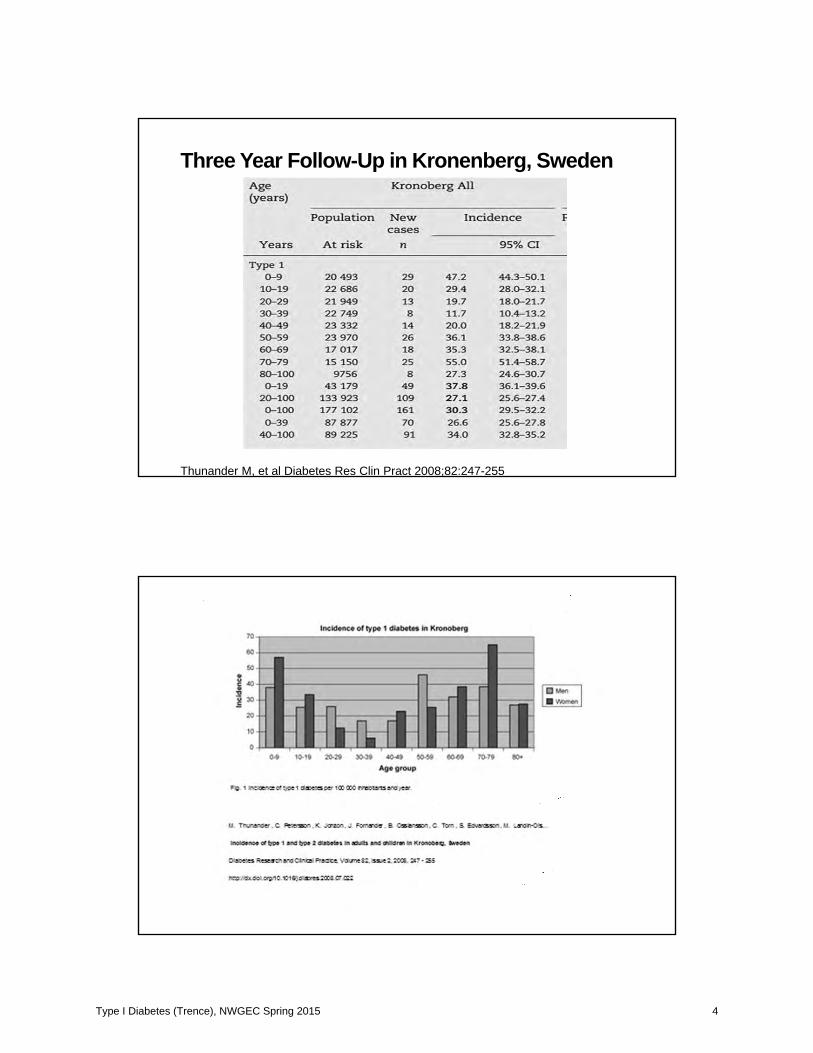
Three Year Follow-Up in Kronenberg, Sweden
Thunander M, et al Diabetes Res Clin Pract 2008;82:247-255
Type I Diabetes (Trence), NWGEC Spring 2015 4
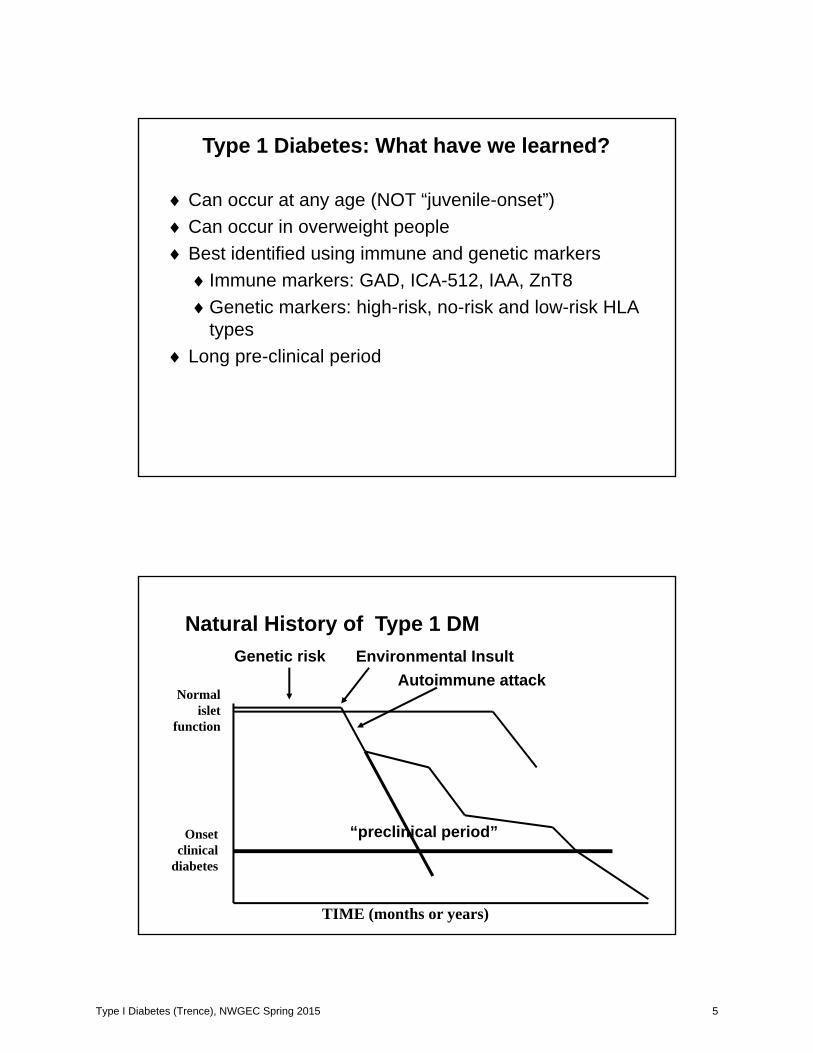
Type 1 Diabetes: What have we learned?
Can occur at any age (NOT “juvenile-onset”)Can occur in overweight peopleBest identified using immune and genetic markers
Immune markers: GAD, ICA-512, IAA, ZnT8Genetic markers: high-risk, no-risk and low-risk HLA types
Long pre-clinical period
Normalislet
function
Onsetclinical
diabetes
TIME (months or years)
Genetic risk Environmental Insult
“preclinical period”
Autoimmune attack
Natural History of Type 1 DM
Type I Diabetes (Trence), NWGEC Spring 2015 5
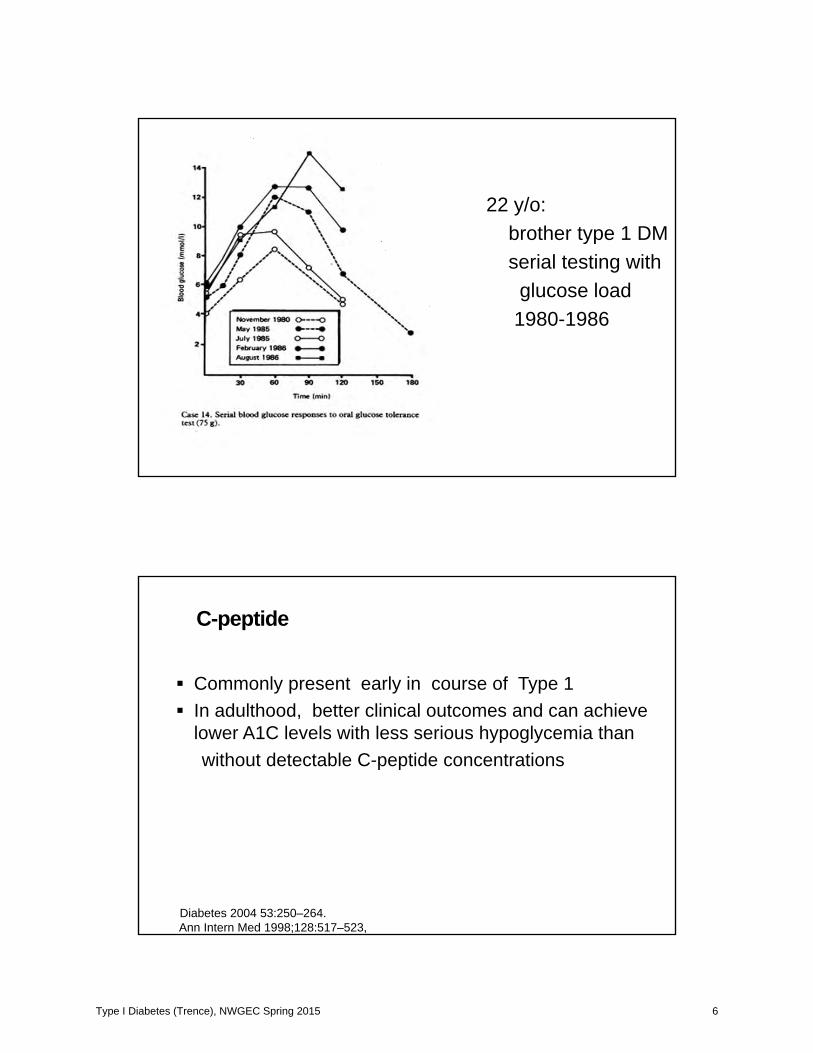
22 y/o: brother type 1 DMserial testing with
glucose load1980-1986
C-peptide
Commonly present early in course of Type 1 In adulthood, better clinical outcomes and can achieve lower A1C levels with less serious hypoglycemia thanwithout detectable C-peptide concentrations
Diabetes 2004 53:250–264.Ann Intern Med 1998;128:517–523,
Type I Diabetes (Trence), NWGEC Spring 2015 6
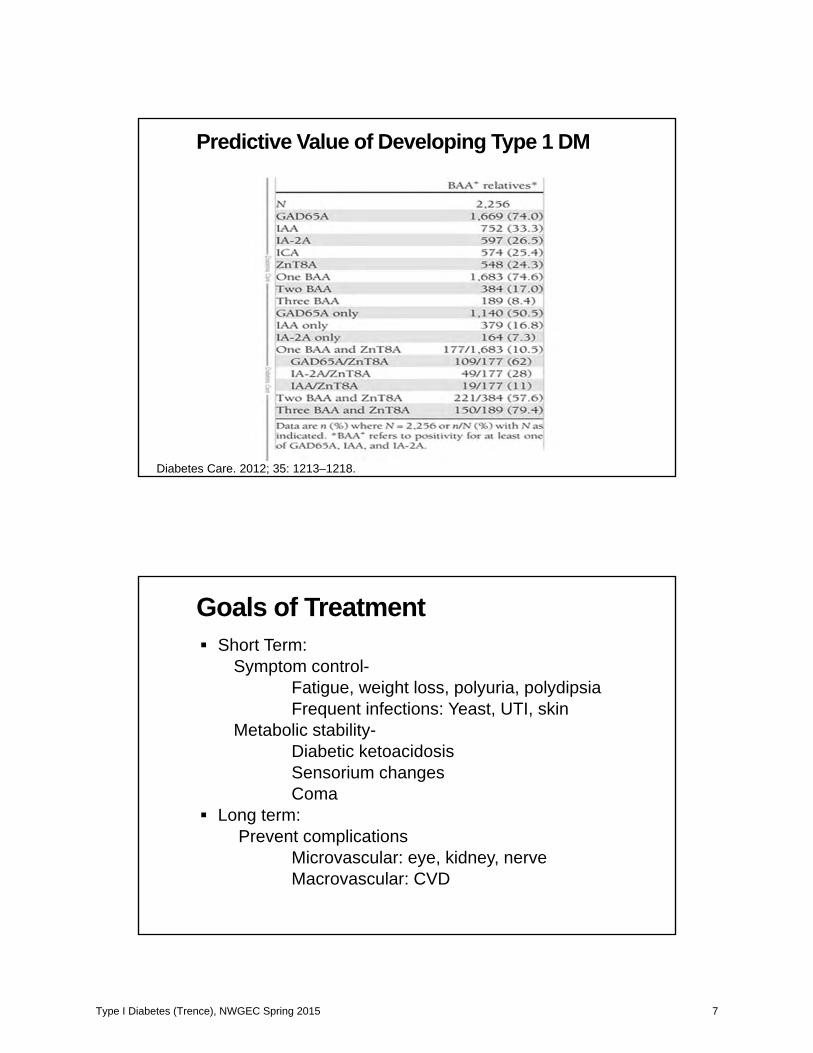
Predictive Value of Developing Type 1 DM
Diabetes Care. 2012; 35: 1213–1218.
Goals of TreatmentShort Term:
Symptom control-Fatigue, weight loss, polyuria, polydipsiaFrequent infections: Yeast, UTI, skin
Metabolic stability-Diabetic ketoacidosisSensorium changesComa
Long term: Prevent complications
Microvascular: eye, kidney, nerveMacrovascular: CVD
Type I Diabetes (Trence), NWGEC Spring 2015 7
A1C Targets Suggested by Different Organizations
AACE target: A1C <6.5%EASD target: A1C <6.5%ADA target: A1C <7% (general)
A1C <6%* (individual patient)
Optimal target: A1C <6% (normal range)
*As close to normal (<6%) without significant hypoglycemia.ADA = American Diabetes Association; EASD = European Association for the Study of Diabetes, AACE = American Association of Clinical Endccriologists.
Barrier: hypoglycemia!!!!!
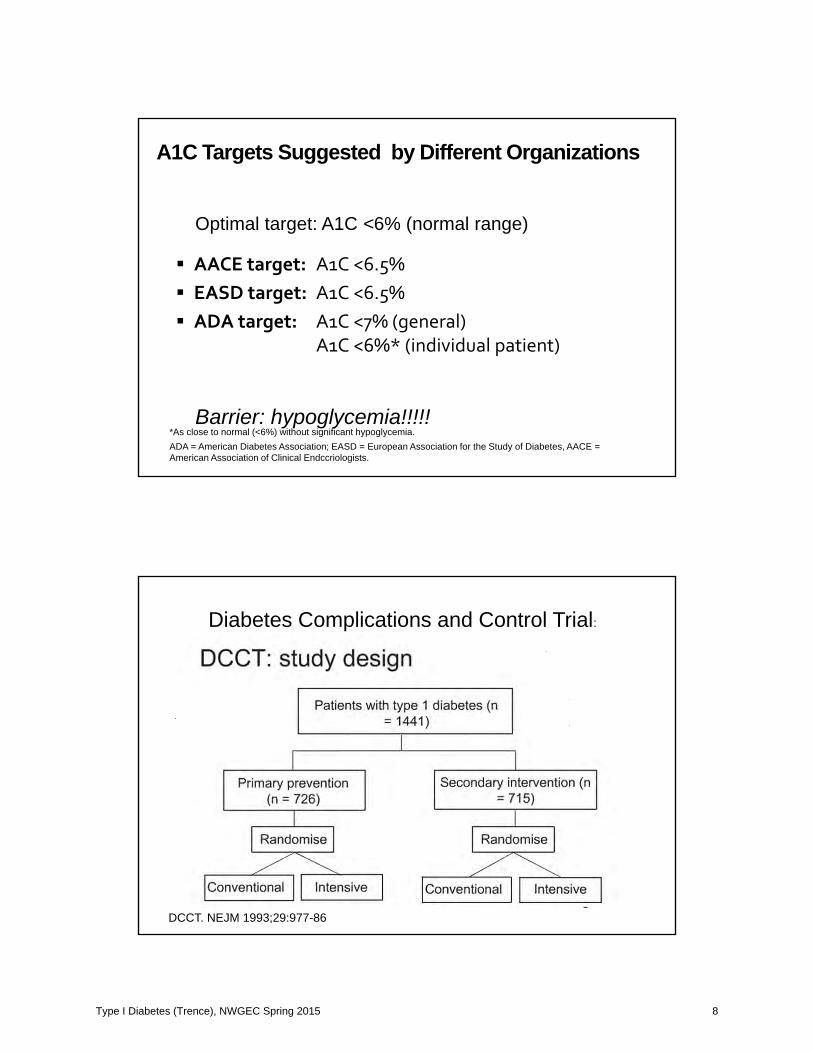
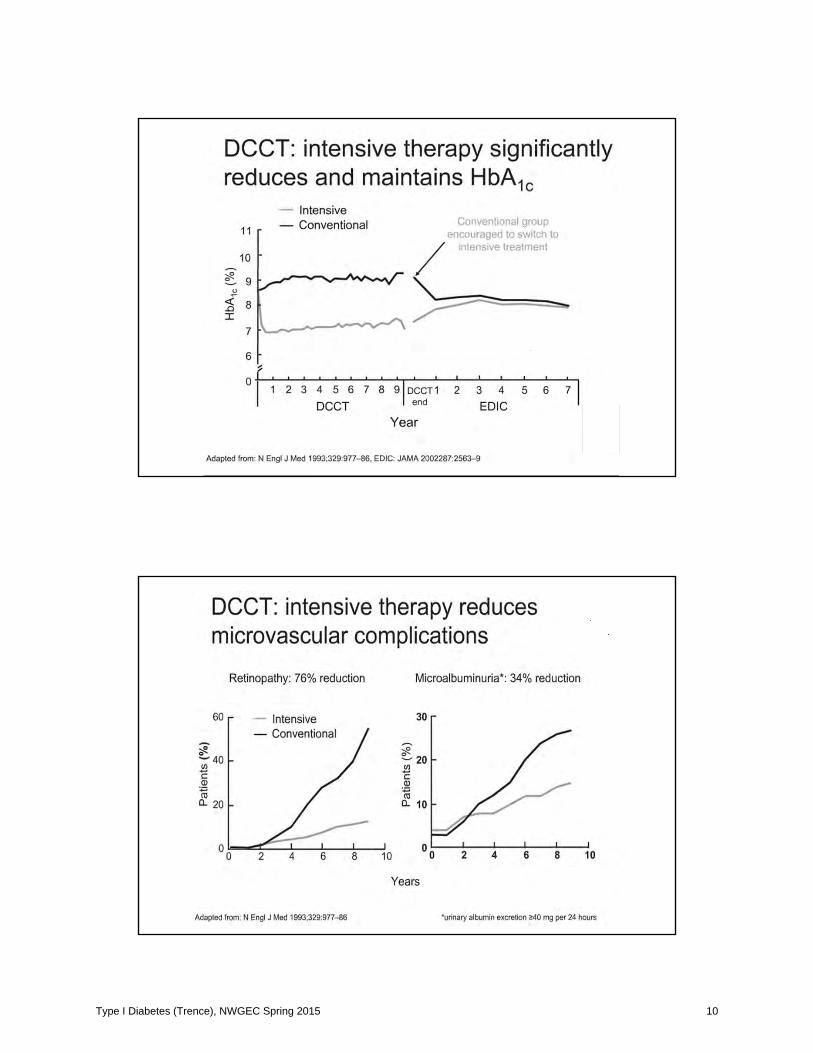
Diabetes Complications and Control Trial:
DCCT. NEJM 1993;29:977-86
Type I Diabetes (Trence), NWGEC Spring 2015 8
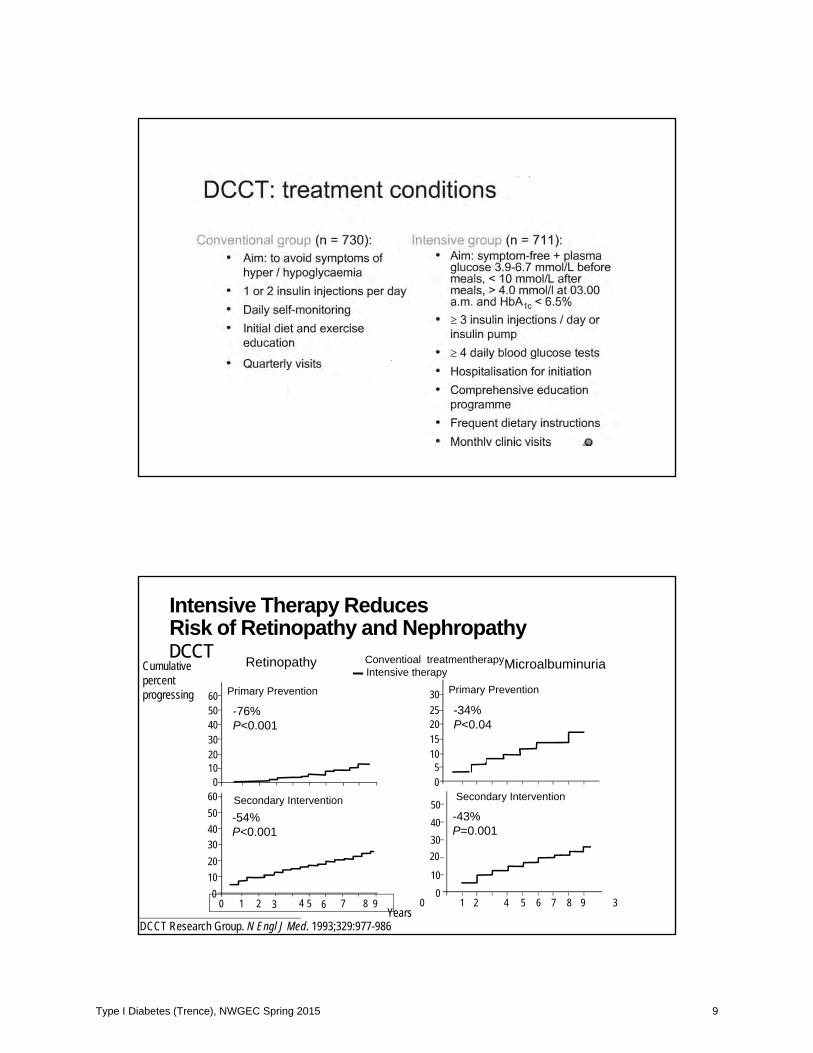
Intensive Therapy ReducesRisk of Retinopathy and NephropathyDCCT Retinopathy MicroalbuminuriaCumulative
percent progressing
DCCT Research Group. N Engl J Med. 1993;329:977-986
00
6050403020100
-76%P<0.001
605040302010
0 1 2 3 4 5 6 7 8 9
Secondary Intervention-54%P<0.001
302520151050
-34%P<0.04
50403020
100
1 2 34 5 6 7 8
Secondary Intervention
-43%P=0.001
Conventioal treatmentherapyIntensive therapy
Years9
Primary PreventionPrimary Prevention
Type I Diabetes (Trence), NWGEC Spring 2015 9
Type I Diabetes (Trence), NWGEC Spring 2015 10
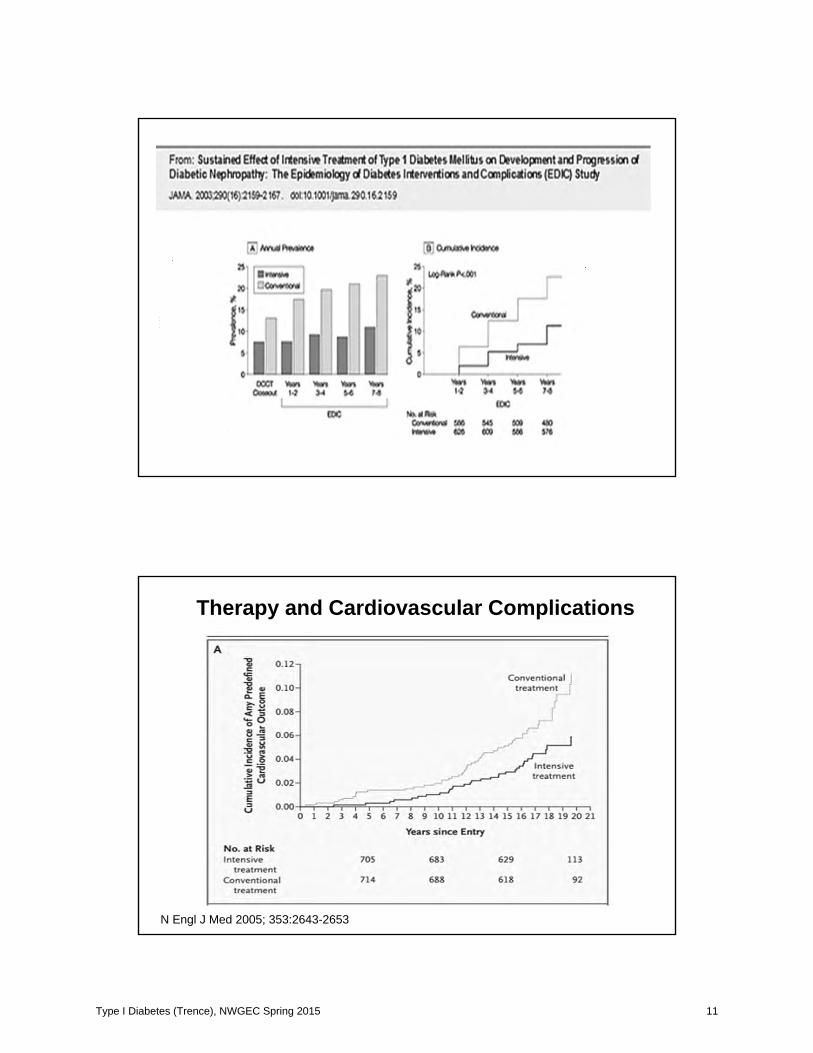
Therapy and Cardiovascular Complications
N Engl J Med 2005; 353:2643-2653
Type I Diabetes (Trence), NWGEC Spring 2015 11

Swedish Registry 1998-2011: Type 1 DM, mean age 36 at entry
N Engl J Med 2014;371:1972-8
Type I Diabetes (Trence), NWGEC Spring 2015 12
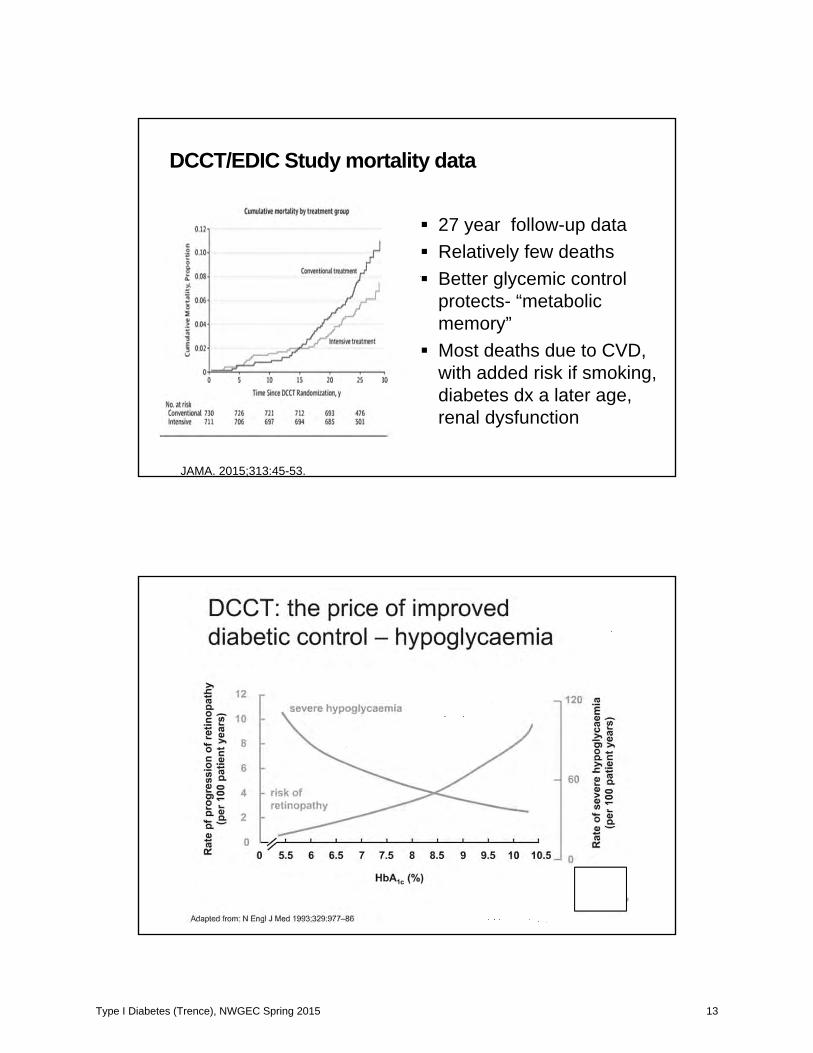
DCCT/EDIC Study mortality data
27 year follow-up dataRelatively few deathsBetter glycemic control protects- “metabolic memory”Most deaths due to CVD, with added risk if smoking, diabetes dx a later age, renal dysfunction
JAMA. 2015;313:45-53.
Type I Diabetes (Trence), NWGEC Spring 2015 13
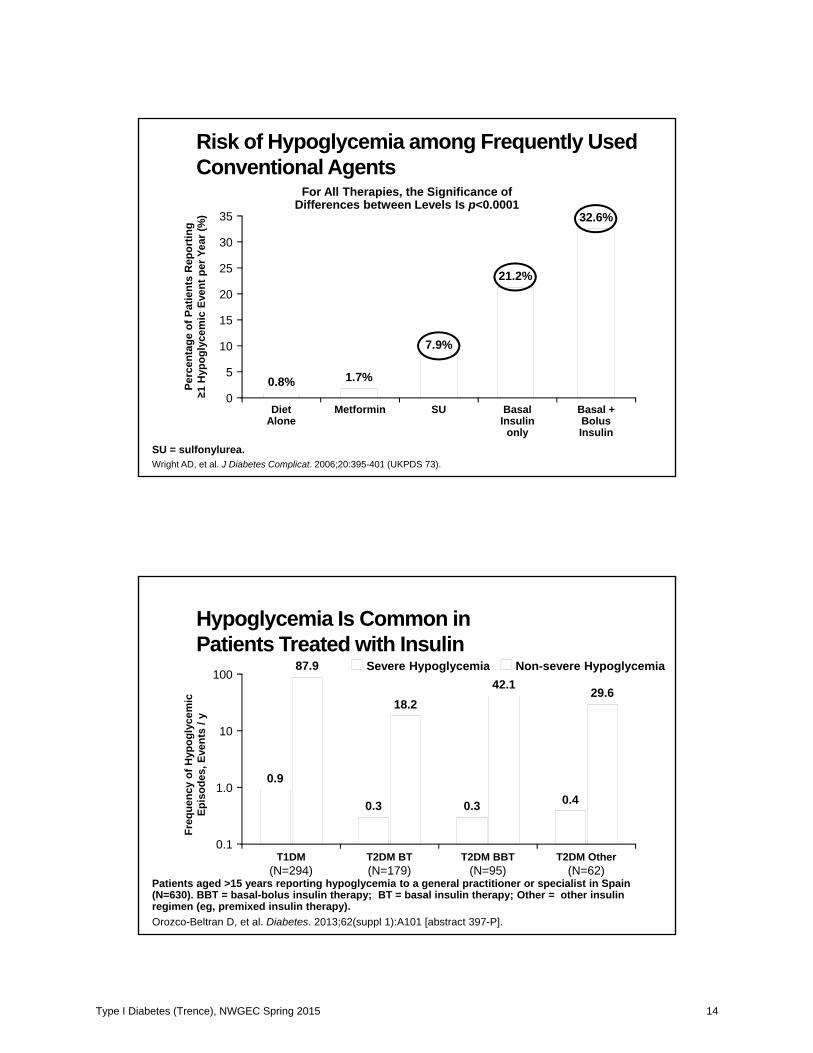
Risk of Hypoglycemia among Frequently Used Conventional Agents
SU = sulfonylurea.Wright AD, et al. J Diabetes Complicat. 2006;20:395-401 (UKPDS 73).
For All Therapies, the Significance of Differences between Levels Is p<0.0001
Perc
enta
ge o
f Pat
ient
s R
epor
ting
1 H
ypog
lyce
mic
Eve
nt p
er Y
ear (
%)
15
25
35
0
5
DietAlone
0.8% 1.7%
32.6%
10
20
30
7.9%
21.2%
Metformin SU BasalInsulin
only
Basal +BolusInsulin
Hypoglycemia Is Common inPatients Treated with Insulin
Patients aged >15 years reporting hypoglycemia to a general practitioner or specialist in Spain (N=630). BBT = basal-bolus insulin therapy; BT = basal insulin therapy; Other = other insulin regimen (eg, premixed insulin therapy).Orozco-Beltran D, et al. Diabetes. 2013;62(suppl 1):A101 [abstract 397-P].
Freq
uenc
y of
Hyp
ogly
cem
icEp
isod
es, E
vent
s / y
10
100
0.1T1DM
(N=294)
1.0
T2DM BT(N=179)
T2DM BBT(N=95)
T2DM Other(N=62)
0.9
87.9
0.3
18.2
0.3
42.1
0.4
29.6
Severe Hypoglycemia Non-severe Hypoglycemia
Type I Diabetes (Trence), NWGEC Spring 2015 14
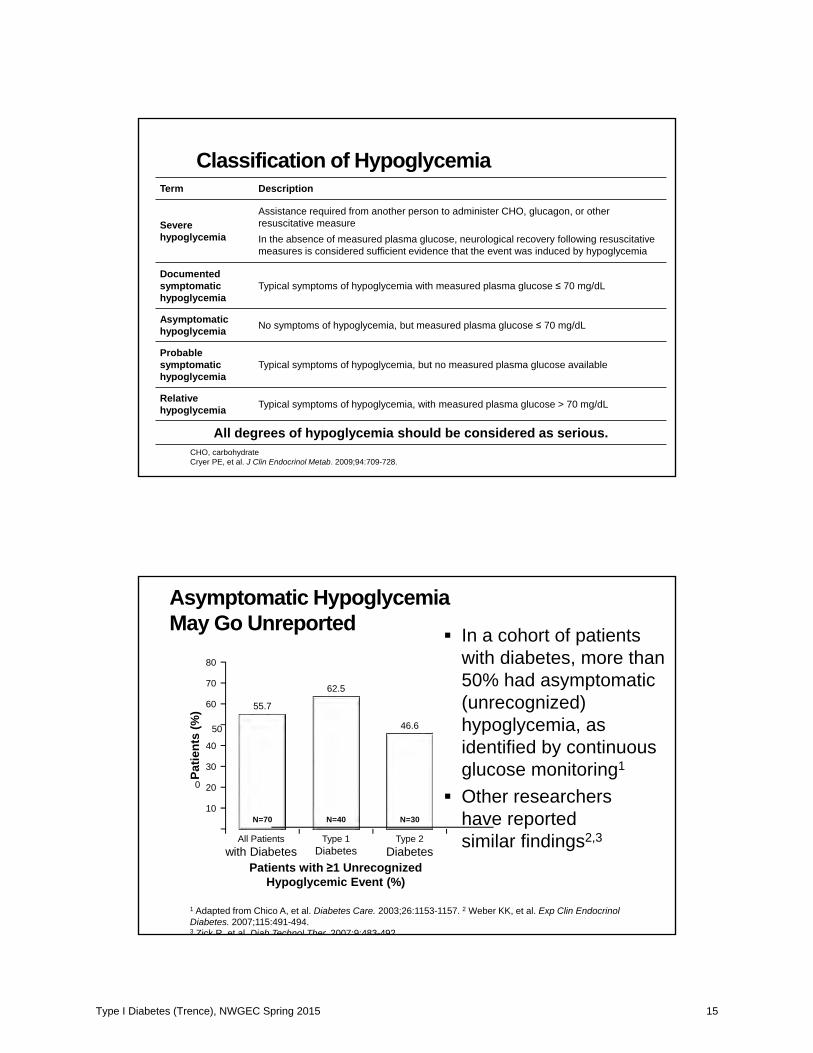
Classification of HypoglycemiaTerm Description
Severe hypoglycemia
Assistance required from another person to administer CHO, glucagon, or other resuscitative measureIn the absence of measured plasma glucose, neurological recovery following resuscitative measures is considered sufficient evidence that the event was induced by hypoglycemia
Documentedsymptomatic hypoglycemia
Typical symptoms of hypoglycemia with measured plasma glucose 70 mg/dL
Asymptomatic hypoglycemia No symptoms of hypoglycemia, but measured plasma glucose 70 mg/dL
Probable symptomatic hypoglycemia
Typical symptoms of hypoglycemia, but no measured plasma glucose available
Relative hypoglycemia Typical symptoms of hypoglycemia, with measured plasma glucose > 70 mg/dL
All degrees of hypoglycemia should be considered as serious.CHO, carbohydrateCryer PE, et al. J Clin Endocrinol Metab. 2009;94:709-728.
Asymptomatic HypoglycemiaMay Go Unreported In a cohort of patients
with diabetes, more than 50% had asymptomatic (unrecognized) hypoglycemia, as identified by continuous glucose monitoring1
Other researchers have reported similar findings2,3
Patie
nts
(%)
20
60
70
80
0
All Patientswith Diabetes
55.7
40
Patients with 1 Unrecognized Hypoglycemic Event (%)
Type 1Diabetes
62.5
Type 2Diabetes
46.6
10
50
30
N=70 N=40 N=30
1 Adapted from Chico A, et al. Diabetes Care. 2003;26:1153-1157. 2 Weber KK, et al. Exp Clin EndocrinolDiabetes. 2007;115:491-494. 3 Zick R et al Diab Technol Ther 2007;9:483-492
Type I Diabetes (Trence), NWGEC Spring 2015 15
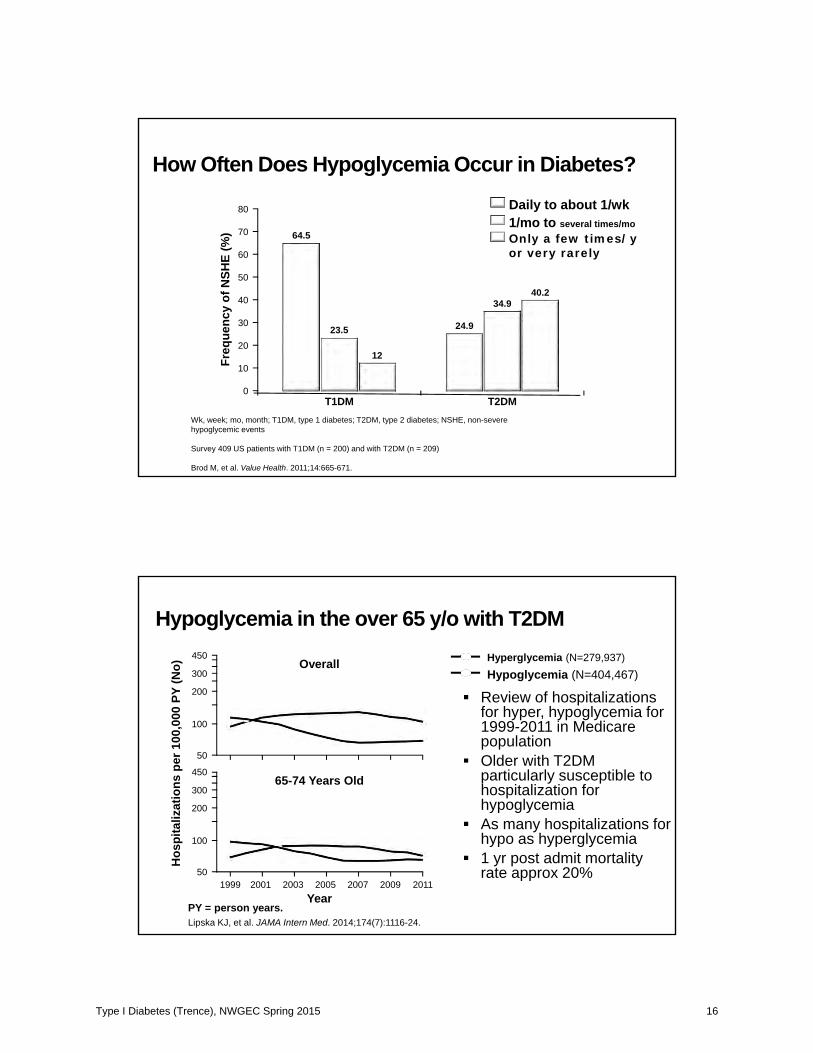
How Often Does Hypoglycemia Occur in Diabetes?
Daily to about 1/wkFr
eque
ncy
of N
SHE
(%)
20
60
80
0
40
64.5
T1DM
23.5
12
24.9
T2DM
34.940.2
10
50
70
30
1/mo to several times/moOnly a few times/y or very rarely
Wk, week; mo, month; T1DM, type 1 diabetes; T2DM, type 2 diabetes; NSHE, non-severe hypoglycemic events
Survey 409 US patients with T1DM (n = 200) and with T2DM (n = 209)
Brod M, et al. Value Health. 2011;14:665-671.
Hos
pita
lizat
ions
per
100
,000
PY
(No)
1999Year
2009200720052001 2003
100
450
50
300
200
65-74 Years Old
Hyperglycemia (N=279,937)Hypoglycemia (N=404,467)
Review of hospitalizations for hyper, hypoglycemia for 1999-2011 in Medicare populationOlder with T2DM particularly susceptible to hospitalization for hypoglycemiaAs many hospitalizations for hypo as hyperglycemia1 yr post admit mortality rate approx 20%
Hypoglycemia in the over 65 y/o with T2DM
PY = person years.Lipska KJ, et al. JAMA Intern Med. 2014;174(7):1116-24.
2011
100
450
50
300
200
Overall
Type I Diabetes (Trence), NWGEC Spring 2015 16
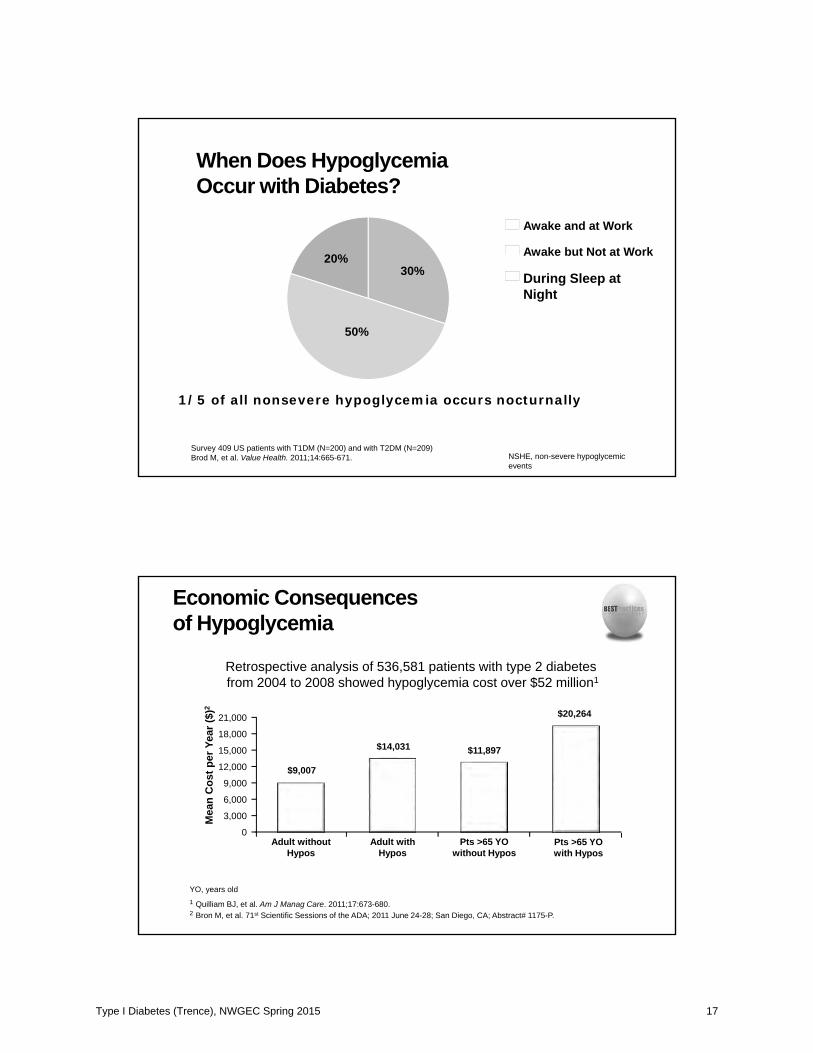
When Does Hypoglycemia Occur with Diabetes?
1/5 of all nonsevere hypoglycemia occurs nocturnally
30%
50%
20%
Awake and at Work
Awake but Not at Work
During Sleep at Night
Survey 409 US patients with T1DM (N=200) and with T2DM (N=209)Brod M, et al. Value Health. 2011;14:665-671. NSHE, non-severe hypoglycemic
events
Economic Consequences of Hypoglycemia
Retrospective analysis of 536,581 patients with type 2 diabetes from 2004 to 2008 showed hypoglycemia cost over $52 million1
Mea
n C
ost p
er Y
ear (
$)2
6,000
18,000
0Adult without
Hypos
$9,00712,000
Adult withHypos
$14,031
Pts >65 YOwithout Hypos
$11,897
3,000
15,000
9,000
21,000 $20,264
Pts >65 YOwith Hypos
YO, years old1 Quilliam BJ, et al. Am J Manag Care. 2011;17:673-680. 2 Bron M, et al. 71st Scientific Sessions of the ADA; 2011 June 24-28; San Diego, CA; Abstract# 1175-P.
Type I Diabetes (Trence), NWGEC Spring 2015 17
Clinical Consequences of Hypoglycemia
Hospital admissions1
In a prospective study of well-controlled elderly T2DM patients, 25% of hospital admissions for diabetes were for severe hypoglycemia
Increased mortality2
9% in a study of severe sulfonylurea-associated hypoglycemia
Road accidents caused by hypoglycemia3
45 serious events per month1 Greco D, et al. Diab Nutr Metab 2004;17:23-26. 2 Campbell IW. Horm Metab Res Suppl. 1985;15:105-111. 3 Hitchen L. BMJ. 2006;332(7545):812.
COSTHASSLE
Type I Diabetes (Trence), NWGEC Spring 2015 18
Type I Diabetes (Trence), NWGEC Spring 2015 19
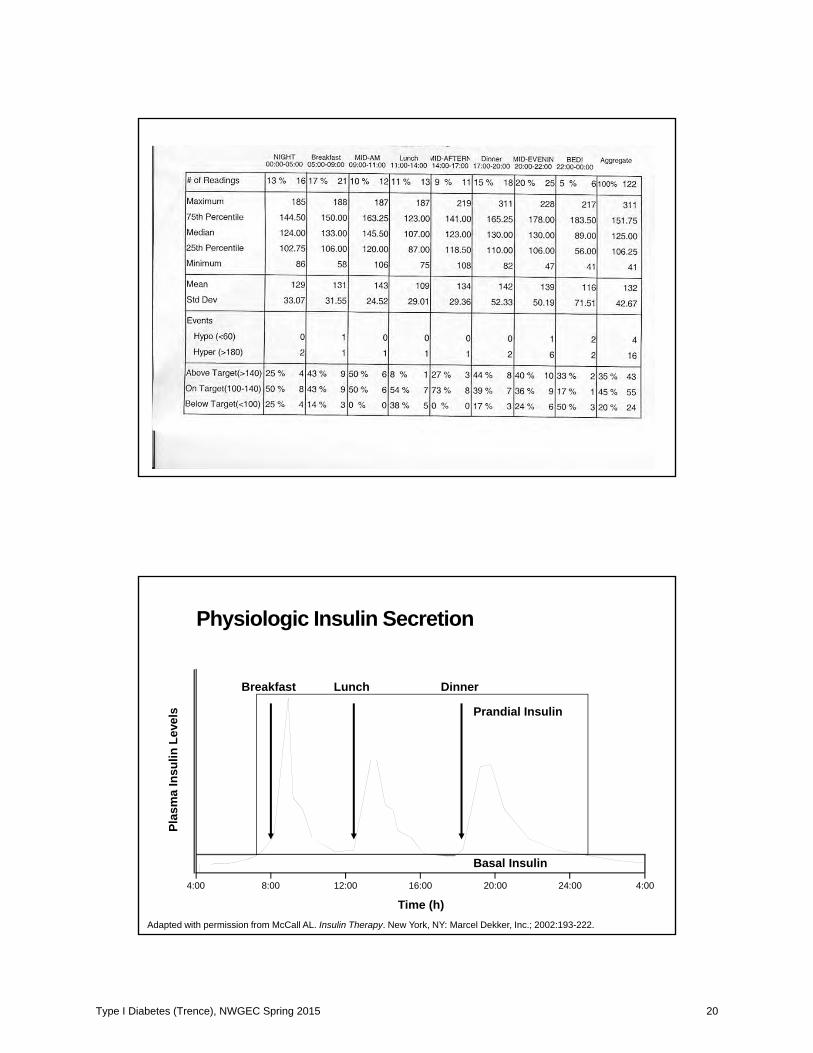
Physiologic Insulin Secretion
Breakfast Lunch Dinner
Basal Insulin
Prandial Insulin
Adapted with permission from McCall AL. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002:193-222.
Time (h)
Plas
ma
Insu
lin L
evel
s
24:00 4:0012:00 20:0016:008:004:00
Type I Diabetes (Trence), NWGEC Spring 2015 20
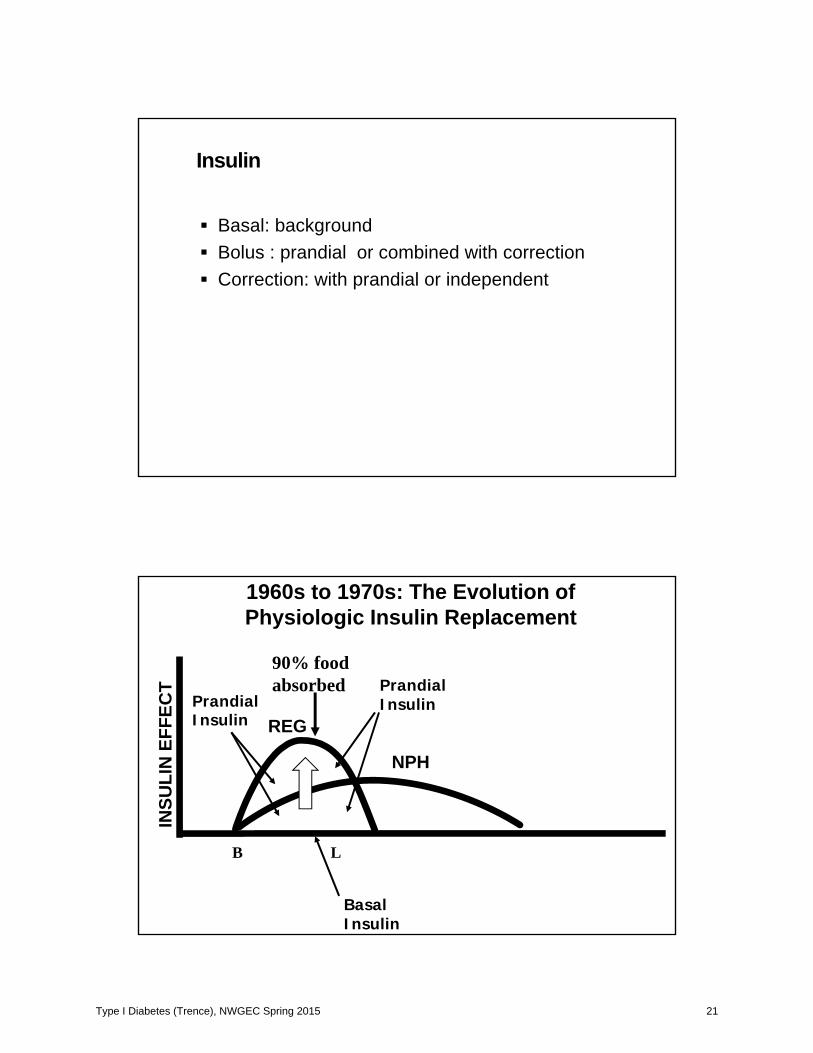
Insulin
Basal: backgroundBolus : prandial or combined with correctionCorrection: with prandial or independent
90% food absorbed
INSU
LIN
EFF
ECT
PrandialInsulin
BasalInsulin
NPH
B L
PrandialInsulin
REG
1960s to 1970s: The Evolution of Physiologic Insulin Replacement
Type I Diabetes (Trence), NWGEC Spring 2015 21
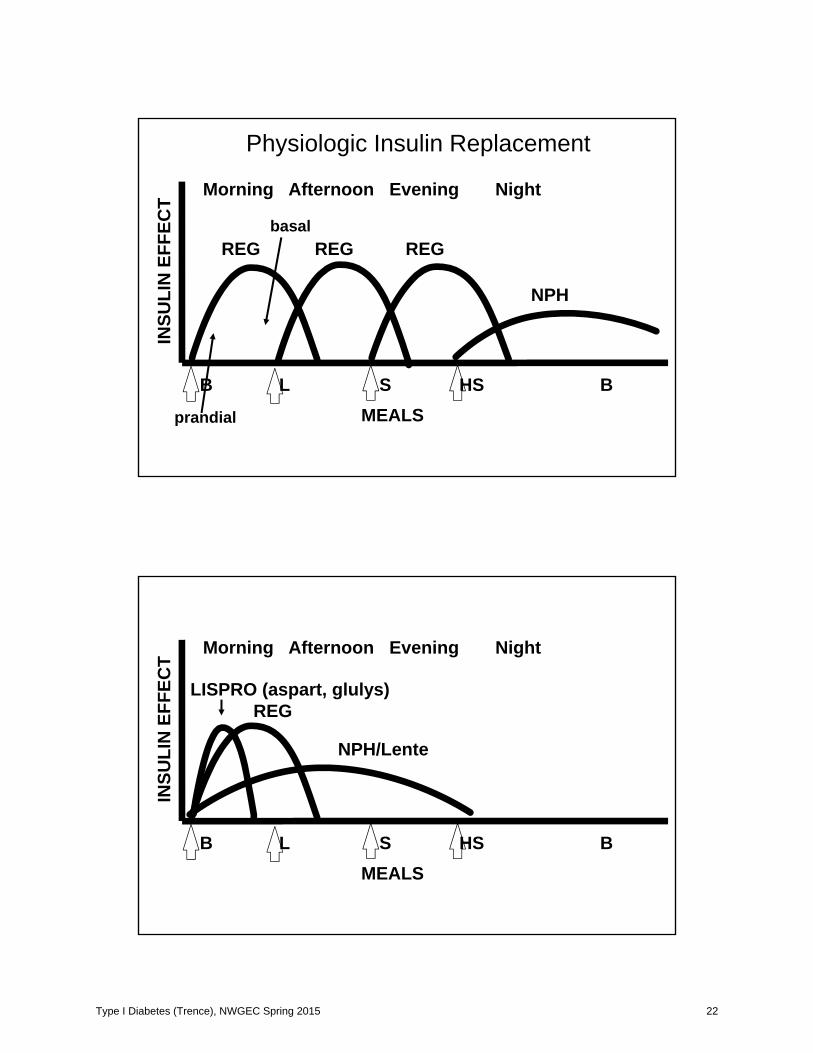
INSU
LIN
EFF
ECT
B L S HS BMEALS
Morning Afternoon Evening Night
REG REG REG
NPH
Physiologic Insulin Replacement
prandial
basal
INSU
LIN
EFF
ECT
B L S HS BMEALS
Morning Afternoon Evening Night
REGLISPRO (aspart, glulys)
NPH/Lente
Type I Diabetes (Trence), NWGEC Spring 2015 22
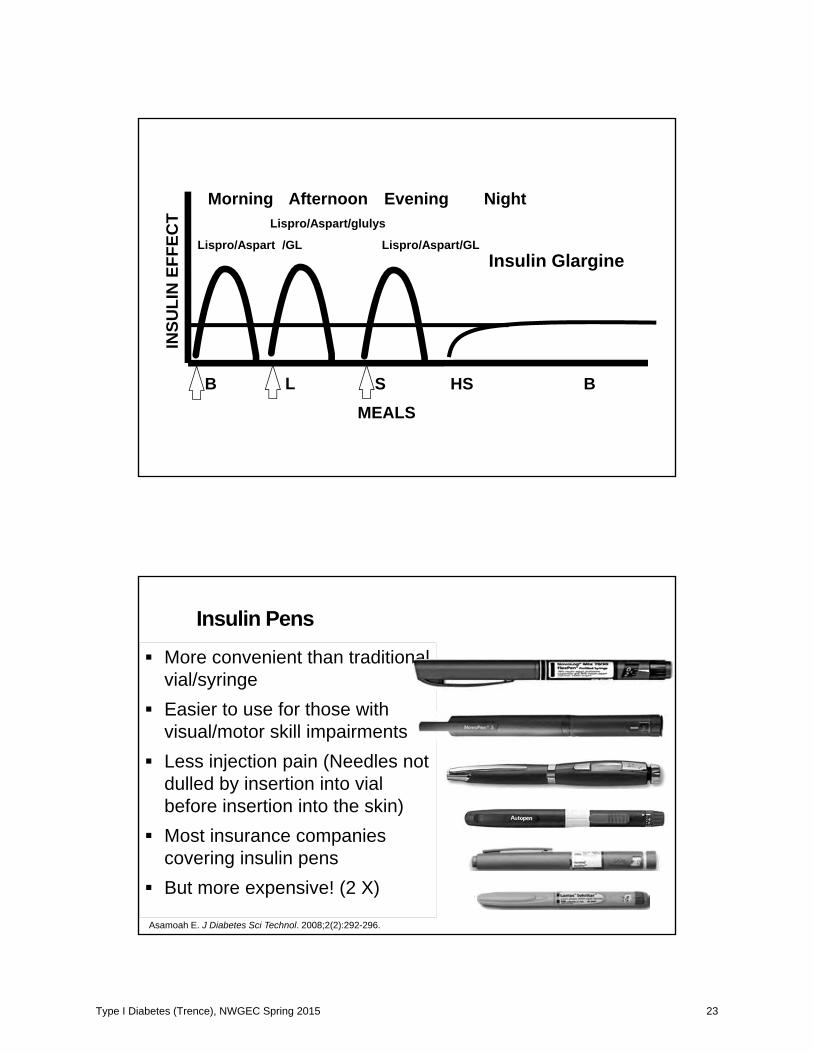
INSU
LIN
EFF
ECT
B L S HS BMEALS
Morning Afternoon Evening Night
Lispro/Aspart /GL Lispro/Aspart/GLInsulin Glargine
Lispro/Aspart/glulys
Insulin Pens
More convenient than traditional vial/syringe Easier to use for those with visual/motor skill impairments Less injection pain (Needles not dulled by insertion into vial before insertion into the skin)Most insurance companies covering insulin pensBut more expensive! (2 X)
Asamoah E. J Diabetes Sci Technol. 2008;2(2):292-296.
Type I Diabetes (Trence), NWGEC Spring 2015 23

INSU
LIN
EFF
ECT
B L S HS BMEALS
Morning Afternoon Evening Night
Basal Infusion
Bolus Bolus Bolus
CSII with LISPRO/ASPART
Type I Diabetes (Trence), NWGEC Spring 2015 24
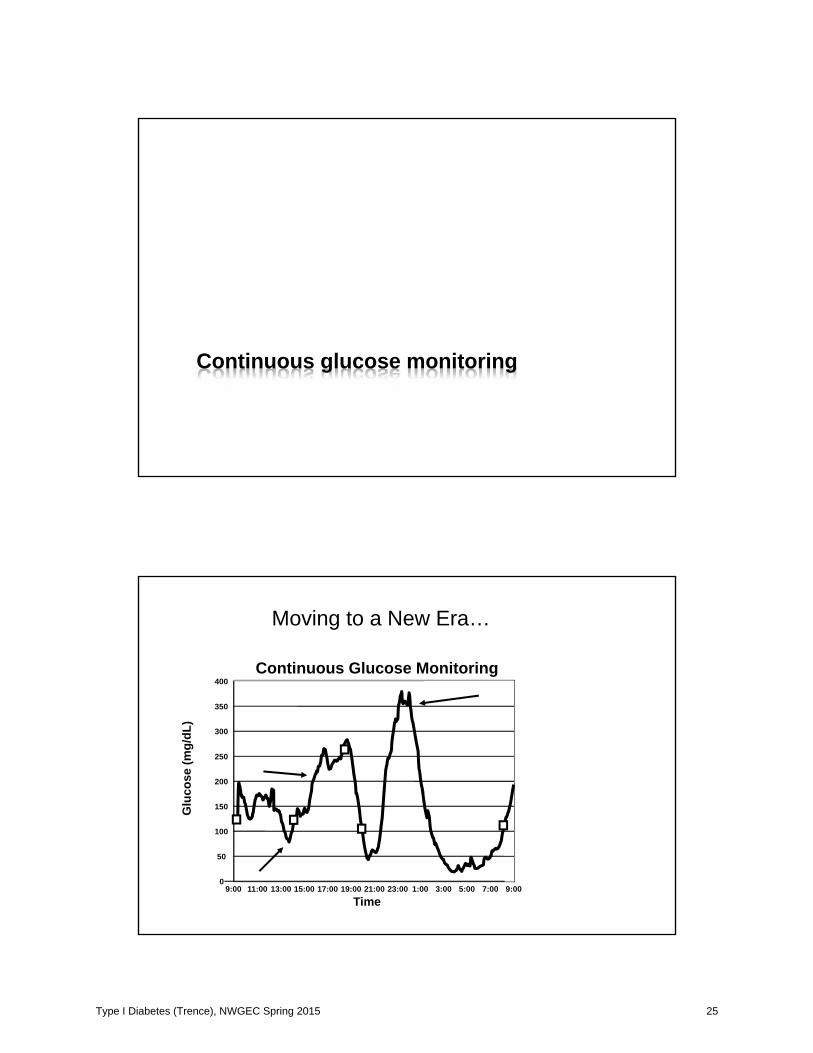
Continuous glucose monitoring
Moving to a New Era…
0
50
100
150
200
250
300
350
400
9:00 11:00 13:00 15:00 17:00 19:00 21:00 23:00 1:00 3:00 5:00 7:00 9:00
Time
Glu
cose
(mg/
dL)
Continuous Glucose Monitoring
Type I Diabetes (Trence), NWGEC Spring 2015 25
DexCom SC Glucose Sensor
Slowly Closing the Loop…
Type I Diabetes (Trence), NWGEC Spring 2015 26
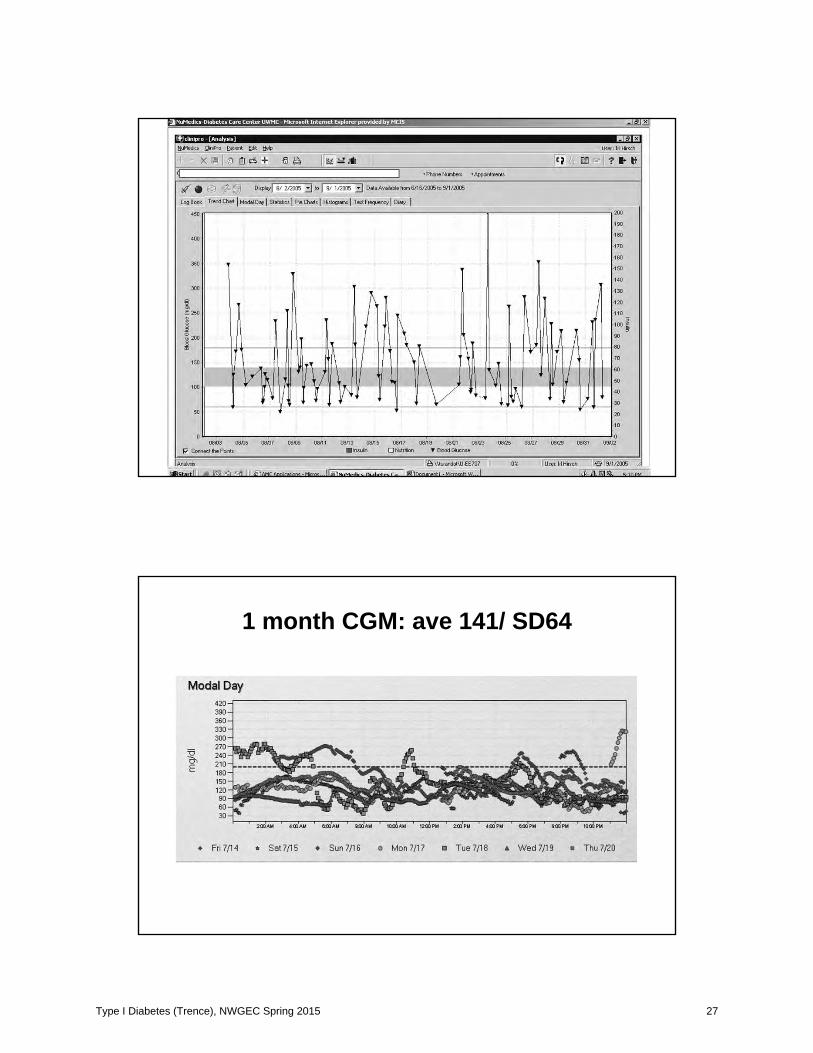
1 month CGM: ave 141/ SD64
Type I Diabetes (Trence), NWGEC Spring 2015 27
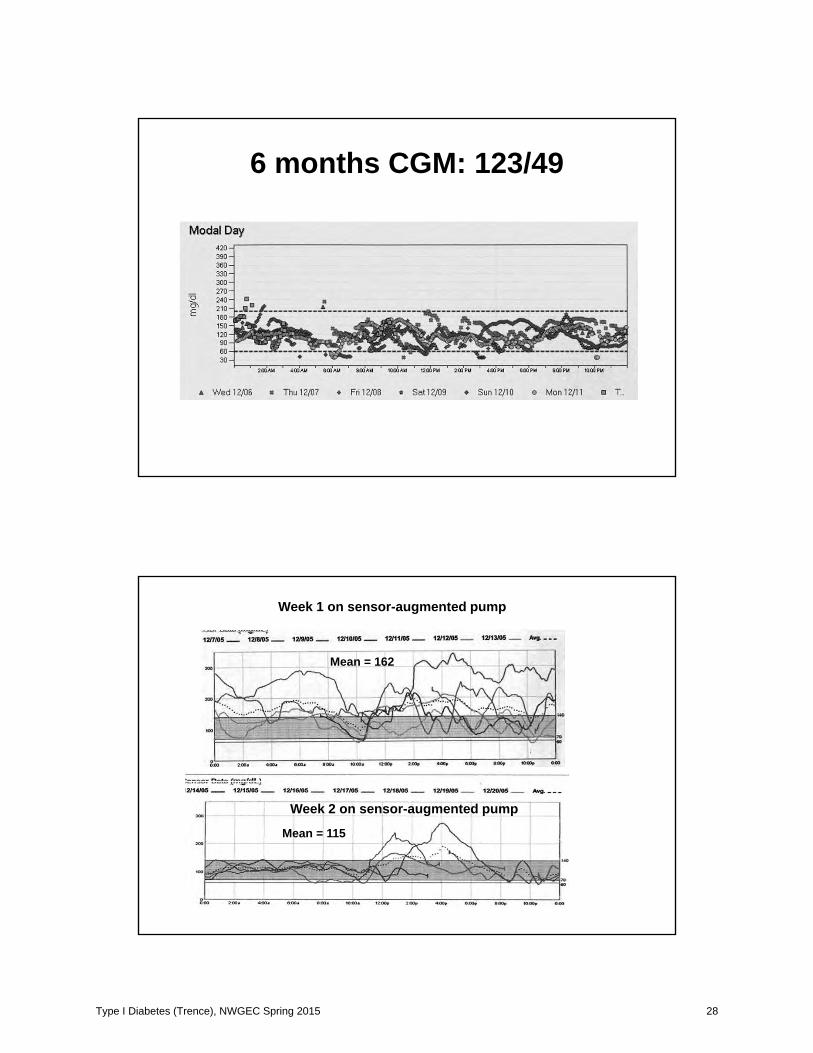
6 months CGM: 123/49
Week 1 on sensor-augmented pump
Week 2 on sensor-augmented pump
Mean = 162
Mean = 115
Type I Diabetes (Trence), NWGEC Spring 2015 28
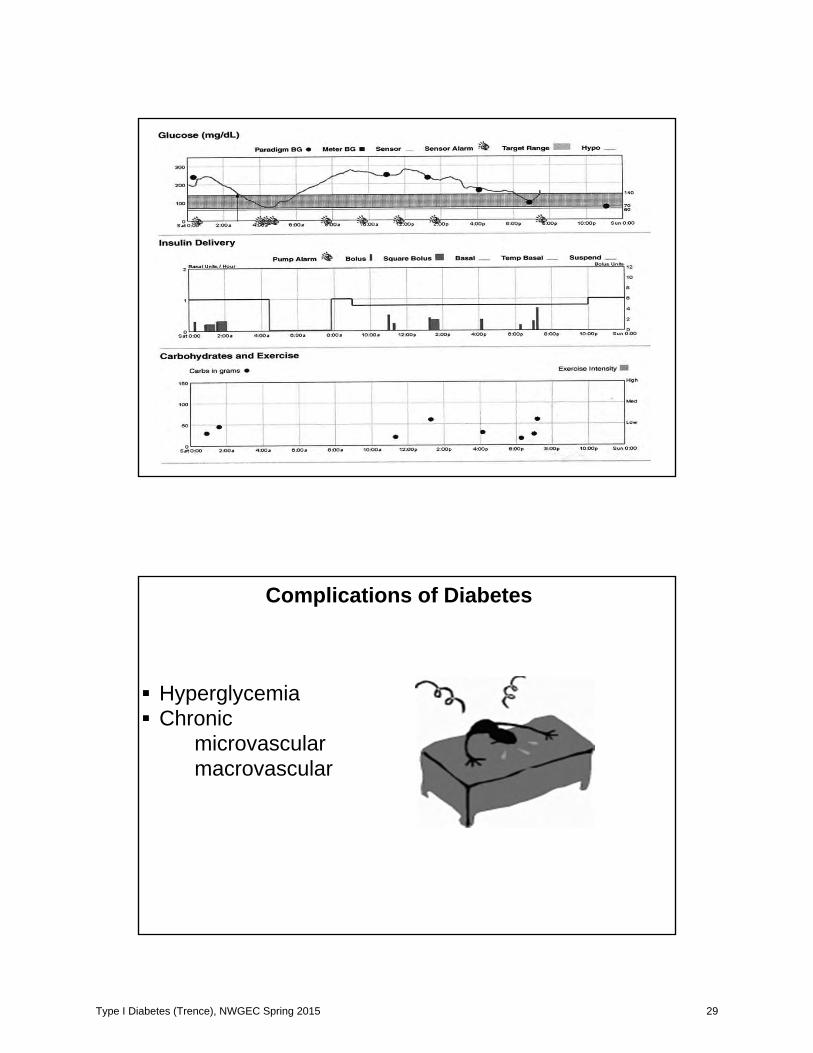
HyperglycemiaChronic
microvascular macrovascular
Complications of Diabetes
Type I Diabetes (Trence), NWGEC Spring 2015 29
Diabetic ketoacidosisInfections: urinary, vaginal, skin
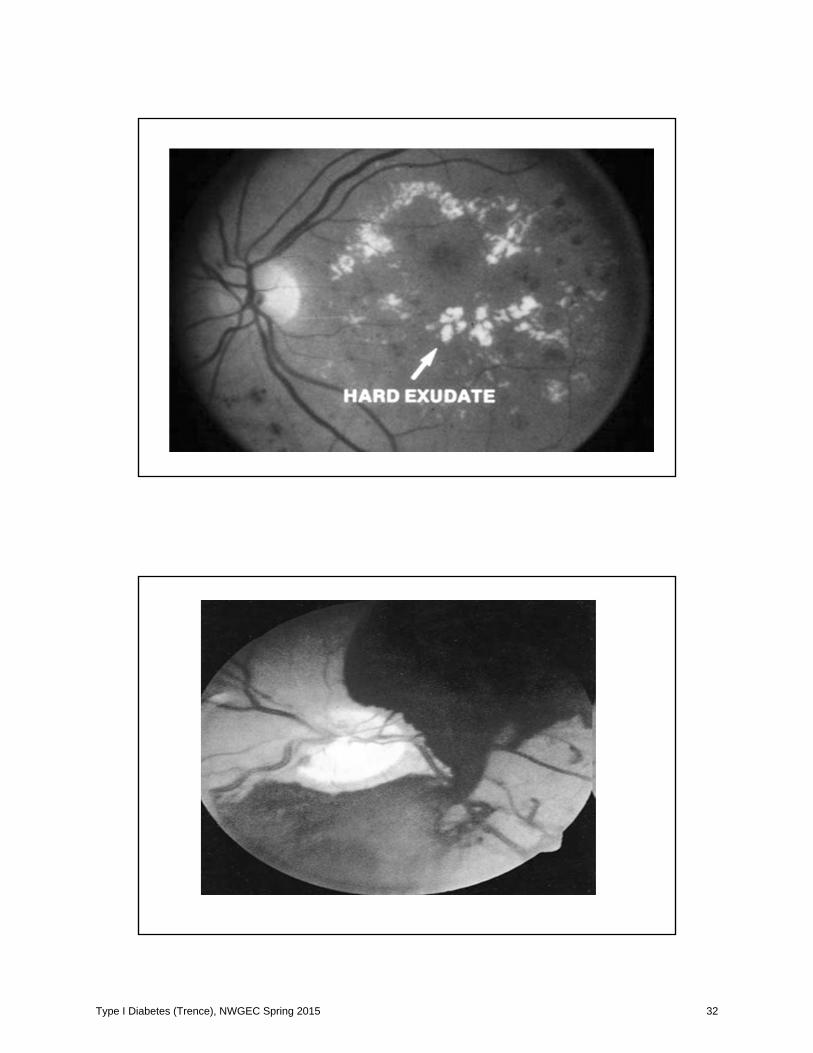
Retinopathy:Most common cause blindness in US
15 yrs DM 1, 50% have more severe form DR20 yrs DM 2, on insulin, 20% have PDR
Screening:DM 1, 5 yrs post diagnosis but after pubertyDM 2, yrly, if photos normal, then q 4yrs
unless proteinuria, severe hyperglycemia
Type I Diabetes (Trence), NWGEC Spring 2015 30
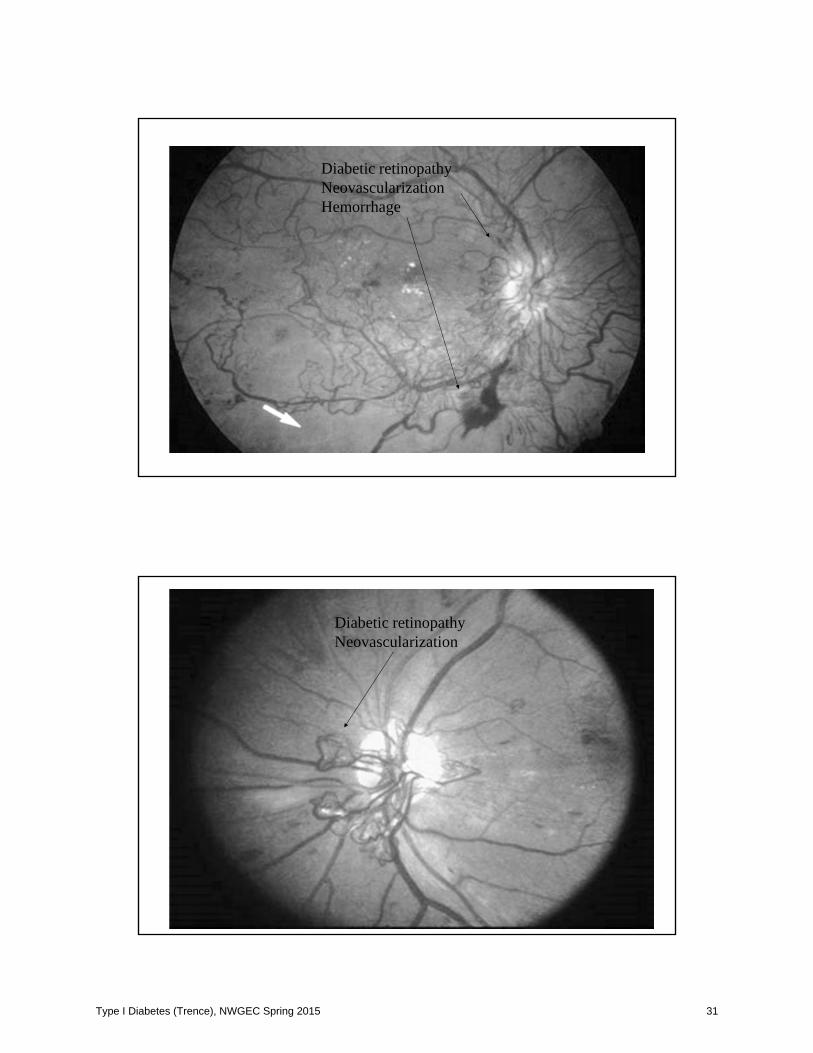
Diabetic retinopathyNeovascularizationHemorrhage
Diabetic retinopathyNeovascularization
Type I Diabetes (Trence), NWGEC Spring 2015 31
Type I Diabetes (Trence), NWGEC Spring 2015 32
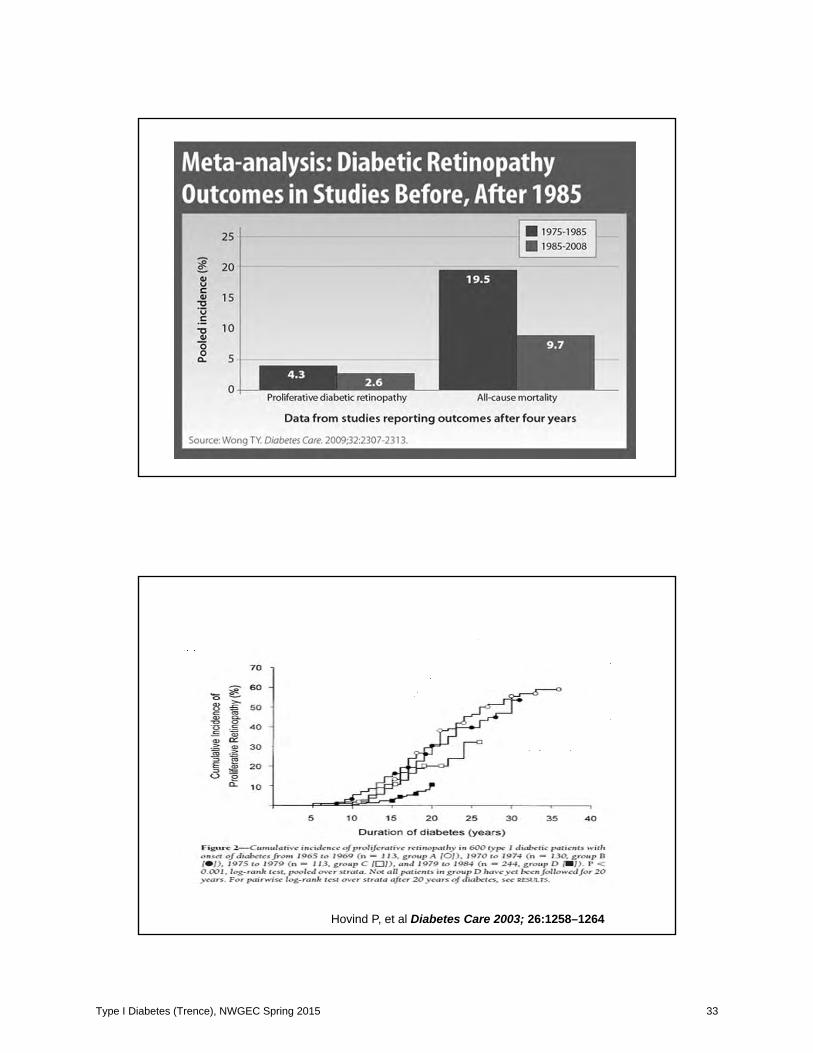
Hovind P, et al Diabetes Care 2003; 26:1258–1264
Type I Diabetes (Trence), NWGEC Spring 2015 33
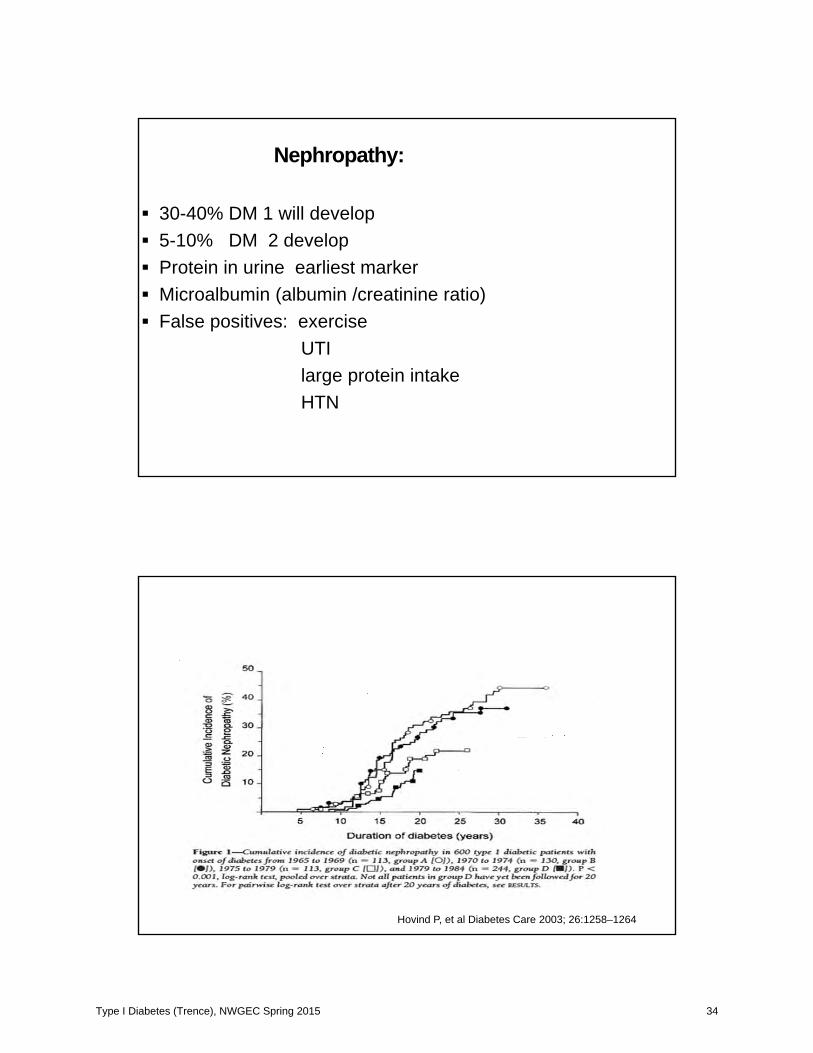
Nephropathy:
30-40% DM 1 will develop5-10% DM 2 developProtein in urine earliest markerMicroalbumin (albumin /creatinine ratio)False positives: exercise
UTIlarge protein intakeHTN
Hovind P, et al Diabetes Care 2003; 26:1258–1264
Type I Diabetes (Trence), NWGEC Spring 2015 34
Type I Diabetes (Trence), NWGEC Spring 2015 35
Challenges in the Management ofType 1 Diabetes in Older Adults
Type 1 Diabetes (T1D) Exchange clinic registry reported characteristics of older adults with type 1 diabetes followed in diabetes centers across US 50 to < 65 years (n = 2,066), mean A1C 7.7% (27% had an A1C < 7.0%, 46% had an A1C < 7.5%, and 11% had an A1C 9.0%), mean self-reported blood glucose testing was
5.5/day 65 years of age(n = 683), mean A1C 7.4% (34% A1C <
7.0%, 52% A1C < 7.5%, and 8% had A1C 9.0%)Mean self-reported blood glucose testing 5.6 times daily.
Dhaliwal R et al Diabetes Spectrum 2014; 27,
Greater frequency of self-monitoring of blood glucose (SMBG) associated with lower A1C levels in both those who used an insulin pump vs insulin via injectionsDiabetic ketoacidosis (DKA) was lower with increasing age and was not associated with duration of diabetes.DKA was more likely in those with higher A1C levels and lower socioeconomic status. No relationship between DKA and pump versusinjection use.
Type I Diabetes (Trence), NWGEC Spring 2015 36
HypoglycemiaSevere hypoglycemia, defined as an episode requiring assistance for treatment, has been associated with cardiac abnormalities including arrhythmias and brain damage. Hypoglycemia unawareness or poor awareness are major risk factors for severe and recurrent hypoglycemia in type 1 diabetes and are of particular concern in the elderly because of increased risk of falls, cognitive impairments, and cardiovascular disease. With aging and long duration of diabetes, there isimpairment of counterregulatory hormone releaseConfusion, dizziness, falling, weakness, difficulty withcommunication, and poor coordination and balance may not be recognized as possible symptoms of hypoglycemia
T1D Exchange: 18.6% with diabetes 40 yearsof age (n = 758) self-reported having had a seizure or loss of consciousness in previous 12 months. Duration of DM associated with occurrence of severe hypoglycemia, also lower education status,lower household income, lack of private insurance,and race (greater in non-Hispanic blacks andHispanics than in non-Hispanic whites). Injection users had more severe hypoglycemia than pump users.
Self-reported severe hypoglycemia lowest with mean A1C 7.0–7.5%.
Type I Diabetes (Trence), NWGEC Spring 2015 37
U.K. Hypoglycemia Study
46% prevalence over 12 months of severe hypoglycemia in adults with type 1 DM of > 15 yrs’ duration (mean age 53 years, A1C 7.8%).Severe hypoglycemia more common in presence of
nephropathy, neuropathy, and depression and with the use of nonselective -blockers and alcohol
Recent study of adults 69 yrs (both type 1 and 2 with an A1C > 8%)72 hours of continuous glucose monitoring (CGM), 65% experienced hypoglycemia at least once.
Arch Intern Med 2011;171:362–364,
Type I Diabetes (Trence), NWGEC Spring 2015 38

Challenges specific to older adults:
Type I Diabetes (Trence), NWGEC Spring 2015 39
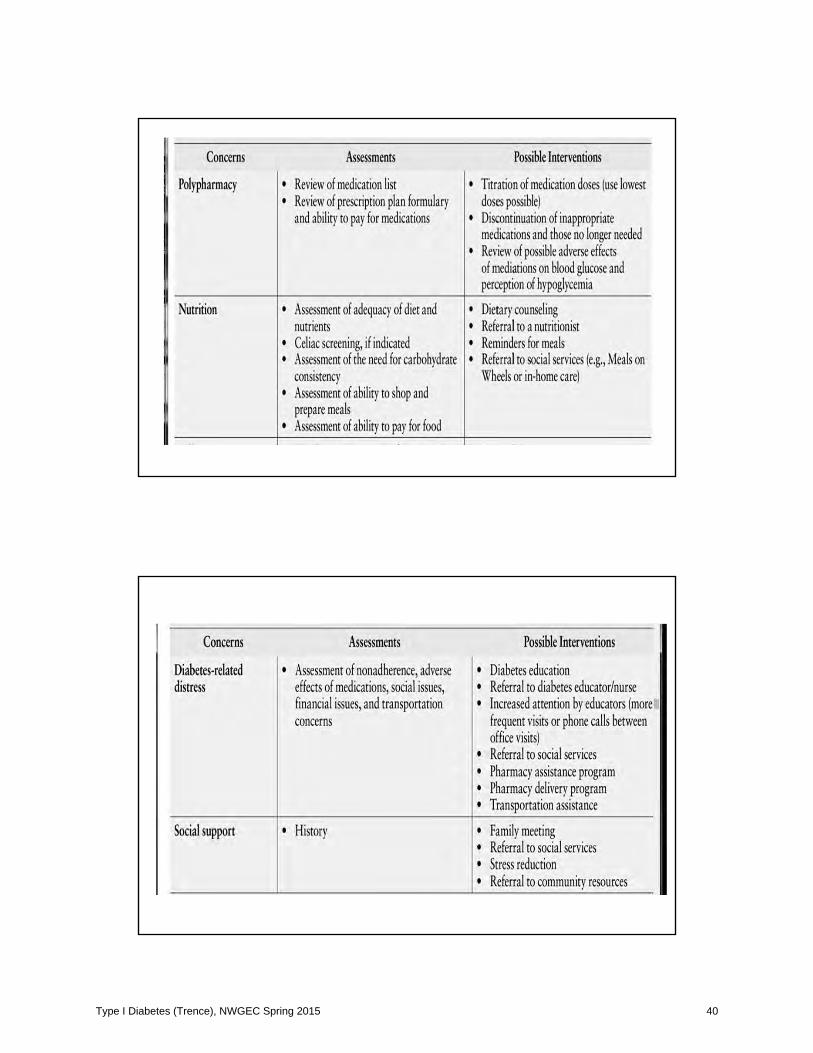
Type I Diabetes (Trence), NWGEC Spring 2015 40

Type I Diabetes (Trence), NWGEC Spring 2015 41

Additional Concerns:
LiteracyIncome/coverage (donut hole)Comprehension levelDenial of diseaseTechnology averseSocial isolationFear
“Too often we underestimate the power of a touch, a smile, a kind word, a listening ear, an honest compliment, or the smallest act of caring, all of which have the potential to turn a life around.”
Leo Buscaglia
Type I Diabetes (Trence), NWGEC Spring 2015 42

















